")
Back to Journals » Advances in Medical Education and Practice » Volume 13
Reintroduction of Post-Baccalaureate Doctor of Pharmacy (PharmD, Post-Bac) Program in Nepal: Exploration of the Obstacles and Solutions to Move Forward
Authors Shrestha S , Shrestha S , Sapkota B , Shakya R, Roien R , Mohamed Ibrahim MI
Received 9 November 2021
Accepted for publication 2 February 2022
Published 18 February 2022 Volume 2022:13 Pages 159—166
DOI https://doi.org/10.2147/AMEP.S348601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Sunil Shrestha,1,2,* Sweta Shrestha,3,* Binaya Sapkota,2,* Rajani Shakya,3 Rohullah Roien,4 Mohamed Izham Mohamed Ibrahim5
1Department of Pharmaceutical and Health Service Research, Nepal Health Research and Innovation Foundation, Lalitpur, Nepal; 2Nobel College of Health Sciences, Affiliated to Pokhara University, Kathmandu, Nepal; 3Department of Pharmacy, School of Science, Kathmandu University, Dhulikhel, Nepal; 4Medical Research Centre, Kateb University, Kabul, Afghanistan; 5Department of Clinical Pharmacy and Practice, College of Pharmacy, QU Health, Qatar University, Doha, Qatar
*These authors contributed equally to this work
Correspondence: Sweta Shrestha; Rohullah Roien, Email [email protected]; [email protected]
Abstract: This commentary article highlights the status of clinical pharmacy education in Nepal, explores the challenges and solutions in sustainably reintroducing Post-Baccalaureate Doctor of Pharmacy (PharmD, Post-Bac) in Nepal, as was previously launched by Kathmandu University (KU) Department of Pharmacy in 2010, and suggests a few prospects forward. Clinical pharmacy practice has remained on the sidelines and subordinate to physicians in Nepal. KU launched the PharmD (Post-Bac.) as a postgraduate program to establish the professional identity of clinical pharmacists in the country. However, despite unremitting efforts, the program did not thrive long and held since 2014. This paper aimed to explore challenges that remained at the forefront of the program and provide possible solutions for its reintroduction. The KU produced three batches of PharmD Post-Bac. graduates and now the revival of the program is crucial. Undoubtedly, a well-trained clinical preceptor can bring significant changes in the quality and competency of the PharmD graduates. Advocacy programs to foster the role of clinical pharmacists in the patient care services and revisiting of Bachelor of Pharmacy (BPharm) curriculum to complement the necessity of the PharmD program are needed. The non-sustenance of the PharmD program is emblematic of the dire mosaic that the clinical pharmacists are facing while delivering patient-oriented services in the country. Hence, strategies need to be formulated for the revival and sustainability of the program.
Keywords: clinical pharmacy, PharmD, pharmacist, Nepal
Introduction
Globally, the pharmacy profession is one of the most well-known and recognized professions. Over recent decades, the pharmacy profession has begun to undertake significant changes in practice. However, in Nepal, pharmacy practice is still in its infancy. There has been a considerable increase in pharmacy colleges and pharmacy graduates; however, a clear career path for pharmacists still lacks.1,2 With the continuity of this situation, the brain drain will be challenging to avoid. Clinical pharmacy is well developed and accepted in western society, but the situation is still woeful in Nepal.1,3,4
Dramatic changes in the health care system are creating many new and exciting roles for pharmacists. Pharmacists are now responsible for the safe and effective distribution of prescription and non-prescription medications. However, they also assume the role of pharmaceutical therapy advisor and manager in providing patient-care services.
