")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Relationship Between Employment Status and Unstable Periods in Outpatients with Bipolar Disorder: A Multicenter Treatment Survey for Bipolar Disorder in Psychiatric Outpatient Clinics (MUSUBI) Study
Authors Ikenouchi A , Konno Y , Fujino Y , Adachi N , Kubota Y , Azekawa T , Ueda H, Edagawa K, Katsumoto E, Goto E, Hongo S, Kato M, Tsuboi T , Yasui-Furukori N , Nakagawa A , Kikuchi T, Watanabe K , Yoshimura R
Received 19 December 2021
Accepted for publication 22 March 2022
Published 8 April 2022 Volume 2022:18 Pages 801—809
DOI https://doi.org/10.2147/NDT.S353460
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Atsuko Ikenouchi,1,2 Yusuke Konno,1,3 Yoshihisa Fujino,3 Naoto Adachi,4 Yukihisa Kubota,4 Takaharu Azekawa,4 Hitoshi Ueda,4 Koji Edagawa,4 Eiichi Katsumoto,4 Eiichiro Goto,4 Seiji Hongo,4 Masaki Kato,5,6 Takashi Tsuboi,5,7 Norio Yasui-Furukori,5,8 Atsuo Nakagawa,5,9 Toshiaki Kikuchi,5,9 Koichiro Watanabe,5,7 Reiji Yoshimura1,5
1Department of Psychiatry, University of Occupational and Environmental Health, Japan, Kitakyushu, Japan; 2Medical Center for Dementia, Hospital of the University of Occupational and Environmental Health, Japan, Kitakyushu, Japan; 3Department of Environmental Epidemiology, Institute of Ecological Sciences, University of Occupational and Environmental Health, Japan, Kitakyushu, Japan; 4The Japanese Association of Neuro-Psychiatric Clinics, Tokyo, Japan; 5The Japanese Society of Clinical Neuropsychopharmacology, Tokyo, Japan; 6Department of Neuropsychiatry, Kansai Medical University, Osaka, Japan; 7Department of Neuropsychiatry, Kyorin University, Tokyo, Japan; 8Department of Psychiatry, Dokkyo Medical University, Tochigi, Japan; 9Department of Neuropsychiatry, Keio University, Tokyo, Japan
Correspondence: Atsuko Ikenouchi, Department of Psychiatry, University of Occupational and Environmental Health, Japan, 1-1 Iseigaoka, Yahatanishiku, Kitakyushu, 807-8555, Japan, Tel +81-93-691-7253, Fax +81-93-692-4894, Email [email protected]
Purpose: To clarify the relationship between the length of unstable periods and employment status of patients with bipolar disorder.
Patients and Methods: Medical records of outpatients with bipolar disorder who visited 176 member clinics of the Japanese Association of Neuro-Psychiatric Clinics were investigated during September–October 2016, and details of their medical care and employment were surveyed using a questionnaire. The odds ratios (ORs) of length of unstable period and unemployment were analyzed with a logistic regression model.
Results: The study included 816 patients, of whom 707 were employed full-time (continuous employment) and 70 were unemployed (loss of employment). Univariate analysis showed that ORs were statistically significant for patients who were unstable for “almost all” of the year (OR = 10.4 [4.48– 24.28] p < 0.001), but not for “few” unstable periods (OR = 1.06 [0.56– 1.98] p = 0.849) and for “significant” unstable periods (OR = 1.65 [0.73– 3.74] p = 0.231) were not significantly different. Multivariate analysis showed that ORs were statistically “significant” for patients who were unstable for “almost all” (OR = 12.1 [4.37– 33.3] p < 0.001), but not for “few” unstable periods (OR = 1.07 [0.55– 2.07] p = 0.846) and for “significant” unstable periods (OR = 1.62 [0.66– 3.98] p = 0.290) did not differ significantly.
Conclusion: Patients with bipolar disorder with a long unstable period were associated with a higher risk of unemployment.
Keywords: mood disorder, loss of employment, nationwide study, real world
Introduction
Bipolar disorder is a chronic psychiatric disorder with both manic and depressive episodes that recur many times, often in one’s late teens or twenties.1 Bipolar I disorder is defined by the presence of symptomatic manic episodes, and the worldwide lifetime prevalence is estimated to be 0.6–1.0%. Bipolar II disorder, defined by the presence of symptomatic hypomanic and major depressive episodes, has a worldwide lifetime prevalence estimated at 0.4 to 1.1%.2 The lifetime prevalence of bipolar disorder in Japan has been estimated to range from 0.09% to 0.60%.2–4
Bipolar disorder results in a significant decline in daily functioning, including participation in work, social relationships, and the ability to live independently.5 The Global Burden of Disease Study showed that disability-adjusted life years (DALYs) become apparent in teenage years and peak in the twenties.6 A Danish study found that patients diagnosed with bipolar disorder were less likely to be employed with an odds ratio (OR) of 0.16.7 Three years before being diagnosed with bipolar disorder, 45% of the people with bipolar disorder were employed. However, this decreased to 34% five years after diagnosis.8 A survey of large Japanese companies revealed that the average number of sick days due to mental illnesses such as depression and bipolar disorder is approximately 120 days.9 A nationwide study in Sweden found that bipolar patients were 30% less likely to be able to work compared to the age-standardized population; of the 40% who were employed, 64% reported sick leave and 46% took more than 100 days/year.10 These results suggest that patients with bipolar disorder have low rates of employment, and those who are employed have high rates of sick leave.
