")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 11
Relationship between early menarche, obesity, and disordered eating behaviors: a school-based cross-sectional survey in Northern Saudi Arabia
Authors Almuhlafi M, Abu Jamilah K, Almutairi AF , Salam M
Received 18 July 2018
Accepted for publication 14 September 2018
Published 15 November 2018 Volume 2018:11 Pages 743—751
DOI https://doi.org/10.2147/DMSO.S180697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Mashael Almuhlafi,1 Khalil Abu Jamilah,1 Adel F Almutairi,2 Mahmoud Salam2
1Department of Family Medicine, North West Armed Forces Hospital, Tabuk, Saudi Arabia; 2Science and Technology Unit, King Abdullah International Medical Research Center, King Saud Bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia
Background: Obesity and disordered eating (DE) behaviors are serious health concerns, regularly observed among female adolescents, which could progress to adverse psychological and nutritional sequels.
Aim: The aim of this study was to determine the prevalence of obesity and the self-reported DE behaviors among high school female students and to evaluate their self-perception of body image, peer pressures, and need for dietary consultation.
Methods: This is a school-based cross-sectional study conducted in 2018. Self-administered surveys and anthropometric measurements were obtained from adolescent females, randomly selected from eight schools in northern Saudi Arabia. Sample characteristics were age, menarche, and DE behaviors (binge eating, self-induced vomiting, and usage of laxatives). Body mass index was converted to percentiles using the age-to-gender scale. Self-perception of body image, perceived peer pressures, and the Eating Attitude Test-26 (EAT-26) were scored, summated, and then presented in percentage mean scores (PMSs) and mean scores (MSs).
Results: Sample comprised 399 participants. One hundred twenty-eight (32.1%) participants reported early age of menarche (≤12 years). Sixty-five (16.3%) participants reported the prevalence of overweight/obesity, 123 (30.8%) participants reported binge eating, 28 (7.0%) participants reported self-induced vomiting, and 21 (5.3%) participants reported usage of laxatives. The PMS of self-perception of body weight and peer pressure was 68.7±27.1 and 41.9±23.5, respectively. One hundred ninety-two (48.1%) participants needed professional dietary help. Students with early age of menarche were 1.7 times more likely to be overweight/obese (adjusted [adj] P=0.018) compared to others. Overweight/obese participants had significantly poorer self-perception of body image (PMS =47.4±25.0) and higher perceived peer pressure (PMS =49.5±23.1) compared to underweight/normal weight students (PMS =72.8±25.6 [P<0.001] and PMS =40.5±23.3 [P=0.005], respectively). Participants with early age of menarche complained of higher perceived peer pressure compared to others (P=0.045). Participants with DE behaviors had higher peer pressure (PMS =46.8±23.5) and higher scores on E-26 (MS =22.2±11.4) compared to their counter groups (P=0.002 and 0.016, respectively).
Conclusion: The high rate of overweight/obesity and DE behaviors among female adolescents is alarming. Special consideration should be made for those with early menarche who were more prone to overweight/obesity.
Keywords: adolescent, peer, E-26, body image, binge, self-induced vomiting
Background
Disturbed eating behaviors involve various abnormal eating patterns or attitudes, such as binge eating (uncontrolled eating), self-induced vomiting (purging), chronic restrained eating, and usage of dietary pills.1 Disordered eating (DE) behaviors might lead to adverse psychological and medical sequels.2 If untreated disturbed eating behaviors might progress to more serious eating disorders such as anorexia nervosa and bulimia nervosa.3 Eating disorders are severe psychiatric conditions diagnosed by clinical experts based on a set of criteria, mainly the Diagnostic and Statistical Manual of Mental Disorders (DSM V tool).4 People with DE behaviors regularly report irregular or chaotic eating patterns, ignoring physical feelings of hunger and satiety, and/or emotional eating.5 Two prominent consequences of these behaviors include body image disturbance and dissatisfaction.2
Various risk factors leading to a disturbance in eating behaviors were identified in the literature, such as depression and social stressors.2 For instance, the desire to achieve an ideal body shape is the most prominent factor associated with DE behaviors.6 Adolescent females are more prone to DE behaviors than males or other age groups. In fact, these behaviors are considered to be the most prevalent health problem next to obesity among adolescent females.5 This is probably attributed to changes in the lifestyle of adolescent girls, which affect their eating behaviors. DE behaviors usually exist during adolescence as a result of the physical changes during puberty when females experience a gain in body fat.7 Media, peers, athletes, and parents are the most influential sociocultural factors that could act as determinants of body image disturbances. These factors impact body satisfaction through two mechanisms that are the social comparison and ideal body internalization.8 The emphasis of family on body shape, beauty, and lifestyle could lead to DE behaviors among young females in particular.9 Also, media plays a great role in body dissatisfaction as exposure to the ideal body form of celebrities can change personal body image perception in females.10,11 Even parents who had DE behaviors had a negative influence on their children who were reported to be at much higher risk than those with parents without DE habits.1
Early recognition of disturbed eating disorders can aid in the prevention of severe psychiatric forms of eating disorders, as a large number of young females may experiment with inappropriate weight loss measures.12 Disturbed eating behaviors were previously reported among Western females2; yet over the recent decades, this phenomenon has been increasing in the Middle Eastern communities as well.13 Some studies have been carried out in Arabian countries. For example, one study has reported that DE attitudes have been observed among university students in Kuwait and that they were particularly higher among females and obese groups.13
All in all, obesity and disturbed eating behaviors are serious yet can be prevented or resolved if detected at early stages. Female adolescents are, in particular, considered to be at higher risk to develop such disrupted eating patterns. Seldom studies have addressed disturbed eating behaviors in Arabian countries in general and in Saudi Arabia in specific. The true prevalence of disturbed eating behaviors in conservative communities such as in Saudi Arabia could be underreported. Therefore, the aim of this study was to assess the prevalence and associated factors of both obesity and disturbed eating behaviors among high school female students in Saudi Arabia. This study also evaluated their perception toward their body image and peer pressures and identified their need for professional dietary consultation.
