")
Back to Journals » Patient Preference and Adherence » Volume 10
Reducing the risk of venous thromboembolism using apixaban – patient perspectives and considerations. Should more attention be given to females?
Authors Fabbian F , De Giorgi A , Tiseo R, Zucchi B , Manfredini R
Received 26 November 2015
Accepted for publication 22 December 2015
Published 27 January 2016 Volume 2016:10 Pages 73—80
DOI https://doi.org/10.2147/PPA.S82484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Fabio Fabbian, Alfredo De Giorgi, Ruana Tiseo, Beatrice Zucchi, Roberto Manfredini
School of Medicine, University of Ferrara, Ferrara, Italy
Background: New oral anticoagulant agents, such as apixaban, rivaroxaban, dabigatran, or endoxaban, have recently become for patients an alternative option to conventional treatment in the therapy of venous thromboembolism (VTE). Thus, we aimed to review the available information on adverse events (AEs) of apixaban compared to conventional therapy (heparin or vitamin K antagonists) in randomized controlled trials (RCTs) on patients treated for VTE, with a particular attention to sex subgroups.
Methods: An electronic search in MEDLINE and Embase was performed by using the keywords “apixaban” and “venous thromboembolism”. All RCTs focused on apixaban in the treatment and prevention of VTE were evaluated for the presence of AEs. AEs were classified as serious, bleeding, and cause of discontinuation. Moreover, we also searched by using the keywords “gender” and “venous thromboembolism” and “anticoagulants”.
Results: Considering all subjects enrolled in the eleven RCTs as a whole to investigate the occurrence of AEs, we extrapolated an events/subjects rate of 57.8% for AEs (6,445/11,144), 7.7% for serious AEs (975/12,647), 9.1% for bleeding events (1,229/13,454), and 3.2% for discontinuation of apixaban (421/13,039). The percentage of AEs was lower in subjects treated with apixaban than in those treated with conventional VTE therapy (53% vs 56.3%, respectively). However, only one study provided data on separate analysis by sex of either efficacy or safety of apixaban.
Conclusion: Under the patient’s perspective, apixaban could represent a good choice in the treatment of VTE, due to its pharmacological, economical, and safety profile. These positive aspects are certainly present in both sexes, since the available studies include a correct percentage of women, but data with separate analyses by sex are extremely limited. Future clinical trials should include in their results on clinical impact and outcomes a stratification by sex, and studies aimed to evaluate possible sex-related differences for these drugs should be strongly encouraged.
Keywords: venous thromboembolism, deep vein thrombosis, apixaban, adverse events, sex
Introduction
Venous thromboembolism (VTE) represents a common clinical condition that encompasses deep vein thrombosis (DVT) and pulmonary embolism (PE), with an overall annual incidence of 108 per 100,000 inhabitants in the USA.1 In fact, PE and DVT are considered a different expression of the same clinical condition, since ~70% of patients with PE had a DVT, and 30%–70% of patients with DVT had a clinical or subclinical PE.2 Physicians should always consider PE which represents a life-threatening condition, ranking second among causes of out-of-hospital sudden death in the general population,3 and also in hospitalized patients, mortality due to PE is high.4 For these reasons, treatment of VTE should be familiar to any clinician. Therapy of PE and DVT was based on anticoagulant approach with parenteral or subcutaneous heparin or oral anticoagulants, represented by warfarin or new oral anticoagulants (NOAs), such as apixaban, rivaroxaban, dabigatran, or endoxaban.5 The vitamin K antagonists (VKAs) warfarin and acenocoumarol represent the old standard treatment for VTE, and their efficacy in prevention of recurrent VTE could be quantified as decreasing recurrent risk of ~3%.6 The main limitations of this therapy are the need of frequent control of coagulation pattern (international normalized ratio, INR) with some costs and logistic discomfort for patients, possible food and drug interactions leading to alterations of anticoagulant effect, and high incidence of bleeding complications. Thus, a low adherence to this therapy could be an expected consequence, and trials dealing with patients on VKAs for VTE showed that poor adherence could be detected by low percent of time in therapeutic range and with an increased risk of thromboembolic complications.7 NOAs include factor Xa inhibitors (rivaroxaban, apixaban, and endoxaban) and factor IIa inhibitors (dabigatran). NOAs do not require routine laboratory monitoring and frequent changes in dosage, suggesting an improvement in pharmacological adherence. However, results from a meta-analysis study of 18 randomized trials including >100,000 patients showed that total study discontinuation rates were not significantly different between NOAs and conventional therapy in VTE and prevention of stroke in atrial fibrillation (AF), whereas drug discontinuation with NOAs was significantly higher than with placebo in acute coronary syndromes.8 NOAs could suffer main drug interaction, and clinical contraindications could limit their potential use; however, these drugs do not require frequent evaluations of coagulation parameters and do not show changes in their pharmacological effectiveness related to foods or body weight.9,10 Moreover, NOAs are considered to be a favorable alternative to heparin in long-term VTE treatment, but bleeding risk and the absence of reversal agent are their major limitations.11 However, only a few data are available on possible differences by sex in the prescription of drugs, even if a little more is known on the use of antiplatelet agents (APAs). Results from a multicenter study in Italy, aiming to evaluate the existence of sex differences in treatment at hospital admission and prescription at discharge, showed the presence of statistical differences, among others, for APAs. At admission, men were more likely to be on APAs (41.7% vs 36.7%; P=0.0029), and at discharge, APAs (43.7% vs 37.3%; P=0.0003) continued to be prescribed more often in men.12 A recent study carried out in the Netherlands compared adherence to NOAs with adherence to APAs. Mean adherence to NOAs was 84.2% compared with 87.3% to APAs. One in four NOAs users had a percentage of days covered by medication <80% compared with one in five APA users. No data by sex subgroups were available.13
Thus, due to the paucity of available data, we decided to put ourselves in patients’ shoes, and the aim of this review was to analyze all adverse events (AEs) of apixaban compared to conventional therapy (heparin or VKAs) in randomized controlled trials (RCTs) of VTE treatment, with a particular attention to possible differences by sex.