These employment problems affect both the individual and society. Bipolar disorder has significant direct and indirect costs. Miller et al reported that the estimated total costs due to bipolar disorder in the US in 2009 were $151 billion (direct costs: $30.7 billion; indirect costs: $120.3 billion).11 Since there are approximately 120,000 people with bipolar disorder in Japan, it is medically and socially important to develop supportive measures.12
The factors affecting the employment of patients with bipolar disorder are not well known. We previously reported a higher risk of unemployment during episodes of mania and depression compared to remission.13 Stability of the bipolar patients’ condition may be one of the factors associated with continued employment. The present study aimed to clarify the relationship between the duration of instability and employment status of patients with bipolar disorder.
Materials and Methods
Participants and Methods
A retrospective cohort investigation of the Multicenter Treatment Survey for Bipolar Disorder in Psychiatric Clinics (MUSUBI) project was conducted at 1650 member clinics of the Japanese Association of Neuro-Psychiatric Clinics (JAPC).13–18 The JAPC member clinics treat about 30% of mood disorder patients in Japan.16 A total of 176 JAPC members took the survey in this study. All investigators at these clinics are psychiatrists, most of whom are either board certified by the Japanese Society of Psychiatry and Neurology or board certified by the Ministry of Health, Labor and Welfare.
All medical records of patients with bipolar disorder who visited the 176 member clinics of the JAPC in September- October 2016 were investigated in September-December 2017. We gathered demographic information about the patients (age, sex, marital status, and occupational status), information about psychiatric and physical comorbidities, substance abuse, bipolar disorder subcategories, rapid cycling, psychotic symptoms, depressive symptoms, manic symptoms, suicidal ideation, details of pharmacological treatment, and unstable period at two intervals, October-December 2016 and October-December 2017. The diagnosis of bipolar disorder was based on the International Classification of Diseases and Related Health Problems, 10th edition (ICD-10). Clinical psychiatrists who participated in the survey completed the questionnaire through a retrospective medical record survey.
The unstable period was defined as the time when some psychiatric symptoms were strong or when daily functioning was impaired. The unstable period was defined as “few” if it was between 1–33% of the year, “significant” if it was between 34–66%, and “almost all” if it was between 67–100%.
Regarding employment status, we defined full-time workers as those who worked 30 hours or more per week. We defined “continuous employment” as those who were working full time in 2016 (our baseline year) and were still working full time in 2017 (one year later), and “loss of employment” as those who were working full-time in 2016 and were unemployed one year later.
Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki and the Japanese Ethical Guidelines for Medical and Health Research Involving Human Subjects. Before the initiation of the study, the study protocol was reviewed and approved by the institutional review board of the ethics committee of the Japanese Association of Neuro-Psychiatric Clinics and the University of Occupational and Environmental Health, Japan. These ethics committees also exempted us from obtaining informed consent because this study is a retrospective medical record survey. Instead, we published information about this study to give patients the freedom to opt-out. To protect patients’ personal information, we assigned each patient an arbitrary identification number for this study.
Statistical Analysis
In the univariate analysis, we performed a logistic regression between unstable period and continuous employment. To avoid confounding effects of each factor, multivariate logistic regression analysis was then conducted. The multivariate logistic regression analysis used employment status as the dependent variable. We analyzed the OR of unstable period to employment status (few: 1–33%, significant: 34–66%, almost all: 67–100%) using a logistic regression model. Details of all the above patients were included in this model as confounding adjustment factors. The level of probability was set at 5%. The analysis was performed using Stata SE/17 (Stata Corp LLC, College Station, TX, USA).
Results
As the baseline, questionnaires returned from 176 clinics for 3137 outpatients with bipolar disorder, of whom 3081 provided their occupation, were used. Among the 3081 patients, 2292 were aged < 60 years, of which 997 (43.5%) were full-time workers. A follow-up study was conducted one year later on these 968 patients who were full-time workers aged < 59 years. Finally, the study included 816 patients (84.3%), of whom 707 were employed full-time (continuous employment) and 70 were unemployed (loss of employment). Data of the patients in the continuous and loss of employment groups are presented in Table 1. Although the age and bipolar subcategories were relatively similar between the two groups, there were differences in other attributes, symptoms, and treatment.
