")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Relating Medical Errors to Medical Specialties: A Mixed Analysis Based on Litigation Documents and Qualitative Data
Authors Liu J, Liu P , Gong X, Liang F
Received 17 January 2020
Accepted for publication 25 March 2020
Published 20 April 2020 Volume 2020:13 Pages 335—345
DOI https://doi.org/10.2147/RMHP.S246452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Junqiang Liu,1,2 Paicheng Liu,1 Xue Gong,1 Fengbo Liang1
1School of Government, Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Center for Chinese Public Administration Research, Sun Yat-sen University, Guangzhou, People’s Republic of China
Correspondence: Junqiang Liu
School of Government, Sun Yat-sen University, No. 135, Xingang Xi Road, Guangzhou, People’s Republic of China
Tel +86 20-84111433
Email [email protected]
Paicheng Liu
School of Government, Sun Yat-sen University, No. 135, Xingang Xi Road, Guangzhou, People’s Republic of China
Tel +86 18580008701
Email [email protected]
Background: We know a great deal about types, causes, and prevention of medical errors, as well as the risks of each medical specialties. Although we know something about medical errors, much remains to be done in this area particularly around effective prevention. However, little is known about whether medical errors are related to medical specialties. Our objective was to categorize and map the distribution of medical errors and analyze their relationships with medical specialties.
Methods: First, public cases of medical disputes were searched on “China Judgment Online” according to the key words including medical errors. Second, we set up a database with 5237 medical litigations. After removing unrelated judgment documents, we used systematic random sampling to extract half of these. Then, we hired two frontline physicians with M.D. to review the litigation documents and independently determine the medical errors and the departments in which they took place. A third physician further reviewed the divergent results. After the descriptive statistical analysis and mind map analysis, semi-structured interviews were further conducted with 63 doctors to reveal the relationships mentioned above.
Results: More than 97.8% of medical errors occurred in clinical departments. The insufficient implementation of informed consent obligations is the top medical error in all medical departments [internal medical departments (12.86%, N=36), surgical departments (14.57%, N=106), specialist departments (13.16%, N=86)]. The types of medical errors in diverse medical departments might be associated with therapeutic means used by physicians. Errors related to surgical operations were common in surgical departments, errors related to diagnoses were common in internal medicine departments, and errors related to therapy were common in specialist departments. A lack of clinical experience and undesirable work system design have contributed to the occurrence of medical errors. Inadequate human resources and unreasonable shift systems have increased the workload of staff members and this has in turn increased the incidence rate of medical errors.
Conclusion: Medical departments are facing medical errors both in humanity and technology. Medical institutions should be alert to the harm caused by medical humanity (mainly including insufficient communication between physicians and patients, insufficient implementation of infringement of informed consent, infringement of patient’s privacy and overtreatment). Improving the clinical skill and vigilance of medical staff is a top priority. Medical institutions should also improve undesirable system designs.
Keywords: medical errors, medical specialties, patient safety, medical disputes, China
Introduction
Medical errors are a stumbling block in regard to improving the quality of medical services; they pose a great threat to patient safety.1 Medical errors are also a major cause of death.2 It is estimated that between 44,000 and 98,000 people die each year in the United States as a result of adverse events caused by medical errors.3 In the global context, the estimated death toll is as high as 400,000 and the actual figure may be even higher.4 In addition, medical errors can lead to social problems. Studies have found that more than 20% of doctor-patient disputes are caused by medical errors.5
In fact, the causes of medical errors are complex; they include the negligence of medical staff, defective regulations within medical institutions, and excessive workloads.6 And excessive fatigue from the defective working system had a further negative performance impairment in shift-work for medical staff.7 On the whole, most medical errors are due to the system, and being system-related, should be fixed by improving the system itself and reducing the risk of errors by managing processes and practices. In view of the fact that methods of reducing errors have been successfully applied to aviation and other fields, improvements to the medical service have emerged, such as increasing investment in human resources, reducing working hours, establishing electronic health records, and reshaping the patient safety culture.8–11 However, these countermeasures are slightly generic, because they tend to target a single department or the hospital as a whole without subdividing medical errors into different departments. Therefore, some scholars think that such general interventions may be ineffective.12,13
What are the types of medical errors that occur in each department? Why do diverse medical errors occur in different departments? What countermeasures should be taken to effectively prevent medical errors? Specialty-specific interventions need to pin down the relationship between the departments and medical errors. Existing studies have found that adverse events treated by internists and neurologists were usually medication-related, whereas adverse events treated by surgeons, orthopedic surgeons, and neurosurgeons were usually procedure-related.14 However, the medical errors that occur in emergency departments are mainly delayed diagnosis and treatment, and improper disposal of patients’ condition.15 Although delayed diagnosis also occurs in pediatric departments, the causes are essentially different.16,17 In anesthesiology department, the most frequent medical errors are omission and incorrect dose.18 In addition, some systematic reviews have deepened our understanding of the relationship between various departments and the types of medical errors that occur within them,19,20 but there is still a lack of empirical study summarizing the situation across all departments.
It is of significance in multiple domains to probe into the types and causes of medical errors in different departments. First, doing so constitutes a key method of ensuring patient safety. Ensuring patient safety requires medical institutions and staff members to minimize the incidence of errors.21 Avoiding medical errors reduces not only the mortality or morbidity within the department but also reduces unnecessary medical costs and related expenses.22,23 Second, the prevention of medical errors can reduce the psychological burden of medical staff, so they will no longer become the second victims of medical errors.24 Meanwhile, their fear, pain, and job burnout will be alleviated.25,26
We hope that the medical staff can obtain experience from this research. Finally, some systematic reviews have summarized the types of medical errors in various specialties, but only combining the existing conclusions to analyze seems to be insignificant in practice. For this reason, we make use of medical disputes in China to make up for the deficiencies of existing research, by collecting statistics, explaining the causes of medical errors in different departments with in-depth interviews, and proposing targeted measures and forms of prevention.
