")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
Reduction of In-Hospital Preoperative Waiting Time of Elective Surgeries in the Amidst of COVID-19 Pandemic: Experience from Ethiopia
Authors Teklewold B , Abebe E, Anteneh D, Haileselassie E
Received 26 April 2022
Accepted for publication 10 October 2022
Published 17 October 2022 Volume 2022:14 Pages 185—194
DOI https://doi.org/10.2147/DHPS.S371839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Siew Siang Chua
Berhanetsehay Teklewold,1 Engida Abebe,1 Dagmawi Anteneh,2 Etsehiwot Haileselassie1
1Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Quality Improvement and Clinical Governance Directorate, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Dagmawi Anteneh, Quality Improvement and Clinical Governance Directorate, St. Paul’s Hospital Millennium Medical College, P.O. Box 1271, Addis Ababa, Ethiopia, Email [email protected]
Background: The higher demand for surgical services during the advancement of the COVID-19 pandemic has resulted from the need for a pre-admission negative result, the need for extra resources, and a shortage of skilled expertise. This quality improvement project aimed to reduce the in-hospital preoperative waiting time of elective cases to less than 24 hours.
Methods: The study was conducted in a tertiary care center. Following the collection of baseline data, we formed a multidisciplinary team to analyze the root causes and intervention ideas of delay using fishbone and driver diagrams, respectively. We prioritize key drivers and implemented several low-cost interventions using Plan-Do-Study-Act (PDSA) model. We monitored the average in-hospital preoperative waiting time of patients.
Results: Overall, in-hospital preoperative waiting time for elective cases has been reduced from a baseline of 4.89 days to 1.32 days on average by the end of 10 months of initiating the project. Similarly, monthly elective case cancellation rate due to COVID-19-related reason has been reduced from baseline 62.5% of the total cancellation to 0%. Due to this, the average monthly inpatient bed utilization has increased from 2.21 patients per month during pre-COVID-19 period to 5.9 patients per month in each bed of the surgical ward by the end of the project.
Conclusion: The implementation of a quality improvement project can optimize operation theatre efficiency, inpatient bed utilization, and reduce the surgical backlog. Meticulous and rigorous effort has to be laid down to do root cause analysis, generate feasible change ideas, and continuous follow-up, and testing of multiple PDSA cycles is required to impact an improvement and sustain it in the long run. The emergence of COVID-19 pandemic could be used as an opportunity to reduce the length of stay in the hospital.
Keywords: quality improvement, PDSA, COVID-19, in-hospital preoperative waiting time, elective surgery, Ethiopia
Introduction
More than 2 years have elapsed since COVID-19 was announced as a public health emergency of international concern by the World Health Organization.1 In Ethiopia, the first confirmed case of COVID-19 was reported on 13 March 2020.2
COVID-19 poses a great deal of challenge in the healthcare system worldwide in both delivering services to affected individuals and running an already existing essential healthcare service.3 Essential surgical services like outpatient visits and emergency and elective surgeries have been affected significantly. A study done in Switzerland showed a 39% and 43% decrement in emergency and elective operations, respectively, while in Ethiopia, elective surgeries were affected substantially (24% – emergency vs 56.3% – elective operation reduction during the pandemic).4,5
Quality improvement (QI) in healthcare is all about understanding of the complex healthcare system; using a methodological approach to problem solving; designing, testing, and implementing changes using real-time measurement; and improving safety, effectiveness and experience of patient care.6 PDSA (Plan-Do-Study-Act) is one of the QI models used widely to improve surgical services: it refers to a systematic approach to testing and measuring ideas in an iterative manner that may lead to an improvement in the processes or outcomes.7 PDSA can be used in various surgical context and objectives such as to improve the quality of postoperative procedures, process mapping and finding improvable points in surgery, to improve communication between patient and medical staff, and to reduce patient waiting time before surgery.8
Preoperative waiting time was lowered from 0.46 days to 0.29 days in 2008 following the implementation of a surgery admission unit for patients undergoing major elective surgery in Spain.9 A study conducted at a university hospital in the Netherlands showed, initiation of an outpatient preoperative evaluation reduces preoperative admission time by a factor of 0.89 (95% CI, 0.88–0.91), rate of same-day admissions increased from 5.26% (692/13,162) to 7.72% (542/7024), and cancellation rate for medical reasons only reduced from 1.95% to 0.93%.10
On top of the underlying large elective surgical backlog volume, COVID-19 pandemic put extra burden on the surgical backlog. This is due to the need for a timely pre-operation negative result for COVID-19, scarcity of expertise and resources due to COVID-19 response, and patient absence for admission after call due to fear and low healthcare-seeking behavior in times of the pandemic on top of temporary postponement of elective procedures in the earlier phase of the pandemic. All this together leads to long in-hospital preoperative stay and increased cancellation. So as to manage and improve this complex surgical backlog list and shorten in-hospital preoperative waiting time, meticulous, safe, feasible, effective, and efficient quality improvement project has to be designed and implemented.