Methods
Study design and setting
During the academic year 2017–2018, a cross-sectional study, based on self-administered anonymous surveys and anthropometric measurements, was conducted in the city of Tabuk, northern Saudi Arabia. Tabuk is situated 2,200 ft above sea level and characterized by a moderate climate compared to other Saudi cities, with a population of 970,694 according to a 2015 census.14 The city has 34 high schools dedicated for female students, of which 28 schools are public and 6 schools are private, capable of accommodating 6,047 students each academic year. The study sought its ethical approval from the Research Ethics Committee at the Armed Forces Hospitals in Northwestern Region, Saudi Arabia (R&REC 2018-219) and its administrative approvals from the educational authorities at the targeted schools.
Subjects and sampling technique
The estimated precalculated sample size was set at 220 students, based on a speculated prevalence of obesity 16%,15 a 5% margin of error, and a 95% CI and a 10% compensatory increase to overcome incomplete surveys. Eight randomly selected schools were drawn out from a pool of 34 schools, and then, one class was randomly selected from each academic level from each of these schools (first, second, and third secondary levels). Twenty students were invited to participate from each class. Eligible study participants were female registered students at the targeted schools who were willing to enroll in this study and signed an assent form. Prior to their participation, students handed their parents a self-explanatory letter and an informed consent indicating their approval on the enrollment of their daughters in this study. The study was observational in nature as no new equipment was tested.
Data collection and management
The data collection was executed by the study investigators in collaboration with school nurses assigned at the targeted schools. The components of the data collection forms included an assessment of the sample characteristics such as age and menarche age (years). Age of menarche was recalled by students to the nearest year. The history of DE behaviors focused on the students’ current indulgence in three unhealthy habits, such as binge eating, self-induced vomiting (purging), and usage of laxatives. The operational definitions of these behaviors were described in the introductory letter of the survey. The anthropometric body measurements, height (cm) and weight (kg), were obtained using the same brand of scales available at the setting. The electronic weight scales were previously calibrated and quality checked prior data collection. Height and weight were converted into percentiles of body mass index (BMI) for females, an age–gender-specific converting scale for females aged between 2 and 20 years. This scale was developed by the National Center for Health Statistics in collaboration with the National Center for Chronic Disease Prevention and Health Promotion.16 Students with <5th percentile were accounted as underweight, students with 5th–84th percentile were accounted as normal weight, students with 85th–94th percentile were accounted as overweight, and students with ≥95th were accounted as obese.
The self-perception of body image (three statements) questioned participants about their satisfaction with their body weight, shape, and size as well as a measured their self-confidence regarding their outer appearance. The perceived peer pressures (four statements) questioned participants about themselves being compared to slimmer persons and whether they were pressured to become slimmer. This domain also questioned participants if the media and the fashion designs/modeling industry had influenced them to lose weight. The two domains were developed by the study investigators and, then, revised by an expert in social science studies who recommended some modifications. The self-perception of body image and the perceived peer pressures domains were translated to Arabic and, then, back translated to English with minimal variations observed. The Arabic version of Eating Attitude Test-26 (EAT-26) encompassed 26 statements rated on a 5-point Likert scale. Originally created in 1982, the EAT-26 has been widely used to determine if a participant complains of disturbed eating behaviors and needs professional attention. However, EAT-26 is not designed to make a clinical diagnosis of an eating disorder or to take the place of a professional dietary diagnosis or consultation.17 The Cronbach’s alpha for the self-body image perception, peer pressure perception, and E-26 was 0.77, 0.56, and 0.75, respectively.
The SPSS (version 25) was used for data entry and analysis. Categorical measures such as the prevalence of weight categories were expressed in frequencies and percentages (n [%]), whereas continuous variables such as scores were presented in mean ± SD. The RR of obesity across the sample characteristics was calculated. Binary logistic regression analysis was performed to control for any confounding effect, so the adjusted (adj) OR and its 95% CI were obtained. The perception of self-body image and peer pressures, as well as E-26, were scored and summated and, then, presented in percentage mean scores (PMSs) and mean scores (MSs), respectively. Higher scores of self-body image perception indicated better perception, whereas higher PMS of peer pressure scores indicated a more peer pressure. Students scoring on E-26 (≥20) were accounted as in need for consultation by a professional dietitian. Categorical outcomes were tested using Pearson’s chi-square (χ2) test. Normally distributed continuous outcomes (perceived peer pressure) were tested across sample characteristics using Student’s t-test, whereas nonnormally distributed data (self-perception of body image and E-26) were tested using Mann–Whitney test (Z). Statistical significance was set at P<0.05, and the Hedges’ g was presented as a measure of the effect size weighted according to the relative size of statistically significant subgroups.
Ethics approval and consent to participate
A self-explanatory letter of invitation to participate was handed to both the students and their parents. Parents signed informed consent forms, whereas their daughters signed assent forms. The study sought its ethical approval from the Research Ethics Committee at the Armed Forces Hospitals in Northwestern Region, Saudi Arabia (R&REC 2018-219), and its administrative approvals from the educational authorities at the targeted schools. This study followed the recommendations of the International Conference on Harmonization for Good Clinical Practice (ICH-GCP) and Declaration of Helsinki.