Methods
We performed a literature search of electronic databases, MEDLINE and Embase, using the keywords “apixaban” and “venous thromboembolism”. The aim of this search was to identify all RCTs that analyze dapixaban for treatment and prevention of VTE, and the main outcome was the collection of data about AEs. AEs were classified as serious, bleeding, and cause of discontinuation. For any study, we required a minimum set of data, including author, journal and year of publication, and total number of patients treated with apixaban and/or with conventional therapy. Moreover, we made a comprehensive search by using the keywords “gender” and “venous thromboembolism” and “anticoagulants”.
Results
As for the first objective, 13 RCTs were identified, but only eleven were included in the analysis. Two RCTs were excluded because authors did not classified AEs as serious, bleeding, and cause of discontinuation.
Table 1 reports the type of AEs considered only in studies in which subjects were treated with apixaban.14–24 Considering all subjects enrolled in the eleven RCTs as a whole to investigate the occurrence of AEs, we extrapolated an events/subjects rate of 57.8% for AEs (6,445/11,144), 7.7% for serious AEs (975/12,647), 9.1% for bleeding events (1,229/13,454), and 3.2% for discontinuation of apixaban (421/13,039). The overall percentages of AEs related to the number of patients treated with apixaban are reported in Figure 1.
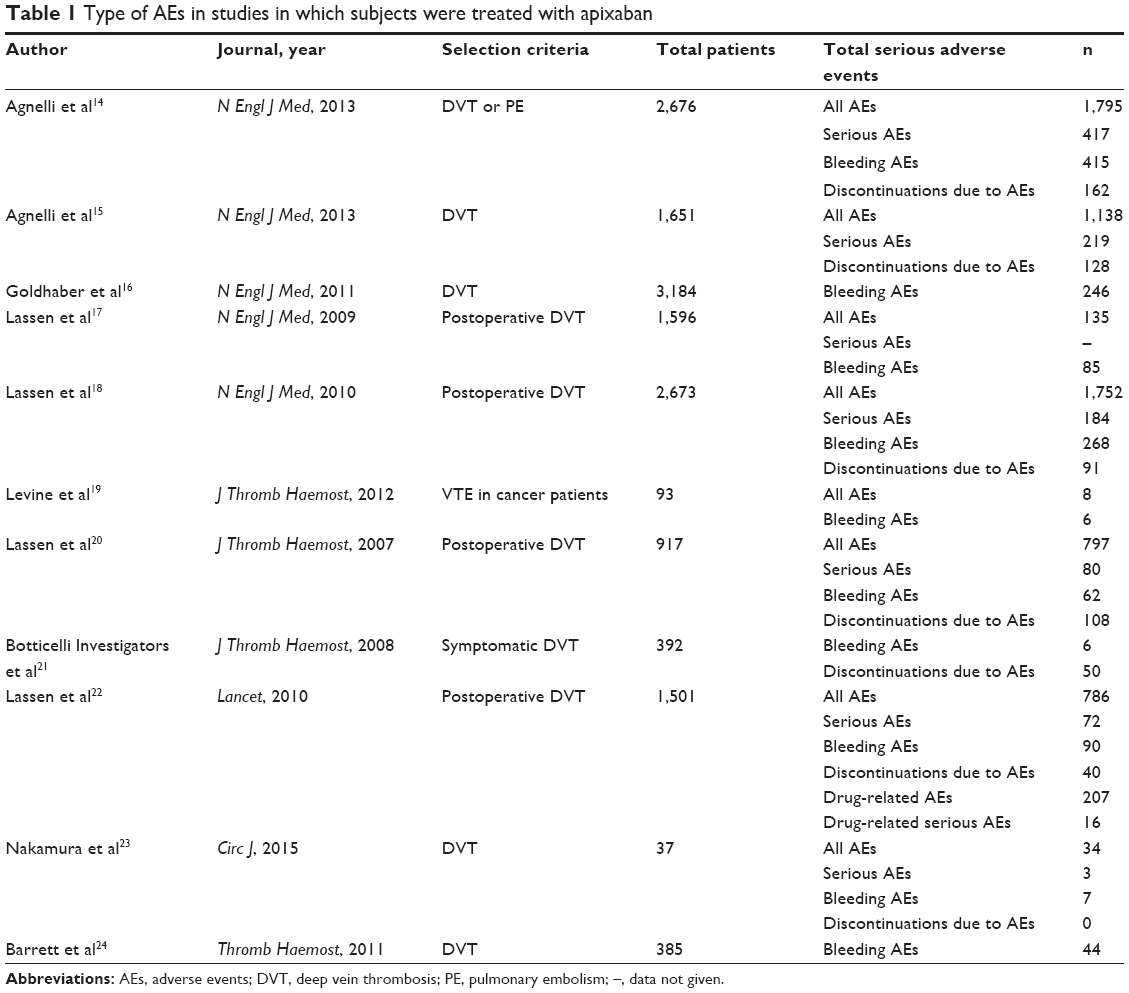 | Table 1 Type of AEs in studies in which subjects were treated with apixaban |
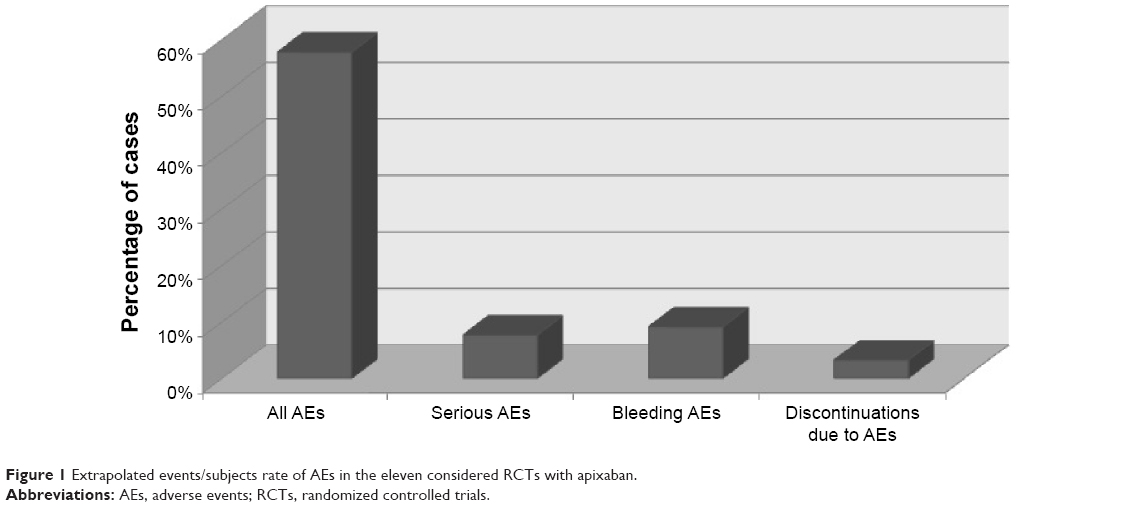 | Figure 1 Extrapolated events/subjects rate of AEs in the eleven considered RCTs with apixaban. |
Table 2 shows the AEs in different studies comparing apixaban and conventional therapy. The percentage of AEs was lower in subjects treated with apixaban than in those treated with conventional VTE therapy (53 vs 56.3%) (Figure 2).
