")
Back to Journals » Clinical Interventions in Aging » Volume 14
Refractory healing after surgical therapy of osteonecrosis of the jaw: associated risk factors in aged patients
Authors Kim JY, Song HC, Jee HG
Received 4 January 2019
Accepted for publication 8 March 2019
Published 6 May 2019 Volume 2019:14 Pages 797—804
DOI https://doi.org/10.2147/CIA.S200455
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Ji-Youn Kim,1 Hyun Chul Song,1 Hyeon-Gun Jee2
1Division of Oral & Maxillofacial Surgery, Department of Dentistry, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 2Healthcare Innovation Park, Seoul National University Bundang Hospital, Seongnam, Republic of Korea
Purpose: Osteonecrosis of the jaw (ONJ), both medication-related and non medication-related, mainly occurs in aged patients. It needs surgical intervention. Refractory healing after an operation of ONJ can significantly lower the quality of life of elderly patients. The purpose of this study was to determine risk factors associated with refractory healing in aged patients.
Patients and methods: We performed a retrospective study of ONJ in aged patients who underwent surgical treatments in a single institute during a 12-year period. Multiple logistic regression analysis was used to determine independent risk factors associated with refractory healing.
Results: A total of 122 patients were included. Of them, 25 patients were identified as the refractory group and 97 patients as the control group. Diabetes mellitus (DM) (AOR=5.03, 95% CI: 1.74–14.52) and glucocorticoid administration (AOR=7.97, 95% CI: 2.52–25.23) were found to be significant risk factors for refractory healing of ONJ.
Conclusion: DM and medication of glucocorticoid might be risk factors for refractory healing of ONJ.
Keywords: osteomyelitis, osteonecrosis, medication-related osteonecrosis of the jaw, surgical therapy, refractory healing, diabetes mellitus, glucocorticoid
Introduction
The average age of the world population is increasing.1 The number of elderly patients who have general complex health problems is also on the rise.2 In dentistry, especially in oral and maxillofacial surgery, aging patients require special consideration for dental treatment.2 High age and comorbid chronic diseases are risk factors of bone infection.3 As people age, they develop multiple health ailments that can lead to polypharmacy which may cause unexpected side effects.4
Osteomyelitis is a common progressive inflammatory disease with various causes such as medications, odontogenic sources, radiation, and traumas, and often the cause is unrevealed.5,6 Osteomyelitis results in osteonecrosis of the jaw (ONJ) when advanced.6 As a widely studied subtype of ONJ, medication-related osteonecrosis of the jaw (MRONJ) is diagnosed as the exposed bone in the maxillofacial region over a period of 8 weeks, current or previous treatment with antiresorptive or antiangiogenic agents, and no history of radiation therapy to the jaws.7,8 Medications that are associated with MRONJ include bisphosphonate, denosumab, sunitinib, bevacizumab, or temsirolimus.9,10 The prevalence of ONJ, including both MRONJ and those not related to MRONJ (non-MRONJ), is high in elderly patients,11 and the onset and progress are influenced by patients’ systemic diseases and consistent medications.12 Regardless of the cause, surgical interventions at varying degrees are usually indicated for the treatment of ONJ.13–15
Refractory healing of ONJ after an operation can remarkably lower the quality of life of elderly patients.11 There is also a possibility of additional operation under general anesthesia and a longer period of admission. Additional resective surgery at the jaw can also induce more severe dysmasesis, indigestion, general weakness, esthetic problems, and financial problems. Even though elderly patients are more vulnerable to above-mentioned problems than younger patients,16 their progression after the operation of ONJ, especially refractory healing, has been rarely studied.
In this study, patients were divided into two groups (refractory group and control group) according to their progression after the operation of ONJ. Systemic diseases and medications that could affect treatment progression were examined for the two groups. Results of this study may aid clinicians to provide better clinical practice to aging patients.
Methods
Patients and data collection
A retrospective study was performed by analyzing digital medical files of patients diagnosed with either osteomyelitis, inflammatory jawbone, or drug-induced osteonecrosis who were treated in the Division of Oral & Maxillofacial Surgery of St. Vincent’s Hospital during a 12-year period (from January 2005 to December 2016). Inclusion criteria were patients with an age of 65 and above diagnosed as ONJ who underwent surgical treatments such as debridement, sequestrectomy, saucerization, and mandibulectomy11 with pre- and post-operative antibiotics medication, and follow-up care in a single institute. Exclusion criteria were: 1) follow-up loss before the first surgical treatment, 2) simple alveolar osteitis without osteonecrosis or sequestrum, 3) MRONJ without exposed necrotic bone such as at-risk or stage 0 MRONJ,13 4) osteoradionecrosis of the jaw due to the exposure to radiation therapy, or 5) incomplete medical records.