This quality improvement project aimed to reduce the average in-hospital preoperative patient waiting time of elective cases to less than 24 hours from a baseline of 117.36 hours over a period of 10 months (January 1–31 October 2021).
Methods
Study Setting
This quality improvement project was conducted at the department of surgery, SPHMMC. It is located in Addis Ababa, the capital city of Ethiopia. The Department of Surgery is offering specialty and subspecialty services which are organized in three wards: general surgery, pediatric surgery, and urology wards. The department currently has 53 inpatient beds, which is scaled down from its initial 109 beds due to the COVID-19 pandemic emergence. It has one operation theatre equipped with six OR tables.11 The department performs over 3824 major surgeries to emergency and elective cases in the three wards annually.12 The project was conducted from 1 January to 31 October 2021.
Team Selection
A multidisciplinary team (MDT) from the inpatient service directorate, surgery department, anesthesia department, liaison office, and healthcare quality improvement team was established. The team consists of five physicians (one anesthesiologist, two surgeons, one quality officer, and one general practitioner), one anesthetist, two scrub nurses, and two liaison officers (one nurse and one health officer).
Study Design and Method
Institution-based interventional quality improvement study design was employed. This study was conducted with continuous, detailed meetings and discussions to prepare a process map, identify root causes and generate intervention ideas for long in-hospital preoperative waiting time. Following this, the PDSA model for quality improvement was applied to test intervention ideas and followed for an improvement in the processes or outcomes in the project with specific measures.
Data Collection and Analysis
Baseline, as well as follow-up in-hospital preoperative waiting time, number of elective surgeries performed, and cancellation rate, were collected from patient medical charts and registries. Data were coded, entered, and cleaned using SPSS version 24 software package by the project coordinator. Simple descriptive statistics such as frequency distributions were computed. The Chi-square test was done as appropriate, and the result was presented in tables, graphs, and run chart.
Strategy and Implementation
The MDT studied the complex process of getting elective surgery, do root cause analysis of long in-hospital preoperative waiting time, plot possible intervention packages with subsequent implementation sequentially, and follow-up of the project.
Process Mapping
The process map of patient flow requiring surgical intervention during COVID-19 pandemic at SPHMMC is redesigned as follows to ease and get the utmost efficient surgical service for elective cases (Figure 1).
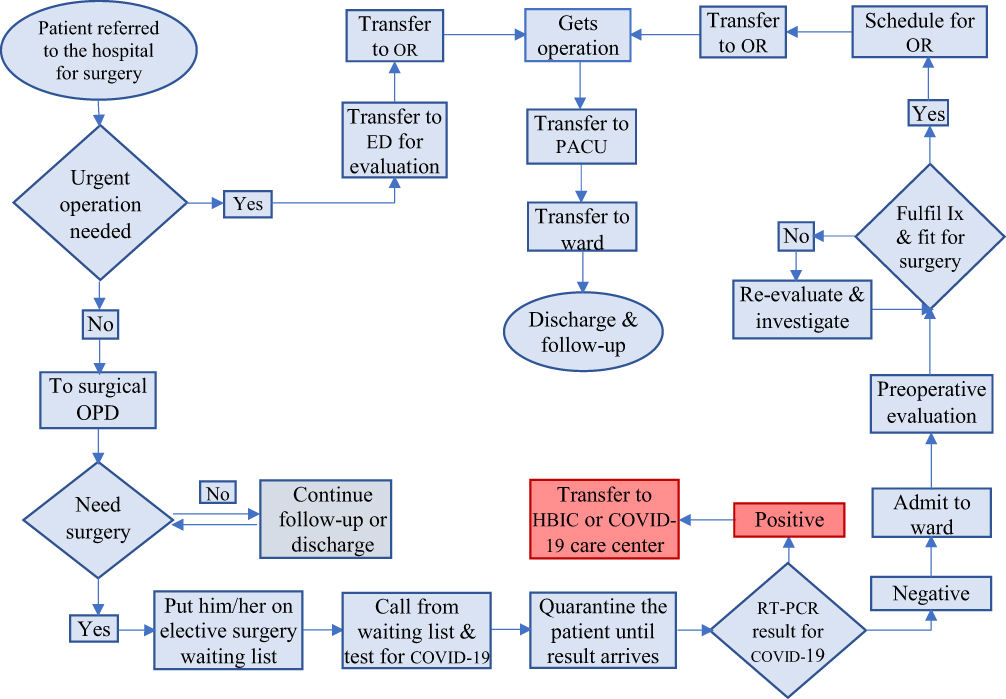 |
Figure 1 Process map depicting all steps in getting surgical operation at SPHMMC during COVID-19 pandemic. Abbreviations: OPD, outpatient department; ED, emergency department; RT, PCR-real-time polymerase chain reaction; HBIC, home-ased isolation and care; Ix, investigation; OR, operating room; PACU, post anaesthesia care unit. |
Root Cause Analysis/Fishbone Diagram
Based on the process map illustrated in Figure 1, factors contributing to long in-hospital preoperative waiting time for elective cases during COVID-19 pandemic at SPHMMC were identified using a fishbone analysis diagram (Figure 2). More than 32 underlying root causes categorized into four groups as patient factor, provider-related factor, work process-related factor, and facility/supply-related factors were identified.
