")
Back to Journals » Clinical Ophthalmology » Volume 13
Refractive errors among Saudi college students and associated risk factors
Authors Alsaif BA, Aljindan MY, Alrammah HM, Almulla MO, Alshahrani SS
Received 2 November 2018
Accepted for publication 14 January 2019
Published 27 February 2019 Volume 2019:13 Pages 437—443
DOI https://doi.org/10.2147/OPTH.S193213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bayan A Alsaif,1 Mohanna Y Aljindan,2 Hanan M Alrammah,1 Malak O Almulla,1 Saad S Alshahrani3
1College of Medicine, King Fahad Hospital of the University, Imam Abdulrahamn Bin Fasial University, Khobar, Saudi Arabia; 2Department of Ophthalmology, King Fahad Hospital of the University, Imam Abdulrahman Bin Fasial University, Khobar, Saudi Arabia; 3Epidemiology Department, King Fahd Specialist Hospital, Dammam, Saudi Arabia
Objectives: To determine the prevalence of refractive errors among freshman students of Imam Abdulrahman Bin Faisal University (IAU), and to examine the relationship of near-work activities and outdoor activities with refractive errors.
Methods: A cross-sectional study of 338 freshman students of IAU (162 males, 176 females) was carried out. Students were selected using a simple random sampling technique. Eye examination was done including non-cycloplegic autorefraction for determining the refractive error status. Myopia was defined as spherical equivalent refraction (SER) ≤-0.75 diopters (D), and it was further divided into low myopia (SER from -0.75 D to -2.99 D), moderate myopia (SER from -3.00 to -5.99 D), and high myopia (SER ≤-6.00 D). Hyperopia was defined as SER ≥1.00 D and emmetropia as having an SER value between that of low myopia and hyperopia. SER was calculated as sphere + 1/2 cylinder. A questionnaire detailed on activities was completed by participants.
Results: Myopia was found in 47.9% of the students (95% CI 42.7%–53.3%). The most prevalent type of myopia was low myopia (66.7%; 95% CI 59.1%–73.5%). Hyperopia and emmetropia were found in 6.5% (95% CI 4.3%–9.7%) and 45.6% (95% CI 40.3%–50.9%) of the students, respectively. Parental myopia was significantly associated with the myopic status of the students (P=0.007, Fisher’s exact test). About 6% of myopic students had a history of myopia in both parents. In addition, both parents had a history of myopia in 1.9% of emmetropic students, whereas such an association was absent in the hyperopic students. Refractive error type in both genders was not significantly predicted by the activity type.
Conclusion: Although the different types of activities did not predict the types of refractive errors, the high prevalence of myopia among the college students at this age requires further studies to explore more about the clinical characteristics and risk factors of the disease.
Keywords: near-work, outdoor activity, college students, axial length, keratometry, anterior chamber depth, myopia, biometry
Introduction
Uncorrected refractive errors are estimated to be the second most common cause of blindness worldwide in 2010.1 They pose an economical burden in terms of contribution to productivity loss with an estimated cost of 121.4 billion international dollars (I$).2 The global prevalence of myopia and high myopia was estimated at 22.9% and 2.7%, respectively, in 2000.3 These percentages increased in 2010 for myopia and high myopia reaching up to 28.3% and 4%, respectively.3 The growing prevalence rate is concerning, warranting preventive measures to deal with its progression and possible sight-threatening complications.