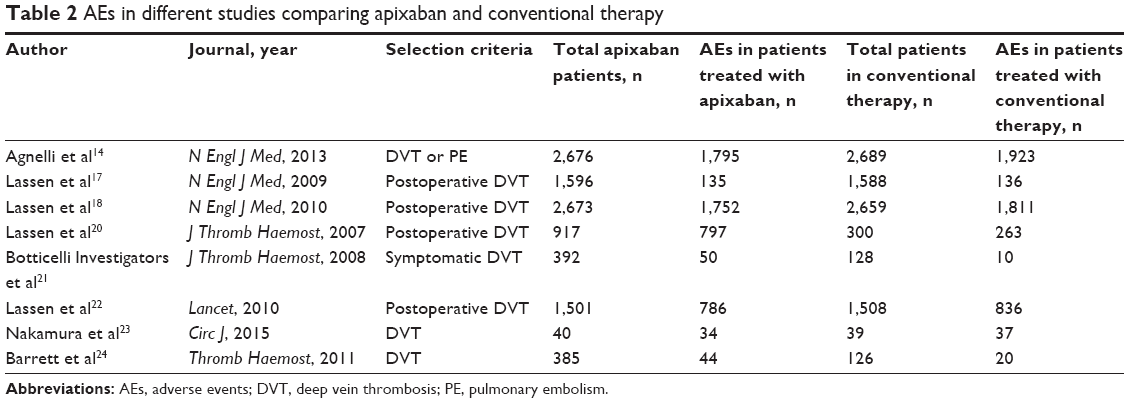 | Table 2 AEs in different studies comparing apixaban and conventional therapy |
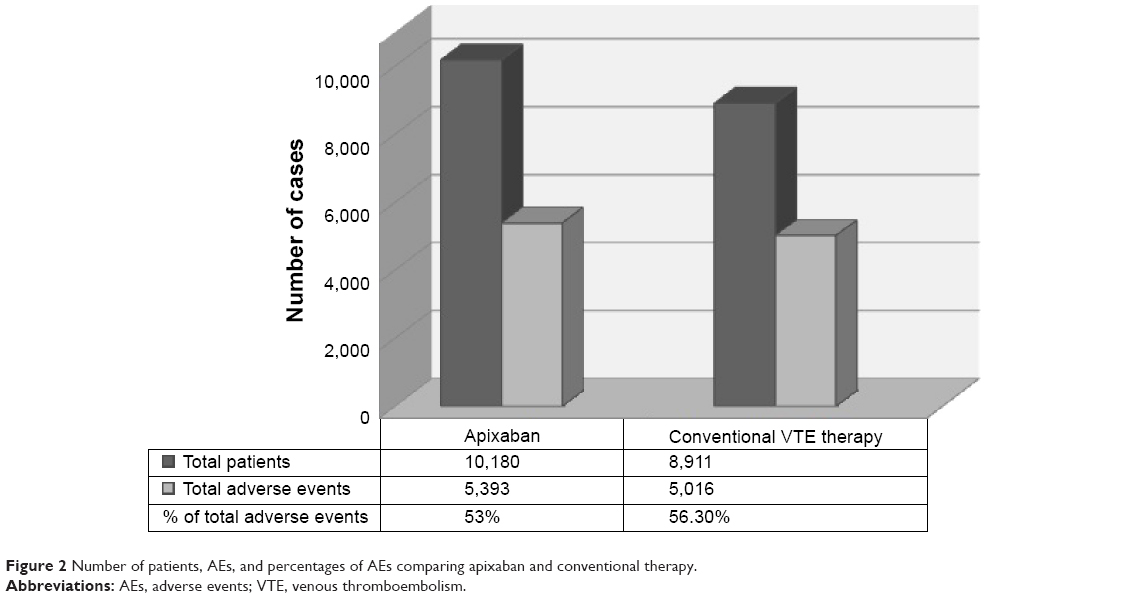 | Figure 2 Number of patients, AEs, and percentages of AEs comparing apixaban and conventional therapy. |
Table 3 provides additional data on the existence or not of subanalysis by sex in the studies comparing apixaban and conventional therapy.