Most pharmacists enter either into the pharmaceutical industries or academia in Nepal and rarely in the community-level health care or hospitals. After being a part of health care for such an extended period since Kathmandu University (KU) first launched the Bachelor of Pharmacy (BPharm) program in 1994 it is high time that pharmacists gain and implement the global experiences in hospital, clinical and community pharmacies. Later, postgraduate programs in pharmacy such as MPharm in Pharmaceutical Care, MPharm in Industrial Pharmacy were launched by KU, MPharm Clinical Pharmacy by Pokhara University (PU), and Purbanchal University. The Medical Education Commission (MEC), the only government body for regulating health science programs of all universities and affiliated colleges in Nepal, has recently permitted KU to launch two new specializations of MPharm, namely in Pharmaceutical Analysis, and Pharmacognosy and Phytochemistry. In addition, MEC has also consented to the relaunch of the postponed PharmD (Post-Bac) program. From 2022 KU would be running two clinical-oriented courses, MPharm in Pharmaceutical Care and PharmD (Post-Bac) in parallel unlike the previous year.
Unlike the developed countries where pharmacy education and curriculum change because of the changing practice, in developing countries, the demand is to change the curriculum with a hope of changing practice - a change model that is quite feasible. According to the International Pharmacy Federation (FIP) framework, the development of initiatives in education, practice or regulation can prompt or serve as drivers of change in others.5
PharmD Program Initiation in Nepal
To meet the demand for change in practice and realize the need to make the pharmacists eligible to provide clinical pharmacy services, PharmD, the post-baccalaureate course, was introduced in the Department of Pharmacy, School of Science, KU, in 2010 for the first time in Nepal.6 The PharmD (Post-Bac) curriculum was so designed that a pharmacist will advise, consult, and help doctors select and dispense medicines to patients and play a significant role in medication therapy management (MTM). The three-year PharmD program received equivalency of Master’s degree in pharmacy from Tribhuvan University (TU), Nepal (the only authority in Nepal to provide equivalency and approve the programs). Other modalities of PharmD programs such as six-year PharmD and five-year PharmD from India and Pakistan, respectively, after the intermediate level, were recognized as the Bachelor’s degree by TU.
The three-year PharmD, Post Bac. program, introduced by KU, was divided into two phases: Phase I – consisting of the first and second academic year with two semesters in each and Phase II – consisting of internship or residency training in the speciality units of hospitals during the third year. PharmD, Post-Bac students, were trained in different dimensions of pharmacy practice during the internship, such as pharmacotherapy of various body systems (eg, cardiovascular, nervous, respiratory, gastrointestinal, and others) and clinical pharmacy practice. In addition, students were deputed in different departments of hospitals (eg, medicine, surgery, anesthesiology, cardiology, dermatology, paediatrics, pharmacy, pharmacovigilance, and medicine information