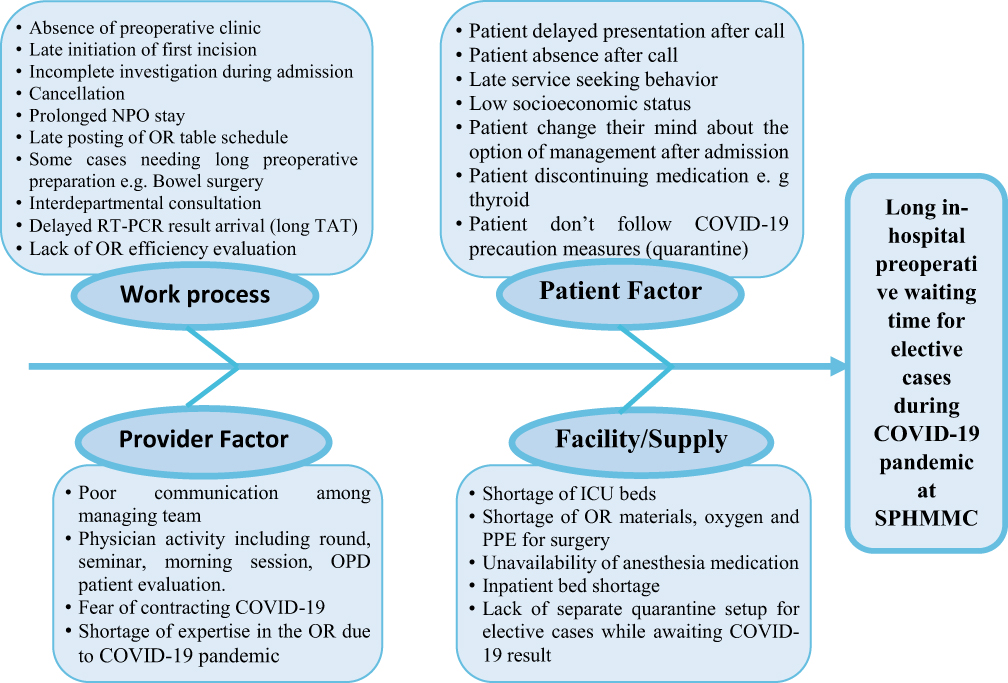 |
Figure 2 Fishbone diagram illustrating root causes of long in-hospital preoperative waiting time for elective cases during COVID-19 pandemic. Abbreviations: NPO, nothing per oral; OR, operating room; OPD, outpatient department; ICU, Intensive Care Unit; PPE, personal protective equipment; RT-PCR, real-ime polymerase chain reaction; SPHMMC, St. Paul’s Hospital Millennium Medical College. |
Driver Diagram
Depending on the root causes identified (Figure 2), two primary drivers, six secondary drivers, and 27 change/intervention ideas were schemed to achieve an in-hospital preoperative waiting time of less than 24 hours for elective surgical cases in the hospital (Figure 3).