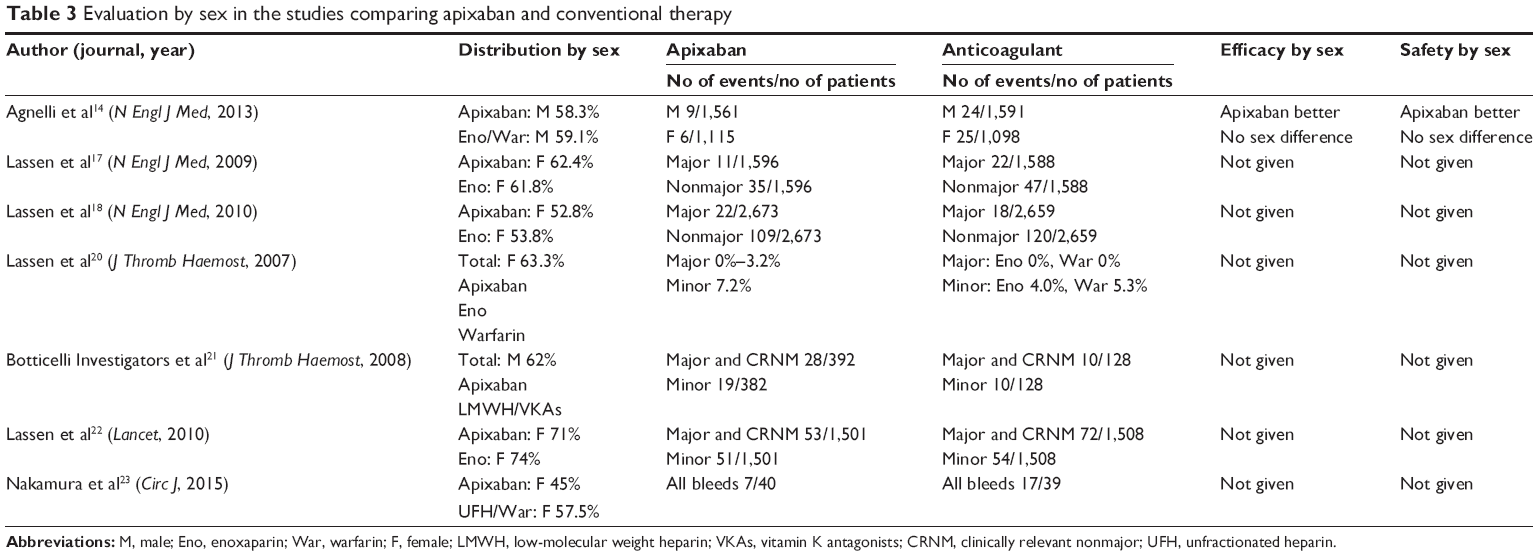 | Table 3 Evaluation by sex in the studies comparing apixaban and conventional therapy |
Discussion
The first observation of the present study is a confirmation of a lower prevalence of AEs related to VTE prevention and treatment with apixaban compared with conventional therapy. Total AEs were reported in 57.8% of patients, 9.1% had bleeding events, 7.7% had serious AEs, and only 3.2% of patients discontinued apixaban due to AEs. Apixaban is a selective inhibitor of factor Xa with an effect on inhibition of the conversion of prothrombin to thrombin,25 recently approved by health authorities in Italy for the treatment and prevention of VTE (May 23, 2015), and previously, for prevention of cerebrovascular events in patients with AF (December 2, 2013). Peak plasma concentration of apixaban is reached after 3 hours post-dose, half-life is ~12 hours, and anticoagulant effect expires after 24 hours post-dose.26 Oral bioavailability is ~52%; fixed therapeutical dosage, low hepatic metabolism (only 15%), and nonrenal metabolism allow minimal drug interactions and formations of reactive metabolites.26 A recent meta-analysis on risk of major bleeding related to NOAs showed a higher risk of hip surgery, acute coronary syndrome, and thromboprophylaxis in medically ill patients.27 The higher rate of major bleeding in these patients was related to longer duration of NOAs therapy and probably to the higher comorbidity. After the publication of the main RCTs with NOAs, several reviews analyzed the therapeutic potential and safety of NOAs compared with VKAs.28 The meta-analysis performed by van der Hulle et al showed that NOAs had lower relative risk (RR) than conventional therapy for major gastrointestinal bleeding (−0.16%), major bleeding (−0.67%), clinically relevant nonmajor bleeding (−1.77%), and fatal bleeding (−0.09%).29 These data were associated with an important efficacy of NOAs in reduction of recurrent VTE (−0.24%) and overall mortality (−0.10%). Similar results were reported by Kakkos et al, with a high safety of NOAs regarding bleeding events but only a non-inferiority in preventing recurrent symptomatic VTE and reduction of DVT.30 Compared to placebo, NOAs had higher efficacy on reduction of VTE recurrence (7.24% vs 1.32%) associated with higher incidence of nonmajor bleeding events and any bleeding. On the contrary, major bleeding events were not statistically different in patients treated with NOAs and placebo.30 An analysis performed by Mantha and Ansell on comparative efficacy of NOAs for the treatment of VTE showed that apixaban could have more effect in VTE prevention compared with dabigatran, rivaroxaban, and endoxaban, even if no statistical difference was detected.31 Similarly, Kang and Sobieraj reported a significantly lower incidence of major bleeding in patients treated with apixaban than in those treated with dabigatran and endoxaban, including lower risk of the composite end point (major and clinically relevant bleeding) compared to other NOAs.32 A further meta-analysis comparing NOAs in VTE patients showed no significant differences in risk for recurrent VTE, major bleeding, or all-cause mortality between the different molecules but identified that low dose of apixaban (2.5 mg BID) was related to less clinically significant nonmajor bleeding than other NOAs.33 Therefore, apixaban has been reported to be an effective and safe alternative to conventional therapy for acute or long-term treatment of VTE and to have a more favorable safety profile compared to other therapies.34 Moreover, apixaban characteristics were confirmed in patients with mild and moderate renal insufficiency compared to VKAs.35 NOAs, compared to conventional therapy, represent an economically acceptable strategy for VTE prophylaxis also in surgical patients.36 To this extent, apixaban is associated with the greatest reduction in medical costs (−$918) compared to VTE patients treated with standard therapy.37