The global distribution of myopia varies substantially with the highest figures being reported from some East Asian countries.4–6 Although genetics play a role, they alone do not explain the increasing prevalence among younger generations or the higher prevalence among higher education students.7 Hence, environmental factors are believed to have a major role in myopia etiology. Some studies have found myopic progression to be less among those who have spent more time engaging in outdoor activities.8–11 A randomized clinical trial study found a significant reduction in myopia progression in the intervention group with more outdoor activity compared to the control group.12 Another study found a reduced incidence rate of myopia with outdoor activity.13 Results of different studies show contradicting results regarding the association of myopia with near-work activities. However, a meta-analysis study concluded that myopia is associated with near-work activities.14 Many studies documenting the prevalence of myopia and patterns of increase in prevalence throughout different periods of time and for different age groups mostly covered Asian and Western countries. Unfortunately, there is scarcity in studies addressing myopia prevalence in the Middle East. A meta-analysis study revealed that although the number of cases of blindness due to cataract, which is the prime reason for blindness, has decreased from 1990 to 2010 in the Middle East and North Africa, the cases of blindness due to uncorrected refractive errors have on the other hand increased.15 Furthermore, uncorrected refractive errors together with cataract were the highest contributors to moderate or severe visual impairment in 2010.15 However, the study provided that information form Saudi Arabia is scarce. A study done in Saudi Arabia has found that in Aljouf Province, refractive errors are the only cause of visual impairment among primary health care attendants aged <30 years.16 A study of two different medical colleges from Hail Province and Riyadh Province has found the prevalence of myopia to be 53.5%.17 The prevalence of refractive errors was 9.8% among children aged 10–13 years in primary schools of Qassim Province, and 47.5% among the students aged 12–14 years from Alhassa region.18,19
Refractive status has been commonly assumed to be best evaluated for epidemiological reports, among the age at finishing secondary schooling (around 18 years of age), as it is believed that myopia most likely stabilizes at this age.20 In this study, our aim was to find out the prevalence of refractive errors among health path freshman students of Imam Abdulrahman Bin Fisal university (IAU), Dammam, Saudi Arabia, and to study the relationship between some risk factors and refractive error status.
Materials and methods
Settings
This is a cross-sectional study conducted in King Fahd University Hospital (KFUH) which is affiliated to Imam Abdulrahman bin Faisal University (IAU). It is located in Al-Khobar, a large city with a population of 573,671 according to the general authority of statistics of Saudi Arabia in 2010.21
The Eastern Province of Saudi Arabia has around 12 universities and colleges. IAU is a big government university established in 1975 and includes 21 colleges. It accepts a large number of students each year from all over the Kingdom; however, most of the students applying to the university are from the Eastern Province, including Dammam, Al-Khobar, Alhassa, Qateef, and Jubail. It has ~45,000 students in various specialties including medicine, dentistry, engineering, basic sciences, and so on. Health sciences in the university include the branches of medicine, dentistry, nursing, and applied medical sciences. Prior to getting admission in any of the health sciences group, the students need to have completed the preparatory year of the health path. The health path accepts ~650 students (aged 17 years and above) of both genders every year. At the beginning of the academic year, all students accepted in the health path must undergo a medical screening test at KFHU by taking the best-corrected visual acuity using a Snellen chart, doing some blood works and followed by a medical interview. For the purpose of our study, some additional ophthalmological examinations were added for the students who participated in our study. Only the students accepted in the health path were the target of our study. The sample size was calculated from the total of 650 students based on an assumption that 50% of the total health path students have myopia. Simple random sampling technique was adopted to select the participants from the total students enrolled in the health path.
Exclusion criteria included a history of glaucoma, cataract, corneal scars, retinal disorders, refractive surgeries, previous cataract surgery, strabismus, amblyopia, and recent corneal operations. An informed written consent was collected from each student after explaining the purpose of the study. After filling the questionnaire, they were asked to head to the ophthalmology clinic to undergo the ophthalmological examination.
The questionnaire
The questionnaire was structured to assess the possible association of some risk factors with refractive errors. It was adopted from different studies.9,22–24 Some sections of the questionnaire were customized to fit the study population and the differences in the living environment that may have an impact on quantifying the outdoor and indoor activities. Then, a pilot study was conducted to validate the questionnaire tool.
Questionnaire-based method to quantify near-work and outdoor activities has been widely used by previous studies.9,23,25 All of the questionnaires were filled by the study participants themselves. The questions covered basic information such as the demographic data, which included age and gender, parental refractive error status, personal history of wearing spectacles or contact lenses, and a family history of myopia or hyperopia. The data regarding the average number of hours spent per week on near-work activity were collected from questions based on homework, reading, playing video games, watching television, and use of smart phone, laptop, and computer. The data regarding time spent on outdoor activities were collected from questions about going for a walk or running, picnics, barbeques, going to the beach, bicycle riding, and outdoor sport.