Results
Sample and outcome characteristics
A total of 480 female high school students were invited to enroll in this study, of whom 399 (83.1%) students agreed to participate. Their mean age was 16.8±0.9 years, of whom 147 (36.8%) students were ≤16 years old and 252 (63.2%) students were >16 years old. One hundred and twenty-eight (32.1%) participants reported menarche at ≤12 years, whereas 271 (67.9%) participants reported it at >12 years, with a mean ± SD of menarche age 13±1.3 years. Thirty-seven (9.3%) students were underweight, whereas 297 (74.4%) students were normal weight. Sixty-five (16.3%) students reported the prevalence of overweight/obese. One hundred twenty-three (30.8%) students reported binge eating, 28 (7.0%) students reported purging, and 21 (5.3%) students reported usage of laxatives in (Table 1).
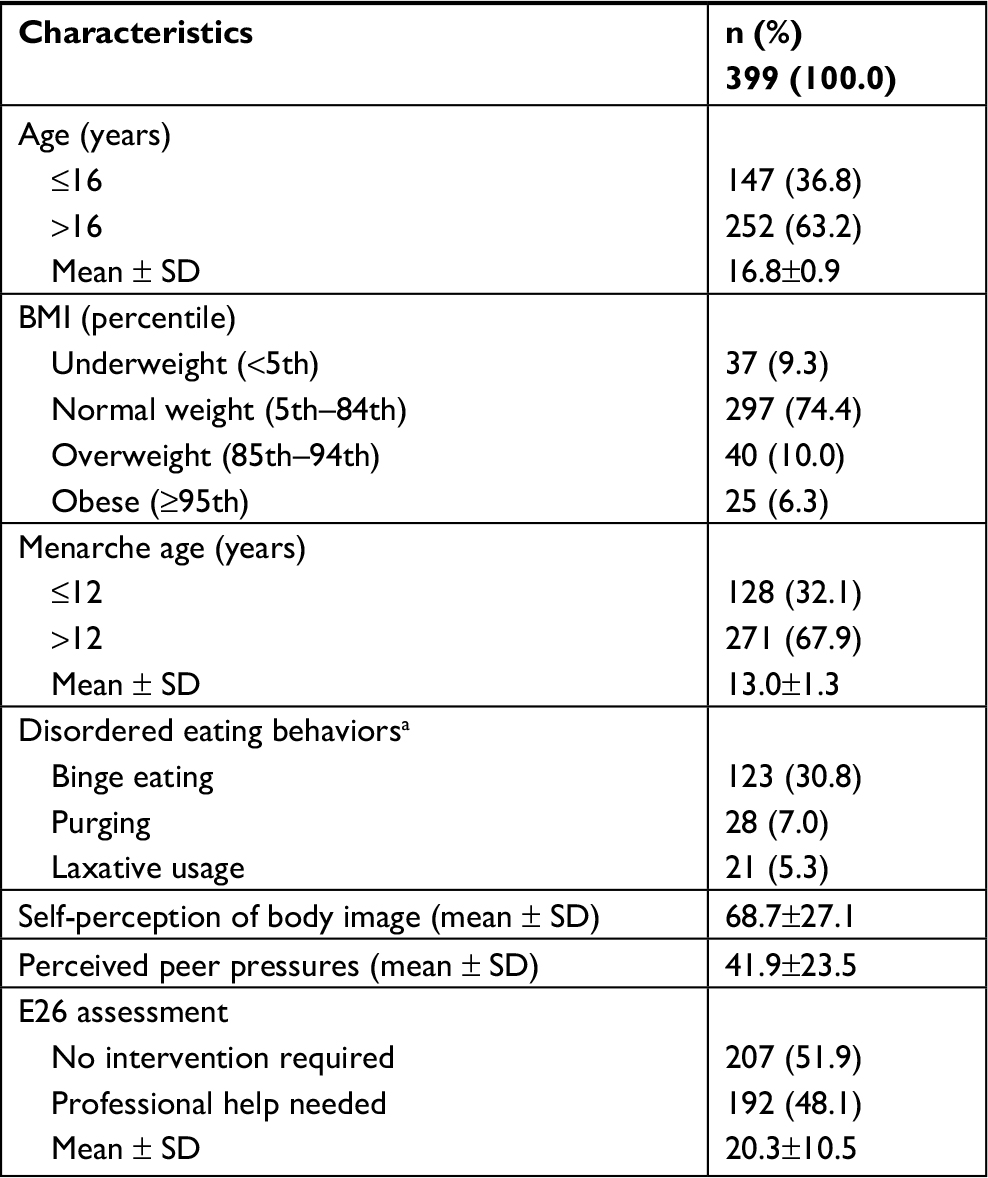 | Table 1 Student and outcome characteristics Note: aMutually exclusive. Abbreviation: BMI, body mass index. |
The frequency of responses is presented in Tables 2 and 3. The PMS of self-perception of body weight was 68.7±27.1, whereas the perceived peer pressure was 41.9±23.5. The MS of E-26 domain was 20.3±10.5, with 192 (48.1%) students who were probably in need for professional dietary help and 207 (51.9%) students who were probably not in need for help.