Methods
Study Design and Sample
“China Judgments Online” provides a large amount of accessible data for the study of medical errors. First, we used a computer crawler to conduct a comprehensive search of medical litigation cases according to the key words including medical errors and retrieved a total of 5237 judgment documents related to medical disputes. Second, we removed 165 unrelated judgment documents. Again, we extracted 2536 of these using a systematic random sampling method. Finally, we invited three physicians to determine the medical errors and departments involved. The above-mentioned medical litigation documents are legal after the court’s judgment takes effect. Then, contents of the cases are based on objective facts from both doctors and patients in regard to medical activities and are representative of the errors that occur in real situations.
Coding of Medical Errors
First, before coding the medical errors, we performed a preliminary division of medical errors based on the existing literature and the classification table published by the Beijing Health Law Society.27–29 Then, we invited 34 frontline doctors to modify and supplement the classification table in turn according to their work experience in practice. The revised classification table covers seven types of first-class errors, 26 types of second-class errors, and 113 types of third-class errors. Table 1 shows part of the classification table. The complete table is presented in the Appendix.
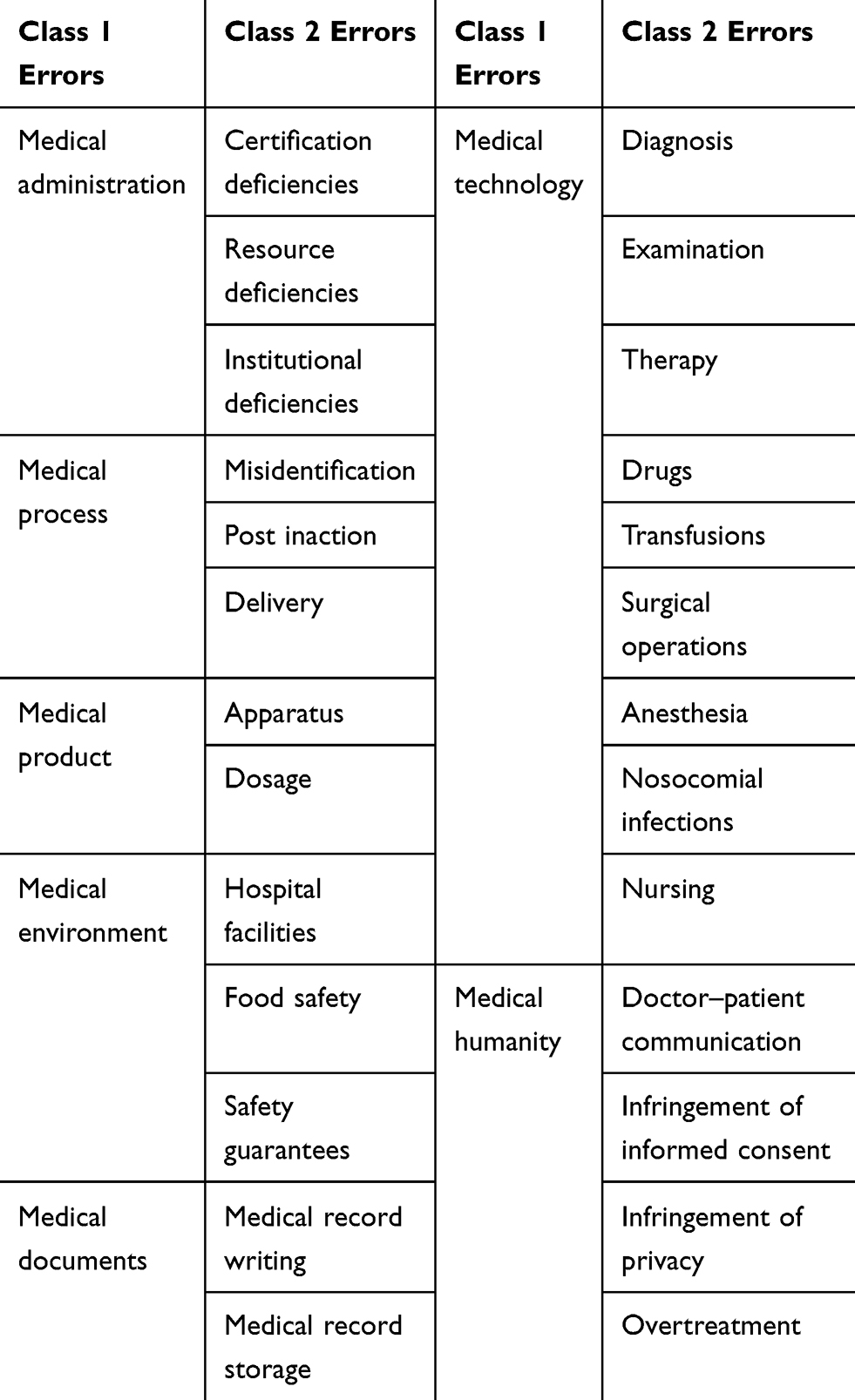 |
Table 1 Medical Error Classification Table (First-Class and Second-Class Errors) |
Coding of Medical Departments
Regarding the division of departments, we refer to the “List of Medical Treatment Subjects in Medical Institutions” and the “Guidelines for Medical Service Capabilities of Tertiary Comprehensive Hospitals (2016 Edition)” promulgated by the National Health Commission of the People’s Republic of China. Based on the documents and the settings of medical institutions in practice, we have constructed a department classification table. The departments are divided into two categories: clinical departments and medical technology departments. The clinical departments are composed of internal medicine, surgical, and specialist departments. The list of specific departments is shown in Figure 1.