centre, gynaecology-obstetrics, neurology, dentistry and others). In addition to this, students were provided weekly three-day exposure to clinical ward rotations at the Dhulikhel Hospital for the first one and half years. Project work of one semester was included at the end of the second year, where the students developed and presented the report of their clinical research output akin to a thesis. Altogether, KU trained 29 PharmD, Post-Bac graduates, all of whom are contributing well to the health care arena in Nepal and abroad in clinical pharmacy setup at tertiary care and medical college hospitals, academia at universities and affiliated colleges, central and provincial government regulatory authority, pharmaceutical products development and marketing, community pharmacies and clinics, Research, training, and publication. The country demands significant input from clinical pharmacists in all these areas, including other unexplored ones such as clinical trials, consultant pharmacists, and others. More quality human resources are required. As there is already a pre-established set-up and faculty availability for the PharmD (Post-Bac) program at the department, KU can reintroduce the postponed program with the new vision. KU has developed the mechanism of providing more bed-side evidence-based clinical rounds and practice opportunities to the future PharmD aspirants under the guidance of a dedicated in-house clinical preceptor, following the pathway of the PharmD program elsewhere.7 The MEC has recently mandated KU to relaunch the PharmD program with ten enrollment in a batch, as of the previous format.8 As KU is the pioneer in introducing undergraduate and postgraduate programs in pharmacy in Nepal, the introduction or postponement of any of its programs carries national attention. The ad-hoc postponement of the only PharmD (Post-Bac) program was not free of its national-level impact in clinical pharmacy and the whole pharmacy profession in the country. The Department of Pharmacy (KU) initiated the Pharm D (Post-Bac) program to produce specialized, trained human resources to cater for the needs of individualized patient care and support the paradigm shift towards patient-oriented practice. Despite realizing the untapped potential of clinical pharmacists, the university was bound to keep the PharmD program on hold. Amidst the multiple arrays of challenges faced, the most significant setback was the frail job market for the clinical pharmacists and the relatively low pay scale offered by the working institutions. Considering the risk of unemployment along with challenges mentioned above, an unpleasant decision for holding the program was taken. However, a silver lining was seen when the Ministry of Health and Population (MOHP), Nepal, developed the Hospital Pharmacy Directive 2072 in 2015, stating the recruitment of a clinical pharmacist in every hospital with 51–100 beds.9 This was thought to amplify the importance and platforms of clinical pharmacists seemingly. However, as of 2021, the implementation is hardly visible in practice, irrespective of positive changes. Despite reflecting on the many challenges that still can stand as an impediment to the program, KU spearheaded a second bold attempt to change the status quo for clinical pharmacists and an effort to consolidate a more patient-oriented approach in health care.