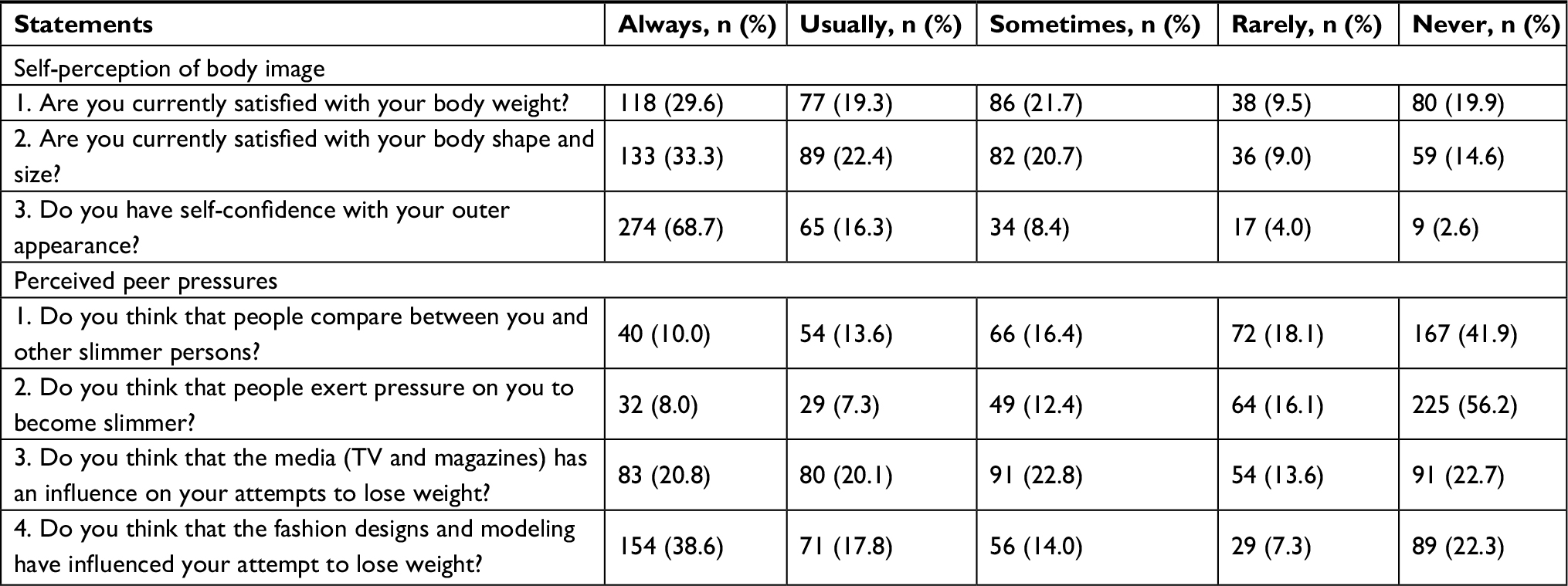 | Table 2 Responses to the self-perception and perceived peer pressure statements Note: n, frequency. |
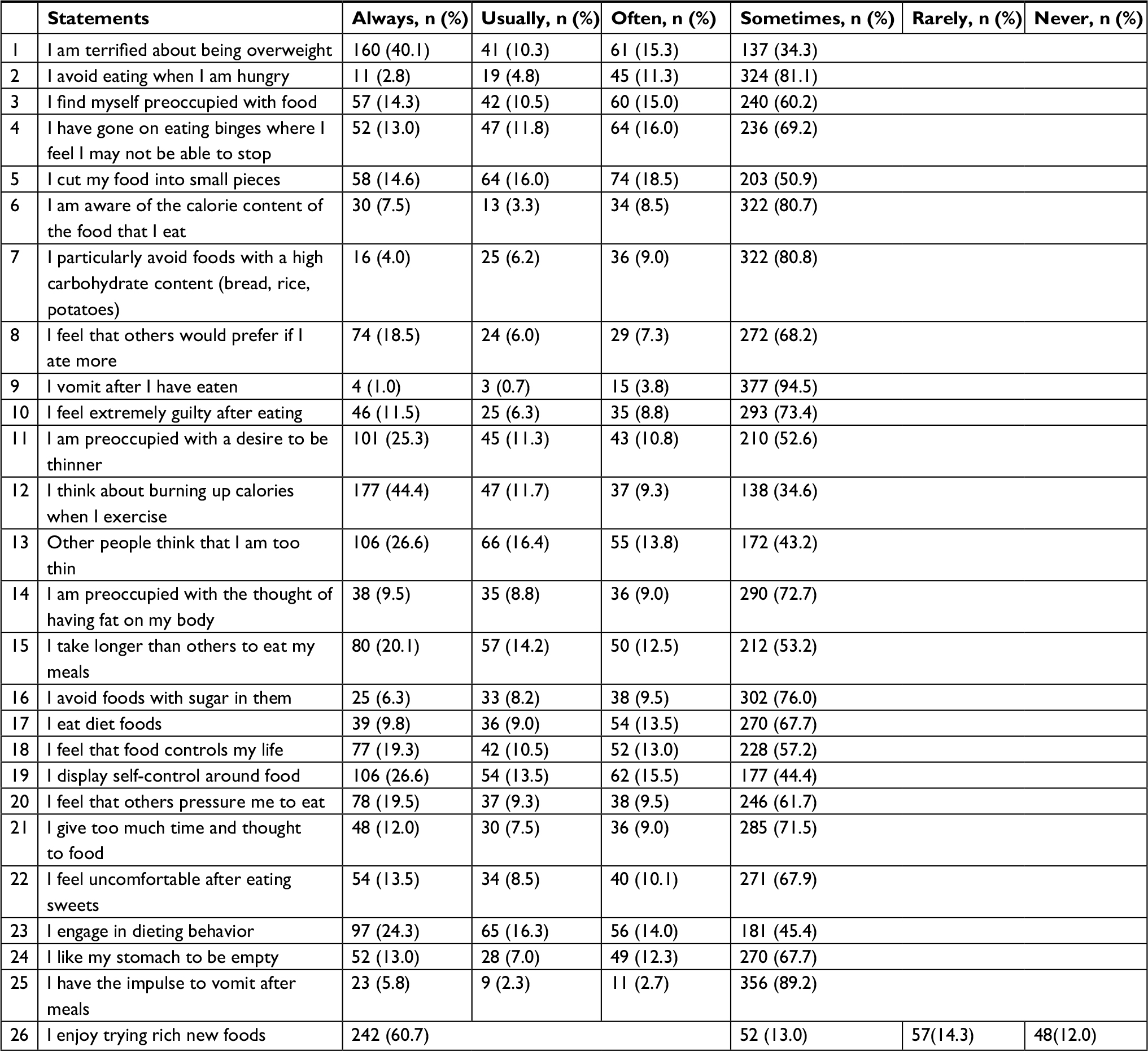 | Table 3 Responses to the E26 statements Note: n, frequency. |
Factors associated with outcomes
Bivariate analysis showed that overweight/obesity was more prevalent among high school students with the age of menarche of ≤12 years (RR =1.7 [1.1–2.7]) compared to those with the age of menarche >12 years (P=0.018). A binary logistic regression analysis also showed that students with the age of menarche of ≤12 years were 1.9 times more likely to be overweight/obesity (adj P=0.018) (Table 4).