Examination
All participants, after completing the questionnaires, headed to the examination. Examination was done in the ophthalmology clinic of KFUH by an expert technician. The examination included assessment of intraocular pressure by non-contact “air puff” tonometer, and refraction by non-cycloplegic autorefraction using an autorefractometer (Tonoref II ARK-510A autorefractometer; Nidek Inc, Aichi, Japan). Biometric and keratometric measurements were obtained using IOLMaster 500 (Carl Zeiss Meditec AG, Jena, Germany) and Pentacam HR corneal topography (Oculus, Wetzlar, Germany). The parameters like axial length, anterior chamber depth, and corneal curvature were measured. The same devices operated by the same examiner were used for all the participants.
Definition of variables
Measurements were done for both right and left eyes, and an average of three readings was taken. Refractive error status of the participants was classified based on the spherical equivalent of refraction (SER) value into emmetropia, hyperopia, and myopia. The SER was calculated as (sphere + ½ cylinder). Myopia was considered if SER ≤−0.75 D, emmetropia if SER is between −0.75 D and 1 D, and hyperopia if SER ≥1 D. Myopia was further classified as low, moderate, and severe. Low myopia was defined as SER of −0.75 to −2.99 D, moderate as SER from −3.00 to −5.99 D, and severe as SER ≥−6.00 D.
Data analysis
Chi-squared tests and independent t-tests were used to test the associations among categorical and continuous variables, respectively. We performed a stepwise multiple linear regression procedure to evaluate the relationship between SER and other independent variables. For all the analyses, a two-sided P-value of ≤0.05 was considered statistically significant. Data analysis was performed using SPSS software version 25.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 338 students were examined (162 males and 176 females), with a zero non-participation rate. Since SER measurements of right and left eyes were highly correlated (Pearson’s correlation =0.9), only the data of the right eye were used for analysis. About 47.9% of the students had myopia (42.6% males and 57.4% females) (Tables 1 and 2). Among the myopes, 66.67%, 27.78%, and 5.56% were low, moderate, and high myopes, respectively (Table 2). Hyperopes constituted 6.5% and emmetropes 45.6% of the total participants. There was no difference in the prevalence rates of different myopia types between female and male students (χ2=1.60, P=0.44).
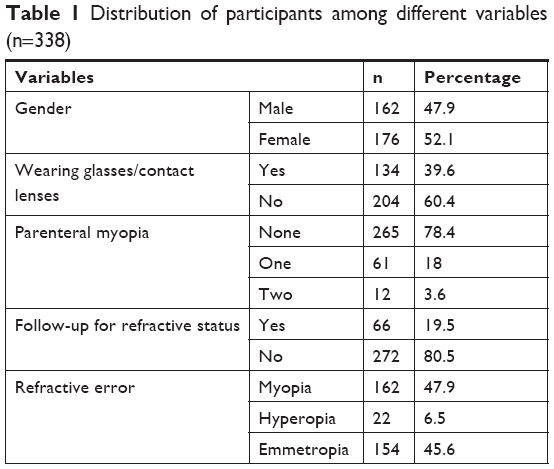 | Table 1 Distribution of participants among different variables (n=338) |
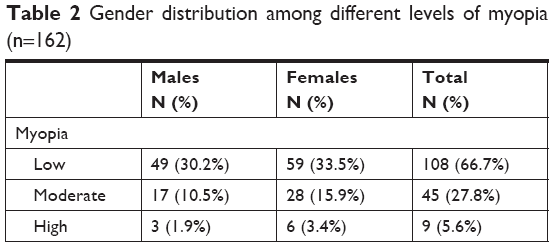 | Table 2 Gender distribution among different levels of myopia (n=162) |
The mean values of SER were −2.40 D, 0.00 D, and 2.32 D for myopes, emmetropes, and hyperopes, respectively (Table 3). It was observed that the mean SER values decreased in both male and female gender students with no history of parental myopia compared to the students with a parental history of myopia (Table 3). As shown in Table 4, axial length and anterior chamber depth measurements were significantly higher in myopes compared to non-myopes, including hyperopes and emmetropes. Other biometric parameters and keratometry results of myopes and non-myopes are shown in Table 4. A multiple regression analysis was run to test if different hypothesized factors, including gender, parental history of myopia, amount of near-work activity, and outdoor activities, can predict SER. The result of regression analysis showed that only 7.9% of the variance is explained by the model and that the model was a significant predictor of the SER (F (5,332)=6.7, P≤0.001) (Table 5). Gender factor has shown a significant contribution to the model (β=0.593, P=0.013), as well as the parental history of myopia with one parent and both parents being significant contributors to the model (β=−0.926, P=0.002 and β=−2.433, P≤0.001), respectively. Both near-work and outdoor activities have not shown any significant impact on SER while adjusting for other independent variables (β=−0.033, P=0.20 and β=0.00, P=0.99) respectively.