Patients were identified into the refractory group and the control group. The refractory group was defined as patients with refractory wound healing who showed partial healing (when a reduction was found in the symptoms and signs of ONJ) or no healing (when symptoms and signs were similar to those before surgery) after the first surgery.15 The control group was defined as patients with complete healing without any reoperation. Patients’ demographic data, MRONJ stages, systemic disease status, and medication status (administration of glucocorticoids, methotrexate and other immunosuppressant agents for systemic disease treatment) were retrieved, reviewed, and analyzed by reviewing clinical medical records. This study was reviewed and approved by the Institutional Review Board (IRB) of St. Vincent’s Hospital, the Catholic University of Korea (IRB approval number: VC18RESI0146) and was carried out in accordance with the latest version of the Declaration of Helsinki. Informed consent was exempted because the study involved identification-masked data acquired during routine clinical care.
Data analysis
Statistical data analysis was performed with IBM® SPSS® Statistics version 21.0 (SPSS, Chicago, IL, USA). Initially, bivariate logistic regression analysis was carried out to screen variables to be used for multivariate analysis and those with p-values ≤0.2 were selected. In a multivariate logistic regression for final statistical analysis, adjusted odds ratio (AOR) and 95% confidence interval (CI) were calculated. Hosmer-Lemeshow test was performed to assure the fit of the logistic regression model. p-values of ≤0.05 were considered statistically significant for the multivariate analysis.
Results
Demographic characteristic of patients
A total of 122 patients were included in this study. Among them, 25 patients were identified as the refractory group and 97 patients as the control group. In the refractory group, 23 patients showed partial healing after the first operation and complete healing after reoperation(s). Two patients showed no healing after the first operation. The average follow-up period was 12.83±16.73 months (refractory group 14.14±15.90 months and control group 12.49±17.0 months). The mean age of all patients was 76.75±6.50 years. The mean age of the refractory group (75.92±5.87 years) was similar to that of the control group (76.97±6.50 years). Most patients were females (105, 86.1%). Regarding the subtype of ONJ, approximately two-thirds of the patients (79, 64.8%) were diagnosed as MRONJ. The percentage of MRONJ patients was higher in the refractory group (80.0%) than that in the control group (60.8%). However, in binary logistic regression analyses, gender, and ONJ subtype did not show statistically significant association with refractory healing (Table 1).
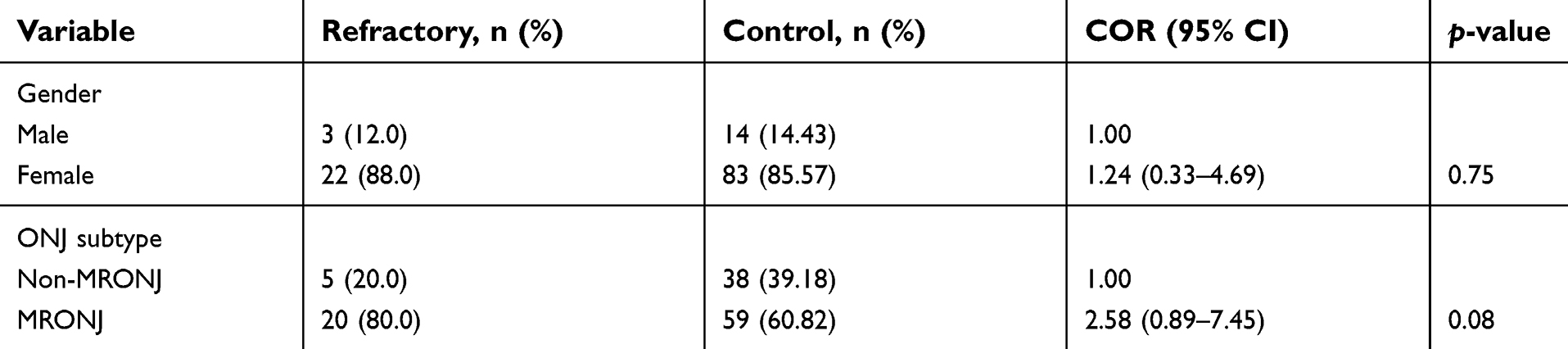 | Table 1 Demographic characteristics of the patients |
Systemic diseases associated with refractory healing of ONJ
We sought to determine systemic diseases associated with refractory healing of ONJ. A total of 21 different types of diseases were present in our patients. The average number of systemic diseases per patient was 2.83±1.63 (0–8). Systemic diseases analyzed were osteoporosis, cardiovascular diseases, pulmonary diseases, hyperlipidemia, neuropsychological diseases, cognitive disorders, ophthalmic disorders, spinal diseases, gastrointestinal diseases, degenerative arthritis, rheumatoid arthritis, diabetes mellitus (DM), and urogenital diseases. Systemic diseases excluded from statistical analyses due to insufficient sample size were renal diseases (n=4), adrenal insufficiency (n=3), thyroid diseases (n=3),cerebrovascular diseases (n=2), iatrogenic Cushing’s syndrome (n=2), thyroid cancer (n=2), colon cancer (n=2), and multiple myeloma (n=1). All 25 DM patients had type 2 disease. In binary logistic regression analyses, rheumatoid arthritis and DM were systemic diseases which had statistically significant associations with refractory healing (Table 2).