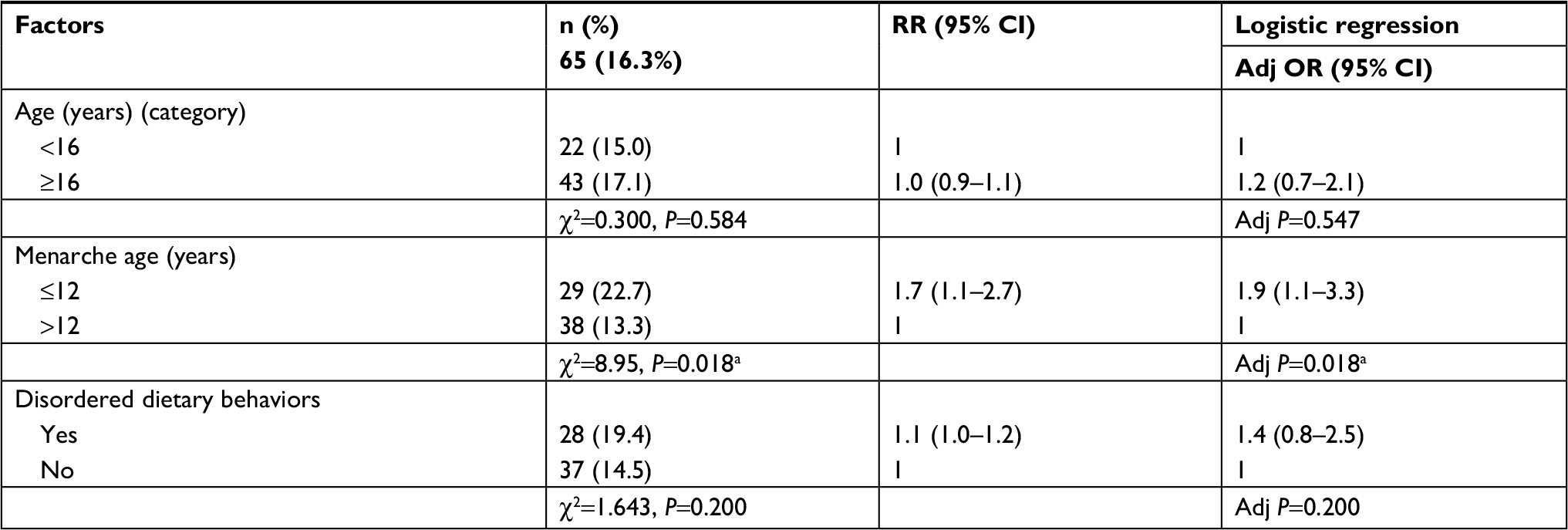 | Table 4 Prevalence of overweight/obesity and its associated factors Notes: n, frequency; χ2, Pearson’s chi-square. aStatistically significant at <0.05. Abbreviation: adj, adjusted. |
Overweight/obese high school students had significantly lower scores of self-perception of body image (PMS =47.4±25.0) and higher scores of perceived peer pressure (PMS =49.5±23.1) compared to nonobese students (PMS =72.8±25.6 [P<0.001] and PMS =40.5±23.3 [P=0.005], respectively). Students with the age of menarche of ≤12 years complained of higher perceived peer pressure scores compared to those with the age of menarche of >12 years (P=0.045). Students who had disordered dietary behaviors (binge eating, purging, and/or usage of laxatives) had higher peer pressure scores (PMS =46.8±23.5) and higher scores on E-26 (MS =22.2±11.4) compared to their counter groups (P=0.002 and 0.016, respectively) (Table 5).