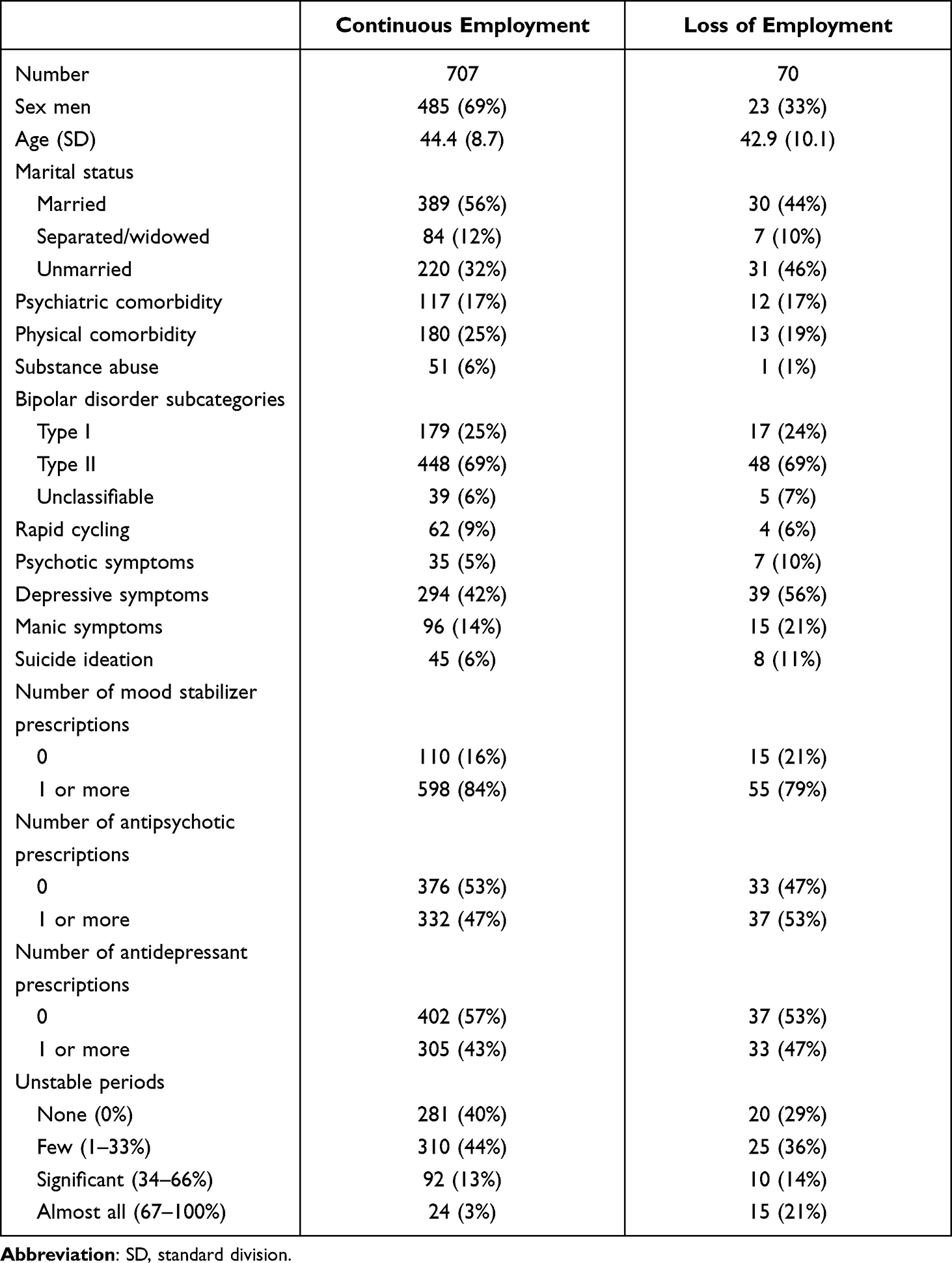 |
Table 1 Clinical Characteristics of Patients with Continuous Employment and Loss of Employment |
The findings of the univariate and multivariate analyses are shown in Table 2. The univariate analysis showed that the OR for unemployment was statistically significant for those who were unstable for “almost all” of the year, ie, those who spent 67–100% of the year in an unstable (OR = 10.4 [4.48–24.28] p < 0.001) state of mind. However, no significant differences were found for those who had “few” unstable periods (OR = 1.06 [0.56–1.98] p = 0.849) or “significant” periods of instability (OR = 1.65 [0.73–3.74] p = 0.231). The multivariate analysis showed that the OR for unemployment was statistically significant for those who had “almost all” unstable periods (OR = 12.1 [4.37–33.31] p < 0.001). No significant difference was noted for “few” unstable periods (OR = 1.07 [0.55–2.07] p = 0.846) and “significant” unstable periods (OR = 1.62 [0.66–3.98] p = 0.290).
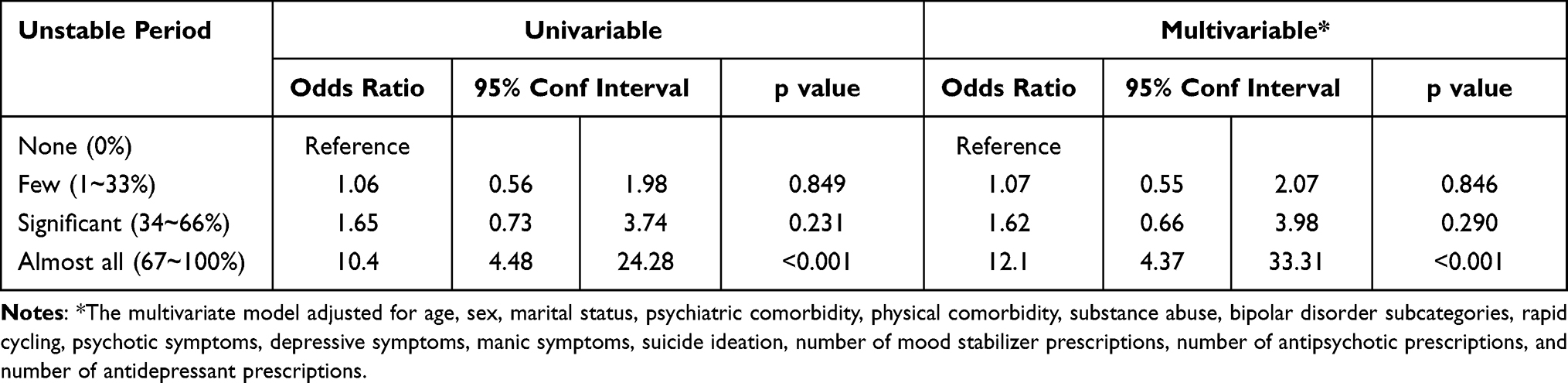 |
Table 2 Association Between Unstable Periods and Continuous Employment |
The multivariate analysis showed no significant differences for physical complications (OR = 0.48 [0.23–1.02] p = 0.055), substance abuse (OR = 0.15 [0.15–1.58] p = 0.115), and rapid cycling (OR = 0.39 [0.07–2.03] p = 0.262). Significant differences were noted for women (OR=4.60 [2.51–8.42] p < 0.001) as compared to men.