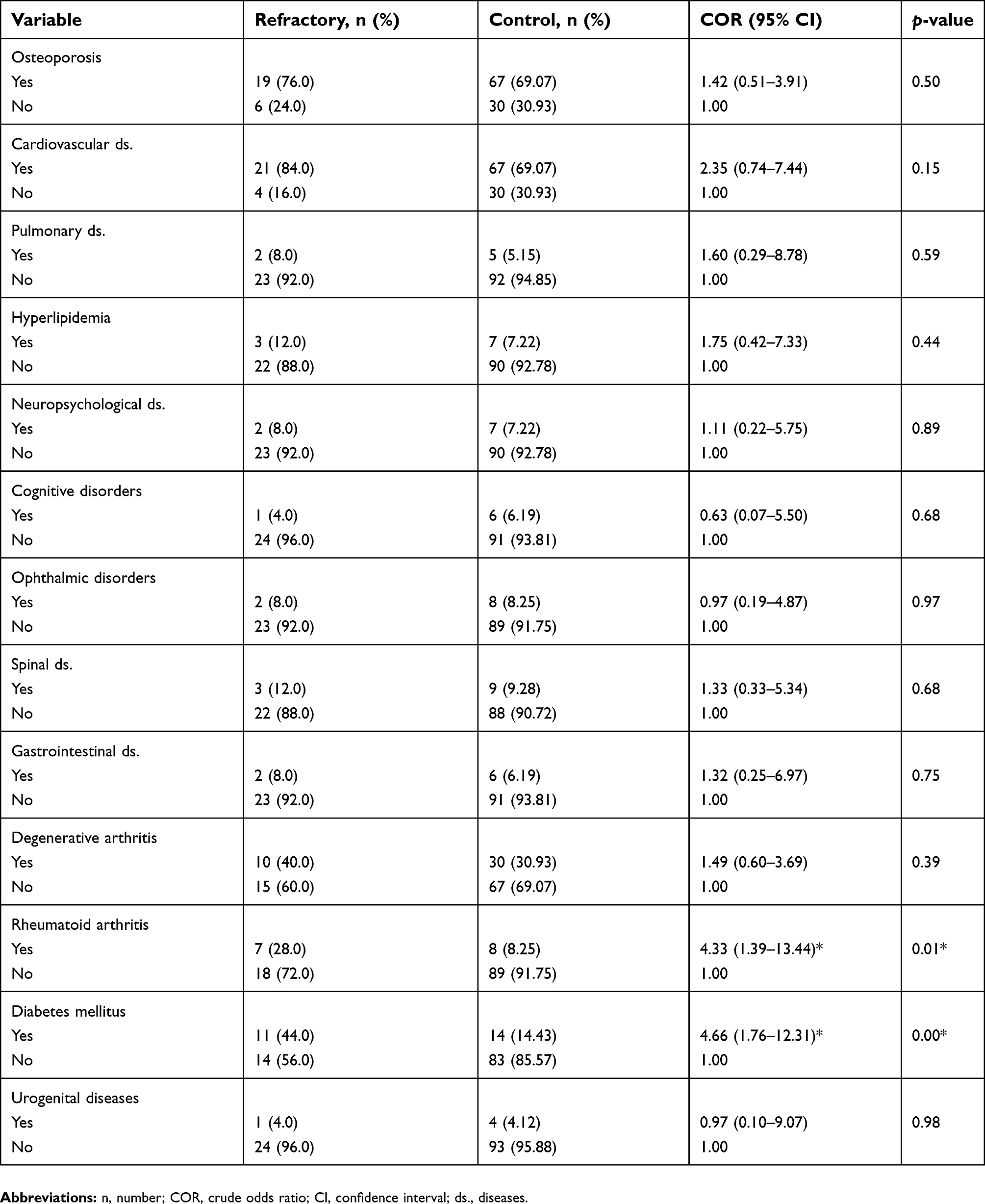 | Table 2 Systemic diseases associated with refractory healing |
Additionally, bisphosphonate administration data were analyzed in osteoporosis patients (n=86). In 76 osteoporosis patients with bisphosphonate administration history, 18 patients showed refractory healing (23.7%). In 10 non-bisphosphonate administrated osteoporosis patients, one patient showed refractory healing (10.0%). However, in binary logistic regression analyses, no statistically significant association with refractory healing was observed with bisphosphonate administration (data not shown).