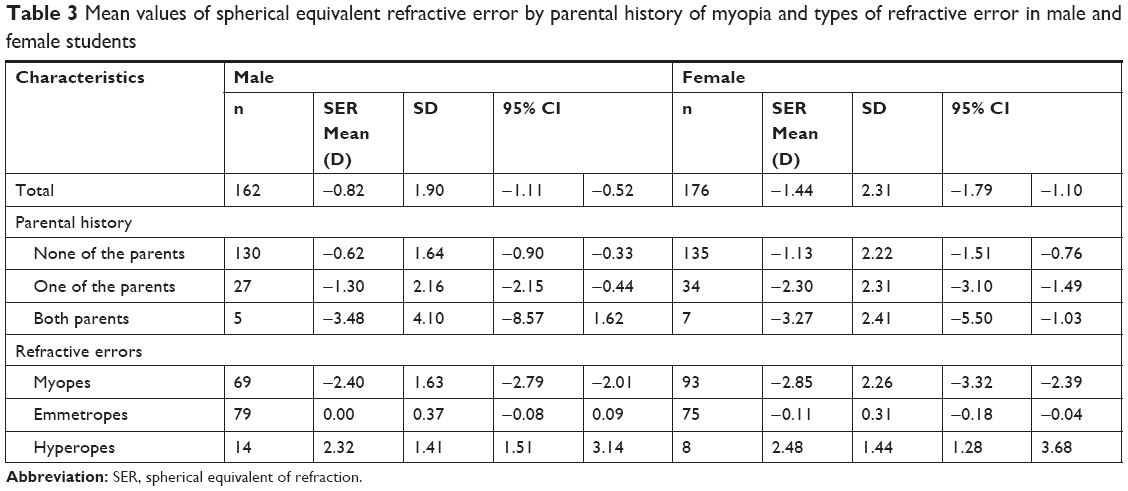 | Table 3 Mean values of spherical equivalent refractive error by parental history of myopia and types of refractive error in male and female students |
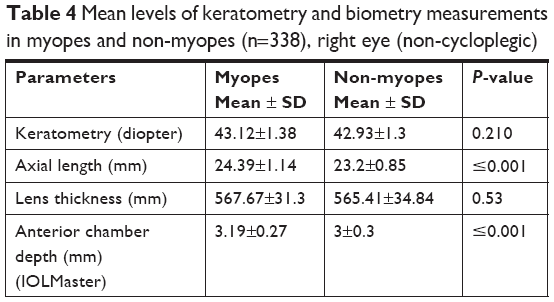 | Table 4 Mean levels of keratometry and biometry measurements in myopes and non-myopes (n=338), right eye (non-cycloplegic) |
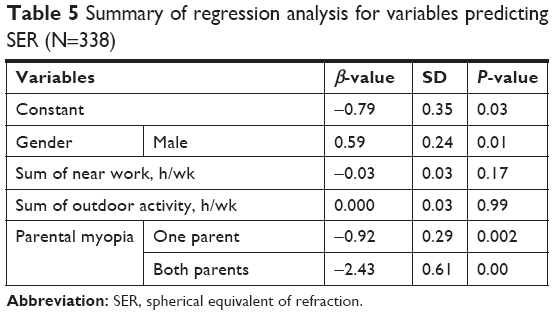 | Table 5 Summary of regression analysis for variables predicting SER (N=338) |
When all other variables including total near-work activity, total outdoor activity, and parental history of myopia are adjusted, the mean SER of male gender was significantly higher by 0.59 times (P=0.013) compared to female gender.