Discussion
This study was conducted to investigate the impact of unstable periods on continued employment in patients with bipolar disorder. In this nationwide multicenter study, we investigated the employment status of patients with bipolar disorder in Japan from 2016 to 2017. The findings suggested that the employment rate of patients with bipolar disorder was 43.5%. Studies published overseas have reported that the employment rate of bipolar patients is 40–60%, which is similar to the results of this study.8,19,20
Among those who were employed, patients with bipolar disorder who were unstable for more than two-thirds of the time had 12.1 times higher risk of loss of employment in the multivariate analysis compared to those who were stable. In contrast, patients with bipolar disorder who were unstable for less than two-thirds of the time did not have an increased risk of unemployment. In other words, patients with mild to moderate mood instability can sustain employment. The reason for the drastic increase in the OR over the border is unknown.
Previous reports indicate that two-thirds of employed patients with bipolar disorder take sick leave, and half of these patients take more than 100 days of leave per year.10 Bipolar disorder results in impaired cognitive and occupational functioning, which leads to poor workplace performance and reduced job functioning.21–23 Factors associated with poor occupational and functional outcomes in bipolar disorder include the number of affective episodes,24 severity of total symptoms,25 subclinical depressive symptoms,26 history of psychotic symptoms,27 history of psychiatric hospitalization,8,25,28 comorbid psychiatric disorders,24,29 substance abuse,8,24 age,8 and age of onset.29,30 We also reported that patients with depressive or manic episodes have a higher risk of unemployment than those in remission.13 It has been reported that the primary factor associated with occupational dysfunction in patients with bipolar disorder is impairment in executive functioning, rather than other important clinical factors such as general cognitive functioning (IQ) or severity of illness.31 Kato et al reported that patients with bipolar disorder employed in Japan had significantly higher activity impairment, presenteeism, and lower work productivity, resulting in greater indirect costs, and total indirect costs were higher for patients with bipolar disorder than for those with major depressive disorder, and even higher for patients with severe depressive symptoms.3
Environmental factors such as support systems for the patients in the company and their family members might influence the continuation of employment.8,25 In Japan, employees can take sick leave, and this period can vary from a few months to several years, depending on the workplace. Typically, no salary is paid during this period, but the health insurance association will provide an injury and illness allowance for one year and six months. This is available to all workers, but some companies offer more generous coverage. These leave programs vary among countries, so these results may not be generalizable to countries outside Japan.
In this study, the incidence of psychotic symptoms and suicidal ideation was lower in the continuous employment group than in loss of employment group, but there was no difference in the incidence of psychological comorbidities. Meanwhile, the incidence of physical comorbidity, substance abuse, and rapid cycling was higher among the continuously employed group than among the unemployed group in this study. Some unmeasured biases may have influenced these results.
The rate of continued employment was higher for men with bipolar disorder than for women with the same disorder. This difference is consistent with the findings of several studies.32,33 One possible reason for this gender difference is that women with bipolar disorder often spend more time in a depressed state and have more rapid changes in their condition than men.32,33 Depressive symptoms and faster illness cycle lapse are both associated with decreased employability.25,34,35 In addition, a survey by the Ministry of Health, Labor and Welfare (2019) reported that the turnover rate of full-time workers in Japan in 2019 was 13.4% for men and 18.2% for women.36 Therefore, this result may be influenced by social gender differences in Japan.
Previous studies have reported that among patients with bipolar disorder, being unemployed is associated with poorer cognitive and social functioning, higher depressive symptoms, and lower educational qualification.25,34,37–39 Conversely, longitudinal qualitative studies show that people with bipolar disorder who obtain employment often experience a significant improvement in their living conditions.40,41 The likelihood of future psychiatric hospitalization is reduced when unemployed people with severe mental illness find employment, especially when employment is maintained for more than six months.42 Clinicians should support patients in maintaining employment, not only because working is a valuable outcome in and of itself, but also because working leads to fewer hospitalizations.
The strength of this study is that it is a real-world study using data from a multi-institutional setting that treats the majority of the patients with mood disorders in Japan. However, the current study also has several limitations. First, the risk of long-term unemployment is unknown because the present study only included a one-year retrospective follow-up. Considering the course of bipolar disorder, a longer study is desirable, including a survey of those who have started working. Second, the follow-up rate after one year was relatively good at 84.3%, but the effect of dropouts was unknown. Third, since our study focused on the relationship between symptom instability and unemployment over a one-year period, the modifying effects of treatment and detailed comorbidities are unknown. In particular, the impact of treatment is unknown because they are clinically controlled by the patient’s primary care physician. In this study, medications and other treatments were considered, but adherence was unknown, and non-pharmacological treatments such as psychotherapy were not considered. Fourth, although the study was conducted by well-trained physicians, it was conducted concurrently with routine clinical care, and thus was assessed in a single interview and no structured clinical interview was conducted, which may have resulted in rater variability. Fifth, we did not assess baseline functioning and did not use a rating scale, which may have reduced the accuracy of the assessment.
Conclusion
The MUSUBI Study found that 43.5% of patients with bipolar disorder receiving outpatient treatment were full-time workers. Assessment of stability by a well-trained physician predicts the risk of unemployment; patients with bipolar disorder whose condition is unstable most of the time are at a high risk of unemployment. In order for patients with bipolar disorder to continue working, there is a need for support which will increase the period of stability.