Medications associated with refractory healing
Bivariate analysis was performed to determine the association of medications known to delay surgical wound healing.17,18 Medication-taking history of methotrexate, glucocorticoids, or other immunomodulating drugs (adalimumab, lenalidomide) was reviewed and analyzed. All patients (7 patients) who had taken methotrexate used it for treating rheumatoid arthritis. Glucocorticoids were taken for treating degenerative arthritis, rheumatoid arthritis, spinal diseases, adrenal insufficiency, or multiple myeloma. Immunomodulating drugs were taken for treating rheumatoid arthritis (n=2) or multiple myeloma (n=1) were excluded from statistical analysis because of the small number of patients. All bisphosphonate administrated ONJ patients were diagnosed as MRONJ,12 and therefore bisphosphonate use was not analyzed separately. In binary logistic regression analyses, methotrexate administration and glucocorticoid administration showed statistically significant associations with refractory healing (Table 3).
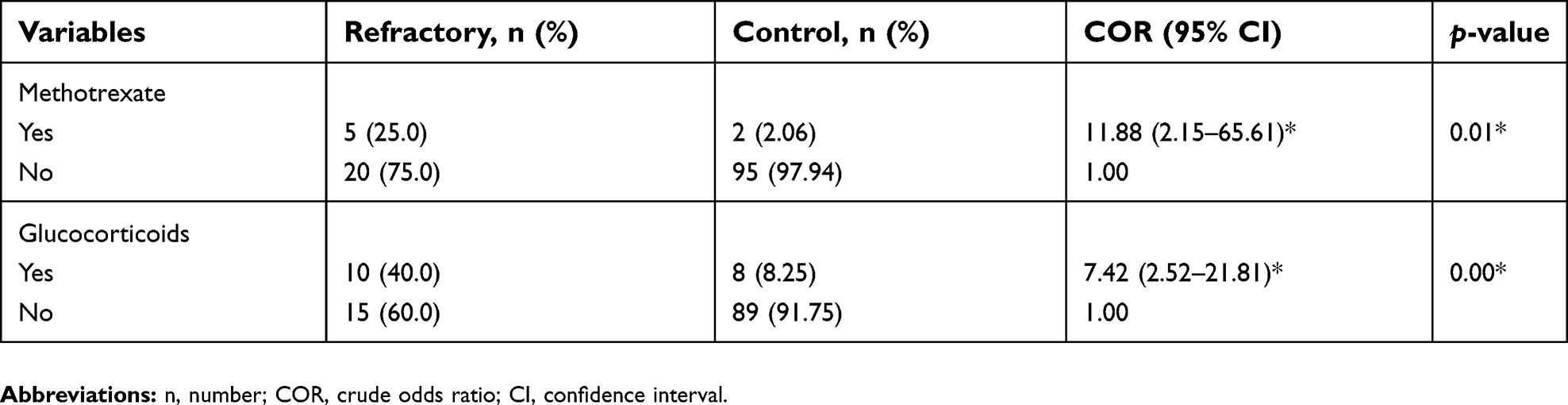 | Table 3 Medications associated with refractory healing |
Multivariate analysis of factors associated with refractory healing of ONJ
Variables that showed p-value ≤0.2 in bivariate logistic regression analysis were entered into multivariate logistic regression analysis (Table 4). DM patients were five times more likely to have refractory healing after treatment of osteonecrosis than non-DM patients (AOR =5.03, 95% CI: 1.74–14.52). Patients who had taken glucocorticoids were about eight times more likely to have refractory healing after treatment of ONJ than those not had taken glucocorticoids (AOR =7.97, 95% CI: 2.52–25.23).