Discussion
There are several important findings in this study. First, the prevalence of myopia among the college students was about 48%. Second, there was no association between the refractive error status and near-work or outdoor activity.
The prevalence of myopia found in this study was quiet high when compared to other countries. For instance, it was estimated as 32.9% in Turkish medical students, 13% in adolescent Norwegians, 19.7% in young Jordanians, and 34.2% in young Europeans aged 20–24 years.10,11,26,27 However, our prevalence was less than that reported in high school Chinese students (87.7%), 18-year-old Chinese (72.8%), young Taiwanese men (86.1%), and young Singaporeans (73.9%).28–31 The high reported prevalence has been widely observed in East Asians, which could possibly be explained by the differences in environmental factors among East Asian children compared to Western children, in terms of less time spent outdoors as they are subjected to a more rigorous educational system.25–32 It is important to note that refractive errors were measured without cycloplegia, which could overestimate the percentage of myopia.33 Myopia overestimation and hyperopia/emmetropia underestimation were observed previously when a cutoff of −0.5 D was used.33,34 However, the magnitude of overestimation is unknown when a cutoff of −0.75 D is used. Up to our knowledge, there have been only a few studies that examined myopia prevalence in young Saudis. Algorinees et al used cycloplegic refraction and reported that the prevalence rate of myopia was similar among their medical students (age range 18–20 years) from two different medical colleges, one located in Hail city (north of Saudi Arabia) and the other in Al Kharj city (near to Riyadh, capital of Saudi).17 Comparable reports of myopia prevalence were also reported by Alsaqr et al, with a percentage of 53.3% among school students of Riyadh, and by Al-Rashidi et al, with a percentage of 53.7% among students of Qassim Medical College (Buraydah city, Qassim Province).35,36 In this current study, the most common type was low myopia, making up to 66.7% of myopic students. The same definition of low myopia, with an SER between −0.75 D and −2.99 D, was used by Al-Rashidi et al, and an SER less than or equal to −0.5 D was used by Alsaqr et al with the same finding.35,36 However, Algorinees et al, who also used the same definition for moderate myopia found that moderate myopia was the most prevalent among their participants, which might be attributed to the age range of their participants as they included older participants reaching the age of 27 years.17 This trend toward a more myopic shift among students with increasing age has been observed in other studies.29,37 High myopia specifically necessitates the adaptation of prompt measures, owing to the fact that it leads to vision-threatening conditions such as myopic macular degeneration, choroidal neovascularization, and myopic glaucoma, hence determining its prevalence is crucial. In this study, high myopia, defined as an SER ≤−6.00 D, was found in 5.6% of the participants. This prevalence was found to be less than that reported among Chinese college students (19.5%).37 However, our results were comparable to the studies conducted in Saudi Arabia (8.04% vs 10.2%).17,36
In regard to the prevalence of myopia among male and female participants, no significant difference was observed in this study, similar to that reported in Turkish students.11 However, the mean SER value of male gender was 0.59 times higher (P=0.013) than those of the female gender. Similarly, males have exhibited a more hyperopic SER in other studies.10,29 In agreement with previous studies, parental myopia was a significant factor contributing to the occurrence of myopia.11,38 Parental myopia was sometimes interpreted as an evidence for a genetic role; however, as there is growing evidence for the greater influence of environmental factors, it remains difficult to explain the complex interactions between environmental and genetic factors in myopia.
The possible association between near-work activity and myopia can be explained on the basis that increasing amount of near work done can consequently increase accommodation, which in turn could potentially cause myopia. However, evidence from animal studies on experimental myopia has shown that accommodation is not an influencing factor.39,40 Another explanation for the link between education and myopia was proposed as follows: during near work, accommodative lag results in a hyperopic defocus which might stimulate the eye to grow, considering that imposed hyperopic defocus in animal models was found to be a strong stimulus for the eye growth.41,42
Multiple studies have shown an association of near work with myopia. For instance, a longer axial length was used as a substitute for myopia and was found to be associated with a longer time spent studying indoors.43 Furthermore, for each additional 1 hour on writing/reading and computer work outside of school, odds of myopia increased by 24% and 16%, respectively.10 A meta-analysis study on the association of myopia with near-work activities had found that the odds of myopia increased by 2% for every diopter-hour spent on near work per week, where diopter-hour was defined as (3* reading +2 *computer use +2 *video games in hours per day).14 In this study, we did not find a significant association between myopia and amount of near work performed after adjusting for other factors. It should be noted that there is no universal definition for near work, and hence quantification of near work may vary and so might the results. Although a questionnaire-based survey for quantifying near work has been the main method used by most previous studies, it is prone to have recall bias in terms of recalling previous time spent on various near-work activities besides its possible inability to detect individual differences.