The second main observation from this study is that the variable “sex” is not considered so much. For example, occurrence of VTE in patients with cancer is associated with unfavorable prognosis, and VTE treatment is less effective and more complicated in cancer patients. Comparison of efficacy and safety between NOAs and VKAs in cancer patients has been reported, but there are no guideline recommendations for women-specific cancer types or women-specific issues in the prevention and treatment of VTE.38 Only a very minimal part of the studies comparing apixaban vs conventional therapy takes sex into consideration. In the ARISTOTLE study, 11,785 (64.7%) men and 6,416 (35.3%) women with AF or flutter were randomized to receive either warfarin or apixaban. Results showed that women had a similar rate of stroke or systemic embolism but a lower risk of mortality and less clinically relevant bleeding than men.39 As for the previously cited RCTs on treatment of VTE, only one study provided data on separate analysis by sex of either efficacy or safety of apixaban.14 Such a lack of data on sex subgroups is rather surprising. In fact, women are at higher risk of VTE, even though age plays crucial role. Results from an epidemiologic study on hospitalization for PE in a large population of Northwestern Italy (60,853 patients, 59.6% females, mean age 73±14 years) found an overall crude incidence rate significantly higher for women compared with men (55.4 and 40.6 events per year per 100,000 inhabitants, respectively; P<0.001), but this difference completely disappeared after standardization for age.40 Again, women are at risk of VTE after total hip arthroplasty or total knee arthroplasty. A study on 14 retrospective case–control or prospective cohort studies, including 18,075 patients who developed VTE after total hip arthroplasty or total knee arthroplasty out of a total of 1,723,350 cases, found that three main risk factors were significantly associated with VTE: history of VTE, varicose vein, and congestive cardiac failure. However, authors recognized other six significant factors increasing VTE risk, such as female sex, age ≥80 years, hypertension, active cancer, obesity (BMI ≥30), and black race.41 The outcome during the course of anticoagulant therapy may differ according to the patient’s sex, but available data are not always univocal. According to the Spanish data from the Registro Informatizado Enfermedad Trombo Embólica Registry on >47,000 patients, women (51% of total sample) were older, more likely presented with PE, and were more likely to have recent immobilization but less likely to have cancer than men. Compared with men, women had a lower rate of DVT recurrences, a higher rate of major bleeding, and higher mortality due to PE, although rate of PE recurrences was similar. However, on multivariable analysis, any influence of sex on the risk for recurrent DVT, major bleeding, or fatal PE was no longer statistically significant.42 A subanalysis of the same registry focused on the outcome of cancer patients with acute VTE showed that, compared with men, women had a significantly lower rate of fatal bleeding and death, and a nonsignificantly lower rate of PE recurrences and major bleeding.43 Also, the meta-analysis studies, mostly addressed to both AF and VTE patients, are not conclusive. A systematic review and meta-analysis was performed to determine if the risk of major bleeding may differ between men and women receiving anticoagulation for AF or VTE. Forty-two studies including >94,000 patients were analyzed: 83% had AF and 17% had VTE; 37,250 patients (40%) were women. The RR of major bleeding for men vs women was 1.02, in particular 1.02 in patients with AF and 0.80 in patients with VTE. Thus, the risk of major bleeding on anticoagulation seems to be the same in both sexes, especially in the case of AF, whereas in patients with VTE, the risk of bleeding may be marginally lower in men compared with women.44 Again, another recent comprehensive systematic review and meta-analysis of 13 studies (>100,000 patients) showed that NOAs had a similar efficacy and safety compared with VKAs in female and male patients treated for nonvalvular AF and acute VTE. However, in the extended treatment of VTE, a trend toward an increased risk of bleeding in male patients as compared with female patients was observed for NOAs compared with placebo.45