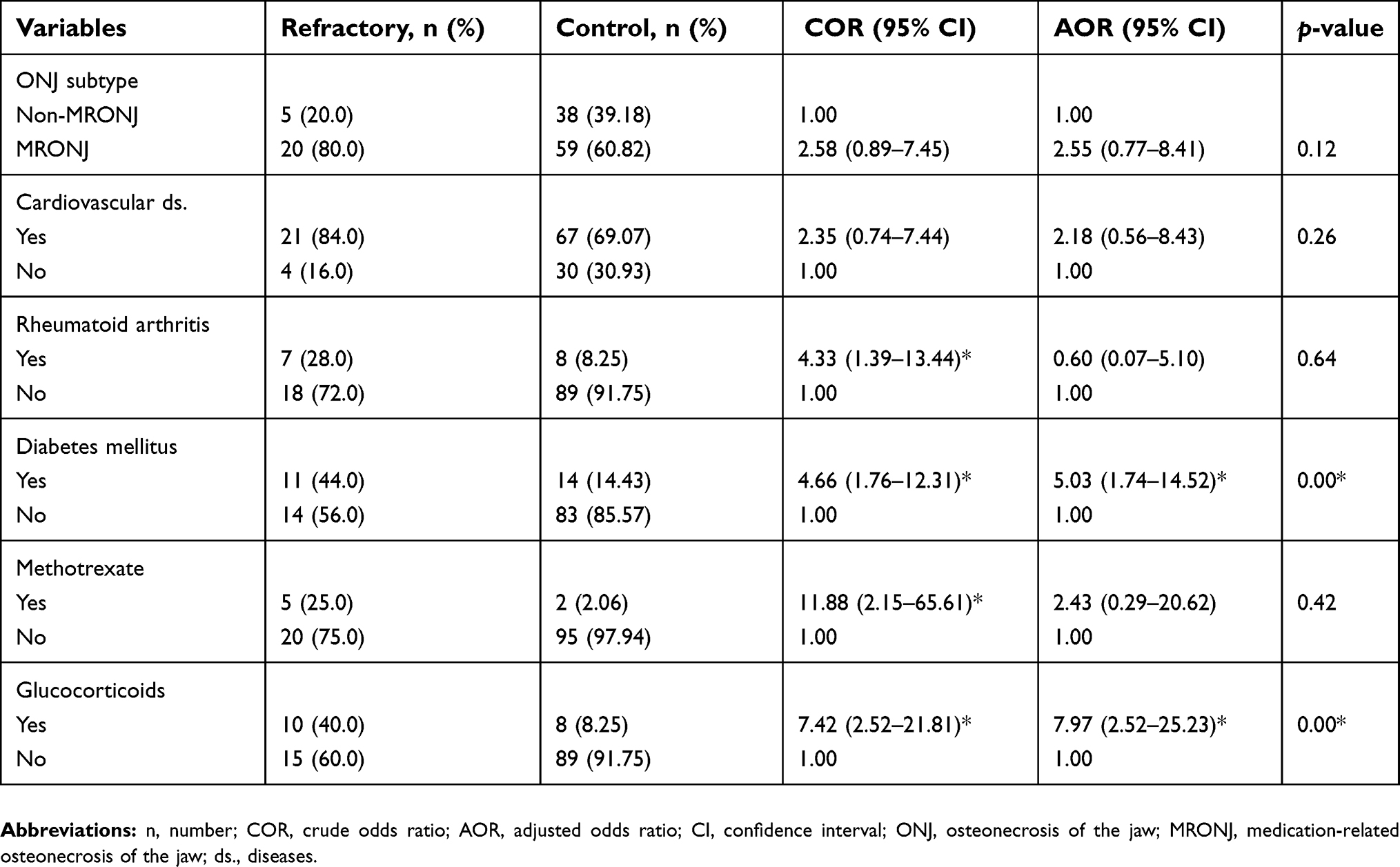 | Table 4 Multivariate analysis for selected variables associated with refractory healing of osteonecrosis |
Discussion
Risk factors for the occurrence of ONJ have been reported to be old age, bisphosphonate medication (especially when intravenously administered), DM, cancer chemotherapy, glucocorticoids medications, cardiovascular diseases, radiation therapy, bone marrow transplantation, anemia, metastasis, antiangiogenic medication, and rheumatoid arthritis.11,15,19 However, few studies have studied for refractory healing of ONJ after surgical treatment. Among the systemic risk factors for the occurrence of ONJ mentioned above, out results of logistic regression analysis showed that refractory wound healing after surgical intervention was increasingly manifested in DM patients and glucocorticoid administered patients.
DM is one of the medical comorbidities and a previously reported risk factor for the occurrence of ONJ.6,12 DM significantly increased the risk of developing MRONJ by 2.78- to 6.70- fold, although there were also studies reporting no significant association between the two.20–23 In DM patients, bone turnover and remodeling are altered, and increased insulin levels can also affect bone and elevate levels of advanced glycation end products causing complex alterations of vitamin D-related bone regulation.24,25 Also, high blood glucose level can inhibit osteoclast differentiation and function and induce osteoblast and osteocyte apoptosis.26 DM is also related to altered angiogenesis, macro-microvascular changes, and endothelial damages that can lead to the development of osteonecrosis.27 Also, altered immune responses in DM patients could increase the risk of chronic infection.25 In agreement with these reports, DM patients were more likely to have refractory healing after surgical treatment of ONJ in this study.