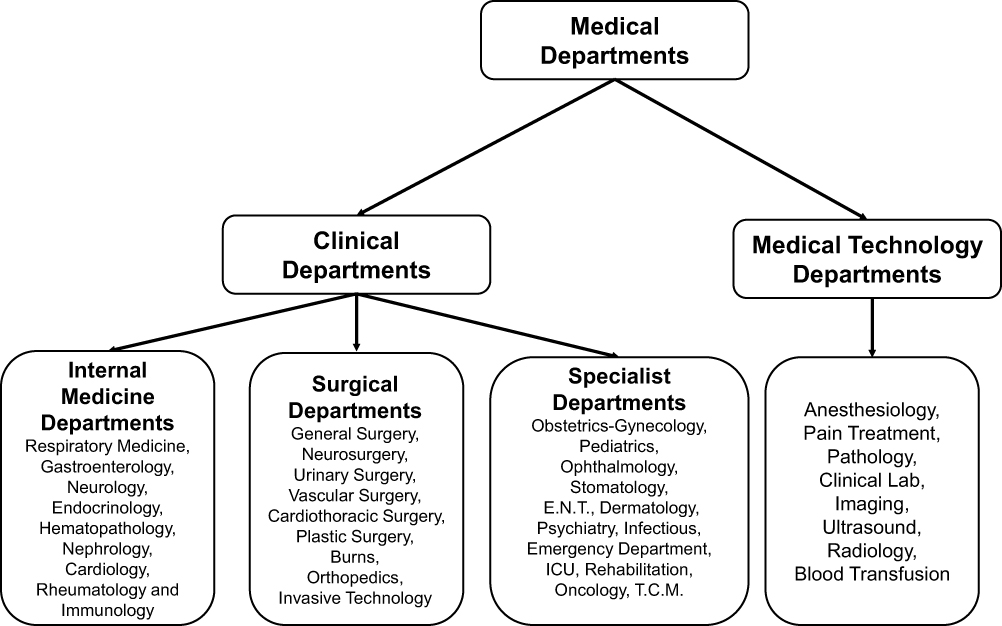 |
Figure 1 Medical department categories. |
The Chinese government divides medical institutions into three categories: primary care institutions, secondary hospitals, and tertiary hospitals. Because the size of primary care institution is small and medical resources are limited, it is impossible to establish a complete department system. Therefore, we regard medical errors in primary hospitals, private clinics, township hospitals, and private medical institutions as medical errors that have occurred in primary care institutions and no longer subdivide the specific departments.
Data Collection
The data collection of medical errors and departments were encoded by three physicians who have seven years of clinical experience. To ensure the reliability and validity of the study,30 we first sent the medical litigation documents to two physicians and asked them independently to determine the medical errors and departments involved. Then, we invited the third physician to review the divergent results and make a final judgment. We compared the results of the third physician’s judgments with the two physicians’ and included the identical results in the database.
Of the 2536 litigation documents, 524 were unrelated to medical disputes. After removing these samples, we obtained data regarding 2012 medical errors. Inconsistencies in the judgments made by the three physicians were found in 25 of the 2012 medical litigation documents. As a result, we eliminated the data regarding the 25 medical errors and finally analyzed statistical data regarding 1987 medical errors. Figure 2 shows the specific process of data collection.
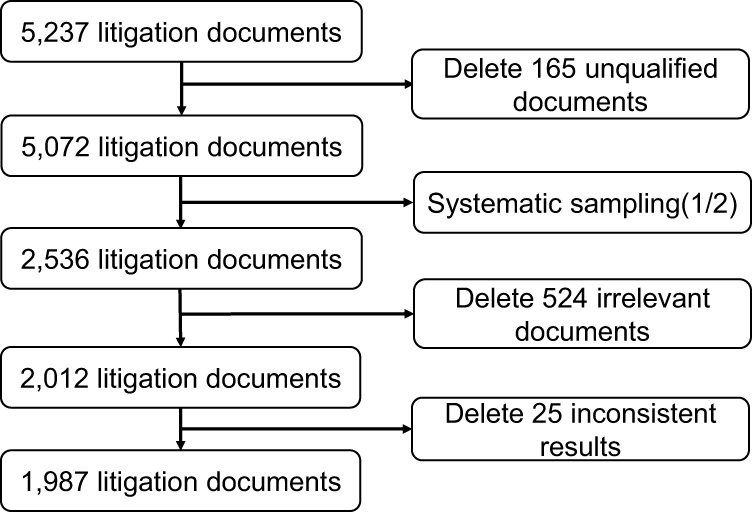 |
Figure 2 Specific process of data collection. |
Results
In order to present the rate of medical errors in different departments, we calculated the types and number of medical errors in each department. Table 2 shows that over 97.8% of medical errors occur in clinical departments (n = 1714). After subdivision, those medical errors are mainly concentrated in surgical departments and specialist departments, which account for 83.7% of clinical departments. As for internal medicine departments, their total number of medical errors is only 1/3.2 of surgical departments and 1/2.7 of specialist departments.