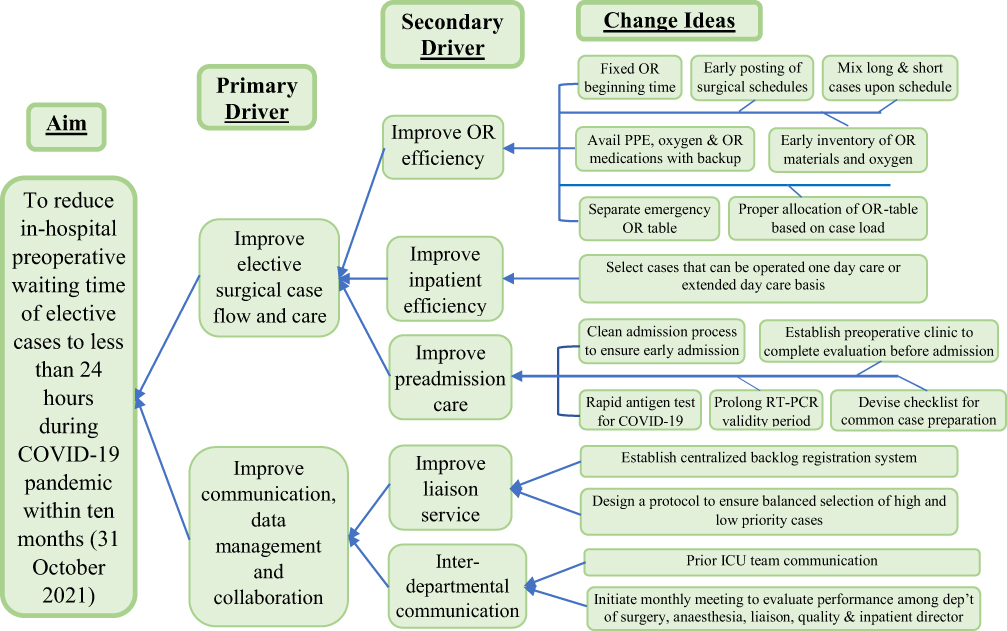 |
Figure 3 Driver diagram showing the AIM, primary and secondary drivers, and intervention/change ideas to improve in-hospital preoperative waiting time of elective cases. Abbreviations: OR, operating room; ICU, Intensive Care Unit; PPE, personal protective equipment; RT, PCR-real-time polymerase chain reaction; COVID-19, coronavirus infectious disease 2019. |
Measurement
Process Measures
- Percent of elective cases seen at preoperative clinic among admitted patients.
- Cancellation rate due to COVID-19-related reasons.
Outcome Measures
The mean in-hospital preoperative waiting time.
Balancing Measures
- Frequent alerts, meetings, and extra work to residents, nurses, liaison officers, and COVID-19 test sample collectors on different activities and interventions of the QI project led to increased workload.
- Availing RDT for COVID-19 and establishing a preoperative clinic requires robust financial, human resource, and facility cost.
- Incidence of surgical site infection might decrease while trying to shorten preoperative stay.13
- Compromise of academic activities to undergraduate students and residents due to short stay of patients preoperatively.