Outdoor activity has been investigated by some researchers for the possibility of a protective effect from myopia progression. Some of them did not find an association, while some found only a weak association.22,38 A 3-year cohort study by Lin et al did not find a protective effect of outdoor activity.24 Similarly in our study, we could not demonstrate a significant association between outdoor activity and myopia. Nevertheless, a significant association has been reported by multiple other researchers.9,10,23 Two clinical trials have demonstrated promising results with one showing a significant reduction in myopia progression in the intervention group and the other showing a reduced incidence rate of myopia with outdoor activity.12,13 Furthermore, an interventional study showed a significant reduction in myopia onset with outdoor activity during class recess; however, they did not find a significant retardation of myopia progression among myopes with or without atropine treatment.44 A recent meta-analysis has concluded that increased outdoor activities is effective among non-myopes in regard to myopia onset and myopic shift, but not for myopic progression among myopes.45 It has been proposed that the protective effect of outdoor activity is achieved through the increased release of the retinal transmitter dopamine.9 This theory has been proposed based on the findings of experimental myopia, where dopamine was found to exhibit a protective effect against eye growth.46
Failure to find a significant association between myopia and outdoor activity could be attributed to the method used for measuring the outdoor activity, in which our case was a survey questionnaire. Alvarez et al conducted a study to evaluate questionnaire-based method in reporting accurate data on light exposure with the help of a wearable light sensor. They found inconsistent reports of light exposure compared with what is recorded by the sensor.47
Study limitations
Although a validated questionnaire was used and this was the main method adopted by previous studies, the study could be limited by the difficulties of quantifying the amount of outdoor and indoor activities. In addition, because all of our study participants were from the health path, who are expected to spend more time in near work and less time outdoors, variations among them are expected to be less evident, and a significant association between outdoor or indoor activities and myopia is less likely to be found. Moreover, the use of non-cycloplegic refraction could give a slightly higher myopic reading with a mean of 0.17±0.52 D when the definition of ≤−0.5 is used for defining myopia.34 Nevertheless, we adopted a different definition for myopia, −0.75 instead of −0.5, which has been adopted by some previous studies as well.11,48,49 Yet, the effect of this change is not known and is not supported by evidence. Moreover, cycloplegia was done in one Saudi study which reported the same percentage of prevalence as our study. The study participants were exclusively from the health path and so are more likely to have myopia compared with a natural population-based study done with cycloplegia, but unfortunately there is not such a study in Saudi Arabia to compare our results with.
Conclusion
In this cross-sectional study, a high prevalence of refractive errors was found among Saudi freshman students of IAU. Myopic students were more likely to report a history of parental myopia. Near-work and outdoor activities did not have a significant effect on the SER.
Ethical approval
The research was conducted in compliance with the tenets of the Declaration of Helsinki. It has been approved by the Ethical Committee and the Medical Research Review Board of IAU.
Acknowledgments
We would like to thank those who have assisted us with organizing the order of examination: Arwa Ibrahim, Salsabeel Alkhudairi, Zahra Alsaeed, and Anwar Alzahrani.
Disclosure
The authors report no conflicts of interest in this work.