Potential Areas for PharmD Graduates in Hospitals of Nepal
With the increase in various general and specialty hospitals in Nepal, there is an emerging scope for PharmD graduates in Nepal. After PharmD graduation, clinical pharmacists can play an essential role in identifying, preventing, and mitigating drug therapy-related problems and stand as pharmaceutical care providers. A few of the potential clinical pharmacy areas that PharmD graduates can focus on and are doing well in the capacity of clinical pharmacists are listed in Table 1.
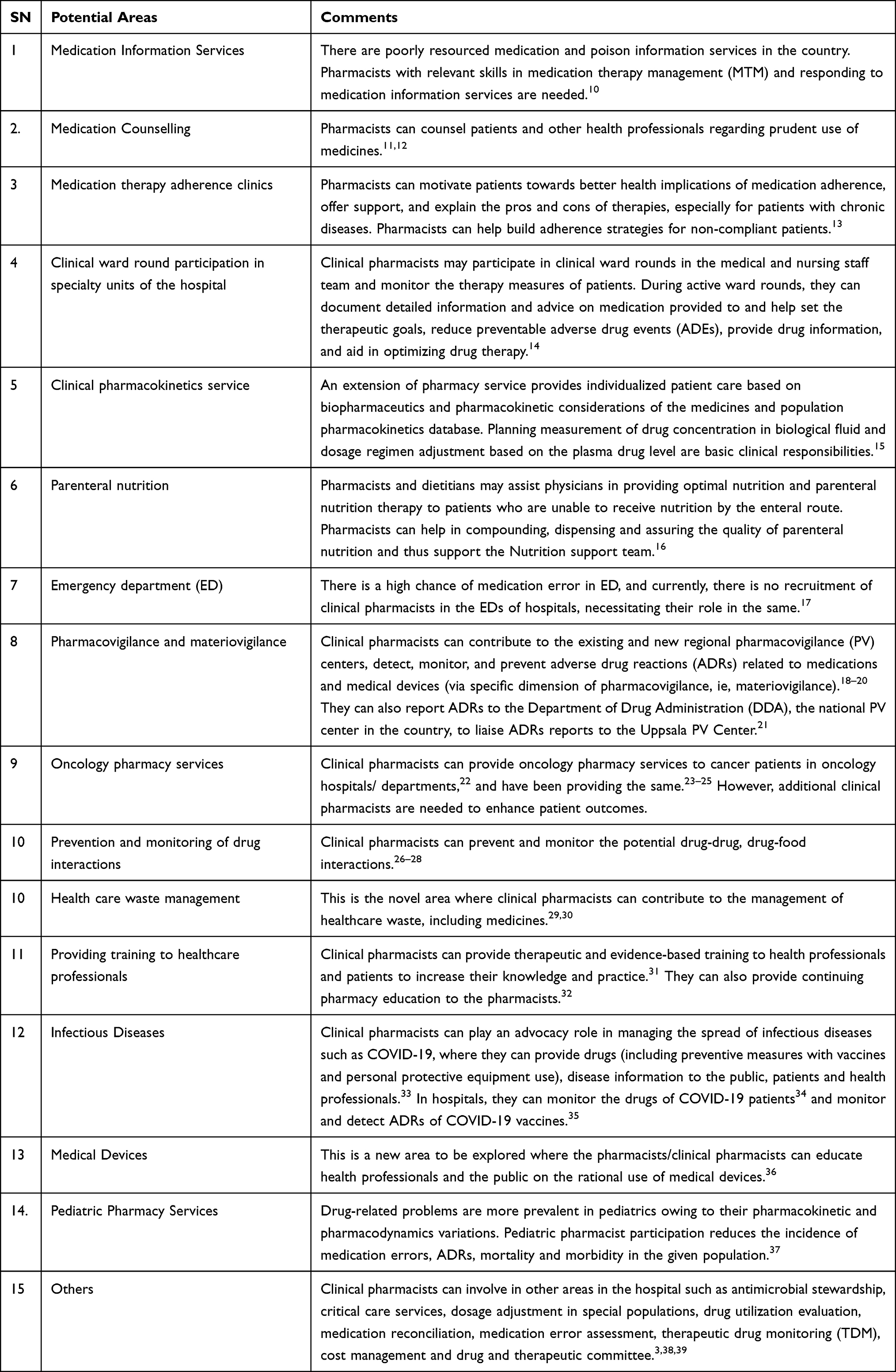 |
Table 1 Potential Areas for PharmD Graduates |
PharmD graduates have other potential roles as well besides those mentioned in Table 1, such as academics, clinical research, marketing, and regulatory affairs.38
Challenges and Potential Solutions to the PharmD Program
Comparison of PharmD Program with MPharm Pharmaceutical Care and MPharm Clinical Pharmacy Programs
Although two-year courses MPharm in Pharmaceutical Care (being run by KU), and MPharm Clinical Pharmacy (being run by PU and Purbanchal University) may appear to be potential alternatives to the PharmD program, these programs are devoid of dedicated annual internship in their core curricula. The PharmD graduates undergo an intensive internship of one year to empower them with the knowledge and skills required to provide individualized patient care, medication review, therapeutic drug monitoring (TDM), clinical ward round participation, etc.
Owing to the one-year short duration, these two programs have condensed internship exposures to only six weeks in hospitals and have aligned more of their focus to academia and research practice. Hence, PharmD program can surpass all theoretical, practical, and clinical practice requirements of these programs and can successfully cater to many service-based requirements in the hospital and community pharmacies, academia, research, and regulatory affairs. Also, PharmD can better be viewed as a practice-based course that prepares the graduates exclusively for direct patient care services with the needful knowledge, exposure, and competency. Besides, PharmD is the only program globally compatible for further specialty certification courses like Board-Certified courses in the USA.
The dominant driving force behind pioneering the PharmD program in Nepal was meeting national need for skilled human resources with clinical competency to practice in a team of health-care professionals involved in direct patient care. Though small, PharmD graduates of this university have made their decent presence in various clinical settings, government regulatory settings, pharmaceutical products development and marketing, research areas with multiple publications in renowned journals, and academia, which clearly reflects success of the program.
There are several possible challenges, such as recognising the role of clinical pharmacists, implications of higher course fees and return of investment, and availability of trained clinical preceptors (Table 2). However, despite the possible hurdles, their national need for skilled human resources with clinical competency to practice in a team of health-care professionals involved in direct patient care was the dominant driving force behind pioneering the PharmD program in Nepal.