Glucocorticoid is a commonly used medication to treat autoimmune diseases such as rheumatoid arthritis and systemic lupus erythematous as well as chronic inflammatory diseases such as degenerative osteoarthritis.28,29 Systemic glucocorticoids play an integral role in the management of many inflammatory conditions by upregulating the transcription of anti-inflammatory genes or by downregulating the transcription of inflammatory genes.30 However, glucocorticoids are also associated with serious risks, including osteoporosis, fractures, and osteonecrosis.30 Glucocorticoids can stimulate osteoclastic activity initially, followed by a decrease in bone formation by suppressing osteoblastic activity. They can promote apoptosis of osteoblasts and osteocytes, possibly leading to the osteonecrotic condition of bony tissue.31 In addition, many previous studies have reported that glucocorticoids are associated with an increased risk of MRONJ development.32 In this study, patients who had taken glucocorticoids were also eight times more likely to refractory healing after surgical treatment of ONJ than patients who had not taken glucocorticoids. Thus, glucocorticoids might be a key risk factor for refractory bone healing after the operation of ONJ.
We report that cardiovascular diseases and rheumatoid arthritis which are representative risk factors for the occurrence of ONJ13,19 are not risk factors for refractory healing. Although rheumatoid arthritis was not a significant risk factor for ONJ refractory healing, glucocorticoid administration for treatment of rheumatoid arthritis showed statistical significance. Regarding bisphosphonate treatment, it has been reported that the risk of developing MRONJ appears to increase when the duration of therapy exceeds 3 years for patients receiving high dosage intravenous bisphosphonate.33,34 However, when MRONJ patients in this study were considered, there was no significant association of route or type of bisphosphonate applications, exposed duration of bisphosphonate or stage of MRONJ with refractory healing in binary logistic regression analyses (Table S1). Further study on risk factors of refractory healing with a larger size of bisphosphonate medicated malignant patients may provide additional information.
In this study, systemic risk factors associated refractory healing of ONJ in aged patients were analyzed and discussed. Results of this study suggest that glucocorticoid-taking patients and DM patients have a high risk of refractory healing after surgical treatment of ONJ. Clinicians should be aware of these clinical points for better clinical interventions in this aging society.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ito R, Kubota K, Inui A, et al. Oral-maxillofacial trauma of a geriatric population in a super-ageing country. Dent Traumatol. 2017;33(6):433–437. doi:10.1111/edt.12371
2. Sato Y, Kitagawa N, Isobe A. Implant treatment in ultra-aged society. Jpn Dent Sci Rev. 2018;54(2):45–51. doi:10.1016/j.jdsr.2017.12.002
3. Lee F-H, Shen P-C, Jou IM, Li C-Y, Hsieh J-L. A population-based 16-year study on the risk factors of surgical site infection in patients after bone grafting: a cross-sectional study in Taiwan. Medicine. 2015;94(47):e2034. doi:10.1097/MD.0000000000000874
4. Singh ML, Papas A. Oral implications of polypharmacy in the elderly. Dent Clin North Am. 2014;58(4):783–796. doi:10.1016/j.cden.2014.07.004
5. Hong SO, Lee CY, Jung J, Kim DY, Walter C, Kwon YD. A retrospective study of osteomyelitis and osteonecrosis of the jaws and its etiologic implication of bisphosphonate in Asians. Clin Oral Investig.
6. Baur DA, Altay MA, Flores-Hidalgo A, Ort Y, Quereshy FA. Chronic osteomyelitis of the mandible: diagnosis and management–an institution’s experience over 7 years. J Oral Maxillofac Surg. 2015;73(4):655–665. doi:10.1016/j.joms.2014.10.017
7. Manzon L, Ettorre E, Viscogliosi G, et al. Bisphosphonate therapy and osteonecrosis of the jaw complicated with a temporal abscess in an elderly woman with rheumatoid arthritis: a case report. Clin Interv Aging. 2014;9:1409–1413. doi:10.2147/CIA.S67726
8. Ramaglia L, Guida A, Iorio-Siciliano V, Cuozzo A, Blasi A, Sculean A. Stage-specific therapeutic strategies of medication-related osteonecrosis of the jaws: a systematic review and meta-analysis of the drug suspension protocol. Clin Oral Investig. 2018;22(2):597–615. doi:10.1007/s00784-017-2325-6
9. Guimaraes EP, Pedreira FR, Jham BC, de Carli ML, Pereira AA, Hanemann JA Clinical management of suppurative osteomyelitis, bisphosphonate-related osteonecrosis, and osteoradionecrosis: report of three cases and review of the literature. Case Rep Dent. 2013;2013:402096.