References
Bourne RR, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Glob Health. 2013;1(6):e339–e349. | ||
Smith TST, Frick KD, Holden BA, Fricke TR, Naidoo KS. Potential lost productivity resulting from the global burden of uncorrected refractive error. Bull World Health Org. 2009;87(6):431–437. | ||
Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. | ||
Rudnicka AR, Kapetanakis VV, Wathern AK, et al. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention. Br J Ophthalmol. 2016;100(7):882–890. | ||
Wu P-C, Huang H-M, Yu H-J, Fang P-C, Chen C-T. Epidemiology of myopia. Asia Pac J Ophthalmol. 2016;5(6):386–393. | ||
Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32(1):3–16. | ||
Williams KM, Bertelsen G, Cumberland P, et al. Increasing prevalence of myopia in Europe and the impact of education. Ophthalmology. 2015;122(7):1489–1497. | ||
Jacobsen N, Jensen H, Goldschmidt E. Does the level of physical activity in university students influence development and progression of Myopia? – A 2-year prospective cohort study. Invest Ophthalmol Vis Sci. 2008;49(4):1322. | ||
Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279–1285. | ||
Khader YS, Batayha WQ, Abdul-Aziz SM, Al-Shiekh-Khalil MI. Prevalence and risk indicators of myopia among schoolchildren in Amman, Jordan. East Mediterr Health J. 2006;12(3–4):434–439. | ||
Onal S, Toker E, Akingol Z, et al. Refractive errors of medical students in Turkey: one year follow-up of refraction and biometry. Optom Vis Sci. 2007;84(3):175–180. | ||
Jh Y, Rr L. Influence of near-work and outdoor activities on myopia progression in school children. Chinese J Contemp Pediatr. 2011;13:32–35. | ||
He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in China. JAMA. 2015;314(11):1142–1148. | ||
Huang HM, Chang DS, Wu PC, Ds C, Pc W. The association between near work activities and myopia in Children-A systematic review and meta-analysis. PLoS One. 2015;10(10):e0140419. | ||
Khairallah M, Kahloun R, Flaxman SR, et al. Prevalence and causes of vision loss in North Africa and the Middle East: 1990–2010. Br J Ophthalmol. 2014;98(5):605–611. | ||
Al-Shaaln FF, Bakrman MA, Ibrahim AM, Aljoudi AS, Ibrahim AM. Prevalence and causes of visual impairment among Saudi adults attending primary health care centers in northern Saudi Arabia. Ann Saudi Med. 2011;31(5):473–480. | ||
Algorinees RM, Alqahtani NT, Aljarbou AM, et al. Prevalence of myopia and its related risk factors among medical students in Saudi Arabia. Adv Ophthalmol Vis Syst. 2017;6(1):00165. | ||
Aldebasi YH. Prevalence of correctable visual impairment in primary school children in Qassim Province, Saudi Arabia. J Optom. 2014;7(3):168–176. | ||
Al Wadaani FA, Amin TT, Ali A, Khan AR. Prevalence and pattern of refractive errors among primary school children in Al Hassa, Saudi Arabia. Glob J Health Sci. 2012;5(1):125–134. | ||
Morgan IG, French AN, Ashby RS, et al. The epidemics of myopia: aetiology and prevention. Prog Retin Eye Res. 2018;62:134–149. | ||
General Authority for Statistics. Detailed results for the eastern region (general population and housing census 2010). 2010. Available from: https://www.stats.gov.sa/en. Accessed December 22, 2018. | ||
Wu LJ, You QS, Duan JL, et al. Prevalence and associated factors of myopia in high-school students in Beijing. PLoS One. 2015;10(3):e0120764. | ||
French AN, Morgan IG, Mitchell P, Rose KA. Risk factors for incident myopia in Australian school children: the Sydney adolescent vascular and eye study. Ophthalmology. 2013;120(10):2100–2108. | ||
Lin Z, Vasudevan B, Mao GY, et al. The influence of near work on myopic refractive change in urban students in Beijing: a three-year follow-up report. Graefes Arch Clin Exp Ophthalmol. 2016;254(11):2247–2255. | ||
Ip JM, Saw SM, Rose KA, et al. Role of near work in myopia: findings in a sample of Australian school children. Invest Ophthalmol Vis Sci. 2008;49(7):2903–2910. | ||