As for low adherence to anticoagulant therapy, there are no univocal data available. Previous findings reported that risk factors related to lower adherence of VKAs therapy included younger age, male sex, poor cognitive function, poverty, and higher educational attainment.46 In a study on a total of 2,068 patients in Denmark, performing self-management of VKAs, males achieved a significantly better therapeutic INR control than females. In fact, females spent 71.1% of the time within therapeutic INR target range, whereas males spent 76.4% (P<0.0001), but the incidence of major complications was low and similar in both sexes.47 Again, a Swedish study evaluated the persistence with presently available antithrombotic treatments in AF patients. The overall persistence with any oral anticoagulant was 88.2% at 1 year and 82.9% at 2 years. After 1 year, the crude persistence was 85.0% with warfarin, 85.9% with apixaban, 74.4% with dabigatran, and 77.4% with rivaroxaban. Multivariate analysis confirmed significantly higher persistence with warfarin and apixaban than with dabigatran or rivaroxaban, persistence at 1 year after initiations on warfarin, and that apixaban had higher odds for persistence than initiation on dabigatran and rivaroxaban. However, female sex was one of the factors significantly associated with lower persistence.48 On the contrary, different results were reported by a recent study aimed to assess self-reported anticoagulation adherence in a tertiary center anticoagulation clinic. Main indications for anticoagulation were VTE (72%) and AF (18%); 74% of patients were on VKAs, and 26% on NOAs (rivaroxaban 79%, dabigatran 19%, apixaban 2%). Predictors of anticoagulation adherence were, in decreasing order, use of additional oral medications (odds ratio [OR] =2.78), retired employment status (OR =2.31), female sex (OR =1.58), and age (OR =1.02). In multivariate analyses, age, female sex, and use of other oral medications remained significantly associated with anticoagulation adherence.49
In conclusion, in the patient’s perspective, apixaban could represent a good choice in the treatment of VTE, due to its pharmacological, economical, and safety profile. These positive aspects are probably present in both sexes, since the available studies include a correct percentage of women. Future clinical trials should include in their results on clinical impact and outcomes a stratification by sex, and studies aimed to evaluate possible sex-related differences for these drugs should be strongly encouraged.
Acknowledgment
This work has been supported, in part, by a research grant from the University of Ferrara (Fondo Ateneo Ricerca).
Disclosure
No conflicts of interest exist for any author.
References
Go AS, Mozaffarian D, Roger VL, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics – 2014 update: a report from the American Heart Association. Circulation. 2014;129(3):399–410. | ||
Stein PD, Matta F, Musani MH, Diaczok B. Silent pulmonary embolism in patients with deep venous thrombosis: a systematic review. Am J Med. 2010;123(5):426–431. | ||
Manfredini R, Portaluppi F, Grandi E, Fersini C, Gallerani M. Out-of-hospital sudden death referring to an emergency department. J Clin Epidemiol. 1996;49(8):865–868. | ||
Fabbian F, Gallerani M, Pala M, et al. In-hospital mortality for pulmonary embolism: relationship with chronic kidney disease and end-stage renal disease. The hospital admission and discharge database of the Emilia Romagna region of Italy. Intern Emerg Med. 2013;8(8):735–740. | ||
Konstantinides SV, Torbicki A, Agnelli G, et al; Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033–3069, 3069a–3069k. | ||
Hutten BA, Prins MH. Duration of treatment with vitamin K antagonists in symptomatic venous thromboembolism. Cochrane Database Syst Rev. 2006;(1):CD001367. | ||
Di Minno A, Spadarella G, Tufano A, Prisco D, Di Minno G. Ensuring medication adherence with direct oral anticoagulant drugs: lessons from adherence with vitamin K antagonists (VKASs). Thromb Res. 2014;133(5):699–704. | ||
Chatterjee S, Sardar P, Giri JS, Ghosh J, Mukherjee D. Treatment discontinuations with new oral agents for long-term anticoagulation: insights from a meta-analysis of 18 randomized trials including 101,801 patients. Mayo Clin Proc. 2014;89(7):896–907. | ||
Kubitza D, Becka M, Zuehlsdorf M, Mueck W. Body weight has limited influence on the safety, tolerability, pharmacokinetics, or pharmacodynamics of rivaroxaban (BAY 59-7939) in healthy subjects. J Clin Pharmacol. 2007;47(2):218–226. | ||
Upreti VV, Wang J, Barrett YC, et al. Effect of extremes of body weight on the pharmacokinetics, pharmacodynamics, safety and tolerability of apixaban in healthy subjects. Br J Clin Pharmacol. 2013;76(6):908–916. | ||
Verso M, Agnelli G, Prandoni P. Pros and cons of new oral anticoagulants in the treatment of venous thromboembolism in patients with cancer. Intern Emerg Med. 2015;10(6):651–656. | ||
Hanemmjer S, Sodihardjo F, Horikx A, et al. Trends in antithrombotic drug use and adherence to non-vitamin K oral anticoagulants in the Netherlands. Int J Clin Pharm. 2015;37(6):1128–1135. | ||