10. Alsehimy M, Al-Dharrab A. Risk factor assessment of osteomyelitis of the jaws in the Saudi population: a 10-year retrospective study. Egypt J Oral Maxillofac Surg. 2012;3(1):23–29. doi:10.1097/01.OMX.0000412879.34163.b4
11. Kim HY, Lee SJ, Kim SM, et al. Extensive surgical procedures result in better treatment outcomes for bisphosphonate-related osteonecrosis of the jaw in patients with osteoporosis. J Oral Maxillofac Surg. 2017;75(7):1404–1413. doi:10.1016/j.joms.2016.12.014
12. McGowan K, McGowan T, Ivanovski S. Risk factors for medication-related osteonecrosis of the jaws: A systematic review. Oral Dis. 2018;24(4):527–536. doi:10.1111/odi.12708
13. Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw–2014 update. J Oral Maxillofac Surg. 2014;72(10):1938–1956. doi:10.1016/j.joms.2014.04.031
14. Pincus DJ, Armstrong MB, Thaller SR. Osteomyelitis of the craniofacial skeleton. Semin Plast Surg. 2009;23(2):73–79. doi:10.1055/s-0029-1214159
15. Lopes RN, Rabelo GD, Rocha AC, Carvalho PA, Alves FA. Surgical therapy for bisphosphonate-related osteonecrosis of the jaw: six-year experience of a single institution. J Oral Maxillofac Surg. 2015;73(7):1288–1295. doi:10.1016/j.joms.2015.01.008
16. Mo L, Ding D, Pu S-Y, et al. Patients aged 80 years or older are encountered more potentially inappropriate medication use. Chin Med J. 2016;129(1):22–27. doi:10.4103/0366-6999.172558
17. Busti AJ, Hooper JS, Amaya CJ, Kazi S. Effects of perioperative antiinflammatory and immunomodulating therapy on surgical wound healing. Pharmacotherapy. 2012;25(11):1566–1591. doi:10.1592/phco.2005.25.11.1566
18. Jain A, Witbreuk M, Ball C, Nanchahal J. Influence of steroids and methotrexate on wound complications after elective rheumatoid hand and wrist surgery. J Hand Surg Am. 2002;27(3):449–455.
19. Yamazaki T, Yamori M, Tanaka S, et al. Risk factors and indices of osteomyelitis of the jaw in osteoporosis patients: results from a hospital-based cohort study in Japan. PLoS One. 2013;8(11):e79376–e79376. doi:10.1371/journal.pone.0079376
20. Molcho S, Peer A, Berg T, Futerman B, Khamaisi M. Diabetes microvascular disease and the risk for bisphosphonate-related osteonecrosis of the jaw: a single center study. J Clin Endocrinol Metab. 2013;98(11):E1807–1812. doi:10.1210/jc.2013-2434
21. Kajizono M, Sada H, Sugiura Y, et al. Incidence and risk factors of osteonecrosis of the jaw in advanced cancer patients after treatment with zoledronic acid or denosumab: a retrospective cohort study. Biol Pharm Bull. 2015;38(12):1850–1855. doi:10.1248/bpb.b15-00385
22. Paek SJ, Park WJ, Shin HS, Choi MG, Kwon KH, Choi EJ. Diseases having an influence on inhibition of angiogenesis as risk factors of osteonecrosis of the jaw. J Korean Assoc Oral Maxillofac Surg. 2016;42(5):271–277. doi:10.5125/jkaoms.2016.42.5.271
23. Yamazaki T, Yamori M, Yamamoto K, et al. Risk of osteomyelitis of the jaw induced by oral bisphosphonates in patients taking medications for osteoporosis: a hospital-based cohort study in Japan. Bone. 2012;51(5):882–887. doi:10.1016/j.bone.2012.08.115