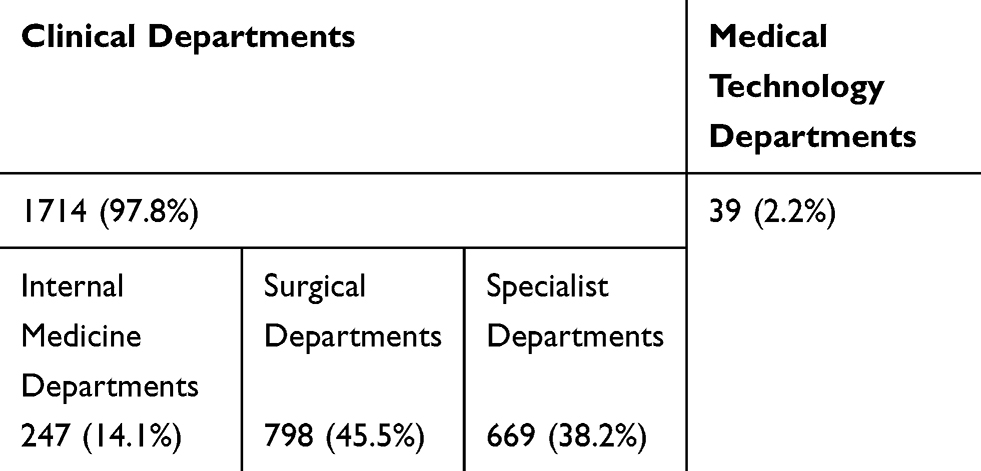 |
Table 2 The Number and Percentage of Medical Errors in Different Departments |
Table 3 shows the number of medical errors in specific departments, with surgical departments and specialist departments dominating the ranking. In addition to the orthopedic and obstetrics-gynecology departments, the number of medical errors in the general surgery department is much higher than in other departments. The frequency of medical errors in medical technology departments is far lower than in clinical departments, the blood transfusion department had the highest frequency of medical errors (n = 22).
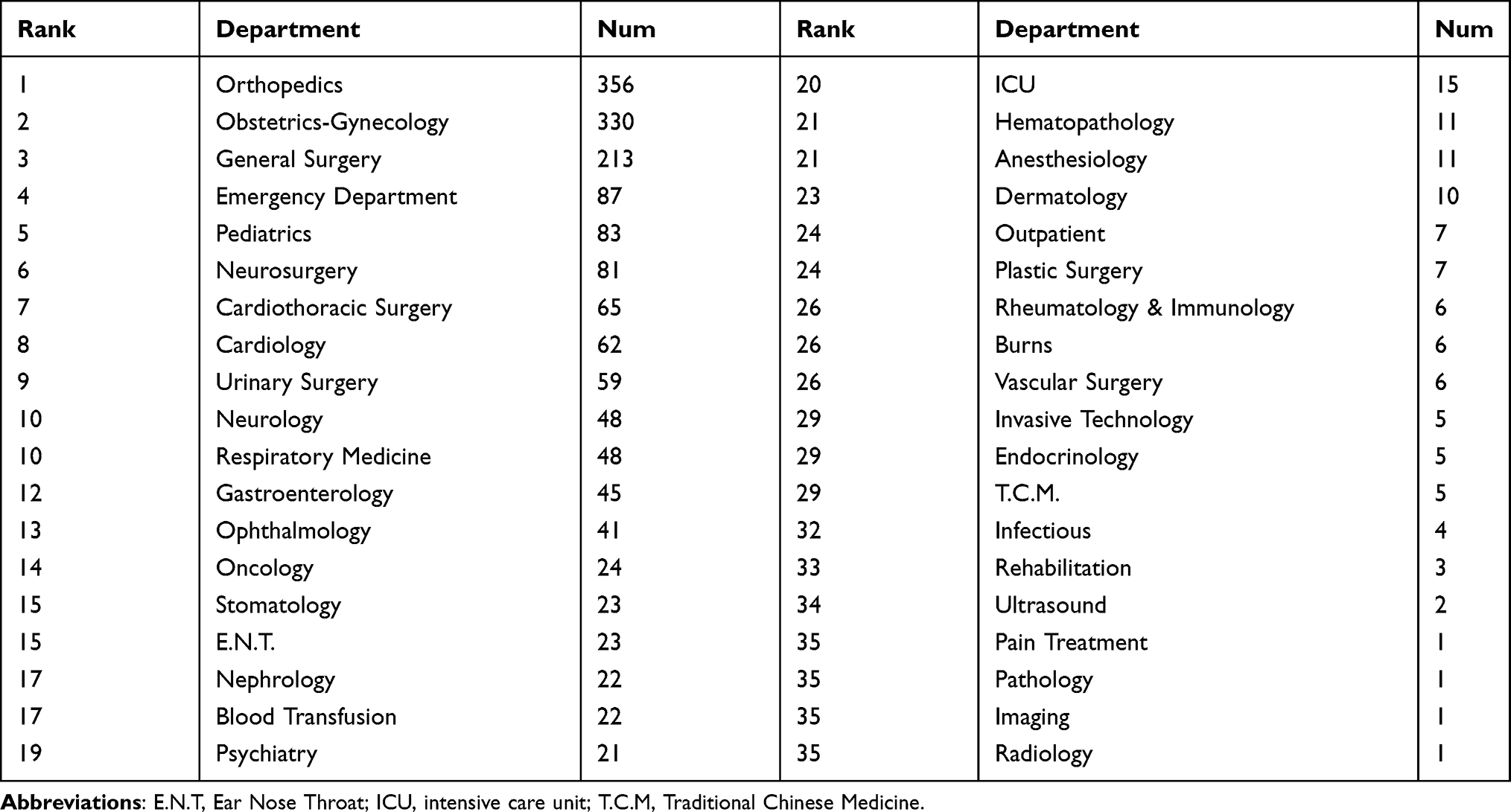 |
Table 3 The Number of Medical Errors in Specific Departments |
The types of medical errors in specific departments show different characteristics. In order to distinguish the class 3 errors in different clinical departments, we calculated the percentage of some frequent errors in each department. The line of different color means different sort of clinical department and there are detailed instructions of lines in different color in the Figure 3. The four-digit number on the ordinate is the error code. Due to the limited graphic space, please refer to the classification table of medical errors in the Appendix to match the specific error according to the need.