PDSA Implementation
Based on the driver diagram in Figure 3, we select five change ideas that have higher score using a focusing matrix to implement and test using a PDSA cycle (Table 1). Each change idea were implemented starting from January 2021 consecutively every 10 weeks while keeping the previous intervention in place (Table 2). We record and track all elective cases admitted and operated on for preoperative stay, the type of pathology they have, the area of admission, and cancellation rate on a weekly base. Depending on the findings, we made an iterative assessment of each PDSA cycle to sustain strengths and devise solutions to drawbacks for a better outcome.
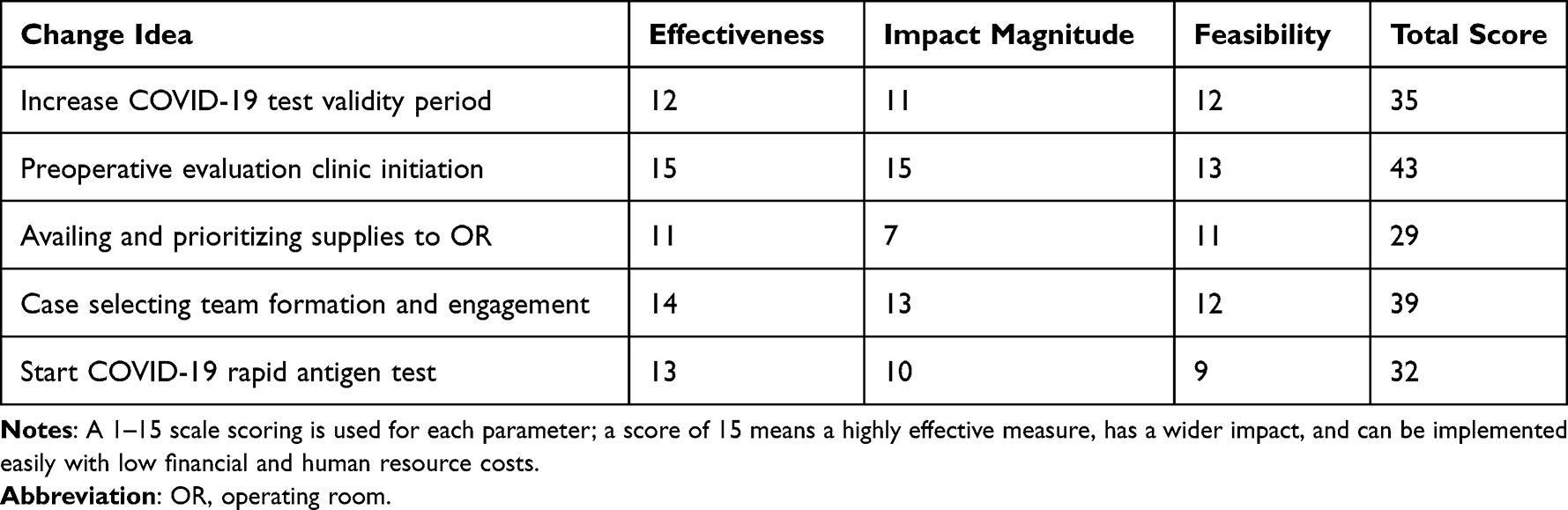 |
Table 1 Change Idea Prioritization to Test and Implement Using a Focusing Matrix |
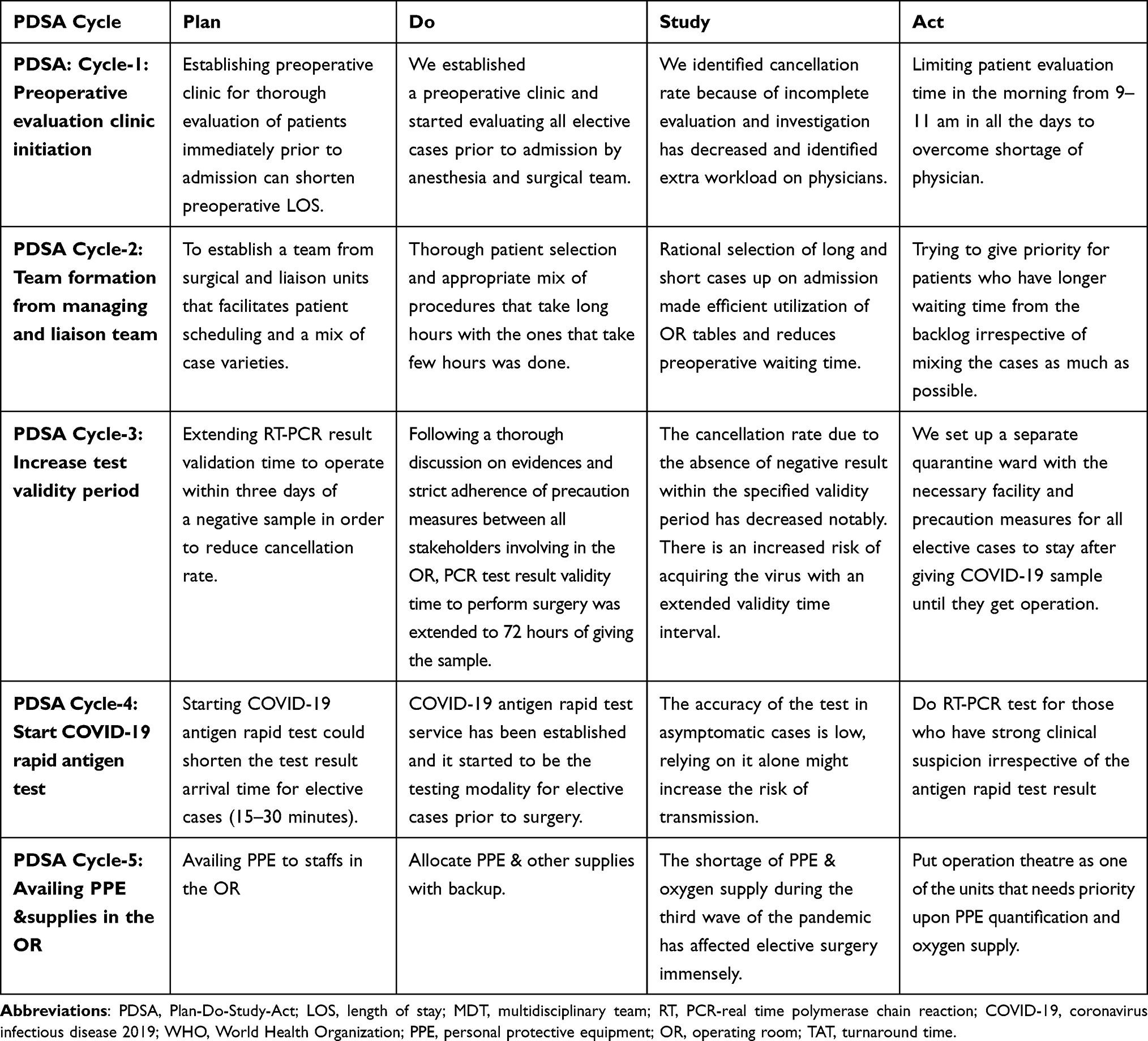 |
Table 2 Summary of PDSA Cycles on Reducing the In-Hospital Preoperative Waiting Time of Elective Cases During COVID-19 Pandemic |
Results
Overall, the in-hospital preoperative waiting time for elective cases has been reduced from a baseline of 4.89 days (117.36 hours) to 1.32 days (31.68 hours) on average by the end of 10 months of initiating the project (Figure 4 and Table 3).