Abbreviations
DALYs, disability-adjusted life years; OR, odds ratio; MUSUBI, Multicenter Treatment Survey for Bipolar Disorder in Psychiatric Clinics; JPAC, Japanese Association of Neuro-Psychiatric Clinics; ICD-10, International Classification of Diseases and Related Health Problems, 10th edition.
Ethics Approval
The study was approved by the Ethics Committee of the Japanese Association of Neuro-Psychiatric Clinics (ID: 20160822. 20180723) and the Ethics Committee of Medical Research at the University of Occupational and Environmental Health, Japan (UOEHCRB20-112).
Consent for Publication
The study was disclosed on our webpage, and patients were allowed to opt out.
Acknowledgments
This study was supported by the Ken Tanaka Memorial Research Grant. The authors thank the following psychiatrists belonging to the Japanese Association of Neuro-Psychiatric Clinics: Dr. Toshihiko Lee, Dr. Norio Okamoto, Dr. Makoto Nakamura, Dr. Junkou Sato, Dr. Kazunori Otaka, Dr. Satoshi Terada, Dr. Tadashi Ito, Dr. Munehide Tani, Dr. Atsushi Satomura, Dr. Hiroshi Sato, Dr. Hideki Nakano, Dr. Yoichi Nakaniwa, Dr. Eiichi Hirayama, Dr. Keiichi Kobatake, Dr. Koji Tanaka, Dr. Mariko Watanabe, Dr. Shiguyuki Uehata, Dr. Asana Yuki, Dr. Nobuko Akagaki, Dr. Michie Sakano, Dr. Akira Matsukubo, Dr. Yukihisa Kibota, Dr. Yasuyuki Inada, Dr. Hiroshi Oyu, Dr. Tsuneo Tsubaki, Dr. Tatsuji Tamura, Dr. Shigeki Akiu, Dr. Atsuhiro Kikuchi, Dr. Keiji Sato, Dr. Kazuyuki Fujita, Dr. Fumio Handa, Dr. Hiroyuki Karasawa, Dr. Kazuhiro Nakano, Dr. Kazuhiro Omori, Dr. Seiji Tagawa, Dr. Daisuke Maruno, Dr. Hiroaki Furui, Dr. You Suzuki, Dr. Takeshi Fujita, Dr. Yukimitsu Hoshino, Dr. Kikuko Ota, Dr. Akira Itami, Dr. Kenichi Goto, Dr. Yoshiaki Yamano, Dr. Kiichiro Koshimune, Dr. Junko Matsushita, Dr. Takatsugu Nakayama, Dr. Kazuyoshi Takamuki, Dr. Nobumichi Sakamoto, Dr. Miho Shimizu, Dr. Muneo Shimura, Dr. Norio Kawase, Dr. Ryouhei Takeda, Dr. Takuya Hirota, Dr. Hideko Fujii, Dr. Yoichiro Watanabe, Dr. Riichiro Narabayashi, Dr. Yutaka Fujiwara, Dr. Kazu Kobayashi, Dr. Yuko Urabe, Dr. Miyako Oguru, Dr. Osamu Miura, Dr. Yoshio Ikeda, Dr. Hidemi Sakamoto, Dr. Yosuke Yonezawa, Dr. Yoichi Takei, Dr. Toshimasa Sakane, Dr. Kiyoshi Oka, Dr. Kyoko Tsuda, Dr. Shigemitsu Hayashi, Dr. Kunihiko Kawamura, Dr. Yasushi Furuta, Dr. Kazuko Miyauchi, Dr. Yoshio Miyauchi, Dr. Mikako Oyama, Dr. Keizo Hara, Dr. Misako Sakamoto, Dr. Shigeki Masumoto, Dr. Yasuhiro Kaneda, Dr. Yoshiko Kanbe, Dr. Masayuki Iwai, Dr. Naohisa Waseda, Dr. Nobuhiko Ota, Dr. Takahiro Hiroe, Dr. Ippei Ishii, Dr. Hideki Koyama, Dr. Terunobu Otani, Dr. Osamu Takatsu, Dr. Takashi Ito, Dr. Norihiro Marui, Dr. Toru Takahashi, Dr. Tetsuro Oomori, Dr. Toshihiko Fukuchi, Dr. Kazumichi Egashira, Dr. Kiyoshi Kaminishi, Dr. Ryuichi Iwata, Dr. Satoshi Kawaguchi, Dr. Yoshinori Morimoto, Dr. Hirohisa Endo, Dr. Yasuo Imai, Dr. Eri Kohno, Dr. Aki Yamamoto, Dr. Naomi Hasegawa, Dr. Sadamu Toki, Dr. Hideyo Yamada, Dr. Hiroyuki Taguchi, Dr. Hiroshi Yamaguchi, Dr. Hiroki Ishikawa, Dr. Sakura Abe, Dr. Kazuhiro Uenoyama, Dr. Kazunori Koike, Dr. Yoshiko Kamekawa, Dr. Michihito Matsushima, Dr. Ken Ueki, Dr. Sintaro Watanabe, Dr. Tomohide Igata, Dr. Yoshiaki Higashitani, Dr. Eiichi Kitamura, Dr. Junko Sanada, Dr. Takanobu Sasaki, Dr. Kazuko Eto, Dr. Ichiro Nasu, Dr. Kenichiro Sinkawa, Dr. Yukio Oga, Dr. Michio Tabuchi, Dr. Daisuke Tsujimura, Dr. Tokunai Kataoka, Dr. Kyohei Noda, Dr. Nobuhiko Imato, Dr. Ikuko Nitta, Dr. Yoshihiro Maruta, Dr. Satoshi Seura, Dr. Toru Okumura, Dr. Osamu Kino, Dr. Tomoko Ito, Dr. Ryuichi Iwata, Dr. Wataru Konno, Dr. Toshio Nakahara, Dr. Masao Nakahara, Dr. Hiroshi Yamamura, Dr. Masatoshi Teraoka, Dr. Masato Nishio, Dr. Miwa Mochizuki, Dr. Tsuneo Saitoh, Dr. Tetsuharu Kikuchi, Dr. Chika Higa, Dr. Hiroshi Sasa, Dr. Yuichi Inoue, Dr. Muneyoshi Yamada, Dr. Yoko Fujioka, Dr. Kuniaki Maekubo, Dr. Hiroaki Jitsuiki, Dr. Toshihito Tsutsumi, Dr. Yasumasa Asanobu, Dr. Seiji Inomata, Dr. Kazuhiro Kodama, Dr. Aikihiro Takai, Dr. Asako Sanae, Dr. Shinichiro Sakurai, Dr. Kazuhide Tanaka, Dr. Masahiko Shido, Dr. Haruhisa Ono, Dr. Wataru Miura, Dr. Yukari Horie, Dr. Tetso Tashiro, Dr. Tomohide Mizuno, Dr. Naohiro Fujikawa, Dr. Hiroshi Terada, Dr. Kenji Taki, Dr. Kyoko Kyotani, Dr. Masataka Hatakoshi, Dr. Katsumi Ikeshita, Dr. Keiji Kaneta, Dr. Ritsu Shikiba, Dr. Tsuyoshi Iijima, Dr. Masaru Yoshimura, Dr. Masumi Ito, Dr. Shunsuke Murata, Dr. Mio Mori, and Dr. Toshio Yokouchi.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Ken Tanaka Memorial Research Grant.