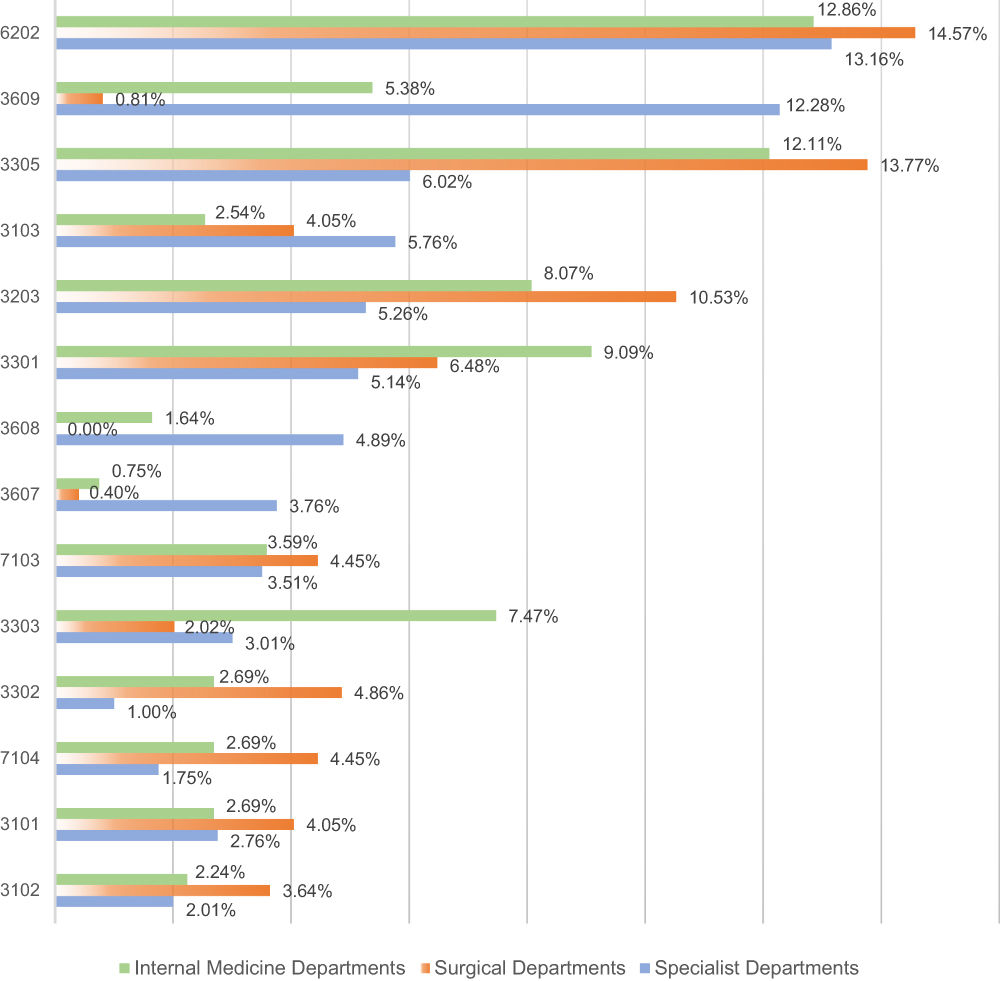 |
Figure 3 The common types of medical errors in clinical departments. |
It can be seen in Figure 3 that the insufficient implementation of informed consent obligations (6202), which belongs to the category of medical humanity errors, is a common error in clinical departments. Although medical technology errors account for a large proportion of the errors that occur in clinical departments, the types of errors that occur in internal medicine departments, surgical departments, and specialist departments become different after subdivision. The medical errors that occur in surgical and specialist departments are partly similar, especially those related to therapy and surgery, including improper observation during treatment (3305), the intraoperative damage of tissues and organs (3608), and post-operation complications (3609). The total number of errors in internal medicine departments is not large, but it also presents a unique trend. Diagnosis- and examination-related errors are common in internal medicine departments, especially delayed diagnosis (3102), missed diagnosis (3103), and insufficient inspection (3203).
In order to better show the relationships between departments and medical errors, we employ mind map to visually analyze the degree of correlation between them. We calculated the number of frequent medical errors in different departments, and divided the errors into six categories based on the number. The larger the number, the higher the weight of the error, and the thicker the line with the department. We adopted different colored lines to substitute different medical departments. As can be seen in Figure 4, medical errors in internal medicine, surgical, and specialist departments jointly point to the insufficient implementation of informed consent obligations and improper observation during treatment. Besides, the lines starting from internal medicine departments also point to insufficient inspection, misdiagnosis, missed diagnosis, and delayed diagnosis. The lines starting from surgical departments are more inclined to point to post-operation complications, the intraoperative damage of tissues and organs, and the failure to cure protopathy. Most specialist departments that adopt surgical treatment are similar to surgical departments in their commonly occurring types of errors, while medical errors in most departments with non-surgical treatment are similar to those occurring in internal medicine departments.