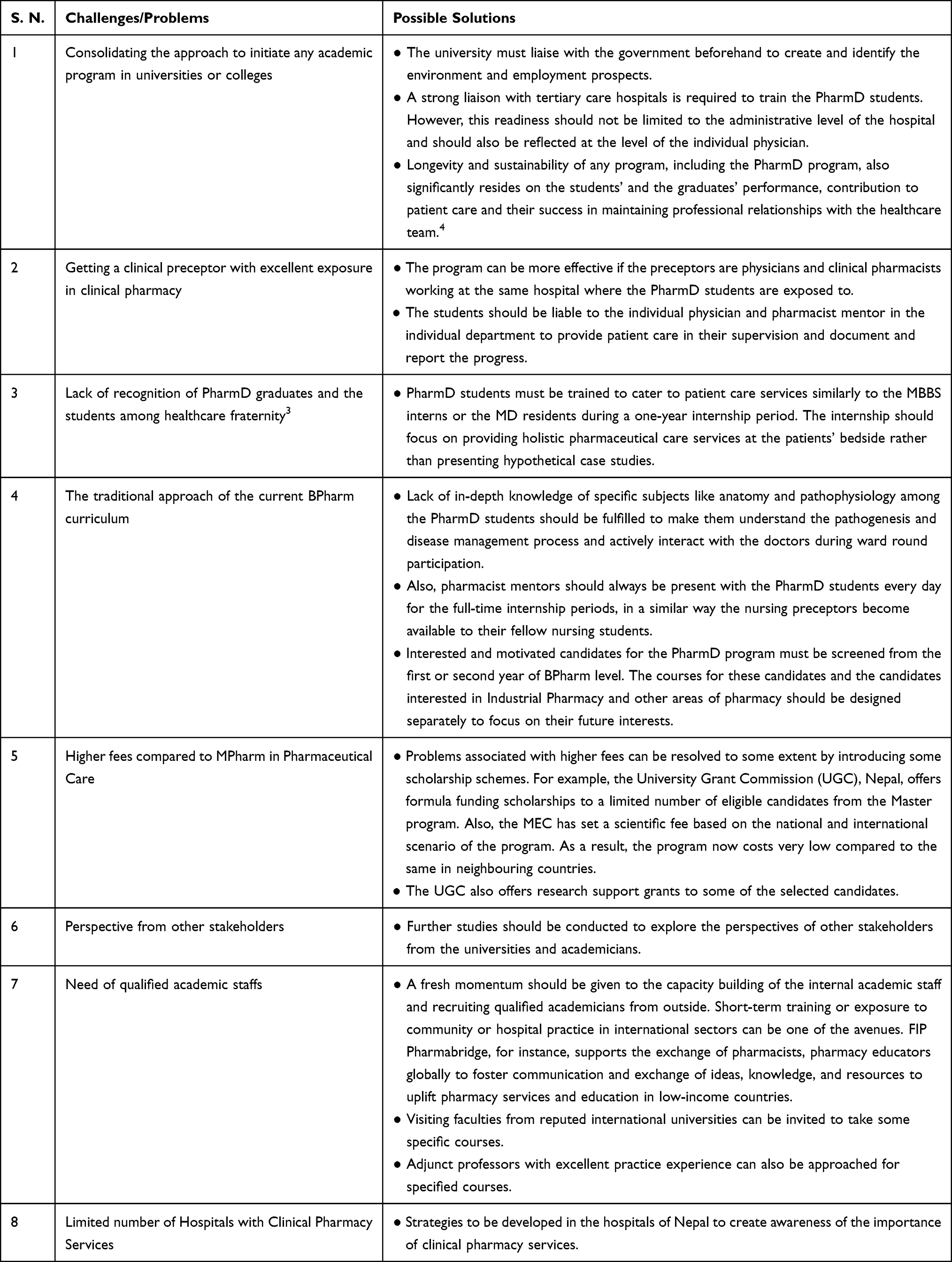 |
Table 2 Challenges and Solutions of PharmD Program |
This achievement was due to the headstrong impulse the graduates moved ahead to establish their identity amidst the challenges. The graduates from the previous batches are firmly in favour of reviving the PharmD program, which according to them, is one of the avenues to revamp the shadowed and unexplored profession of clinical pharmacy. However, they believe that the past three years’ experience of running the PharmD must be brought to the best of its use to bring it up as a sustainable program in the future. The department has greatly valued their feedback and has developed a modality to gradually address these in the reintroduction phase of the program to make the program viable and sustainable and make the impact of the program a milestone in the clinical pharmacy practice in the country.