Disclosure
Atsuko Ikenouchi, Yusuke Konno, Yoshihisa Fujino, and Naoto Adachi declare no conflicts of interest for this article. Yukihisa Kubota has received consultant fees from Pfizer and Meiji Seika Pharma and speaker’s honoraria from Meiji Seika Pharma, Eli Lilly, Janssen Pharmaceutical, Dainippon Sumitomo Pharma, MSD, Lundbeck Japan, Mitsubishi Tanabe Pharma, Takeda Pharmaceutical, Yoshitomi Yakuhin, Otsuka Pharmaceutical, and Eisai. Takeharu Azekawa received speaker honoraria from Eli Lilly, Otsuka Pharmaceutical, Eisai Co., Ltd, Sumitomo Dainippon Pharma, and Pfizer. Hitoshi Ueda has received manuscript fees or speaker’s honoraria from Eli Lilly, Janssen Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, Takeda Pharmaceutical, and Yoshitomi Yakuhin. Koji Edagawa has received speaker honoraria from Eli Lilly, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, Kyowa, and Yoshitomi Yakuhin. Eiichi Katsumoto has received speaker honoraria from Daiichi Sankyo, Eisai, Eli Lilly, Janssen Pharmaceutical, Kyowa Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, Takeda Pharmaceutical Company Limited, TOWA PHARMACEUTICAL CO., LTD, Lundbeck Japan K.K., Viatris Inc., Yoshitomiyakuhin Corporation, and UCB. Eiichiro Goto has received manuscript fees or speaker honoraria from Eli Lilly, Eisai, KYOWA Pharmaceutical Industry, Janssen Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Sumitomo Dainippon Pharma. Seiji Hongo has received manuscript fees or speaker’s honoraria from Eli Lilly, Janssen Pharmaceutical, Kyowa Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, Otsuka Pharmaceutical, Pfizer, Shionogi, Sumitomo Dainippon Pharma, and Yoshitomi Yakuhin. Masaki Kato has received grant funding from the Japanese Ministry of Health, Labor and Welfare, the Japan Society for the Promotion of Science, Japanese Society of Clinical Neuropsychopharmacology, SENSHIN Medical Research Foundation, Japan Research Foundation for Clinical Pharmacology, and speaker’s honoraria from Dainippon Sumitomo Pharma, Otsuka, Meiji Seika Pharma, Eli Lilly, MSD K.K., GlaxoSmithkline, Pfizer, Janssen Pharmaceutical, Shionogi, Mitsubishi Tanabe Pharma, Takeda Pharmaceutical, Lundbeck, and Ono Pharmaceutical. Takeshi Tsuboi has received consultant fees from Pfizer and speaker’s honoraria from Eli Lilly, Meiji Seika Pharma, MSD, Janssen Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Yoshitomi Yakuhin, Mochida Pharmaceutical, Otsuka Pharmaceutical, Kyowa Pharmaceutical, and Takeda Pharmaceutical. Norio Yasui-Furukori has received grant/research support or honoraria from and has been on the speakers of Dainippon Sumitomo Pharma, Mochida Pharmaceutical, MSD, and Otsuka Pharmaceutical. Atsuo Nakagawa has received lecture fees from Pfizer, Eli Lilly, Otsuka, Janssen Pharmaceutical, Mitsubishi Tanabe, Mochida, Dainippon Sumitomo, Yoshitomi Yakuhin, MSD, and NTT Docomo, and participated in an advisory board for Takeda, Meiji Seika, and Tsumura. Toshiaki Kikuchi received consultant fees from Takeda Pharmaceutical and the Center for Cognitive Behavioral Therapy and Training. Koichiro Watanabe has received manuscript fees or speaker’s honoraria from Daiichi Sankyo, Eisai, Eli Lilly, GlaxoSmithKline, Janssen Pharmaceutical, Kyowa Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Shionogi, Sumitomo Dainippon Pharma, Takeda Pharmaceutical, Lundbeck Japan, Viatris, Yoshitomi Yakuhin, and has received research/grant support from Astellas Pharma, Daiichi Sankyo, Eisai, MSD, Mitsubishi Tanabe Pharma, Meiji Seika Pharma, Otsuka Pharmaceutical, Pfizer, Shionogi, Sumitomo Dainippon Pharma, and is a consultant from Eisai, Eli Lilly, Kyowa Pharmaceutical, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, Taisho Toyama Pharma Pharmaceutical. Reiji Yoshimura has received speaker honoraria from Eli Lilly, Janssen, Dainippon Sumitomo, Otsuka, Meiji, Pfizer, and Shionogi. The authors report no other conflicts of interest in this work.