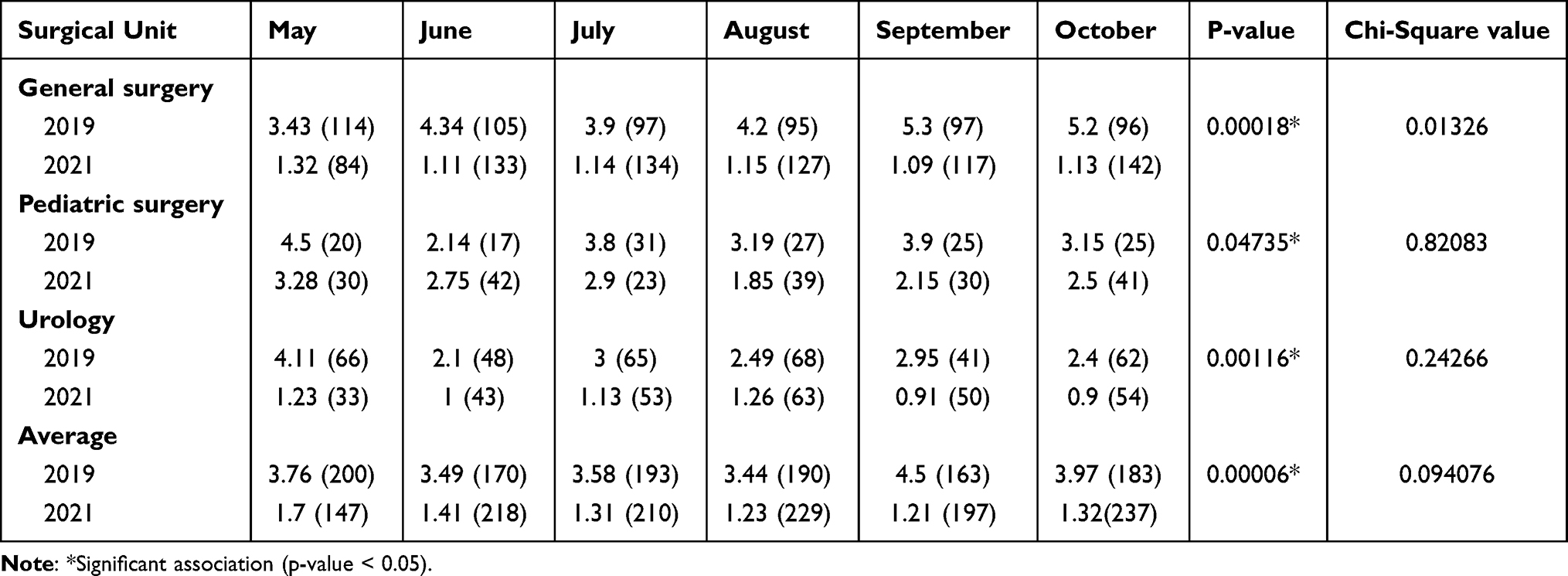 |
Table 3 In-Hospital Preoperative Patient Waiting Time of Elective Cases in Different Units of the Surgical Department Measured in Days with the Total Number of Surgeries Performed |
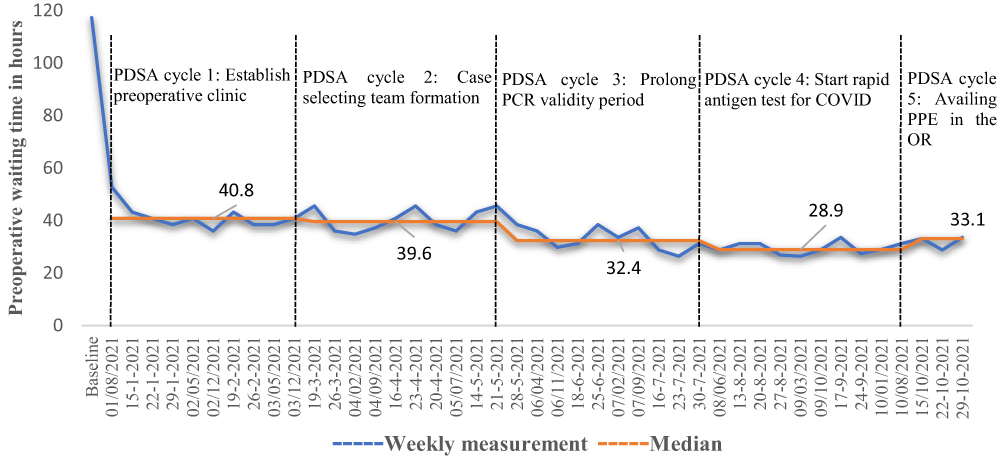 |
Figure 4 A run chart showing implementation of PDSA cycles with its impact on in-hospital preoperative waiting time (in hours) among elective surgical cases at SPHMMC. |
Following the implementation of the first PDSA cycle (preoperative evaluation clinic initiation), the average preoperative stay has been reduced to a median of 40.8 hours from a baseline of 117.36 hours. Similarly, subsequent PDSA cycles were able to reduce preoperative waiting time to a median of 39.6, 32.4, 28.9, and 33.1 hours, respectively (Figure 4).