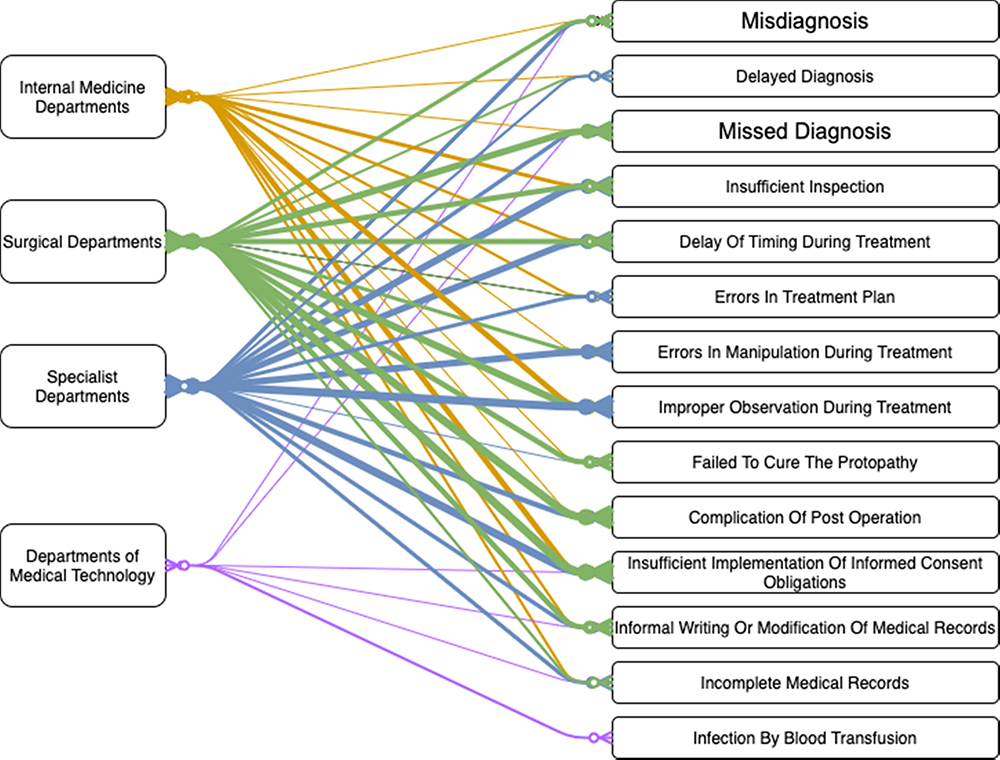 |
Figure 4 Network relationship diagram between departments and medical errors. |
Qualitative Results
Ethics Statements
All contents of the interviews were conducted with physicians face to face. All the participants voluntarily accepted our interview. The privacy, anonymity, and security of participants were rigorously respected in the interview.
To explain the difference between the types and number of medical errors in each department, we interviewed 63 medical staff. Through the introduction of their occupational content and environmental features, we analyzed the logical relationship between different types of medical errors in various departments. Through an unstructured form, the outline of the interview is designed to answer a core question: What are the reasons why such types of medical errors occur in this department? The interview was recorded in writing.
There are Differences Between Medical Institutions of Dissimilar Grades
We found that primary care institutions were more likely to face two types of medical errors: the unqualified practice of medical staff and excessive practice in medical institutions. These errors reflect two problems. On the one hand, the supervision of government is insufficient; on the other hand, the practical skills of the medical staff are inferior.31 Simply speaking, China is facing the vertical disparity of medical resource distribution.32 The vertical disparity means primary care institutions own fewer medical resources than secondary and tertiary hospitals. The poor quality of primary care institutions may result in the failure of the tiered medical services system.33
Patient preference increases the likelihood of medical errors in tertiary hospitals. Excessive visits limit the time allowed for clinical reception,34 and the increasing workload of doctors often induces medical errors. The more advanced technology for diagnosis and treatment in tertiary hospitals plays a fundamental role in the therapeutic process, so patients often regard tertiary hospitals as a “lifesaver”. However, evidence-based medicine is a continuous process of excluding disease causes. Therefore, it is inevitable that there are various diagnosis-related errors in tertiary hospitals when encountering complex cases.
As a doctor in a tertiary hospital, the daily patient visit has exceeded my tolerance. Too many patients queue up; we can only shorten the time allotted for clinical reception. Sometimes the patient’s information is not fully conveyed, and they cannot understand the prescription. And I have encountered too many incurable diseases in the past few years. The cause is not clear. (Gastroenterologist, 35 years old)
Most Medical Errors in Internal Medicine Departments are Related to Diagnosis
The differences between the types of medical errors in diverse departments can be attributed to the treatments adopted by doctors. Surgical departments mainly treat patients through surgery and there are thus some medical errors related to the surgical process.14 Similarly, internal medicine departments tend to make diagnoses and there are hence medical errors related to diagnosis common. Research has found that internal medicine departments are a major area of disputes.35 However, we found that the number of medical errors in internal medicine departments was significantly lower, which may be connected to patients’ weak self-perception of medical errors.
Although rarely using surgery, most of us diagnose and use drugs according to the relevant guidelines. Sometimes, we do a full-scale examination for patients but cannot determine the problem. If the patient is diagnosed in another hospital, they may come back to prosecute us. But our nephrology department is not like surgical departments, which require surgery, so the number of errors will be relatively small. (Nephrologist, 30 years old)
The Types of Medical Errors in Surgical Departments are Similar to Those in Specialist Departments
The high incidence of surgical errors and therapy-related errors are also more frequent, which may be related to the inexperience of surgeons.36 Surgeons in China are trained to follow an apprentice system. The skills and experience are taught by their supervisors, and medical errors may occur when their skills are immature. Previous studies have found that insufficient clinical experience and poor operation skills are partly responsible for medical errors.6 As in many countries, the process of training Chinese medical students does not include courses related to medical errors. This leads to young surgeons lacking experience in regard to avoiding medical errors at work.37
I made an error shortly after work because my clinical experience was poor and there was a problem during operation. Fortunately, the tutor corrected it in time, or it would have been unimaginable. I can only accumulate experience through operations in practice. Before I went to the hospital for an internship, the school never gave us courses related to medical errors. I only started to know about the existence of errors after I started to work. (Neurosurgeon, 34 years old)
Medical errors in specialist departments mainly occur in departments involving pediatrics and obstetrics-gynecology, and emergency departments. The improper observation of disease in pediatric departments is caused by the inexperience of medical staff, as well as poor communication between doctors and patients.16 It is more difficult to determine children’s conditions than adults’ because children often fail to accurately express their disease conditions.