References
1. Bauer M, Glenn T, Alda M, et al. Influence of birth cohort on age of onset cluster analysis in bipolar I disorder. Eur Psychiatry. 2015;30(1):99–105. doi:10.1016/j.eurpsy.2014.10.005
2. Merikangas KR, Jin R, He JP, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. 2011;68(3):241–251. doi:10.1001/archgenpsychiatry.2011.12
3. Kato T, Baba K, Guo W, Chen Y, Nosaka T. Impact of bipolar disorder on health-related quality of life and work productivity: estimates from the national health and wellness survey in Japan. J Affect Disord. 2021;295:203–214. doi:10.1016/j.jad.2021.07.104
4. Nishi D, Ishikawa H, Kawakami N. Prevalence of mental disorders and mental health service use in Japan. Psychiatry Clin Neurosci. 2019;73(8):458–465. doi:10.1111/pcn.12894
5. Strassnig M, Kotov R, Fochtmann L, Kalin M, Bromet EJ, Harvey PD. Associations of independent living and labor force participation with impairment indicators in schizophrenia and bipolar disorder at 20-year follow-up. Schizophr Res. 2018;197:150–155. doi:10.1016/j.schres.2018.02.009
6. Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. doi:10.1016/S0140-6736(13)61611-6
7. Sletved KSO, Ziersen SC, Andersen PK, Vinberg M, Kessing LV. Socio-economic functioning in patients with bipolar disorder and their unaffected siblings—results from a nation-wide population-based longitudinal study. Psychol Med. 2021;2021:1–8. doi:10.1017/S0033291721002026
8. Holm M, Taipale H, Tanskanen A, Tiihonen J, Mitterdorfer-Rutz E. Employment among people with schizophrenia or bipolar disorder: a population-based study using nationwide registers. Acta Psychiatr Scand. 2021;143(1):61–71. doi:10.1111/acps.13254
9. Muto T, Sumiyoshi Y, Sawada S, et al. Sickness absence due to mental disorders in Japanese workforce. Ind Health. 1999;37(2):243–252. doi:10.2486/indhealth.37.243
10. Carlborg A, Ferntoft L, Thuresson M, Bodegard J. Population study of disease burden, management, and treatment of bipolar disorder in Sweden: a retrospective observational registry study. Bipolar. 2015;17(1):76–85. doi:10.1111/bdi.12234
11. Miller S, Dell’Osso B, Ketter TA. The prevalence and burden of bipolar depression. J Affect Disord. 2014;169(suppl 1):S3–S11. doi:10.1016/S0165-0327(14)70003-5
12. Ministry of Health, Labor and Welfare. Patient survey. Available from: https://www.mhlw.go.jp/toukei/list/10-20.html.
13. Konno Y, Fujino Y, Ikenouchi A, et al. Relationship between mood episode and employment status of outpatients with bipolar disorder: retrospective cohort study from the multicenter treatment survey for bipolar disorder in psychiatric clinics (MUSUBI) project. Neuropsychiatr Dis Treat. 2021;17:2867–2876. doi:10.2147/NDT.S322507
14. Yasui-Furukori N, Adachi N, Kubota Y, et al. Factors associated with doses of mood stabilizers in real-world outpatients with bipolar disorder. Clin Psychopharmacol Neurosci. 2020;18(4):599–606. doi:10.9758/cpn.2020.18.4.599
15. Tokumitsu K, Yasui-Furukori N, Adachi N, et al. Real-world clinical features of and antidepressant prescribing patterns for outpatients with bipolar disorder. BMC Psychiatry. 2020;20(1):555. doi:10.1186/s12888-020-02967-5
16. Adachi N, Azekawa T, Edagawa K, et al. Estimated model of psychotropic polypharmacy for bipolar disorder: analysis using patients’ and practitioners’ parameters in the MUSUBI study. Hum Psychopharmacol. 2021;36(2):e2764. doi:10.1002/hup.2764
17. Kato M, Adachi N, Kubota Y, et al. Clinical features related to rapid cycling and one-year Euthymia in bipolar disorder patients: a multicenter treatment survey for bipolar disorder in psychiatric clinics (MUSUBI). J Psychiatr Res. 2020;131:228–234. doi:10.1016/j.jpsychires.2020.09.030
18. Tsuboi T, Suzuki T, Azekawa T, et al. Factors associated with non-remission in bipolar disorder: the multicenter treatment survey for bipolar disorder in psychiatric outpatient clinics (MUSUBI). Neuropsychiatr Dis Treat. 2020;16:881–890. doi:10.2147/NDT.S246136
19. Marwaha S, Durrani A, Singh S. Employment outcomes in people with bipolar disorder: a systematic review. Acta Psychiatr Scand. 2013;128(3):179–193. doi:10.1111/acps.12087
20. Kupfer DJ, Frank E, Grochocinski VJ, Cluss PA, Houck PR, Stapf DA. Demographic and clinical characteristics of individuals in a bipolar disorder case registry. J Clin Psychiatry. 2002;63(2):120–125. doi:10.4088/jcp.v63n0206
21. Judd LL, Schettler PJ, Solomon DA, et al. Psychosocial disability and work role function compared across the long-term course of bipolar I, bipolar II and unipolar major depressive disorders. J Affect Disord. 2008;108(1–2):49–58. doi:10.1016/j.jad.2007.06.014