24. Isidro ML, Ruano B. Bone disease in diabetes. Curr Diabetes Rev. 2010;6(3):144–155.
25. Peer A, Khamaisi M. Diabetes as a risk factor for medication-related osteonecrosis of the jaw. J Dent Res. 2015;94(2):252–260. doi:10.1177/0022034514560768
26. Berti-Couto SA, Vasconcelos AC, Iglesias JE, Figueiredo MA, Salum FG, Cherubini K. Diabetes mellitus and corticotherapy as risk factors for alendronate-related osteonecrosis of the jaws: a study in Wistar rats. Head Neck. 2014;36(1):84–93. doi:10.1002/hed.23260
27. Favus MJ. Diabetes and the risk of osteonecrosis of the jaw. J Clin Endocrinol Metab. 2007;92(3):817–818. doi:10.1210/jc.2007-0098
28. Chiu CT, Chiang WF, Chuang CY, Chang SW. Resolution of oral bisphosphonate and steroid-related osteonecrosis of the jaw–a serial case analysis. J Oral Maxillofac Surg. 2010;68(5):1055–1063. doi:10.1016/j.joms.2009.12.030
29. Wieland HA, Michaelis M, Kirschbaum BJ, Rudolphi KA. Osteoarthritis - an untreatable disease? Nat Rev Drug Discov. 2005;4(4):331–344. doi:10.1038/nrd1693
30. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. doi:10.1186/1710-1492-9-30
31. Weinstein RS, Jilka RL, Parfitt AM, Manolagas SC. Inhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on bone. J Clin Invest. 1998;102(2):274–282. doi:10.1172/JCI2799
32. Saad F, Brown JE, Van Poznak C, et al. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann Oncol. 2012;23(5):1341–1347. doi:10.1093/annonc/mdr435
33. Khosla S, Burr D, Cauley J, et al. Bisphosphonate-associated osteonecrosis of the jaw: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2007;22(10):1479–1491. doi:10.1359/jbmr.0707onj
34. Vestergaard P, Schwartz K, Rejnmark L, Mosekilde L, Pinholt EM. Oral bisphosphonate use increases the risk for inflammatory jaw disease: a cohort study. J Oral Maxillofac Surg. 2012;70(4):821–829. doi:10.1016/j.joms.2011.02.093
Supplementary material
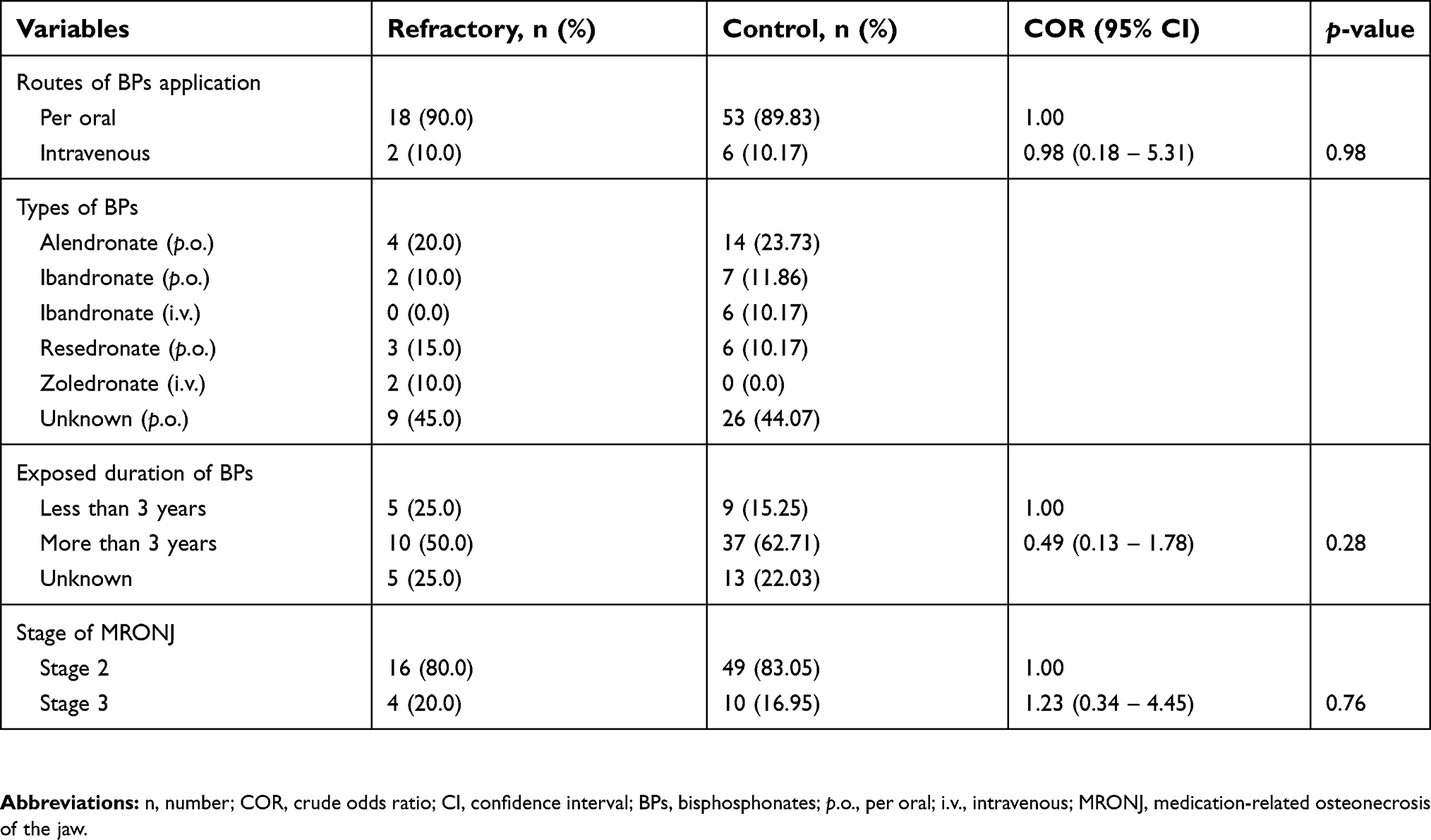 | Table S1 Refractory healing in MRONJ patients |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.