Higher Cost
Those with PharmD qualifications might have a higher expectation for salary firstly due to the relatively higher cost of the program and the challenging nature of clinical practice jobs. There exists a difference in the tuition fees of MPham in Pharmaceutical Care and PharmD, Post Baccalaureate programs. Secondly, a PharmD graduate spends one extra year to achieve the degree in contrast to the two-year postgraduate programs in Pharmaceutical Care and Clinical Pharmacy. A higher expected salary for those with PharmD qualifications might be a barrier to entering the market later. However, this is a subjective perception that may vary among individuals.
The challenges and solutions to the PharmD program are shown in Table 2.
Conclusion
This commentary targets reflection on the challenges faced in the past and internalizing the possible remedies to the PharmD program’s reintroduction and making it sustainable. There is a realization that we need to be more patient-oriented health professionals and be a part of the health-care team. When considering education as a practice change driver, it is essential to consider various elements like infrastructure, availability of hospital-based pharmacy practice environment and exposures, employment opportunities, etc., to ensure the program sustainability. The initiation of the PharmD course by KU Department of Pharmacy had provided a roadmap for the upliftment of clinical pharmacy practice in Nepal. However, the sudden postponement of the program has created an irreparable vacuum to the same, which is, fortunately, being fulfilled by the MEC’s new decision of authorizing the university to reintroduce the program from 2022 intake. Reintroducing the program with the new vision of evidence-based clinical ward rounds in speciality units of the hospital in the guidance of a dedicated in-house clinical preceptor would help the program be sustainable in the days to come.
Acknowledgments
The authors would like to acknowledge Dr. Santosh Thapa (Jeevee Health, Nepal) and Dr. Saval Khanal (Warwick Medical School, University of Warwick, United Kingdom) for their constructive review and suggestions during preparation of the initial draft of the manuscript.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Ranjit E. Pharmacy practice in Nepal. Can J Hosp Pharm. 2016;69(6):493–500. doi:10.4212/cjhp.v69i6.1614
2. KC B, Palaian S, Khanal S, Alam K, Khan G, Budhathoki U. History and evolution of pharmaceutical education in Nepal: education versus practice. J Nepal Pharm Assoc. 2017;28(1):12–15.
3. Shrestha S, Shakya D, Palaian S. Clinical pharmacy education and practice in Nepal: a glimpse into present challenges and potential solutions. Adv Med Educ Pract. 2020;11:541. doi:10.2147/AMEP.S257351
4. KC B, Palaian S,Ibrahim MIM. PharmD education in Nepal: the challenges ahead. Am J Pharm Educ. 2011;75(2):38c. doi:10.5688/ajpe75238c
5. Law M, Bader L, Uzman N, Williams A, Bates I. The FIP Nanjing statements: shaping global pharmacy and pharmaceutical sciences education. Res Soc Admin Pharm. 2019;15(12):1472–1475. doi:10.1016/j.sapharm.2019.03.013
6. KU. Introduction to Department of Pharmacy. Kathmandu University School of Science, Nepal. Available from https://pharm.ku.edu.np/about-pharmacy. Accessed January 8, 2022.
7. Patel TC, Malhotra JV, Saseen JJ. Advancing Pharm. D. training in Egypt through a structured preceptor development program. Pharmacy. 2020;8(3):135. doi:10.3390/pharmacy8030135
8. MEC. Medical Education Commission. Seat allocation for PG; 2021. Available from: https://www.mec.gov.np/public/uploads/shares/news_notice/pg/pg_seats_2021.pdf.