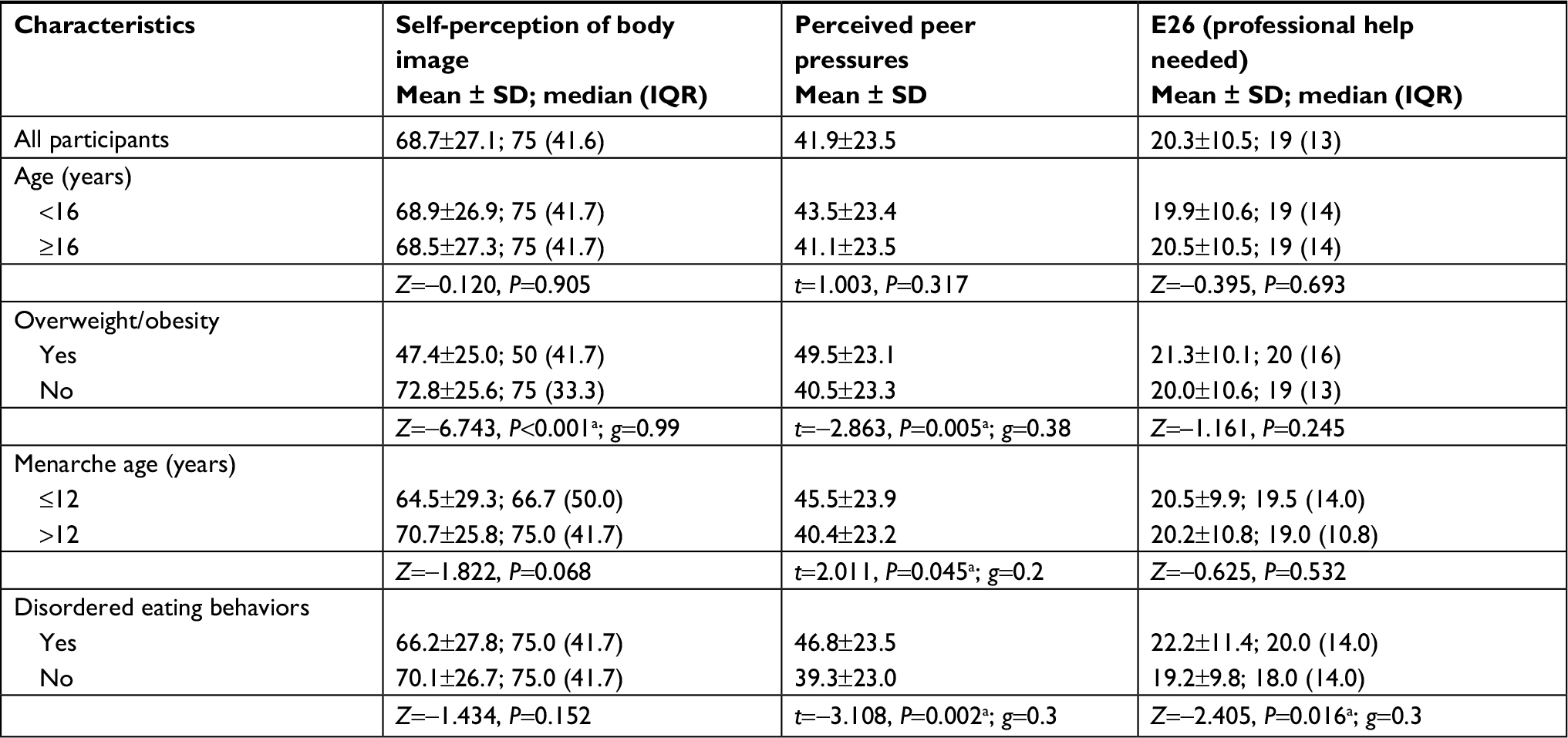 | Table 5 Self-perception of body image, perceived peer pressure, and E26 scores across sample characteristics Notes: Z, Mann–Whitney test Z-score; g, Hedges’ g; t, Student’s t-test. aP-value: statistically significant at <0.05. Abbreviations: MS, mean score; PMS, percentage mean scores. |
Discussion
Battling obesity and overweight has to be one of the toughest challenges for any person, but it must be especially difficult for those in their adolescence years. The findings of the current study indicate that 16.3% of Saudi Arabian high school girls are obese or overweight. This is not surprising, since a recent study reported an even higher percentage of overweight (26.6%), obesity (10.6%), and severe obesity (2.4%) among Saudi Arabian adolescents (13–18 years) in comparison to younger school-age children.18,19 Another recent study found an almost similar percentage for overweight (11.7%) and obesity (7.8%) among Saudi high school girls.15 Females at this transitional stage (between teenage and adulthood) experience a wide array of changes, including changes to their physical appearance, hormonal levels, and social relationships. This is the stage where friendships advance and adolescents may engage in risky behaviors to prove themselves or to seek attention. Peers at this stage of life may be supportive and caring, whereas some peers may pressure adolescents to experiment with unhealthy habits, such as DE behaviors. A female at this stage has also started to build her identity, yet her parent’s expectations regarding her fitness may become potential stressors. Therefore, it is no wonder that females at such a confusing life stage are prone to DE behaviors and obesity.
This study revealed that overweight and obese females had a more negative body image compared to normal-weight females. Negative body image can damage an individual’s psychological welfare, especially in females, as indicated in a study conducted in Hungary.20 In a South African study, those adolescents who perceived their body size as normal reported to feel high levels of respect, satisfaction, and happiness, whereas those who perceived themselves as obese felt the opposite.21 A study conducted among college-age females in south-western Saudi Arabia reported that almost 44% wanted to become thinner, whereas 19.7% wanted to become heavier due to their perceived body image.22 This willingness to change their body image, in combination with the lack of awareness of proper dieting, can lead to experimenting with and/or adopting DE behaviors. Being dissatisfied with body size has been associated with unhealthy weight control behaviors.23 A systematic review concluded that one of the strong correlations with unhealthy weight loss measures was the females’ personal concerns with their body weight.24
Losing weight is a common goal among teenagers, which puts them at risk of adopting unhealthy dietary behaviors, such as self-induced vomiting and usage of laxatives.25 This study found that almost 12% of female students admitted to purging and usage of laxative. These kinds of unhealthy methods of weight control were reported to be more prevalent among North American and Spanish adolescent girls, specifically among those who are overweight and obese.26 In a similar context, one Kuwaiti study reported that the prevalence of DE behaviors was 31.8% and 33.6% among men and women, respectively.13 Another study found that obesity was associated with unhealthy weight control behaviors (such as diet pills and self-induced vomiting) among both genders in the USA.23,27 Among adolescents from seven Arabian countries, the risk of DE attitudes was twice as high among obese females as in males.28 It is speculated that adolescents may not be fully aware of certain DE behaviors – meaning that because of their young age, they have not yet taken responsibility for their general health, diet, physical activity, and lifestyle.