22. Dickerson FB, Boronow JJ, Stallings CR, Origoni AE, Cole S, Yolken RH. Association between cognitive functioning and employment status of persons with bipolar disorder. Psychiatr Serv. 2004;55(1):54–58. doi:10.1176/appi.ps.55.1.54
23. Huxley N, Baldessarini RJ. Disability and its treatment in bipolar disorder patients. Bipolar Disord. 2007;9(1–2):183–196. doi:10.1111/j.1399-5618.2007.00430.x
24. Zimmerman M, Galione JN, Chelminski I, Young D, Dalrymple K, Ruggero CJ. Sustained unemployment in psychiatric outpatients with bipolar disorder: frequency and association with demographic variables and comorbid disorders. Bipolar Disord. 2010;12(7):720–726. doi:10.1111/j.1399-5618.2010.00869.x
25. Reed C, Goetz I, Vieta E, Bassi M, Haro JM. EMBLEM Advisory Board. Work impairment in bipolar disorder patients—results from a two-year observational study (EMBLEM). Eur Psychiatry. 2010;25(6):338–344. doi:10.1016/j.eurpsy.2010.01.001
26. Bonnín CM, Martínez-Arán A, Torrent C, et al. Clinical and neurocognitive predictors of functional outcome in bipolar euthymic patients: a long-term, follow-up study. J Affect Disord. 2010;121(1–2):156–160. doi:10.1016/j.jad.2009.05.014
27. Tohen M, Hennen J, Zarate CM
28. Burdick KE, Goldberg JF, Harrow M. Neurocognitive dysfunction and psychosocial outcome in patients with bipolar I disorder at 15-year follow-up. Acta Psychiatr Scand. 2010;122(6):499–506. doi:10.1111/j.1600-0447.2010.01590.x
29. Hower H, Lee EJ, Jones RN, et al. Predictors of longitudinal psychosocial functioning in bipolar youth transitioning to adults. J Affect Disord. 2019;246:578–585. doi:10.1016/j.jad.2018.12.108
30. Perlis RH, Dennehy EB, Miklowitz DJ, et al. Retrospective age at onset of bipolar disorder and outcome during two-year follow-up: results from the STEP-BD study. Bipolar Disord. 2009;11(4):391–400. doi:10.1111/j.1399-5618.2009.00686.x
31. Drakopoulos J, Sparding T, Clements C, Pålsson E, Landén M. Executive functioning but not IQ or illness severity predicts occupational status in bipolar disorder. Int J Bipolar Disord. 2020;8(1):7. doi:10.1186/s40345-019-0168-6
32. Nivoli AMA, Pacchiarotti I, Rosa AR, et al. Gender differences in a cohort study of 604 bipolar patients: the role of predominant polarity. J Affect Disord. 2011;133(3):443–449. doi:10.1016/j.jad.2011.04.055
33. Erol A, Winham SJ, McElroy SL, et al. Sex differences in the risk of rapid cycling and other indicators of adverse illness course in patients with bipolar I and II disorder. Bipolar Disord. 2015;17(6):670–676. doi:10.1111/bdi.12329
34. Tse S, Chan S, Ng KL, Yatham LN. Meta-analysis of predictors of favorable employment outcomes among individuals with bipolar disorder. Bipolar Disord. 2014;16(3):217–229. doi:10.1111/bdi.12148
35. Gilbert E, Marwaha S. Predictors of employment in bipolar disorder: a systematic review. J Affect Disord. 2013;145(2):156–164. doi:10.1016/j.jad.2012.07.009
36. Ministry of Health, Labor and Welfare. Summary of the 2019 employment trends survey results. Available from: https://www.mhlw.go.jp/toukei/itiran/roudou/koyou/doukou/20-2/dl/kekka_gaiyo-01.pdf.
37. Duarte W, Becerra R, Cruise K. The relationship between neurocognitive functioning and occupational functioning in bipolar disorder: a literature review. Eur J Psychol. 2016;12(4):659–678. doi:10.5964/ejop.v12i4.909
38. Bowie CR, Depp C, McGrath JA, et al. Prediction of real-world functional disability in chronic mental disorders: a comparison of schizophrenia and bipolar disorder. Am J Psychiatry. 2010;167(9):1116–1124. doi:10.1176/appi.ajp.2010.09101406
39. Simon GE, Ludman EJ, Unützer J, Operskalski BH, Bauer MS. Severity of mood symptoms and work productivity in people treated for bipolar disorder. Bipolar Disord. 2008;10(6):718–725. doi:10.1111/j.1399-5618.2008.00581.x
40. Salyers MP, Becker DR, Drake RE, Torrey WC, Wyzik PF. A ten-year follow-up of a supported employment program. Psychiatr Serv. 2004;55(3):302–308. doi:10.1176/appi.ps.55.3.302
41. Becker D, Whitley R, Bailey EL, Drake RE. Long-term employment trajectories among participants with severe mental illness in supported employment. Psychiatr Serv. 2007;58(7):922–928. doi:10.1176/ps.2007.58.7.922
42. Luciano A, Metcalfe JD, Bond GR, et al. Hospitalization risk before and after employment among adults with schizophrenia, bipolar disorder, or major depression. Psychiatr Serv. 2016;67(10):1131–1138. doi:10.1176/appi.ps.201500343
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.