Hagen LA, Gjelle JVB, Arnegard S, Pedersen HR, Gilson SJ, Baraas RC. Prevalence and possible factors of myopia in Norwegian adolescents. Sci Rep. 2018;8(1):13479. | ||
Williams KM, Verhoeven VJ, Cumberland P, et al. Prevalence of refractive error in Europe: the European Eye Epidemiology (E(3)) Consortium. Eur J Epidemiol. 2015;30(4):305–315. | ||
Chen M, Wu A, Zhang L, et al. The increasing prevalence of myopia and high myopia among high school students in Fenghua City, eastern China: a 15-year population-based survey. BMC Ophthalmology. 2018;18(1):159. | ||
You QS, Wu LJ, Duan JL, et al. Prevalence of myopia in school children in greater Beijing: the Beijing childhood eye study. Acta Ophthalmol. 2014;92(5):e398–e406. | ||
Lee YY, Lo CT, Sheu SJ, Yin LT. Risk factors for and progression of myopia in young Taiwanese men. Ophthalmic Epidemiol. 2015;22(1):66–73. | ||
Quek TPL, Chua CG, Chong CS, et al. Prevalence of refractive errors in teenage high school students in Singapore. Oph Phys Optics. 2004;24(1):47–55. | ||
Morgan IG, Rose KA. Myopia and international educational performance. Ophthalmic Physiol Opt. 2013;33(3):329–338. | ||
Sun Y-Y, Wei S-F, Li S-M, et al. Cycloplegic refraction by 1% cyclopentolate in young adults: is it the gold standard? The Anyang University Students Eye Study (AUSES). Br J Ophthalmol. Epub 2018 Jun 21. | ||
Sanfilippo PG, Chu BS, Bigault O, et al. What is the appropriate age cut-off for cycloplegia in refraction? Acta Ophthalmol. 2014;92(6):e458–e462. | ||
Alsaqr A, Abu Sharha A, Fagehi R, et al. The visual status of adolescents in Riyadh, Saudi Arabia: a population study. Clin Ophthalmol. 2018;12:965–972. | ||
Al-Rashidi SH, Albahouth AA, Althwini WA, et al. Prevalence refractive errors among medical students of Qassim University, Saudi Arabia: cross-sectional descriptive study. Open Access Maced J Med Sci. 2018;6(5):940–943. | ||
Sun J, Zhou J, Zhao P, et al. High prevalence of myopia and high myopia in 5060 Chinese university students in Shanghai. Invest Ophthalmol Vis Sci. 2012;53(12):7504–7509. | ||
Guo L, Yang J, Mai J, et al. Prevalence and associated factors of myopia among primary and middle school-aged students: a school-based study in Guangzhou. Eye. 2016;30(6):796–804. | ||
Schmid KL, Wildsoet CF. Effects on the compensatory responses to positive and negative lenses of intermittent lens wear and ciliary nerve section in chicks. Vision Res. 1996;36(7):1023–1036. | ||
Wildsoet CF, Howland HC, Falconer S, Dick K. Chromatic aberration and accommodation: their role in emmetropization in the chick. Vision Res. 1993;33(12):1593–1603. | ||
Schaeffel F, Glasser A, Howland HC. Accommodation, refractive error and eye growth in chickens. Vision Res. 1988;28(5):639–657. | ||
Irving EL, Callender MG, Sivak JG. Inducing myopia, hyperopia, and astigmatism in chicks. Optom Vis Sci. 1991;68(5):364–368. | ||
Guo Y, Liu LJ, Xu L, et al. Outdoor activity and myopia among primary students in rural and urban regions of Beijing. Ophthalmology. 2013;120(2):277–283. | ||
Wu PC, Tsai CL, Wu HL, et al. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology. 2013;120(5):1080–1085. | ||
Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. 2017;95(6):551–566. | ||
Mccarthy CS, Megaw P, Devadas M, Morgan IG. Dopaminergic agents affect the ability of brief periods of normal vision to prevent form-deprivation myopia. Exp Eye Res. 2007;84(1):100–107. | ||
Alvarez AA, Wildsoet CF. Quantifying light exposure patterns in young adult students. J Mod Opt. 2013;60(14):1200–1208. | ||
Rahi JS, Cumberland PM, Peckham CS. Myopia over the lifecourse: prevalence and early life influences in the 1958 British birth cohort. Ophthalmology. 2011;118(5):797–804. | ||
Plainis S, Moschandreas J, Nikolitsa P, et al. Myopia and visual acuity impairment: a comparative study of Greek and Bulgarian school children. Ophthalmic Physiol Opt. 2009;29(3):312–320. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.