9. Hospital pharmacy guideline 2072. Kathmandu (Nepal): Government of Nepal, Ministry of Health and Population. Available from: https://www.dda.gov.np/content/hospital-pharmacy-guideline-2072.
10. Shrestha S, Khatiwada AP, Gyawali S, Shankar PR, Palaian S. Overview, challenges and future prospects of drug information services in Nepal: a reflective commentary. J Multidiscip Healthc. 2020;13:287–295. doi:10.2147/JMDH.S238262
11. Devkota R, Khan GM, Alam K, Sapkota B, Devkota D. Impacts of counseling on knowledge, attitude and practice of medication use during pregnancy. BMC Pregnancy Childbirth. 2017;17(1):131. doi:10.1186/s12884-017-1316-6
12. Ghimirey A, Sapkota B, Shrestha S, Basnet N, Shankar PR, Sapkota S. Evaluation of pharmacist counseling in improving knowledge, attitude, and practice in chronic kidney disease patients. SAGE Open Med. 2013;1:2050312113516111. doi:10.1177/2050312113516111
13. Rahayu SA, Widianto S, Defi IR, Abdulah R. Role of pharmacists in the interprofessional care team for patients with chronic diseases. J Multidiscip Healthc. 2021;14:1701–1710. doi:10.2147/JMDH.S309938
14. Okoro RN, Auwal MA. Hospital pharmacists’ participation in multidisciplinary ward rounds: physicians’ perceptions and attitudes. J Pharm Res Int. 2015;5:319–327.
15. American Society of Health-System Pharmacists. ASHP statement on the pharmacist’s role in clinical pharmacokinetic monitoring. Am J Health Syst Pharm. 1998;55(16):1726–1727. doi:10.1093/ajhp/55.16.1726
16. Katoue MG. Role of pharmacists in providing parenteral nutrition support: current insights and future directions. Integr Pharm Res Pract. 2018;7:125–140. doi:10.2147/IPRP.S117118
17. Shrestha S, Danekhu K, Thapa S, Khanal S, Shankar PR. The unmet need for pharmacists as important members of the emergency department team in resource-limited settings: a case of Nepal. J Pharm Technol. 2019;35(5):219–224. doi:10.1177/8755122519850118
18. Sapkota B, Shrestha R, Chapagai S, Shakya DK, Bista P. Validation of risk of chemotherapy-induced neutropenia: experience from oncology hospital of Nepal. Cancer Manag Res. 2020;12:3751–3758. doi:10.2147/CMAR.S243916
19. Shrestha S, Shrestha S, Khanal S. Establishment of the first cancer hospital-based pharmacovigilance center in Nepal. Res Social Adm Pharm. 2018;14(11):1088–1089. doi:10.1016/j.sapharm.2018.07.017
20. Jha N, Shankar PR, Bajracharya O, Gurung SB, Singh KK. Adverse drug reaction reporting in a pharmacovigilance centre of Nepal. Australas Med J. 2012;5(5):268–271. doi:10.4066/AMJ.2012.1142
21. Shrestha S, Danekhu K, KC B, Palaian S, Ibrahim MIM. Bibliometric analysis of adverse drug reactions and pharmacovigilance research activities in Nepal. Ther Adv Drug Saf. 2020;11:2042098620922480. doi:10.1177/2042098620922480
22. Shrestha S, Shakya S, Khatiwada AP. An urgent necessity for clinical pharmacy services in cancer care in Nepal. JCO Glob Oncol. 2020;6:1392–1393. doi:10.1200/GO.20.00434
23. Khanal S, Poudel A, Sharan K, Palaian S. Oncology pharmacy practice in a teaching hospital in Nepal. J Oncol Pharm Pract. 2010;16(2):75–79. doi:10.1177/1078155209337662
24. Shrestha S, Shrestha S, Palaian S. Can clinical pharmacists bridge a gap between medical oncologists and patients in resource-limited oncology settings? An experience in Nepal. J Oncol Pharm Pract. 2018;25(3):765–768. doi:10.1177/1078155218784734
25. Shrestha S, Shrestha S, Khanal S. Polypharmacy in elderly cancer patients: challenges and the way clinical pharmacists can contribute in resource-limited settings. Aging Med. 2019;2(1):42–49. doi:10.1002/agm2.12051
26. Bista D, Saha A, Mishra P, Palaian S, Shankar PR. Impact of educational intervention on the pattern and incidence of potential drug-drug interactions in Nepal. Pharm Pract (Granada). 2009;7(4):242. doi:10.4321/S1886-36552009000400008
27. Bista D, Saha A, Mishra P, Palaian S, Shankar P. Pattern of potential drug-drug interactions in the intensive care unit of a teaching hospital in Nepal: a pilot study. J Clin Diagn Res. 2009;3(4):1713–1716.