The incidence of medical errors in obstetrics-gynecology departments fluctuates in different periods, and the number of patients in July and August sharply increases each year, which is to some extent associated with the age limit of primary school admission. In July and August, medical services cannot meet the enormous demands of patients. Therefore, the overwhelming number of visits forces obstetricians and gynecologists to overwork and their compressed rest time also to some degree increases the possibility of medical errors.38
If we make a ranking of happiness for doctors in each department, our pediatricians’ happiness is definitely the last. We are surrounded by a group of crying and troubled children every day, and the children do not say where they are uncomfortable; they just cry all the time. (Pediatrician, 31 years old)
We are fatiguing, especially during the summer vacation. Gravidas do not want their children to go to school one year later, so they rush before September First. When their children are born, the workload during this time is particularly large. Without enough doctors, we can only reduce our rest time to meet the needs of the patients. (Obstetrician and Gynecologist, 37 years old)
Emergency departments have always suffered from frequent medical errors, and previous studies have shown that medical errors occur in all aspects of emergency care.39 Good clinical skills are essential for emergency department doctors.40 However, therapy-related errors should be attributed to the complexity of the patients’ conditions.15 Patients are often in urgent situations and sent to the hospital at night, which requires medical staff to have both a wealth of clinical experience and extremely quick response capabilities. The highly stressful working state might induce medical errors.
Young doctors can still work in the emergency departments. Elderly doctors can’t stand the work at all. The work intensity is too great, especially after midnight. Various patients come one after another. Although we have rested for 48 hours, we have not adjusted well most of the time. The main problem is that there are not enough doctors who have rich clinical experience. (Emergency Medicine Specialist, 33 years old)
Discussion and Conclusion
First, ensuring the informed consent of patients correctly is a major premise for avoiding errors related to medical humanity. We found that a large number of doctor-patient disputes are related to the insufficient implementation of informed consent obligations. Compared with surgery or therapy-related errors, this medical error will not result in extremely serious consequences, but it will pose an indirect threat to patient safety. So, medical institutions need to train and educate medical staff accordingly. At the same time, the government needs to strengthen supervision. In addition to strictly controlling the licensing of medical qualifications, daily supervision should focus on the qualifications of medical staff, so as to wipe out illegal medical practices from the beginning.
Second, some countermeasures and suggestions provided by existing research are beneficial to this study. Improving the diagnostic and therapeutic skills and vigilance of medical staff is the primary way to avoid medical errors, especially in pediatric departments and some internal medicine departments, which require doctors with rich expertise and skillful diagnosis abilities.17 Young doctors generally lack clinical experience and sufficient vigilance, thus leading to the failure to effectively control preventable errors.41
Third, medical institutions should properly reduce the working hours and shift frequencies of medical staff. This approach can be used in ICUs12 and we believe it is also applicable to doctors from emergency departments and obstetricians. Reducing working hours and shift frequency requires more manpower reserves.6,9,42 In a word, patient safety necessitates the avoidance of overworked medical staff.
Finally, each department should establish a standardized written handover system. Studies have shown that the implementation of this sort of transmission program not only has no negative impact on workflow but also effectively reduces medical errors.43 For medical technology departments that need to cooperate with clinical departments, the establishment of a written handover system can prevent omissions and errors in the process of information transmission.
Study Limitations
Although using litigation documents to study medical errors may give a selection of medical errors that occur, to this very day, it is the only open data resource in China. This study may be conducive to academia in terms of enhancing their perception of medical errors in the empirical world. In particular, this study enables frontline medical staff to understand the causes of medical errors. We hope that researchers will focus more on these issues and will continue to emphasize and perfect the research on patient safety with samples from different countries and regions.
Acknowledgments
This study is supported by the Major Program of the National Social Science Fund of China (Grant No. 18ZDA362): The Research on Physician–Patient Relationship in the Era of Big Data. Thanks to the three physicians involved in this study for their dedication to error coding. They are Dr. Ren Chen (Associate Chief Physician from the Department of Radiotherapy, Nanfang Hospital of Southern Medical University), Dr Deng Jun (from the Department of Gastroenterology, Sixth Affiliated Hospital of Sun Yat-sen University), and Dr Gao Wenjie (Attending Physician from the Department of Orthopedics, Sun Yat-sen Memorial Hospital, Sun Yat-sen University).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marjoua Y, Bozic KJ. Brief history of quality movement in US healthcare. Curr Rev Musculoskelet Med. 2012;5:265–273. doi:10.1007/s12178-012-9137-8
2. Makary MA, Daniel M. Medical error—the third leading cause of death in the US. BMJ. 2016;353:i2139–2144. doi:10.1136/bmj.i2139
3. Kohn LT, Corrigan JM, Donaldson MS, et al. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
4. James JT, New A. Evidence-based estimate of patient harms associated with hospital care. J Patient Saf. 2013;9:122–128. doi:10.1097/PTS.0b013e3182948a69