This study also found that DE behaviors were more prevalent among girls who had higher perceived peer pressure, and they also had higher scores on the eating attitude scale than others. For female adolescents, peers are mainly their colleagues of the same gender and age group. Peer pressure can be exhibited by idealizing peers who have normal weight, by experiencing pressure from peers with normal weight, or even by bullying.27 One American study reported that overweight teenagers were referred to by their classmates and teachers as being more socially withdrawn and less physically attractive.29 Internalization of being thin as an ideal body image due to watching TV programs makes girls more likely to suffer from DE behaviors.11 The ideal body shape in Western countries, in terms of slimness among females and muscularity among males, has also spread to other communities,21 including Saudi Arabia. Another form of peer pressure is parental misperceptions of their own children’s weight, as parents usually compare their youngsters’ weight with that of their friends and relatives.30 Canadian females, who complained of weight teasing from their families, were found to have DE behaviors.31
Menarche is observed among female children as a transition point into adulthood – a life stage accompanied with a series of biological and psychological changes. In this study, overweight and obesity were more prevalent among high school students with the menarche age of ≤12 years and with higher perceived peer pressure scores compared to those with the menarche age of >12 years. The relationship between early menarche, DE behaviors, and overweight was observed in an Iranian study, in which they found that high school females whose menarche age was less than 11 years had DE attitude.32 In the USA, adolescent girls who experienced menarche at earlier ages tended to suffer from higher rates of negative body image than their peers.33,34 The social expectations of weight and body image toward early menarche females are usually acquired from their peers (family, friends, and the media). These expectations are actual stressors on young females who often find them difficult to overcome, often because they do not have the sufficient cognitive and emotional maturity to respond to such parental and peer expectations.35
Limitations
Few limitations have been encountered in this study. Although multiple schools have been randomly selected and the sample size was statistically convenient, all participants were recruited within the same region of Saudi Arabia. This might have limited its generalizability to other regions, yet screening for overweight/obesity and DE behaviors can be replicated to schools in other regions. A slight chance of recall bias is expected with such retrospective studies, such as the reporting of menarche age, yet students are expected to be accurate in reporting such an important developmental milestone. Though weight and height measurement scales were unified, yet ±1–3 cm in height and ±1 kg of weight were expected due to the standing posture and clothing of students, as well as the data collectors’ skills. This was overcome by the BMI percentile ranges when converting them into weight categories. Although the assessment of self-perception of body image and perceived peer pressure statements were not previously utilized in previous studies, their inter-rater reliability indicated good internal consistency.
Conclusion
The doctor in psychology Dr Jane Mendle once stated, “As children develop physically, it changes how they think about themselves and how people relate to them socially.” This makes the transformation of females during puberty not only limited to their physical appearance. Girls often picture binge eating, purging, and usage of laxatives as an easy way to remain slim. Little do they know that getting indulged in DE behaviors eventually requires professional dietary consultation and corrective actions. The high rate of obesity and DE behaviors among female adolescents in this setting is alarming, as it can progress to a sequel of health disorders. Special consideration should be made for those with early menarche who were more prone to overweight/obesity.
Routine screening of weight and DE behaviors is highly recommended among school children of various ages. Preventing a gain in weight remains much easier than losing weight, so early detection of overweight and initiation of healthy dietary plans are of great importance. Identifying warning signs of peer pressure or bullying among overweight/obese adolescents needs to be dealt with by professionals too. All in all, it is the duty of school administrators to ensure that their students are well aware of the risks of obesity and its consequences.
Data sharing statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
This study was approved by the Armed Forces Hospitals in Northwestern Region, Tabuk, and in collaboration with King Abdullah International Medical Research Center, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia. Special thanks go to the research coordinator Mrs Khadija Al-Qarni and the school administrators for their tremendous support in making this project a success.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Goebel-Fabbri AE. Disturbed eating behaviors and eating disorders in type 1 diabetes: clinical significance and treatment recommendations. Curr Diab Rep. 2009;9(2):133–139. | ||
Schuck K, Munsch S, Schneider S. Body image perceptions and symptoms of disturbed eating behavior among children and adolescents in Germany. Child Adolesc Psychiatry Ment Health. 2018;12(1):10. | ||
Toni G, Berioli M, Cerquiglini L, et al. Eating Disorders and disorders and disordered eating symptoms in adolescents with type 1 diabetes. Nutrients. 2017;9(8):906. | ||