28. Sharma S, Chhetri HP, Alam K. A study of potential drug-drug interactions among hospitalized cardiac patients in a teaching hospital in Western Nepal. Indian J Pharmacol. 2014;46(2):152–156. doi:10.4103/0253-7613.129303
29. Sapkota B, Gupta GK, Mainali D. Impact of intervention on healthcare waste management practices in a tertiary care governmental hospital of Nepal. BMC Public Health. 2014;14(1):1–8. doi:10.1186/1471-2458-14-1005
30. Sapkota B, Gupta GK, Mainali D, Shrestha N. Development and implementation of healthcare waste management policy at Civil Service Hospital, Nepal. J Pharm Pract Res. 2015;45(1):57–63. doi:10.1002/jppr.1054
31. Shrestha S, Sharma S, Bhasima R, Kunwor P, Adhikari B, Sapkota B. Impact of an educational intervention on pharmacovigilance knowledge and attitudes among health professionals in a Nepal cancer hospital. BMC Med Educ. 2020;20:1–10. doi:10.1186/s12909-020-02084-7
32. Poudel A, Khanal S, Alam K, Palaian S. Perception of Nepalese community pharmacists towards patient counseling and continuing pharmacy education program: a multicentric study. J Clin Diagn Res. 2009;3(2):1408–1413.
33. Khatiwada AP, Shakya S, Shrestha S. Paradigm shift of drug information centers during the COVID-19 pandemic. Drugs Ther Perspect. 2020;36(9):389–395. doi:10.1007/s40267-020-00757-3
34. Khatiwada AP, Shrestha S. Pharmacy patronage: identifying the roles of Nepalese pharmacists in tackling COVID-19. J Pure Appl Microbiol. 2020;14(Suppl 1):937–943. doi:10.22207/JPAM.14.SPL1.31
35. Shrestha S, Khatri J, Shakya S, et al. Adverse events related to COVID-19 vaccines: the need to strengthen pharmacovigilance monitoring systems. Drugs Ther Perspect. 2021;37:1–7.
36. Fathelrahman AI, Ibrahim MIM, Wertheimer AI. Medical devices for pharmacy and other healthcare professions. 2021.
37. Balakrishnan R, Ravichandran R, Dillibatcha J, Ravi A, Sam N, Nuthalapati R. Clinical pharmacists’ role in paediatric patients’ medical care. Int J Contemp Pediatr. 2020;7(12):2416–2420. doi:10.18203/2349-3291.ijcp20205110
38. Deshpande PR, Vantipalli R, Chaitanya Lakshmi CH, et al. Clinical pharmacists: the major support to Indian healthcare system in near future. J Pharm Bioallied Sci. 2015;7(3):161–174. doi:10.4103/0975-7406.160005
39. Krishnamoorthy G, Vadlapatla K, Varghese R. A review on Pharm. D education in India. PharmaTutor. 2014;2(4):144–148.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.