In-hospital preoperative waiting time at the department of surgery has been reduced from 3.49 to 4.5 days range to 1.21–1.7 days on a monthly basis while implementing the project as compared to similar 6 months in the pre-COVID-19 period (2019) (p<0.00057). Unit wise, waiting time has been reduced from a range of 3.43–5.3 days to 1.09–1.32 days (p<0.000175), 2.14–4.5 days to 1.85–3.28 days (p<0.047349), and 2.1–4.11 days to 0.9–1.26 days (p<0.001164) in general surgery, pediatric surgery, and urology units, respectively (Table 3).
The average monthly inpatient bed utilization has increased from 2.21 patients per bed per month during the pre-COVID-19 period to 5.9 patients per bed per month in the surgical ward by the end of the project, which is more than 2.5 times efficient utilization of beds for both elective and emergency cases (Table 4).
 |
Table 4 Comparison of the Total Number of Elective Surgeries Performed with the Number of Surgical In-Patient Beds per Month During Similar Six-Months Period (Pre COVID-19 and While Implementing the QI Project) |
The overall operation theatre case cancellation rate has varied during the entire 10 months of the project stay. However, the cancellation rate due to delayed COVID-19 result or positive result has reduced progressively in the later phase of the project and when it is compared with the baseline data in the earlier phase of the pandemic in 2020 (Figure 5).
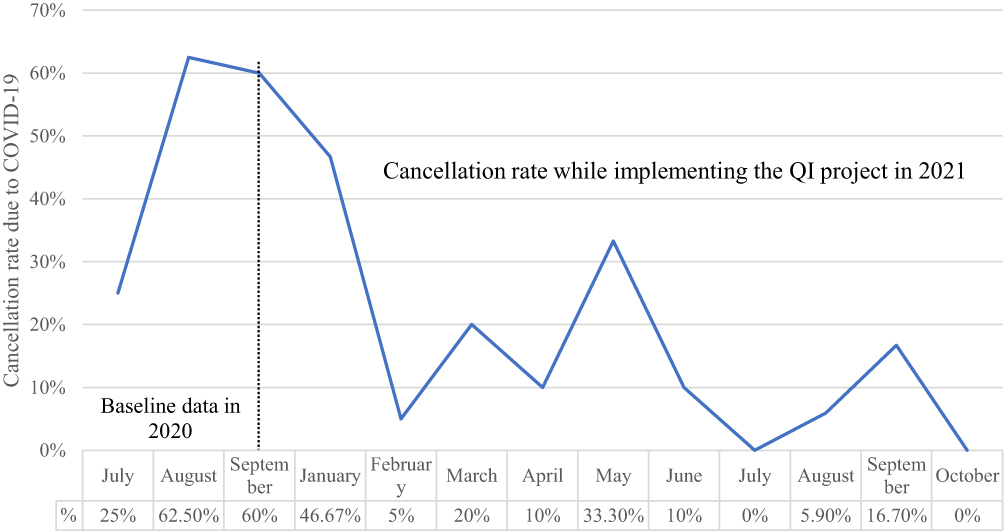 |
Figure 5 Monthly elective case cancellation rate due to COVID-19-related reason at the surgical department of SPHMMC. |
Discussion
The in-hospital preoperative waiting time has been reduced by a factor of 0.27, which is a significant reduction as compared to a study done in Spain and the Netherlands where reduced preoperative waiting time is reduced by a factor of 0.63 and 0.89, respectively.9,10 But as compared to a study done in Spain, the overall preoperative waiting time for elective cases in our study is still high (0.29 days vs 1.32 days).9 This could be due to the fact that there are resource limitations and the presence of academic activities like bedside, round, and other teaching sessions for undergraduate medical students in our setup.
All the five interventions tested has its own impact on reducing preoperative waiting time, but initiating preoperative evaluation clinic took the largest impact making the reduction by a factor of 0.35.