Micali N, Ploubidis G, De Stavola B, Simonoff E, Treasure J. Frequency and patterns of eating disorder symptoms in early adolescence. J Adolesc Health. 2014;54(5):574–581. | ||
Yu Z, Tan M. Disordered eating behaviors and food addiction among nutrition major college students. Nutrients. 2016;8(11):673. | ||
Hogan MJ, Strasburger VC. Body image, eating disorders, and the media. Adolesc Med State Art Rev. 2008;19(3):521–546. | ||
Todd AS, Street SJ, Ziviani J, Byrne NM, Hills AP. Overweight and obese adolescent girls: the importance of promoting sensible eating and activity behaviors from the start of the adolescent period. Int J Environ Res Public Health. 2015;12(2):2306–2329. | ||
Garrusi B, Baneshi MR. Eating disorders and their associated risk factors among Iranian population; a community based study. Glob J Health Sci. 2012;5(1):193–202. | ||
Kluck AS. Family influence on disordered eating: the role of body image dissatisfaction. Body Image. 2010;7(1):8–14. | ||
Thomas J, Khan S, Abdulrahman AA. Eating attitudes and body image concerns among female university students in the United Arab Emirates. Appetite. 2010;54(3):595–598. | ||
Martin JB. The development of ideal body image perceptions in the United States. Nutr Today. 2010;45(3):98–110. | ||
Senekal M, Lasker GL, van Velden L, Laubscher R, Temple NJ. Weight-loss strategies of South African female university students and comparison of weight management-related characteristics between dieters and non-dieters. BMC Public Health. 2016;16(1):918. | ||
Baker JH, Thornton LM, Lichtenstein P, Bulik CM. Pubertal development predicts eating behaviors in adolescence. Int J Eat Disord. 2012;45(7):819–826. | ||
Wikipedia [webpage on the Internet]. Tabuk, Saudi Arabia. Available from: https://en. wikipedia.org/wiki/Tabuk,_Saudi_Arabia. Accessed August, 2017. | ||
Allihaibi MM. Disordered eating attitude among secondary schoolgirls at Al-Iskan sector. Makkah Almukarramah. 2015;4(7):939–945. | ||
Jafari S, Fouladgar M, Naeeni MM, et al. Body mass index, weight-forage, and stature-for-age indices in Iranian School Children in relation to weight and growth disorders: a population-based survey. Int J Prev Med. 2014;5(Suppl 2):S133. | ||
Garner DM, Olmsted MP, Bohr Y, Garfinkel PE. The eating attitudes test: psychometric features and clinical correlates. Psychol Med. 1982;12(4):871–878. | ||
El Mouzan MI, Foster PJ, Al Herbish AS, et al. Prevalence of overweight and obesity in Saudi children and adolescents. Ann Saudi Med. 2010;30(3):203. | ||
Al Qauhiz NM, Nq A. Obesity among Saudi Female University Students: Dietary Habits and Health Behaviors. J Egypt Public Health Assoc. 2010;85(1–2):45–59. | ||
Papp I, Urbán R, Czeglédi E, Babusa B, Túry F. Testing the Tripartite Influence Model of body image and eating disturbance among Hungarian adolescents. Body Image. 2013;10(2):232–242. | ||
Gitau TM, Micklesfield LK, Pettifor JM, Norris SA. Changes in eating attitudes, body esteem and weight control behaviours during adolescence in a South African cohort. PLoS One. 2014;9(10):e109709. | ||
Khalaf A, Westergren A, Berggren V, Ekblom Ö, Al-Hazzaa HM. Perceived and ideal body image in young women in South Western Saudi Arabia. J Obes. 2015;2015:1–7. | ||
Vander Wal JS. Unhealthy weight control behaviors among adolescents. J Health Psychol. 2012;17(1):110–120. | ||
Haynes A, Kersbergen I, Sutin A, Daly M, Robinson E. A systematic review of the relationship between weight status perceptions and weight loss attempts, strategies, behaviours and outcomes. Obes Rev. 2018;19(3):347–363. | ||
Brown CL, Skelton JA, Perrin EM, Skinner AC. Behaviors and motivations for weight loss in children and adolescents. Obesity. 2016;24(2):446–452. | ||
López-Guimerà G, Neumark-Sztainer D, Hannan P, Fauquet J, Loth K, Sánchez-Carracedo D. Unhealthy weight-control behaviours, dieting and weight status: a cross-cultural comparison between North American and Spanish adolescents. Eur Eat Disord Rev. 2013;21(4):276–283. | ||
Vander Wal JS. The relationship between body mass index and unhealthy weight control behaviors among adolescents: the role of family and peer social support. Econ Hum Biol. 2012;10(4):395–404. | ||
Musaiger AO, Al-Mannai M, Tayyem R, et al. Risk of disordered eating attitudes among adolescents in seven Arab countries by gender and obesity: a cross-cultural study. Appetite. 2013;60(1):162–167. | ||
Zeller MH, Reiter-Purtill J, Ramey C. Negative peer perceptions of obese children in the classroom environment. Obesity. 2008;16(4):755–762. | ||
Gwozdz W, Sousa-Poza A, Reisch LA, et al. Peer effects on obesity in a sample of European children. Econ Hum Biol. 2015;18:139–152. | ||
Goldfield G, Moore C, Henderson K, Buchholz A, Obeid N, Flament M. The relation between weight-based teasing and psychological adjustment in adolescents. Paediatr Child Health. 2010;15(5):283–288. | ||
Pourghassem Gargari B, Kooshavar D, Seyed Sajadi N, Safoura S, Hamed Behzad M, Shahrokhi H. Disordered eating attitudes and their correlates among Iranian High School girls. Health Promot Perspect. 2011;1(1):41–49. | ||
Copeland W, Shanahan L, Miller S, Costello EJ, Angold A, Maughan B. Outcomes of early pubertal timing in young women: a prospective population-based study. Am J Psychiatry. 2010;167(10):1218–1225. | ||
Jean RT, Wilkinson AV, Spitz MR, Prokhorov A, Bondy M, Forman MR. Psychosocial risk and correlates of early menarche in Mexican-American girls. Am J Epidemiol. 2011;173(10):1203–1210. | ||
Vaughan EB, Van Hulle CA, Beasley WH, Rodgers JL, D’Onofrio BM. Clarifying the associations between age at menarche and adolescent emotional and behavioral problems. J Youth Adolesc. 2015;44(4):922–939. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.