5. Aoki N, Uda K, Ohta S, Kiuchi T, Fukui T. Impact of miscommunication in medical dispute cases in Japan. Int J Qual Health C. 2007;20:358–362. doi:10.1093/intqhc/mzn028
6. Tanaka M, Tanaka K, Takano T, Kato N, Watanabe M, Miyaoka H. Analysis of risk of medical errors using structural-equation modelling: a 6-month prospective cohort study. BMJ Qual Saf. 2012;22:784–790. doi:10.1136/bmjqs-2010-048330
7. Dawson D, Reid K. Fatigue, alcohol and performance impairment. Nature. 1997;388:235. doi:10.1038/40775
8. Braithwaite J, Marks D, Taylor N. Harnessing implementation science to improve care quality and patient safety: a systematic review of targeted literature. Int J Qual Health C. 2014;26:321–329. doi:10.1093/intqhc/mzu047
9. Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. New Engl J Med. 2004;351:1838–1848. doi:10.1056/NEJMoa041406
10. Menendez ME, Janssen SJ, Ring D. Electronic health record-based triggers to detect adverse events after outpatient orthopedic surgery. BMJ Qual Saf. 2016;25:25–30. doi:10.1136/bmjqs-2015-004332
11. Liu C, Liu W, Wang Y, Zhang Z, Wang P. Patient safety culture in China: a case study in an outpatient setting in Beijing. BMJ Qual Saf. 2014;23:556–564. doi:10.1136/bmjqs-2013-002172
12. Pham JC, Aswani MS, Rosen M, et al. Reducing medical errors and adverse events. Annu Rev Med. 2012;63(1):447–463. doi:10.1146/annurev-med-061410-121352
13. Singer SJ, Vogus TJ. Reducing hospital errors: interventions that build safety culture. Annu Rev Publ Health. 2013;34:373–396. doi:10.1146/annurev-publhealth-031912-114439
14. Magdelijns FJH, Pijpers E, Rouhl RPW, et al. Acute hospital admissions because of health care–related adverse events: a retrospective study of 5 specialist departments. J Am Med Dir Assoc. 2015;16:1–7. doi:10.1016/j.jamda.2015.06.019
15. Schenkel SM, Khare RK, Rosenthal MM, Sutcliffe KM, Lewton EL. Resident perceptions of medical errors in the emergency department. Acad Emerg Med. 2003;10:1318–1324. doi:10.1111/j.1553-2712.2003.tb00004.x
16. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285:2114–2120. doi:10.1001/jama.285.16.2114
17. Conrad VF, Jane GR. Strategies for the prevention of medical error in pediatrics. J Pediatr. 2003;143:155–162. doi:10.1067/S0022-3476(03)00244-0
18. Zhang Y, Dong YJ, Webster CS, et al. The frequency and nature of drug administration error during anaesthesia in a Chinese hospital. Acta Anaesthesiol Scand. 2013;57:158–164. doi:10.1111/j.1399-6576.2012.02762.x
19. Vries END, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA, Incidence T. Nature of in-hospital adverse events: a systematic review. Qual Saf Health Care. 2008;17:216–223. doi:10.1136/qshc.2007.023622
20. Harrison R, Cohen AWS, Walton M. Patient safety and quality of care in developing countries in Southeast Asia: a systematic literature review. Int J Qual Health C. 2015;27:240–254. doi:10.1093/intqhc/mzv041
21. Leape LL, Berwick DM, Bates DW. What practices will most improve safety? Evidence-based medicine meets patient safety. JAMA. 2002;288:501–507. doi:10.1001/jama.288.4.501
22. Zhan CL, Miller MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA. 2003;290:868–874. doi:10.1001/jama.290.14.1868
23. Vincent C, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ. 2001;322:517–519. doi:10.1136/bmj.322.7285.517
24. Wu AW. Medical error: the second victim. Brit J Hosp Med. 2012;73:726–727. doi:10.1136/bmj.320.7237.726
25. West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy–a prospective longitudinal study. JAMA. 2006;296:1071–1078. doi:10.1001/jama.296.9.1071
26. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251:995–1000. doi:10.1097/sla.0b013e3181bfdab3
27. Elder NC, Dovey SM. Classification of medical errors and preventable adverse events in primary care: a synthesis of the literature. J Fam Practice. 2002;51:927–932. doi:10.1016/S0095-4543(02)00043-X
28. Leape LL. Error in medicine. JAMA. 1994;272:1851–1868. doi:10.1001/jama.1994.03520230061039
29. Weingart SN, Wilson RM, Gibberd RW, Harrison B. Epidemiology of medical error. BMJ. 2000;320:774–777. doi:10.1136/ewjm.172.6.390
30. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. New Engl J Med. 2006;354:2024–2033. doi:10.1056/NEJMsa054479
31. Zhang X, Chen LW, Mueller K, Yu Q, Liu J, Lin G. Tracking the effectiveness of health care reform in China: a case study of community health centers in a district of Beijing. Health Policy. 2011;100:181–188. doi:10.1016/j.healthpol.2010.10.003
32. Zhang T, Xu Y, Ren J, Sun L, Liu C. Inequality in the distribution of health resources and health services in China: hospitals versus primary care institutions. Int J Equity Health. 2017;16:42. doi:10.1186/s12939-017-0543-9
33. Yip WC, Hsiao WC. The Chinese health system at a crossroads. Health Affair. 2008;27:460–468. doi:10.1377/hlthaff.27.2.460
34. Hu Y, Zhang Z. Skilled doctors in tertiary hospitals are already overworked in China. Lancet Glob Health. 2015;3:737. doi:10.1016/S2214-109X(15)00192-8
35. Guly HR. Diagnostic errors in an accident and emergency department. Emerg Med J. 2002;18:263–269. doi:10.1136/emj.18.4.263
36. Sousa P, Uva AS, Serranheira F, Nunes C, Leite ES. Estimating the incidence of adverse events in Portuguese hospitals: a contribution to improving quality and patient safety. BMC Health Serv Res. 2014;14:311–316. doi:10.1186/1472-6963-14-311
37. Goldberg RM, Kuhn G, Andrew LB, Thomas HA
38. Rogers AE, Hwang WT, Scott LD, Aiken LH, Dinges DF. The working hours of hospital staff nurses and patient safety. Health Affair. 2004;23:202–212. doi:10.1377/hlthaff.23.4.202
39. He AJ. The doctor–patient relationship, defensive medicine and overprescription in Chinese public hospitals: evidence from a cross-sectional survey in Shenzhen city. Soc Sci Med. 2014;123:64–71. doi:10.1016/j.socscimed.2014.10.055
40. Fordyce J, Blank FSJ, Pekow P, et al. Errors in a busy emergency department. Ann Emerg Med. 2003;42:324–333. doi:10.1016/s0196-0644(03)00398-6
41. Thomas EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000;38:261–267. doi:10.1097/00005650-200003000-00003
42. Rekleiti M, Kyloudis P, Toska A, Saridi M. Patient safety and healthcare quality. Int J Caring Sci. 2012;5:74–79.
43. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. New Engl J Med. 2014;371:1803–1812. doi:10.1056/NEJMsa1405556
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.