In-patient bed utilization has been increased by 2.5 times and the cancellation rate due to COVID-19-related reasons has been reduced progressively following the implementation of this project. This could be majorly due to the reduction of in-hospital preoperative waiting time.
These improvements are the results of the execution of proper change ideas under the right circumstance, regular feedback and communication between stakeholders, continuous follow-up for sustainability, dedicated MDT & leadership, and the presence of regular support from the hospital management.
Despite the enormous challenges paused by COVID-19 to the surgical service, on the flip side this quality improvement project showed that it can be used as an opportunity to curve long in-hospital preoperative waiting time to avoid COVID-19 acquisition and transmission in the hospital.
Quality improvement projects can put forward elective surgical care with minimal cost and collaborative effort of the multidisciplinary team within a short period in times of crisis without compromising the quality of care.
Strengths and Limitation
Utilizing a quality improvement project (PDSA cycle) in times of crisis with a combined effort of a multidisciplinary team and minimal cost to reduce the in-hospital preoperative length of stay has shown us a lot can be done with this kind of initiative to improve the quality of patient care. The strengths of this project include the use of validated QI methods in the entire process of the project; the presence of high-quality baseline data to support our change ideas, and ongoing regular data review and response using PDSA cycles; Implementing several PDSA cycles over a short period; and team-based approach between different service units of the hospital.
The need for a continuous effort to discuss, identify loopholes, and extensive data collection at every step of implementing the project has taught us to employ techniques that can reduce extra effort, cost, and time utilization.
It has been 10 months since we start the implementation of PDSA cycles, which has shown improvement in the preoperative stay, but we could not achieve the target. So, achieving the target and sustaining the project in the long-run has to be considered a limitation.
Conclusion
The implementation of this quality improvement project has optimized operation theatre efficiency, inpatient bed utilization, and reduction of surgical backlog of elective cases during the COVID-19 pandemic. All these improvements were seen from implementing and testing change ideas iteratively through meticulous and rigorous PDSA cycles. Establishing preoperative evaluation clinic, extending test validity period to 3 days, starting COVID-19 rapid antigen test, availing PPE & other supplies like oxygen, medications and materials with backup in the operation theatre, and establishing MDT to select elective cases from surgical and liaison team were the interventions that were implemented to bring all the changes seen in this project.
Ethical Consideration
Ethical approval and consent were obtained from the institutional review board of SPHMMC.
Acknowledgments
The authors would like to thank SPHMMC for the support and for allowing us to do the project. Lastly, our appreciation goes to all liaison and surgical department staff who actively participated in devising and implementing interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. IHR emergency committee on novel coronavirus (2019-nCoV). Available from: https://time.com/5774747/coronavirus-who-public-health-emergency/.
2. Coronavirus statistics worldometer report. Available from: https://www.worldometers.info/coronavirus/.
3. World Health Organization. Maintaining Essential Health Services: Operational Guidance for the COVID-19 Context: Interim Guidance. World Health Organization; 2020.
4. Hu¨bner M, Zingg T, Martin D, Eckert P, Demartines N. Surgery for non-Covid-19 patients during the pandemic. PLoS One. 2020;15(10):e0241331. doi:10.1371/journal.pone.0241331
5. Dandena F, Teklewold B, Anteneh D. Impact of COVID-19 and mitigation plans on essential health services: institutional experience of a hospital in Ethiopia. BMC Health Serv Res. 2021;21:1105. doi:10.1186/s12913-021-07106-8
6. Academy of Medical Royal Colleges. Quality Improvement – Training for Better Outcomes. London: Academy of Medical Royal Colleges; 2016.
7. Varkey P, Reller MK, Resar RK. Basics of quality improvement in health care. Mayo Clin Proc. 2007;82(6):735–739. doi:10.4065/82.6.735
8. Beyranvand T, Aryankhesal A, Aghaei Hashjin A. Quality improvement in hospitals’ surgery-related processes: a systematic review. Med J Islam Repub Iran. 2019;33:129. doi:10.34171/mjiri.33.129
9. Ortiga B, Capdevila C, Salazar A, et al. Effectiveness of a Surgery Admission Unit for patients undergoing major elective surgery in a tertiary university hospital. BMC Health Serv Res. 2010;23. doi:10.1186/1472-6963-10-23
10. Wilton VK, Karel GM, Charles R, et al. The effect of outpatient preoperative evaluation of hospital inpatients on cancellation of surgery and length of hospital stay. Anesth Analg. 2002;94(3):644–649. doi:10.1097/00000539-200203000-00030
11. Six-months (July-December) report of the department of surgery. St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. 2021.
12. Annual liaison report. St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. 2021.
13. Shiferaw WS, Aynalem YA, Akalu TY, Petrucka PM. Surgical site infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Surg. 2020;107. doi:10.1186/s12893-020-00764-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.