Santalucia P, Franchi C, Djade CD, et al. Gender differences in drug use in hospitalized elderly patients. Eur J Intern Med. 2015;26(7):483–490. | ||
Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799–808. | ||
Agnelli G, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699–708. | ||
Goldhaber SZ, Leizorovicz A, Kakkar AK, et al. Apixaban versus enoxaparin for thromboprophylaxis in medically ill patients. N Engl J Med. 2011;365(23):2167–2177. | ||
Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med. 2009;361(6):594–604. | ||
Lassen MR, Gallus A, Raskob GE, Pineo G, Chen D, Ramirez LM; ADVANCE-3 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med. 2010;363(26):2487–2498. | ||
Levine MN, Gu C, Liebman HA, et al. A randomized phase II trial of apixaban for the prevention of thromboembolism in patients with metastatic cancer. J Thromb Haemost. 2012;10(5):807–814. | ||
Lassen MR, Davidson BL, Gallus A, Pineo G, Ansell J, Deitchman D. The efficacy and safety of apixaban, an oral, direct factor Xa inhibitor, as thromboprophylaxis in patients following total knee replacement. J Thromb Haemost. 2007;5(12):2368–2375. | ||
Botticelli Investigators, Writing Committee, Buller H, Deitchman D, Prins M, Segers A. Efficacy and safety of the oral direct factor Xa inhibitor apixaban for symptomatic deep vein thrombosis. The Botticelli DVT dose-ranging study. J Thromb Haemost. 2008;6(8):1313–1318. | ||
Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Hornick P; ADVANCE-2 investigators. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): a randomised double-blind trial. Lancet. 2010;375(9717):807–815. | ||
Nakamura M, Nishikawa M, Komuro I, et al. Apixaban for the treatment of Japanese subjects with acute venous thromboembolism (AMPLIFY-J Study). Circ J. 2015;79(6):1230–1236. | ||
Barrett YC, Wang J, Knabb R, Mohan P. Apixaban decreases coagulation activity in patients with acute deep-vein thrombosis. Thromb Haemost. 2011;105(1):181–189. | ||
Jiang X, Crain EJ, Luettgen JM, Schumacher WA, Wong PC. Apixaban, an oral direct factor Xa inhibitor, inhibits human clot-bound factor Xa activity in vitro. Thromb Haemost. 2009;101(4):780–782. | ||
Raghavan N, Frost CE, Yu Z, et al. Apixaban metabolism and pharmacokinetics after oral administration to humans. Drug Metab Dispos. 2009;37(1):74–81. | ||
Sardar P, Chatterjee S, Lavie CJ, et al. Risk of major bleeding in different indications for new oral anticoagulants: insights from a meta-analysis of approved dosages from 50 randomized trials. Int J Cardiol. 2015;179:279–287. | ||
Imberti D, Gallerani M, Manfredini R. Therapeutic potential of apixaban in the prevention of venous thromboembolism in patients undergoing total knee replacement surgery. J Thromb Thrombolysis. 2012;34(2):208–213. | ||
van der Hulle T, Kooiman J, den Exter PL, Dekkers OM, Klok FA, Huisman MV. Effectiveness and safety of novel oral anticoagulants as compared with vitamin K antagonists in the treatment of acute symptomatic venous thromboembolism: a systematic review and meta-analysis. J Thromb Haemost. 2014;12(3):320–328. | ||
Kakkos SK, Kirkilesis GI, Tsolakis IA. Editor’s choice – efficacy and safety of the new oral anticoagulants dabigatran, rivaroxaban, apixaban, and edoxaban in the treatment and secondary prevention of venous thromboembolism: a systematic review and meta-analysis of phase III trials. Eur J Vasc Endovasc Surg. 2014;48(5):565–575. | ||
Mantha S, Ansell J. Indirect comparison of dabigatran, rivaroxaban, apixaban and edoxaban for the treatment of acute venous thromboembolism. J Thromb Thrombolysis. 2015;39(2):155–165. | ||
Kang N, Sobieraj DM. Indirect treatment comparison of new oral anticoagulants for the treatment of acute venous thromboembolism. Thromb Res. 2014;133(6):1145–1151. | ||
Alotaibi G, Alsaleh K, Wu C, Mcmurtry MS. Dabigatran, rivaroxaban and apixaban for extended venous thromboembolism treatment: network meta-analysis. Int Angiol. 2014;33(4):301–308. | ||
Sobieraj DM, Coleman CI, Pasupuleti V, Deshpande A, Kaw R, Hernandez AV. Comparative efficacy and safety of anticoagulants and aspirin for extended treatment of venous thromboembolism: a network meta-analysis. Thromb Res. 2015;135(5):888–896. | ||
Pathak R, Pandit A, Karmacharya P, et al. Meta-analysis on risk of bleeding with apixaban in patients with renal impairment. Am J Cardiol. 2015;115(3):323–327. | ||
Mahmoudi M, Sobieraj DM. The cost-effectiveness of oral direct factor Xa inhibitors compared with low-molecular-weight heparin for the prevention of venous thromboembolism prophylaxis in total hip or knee replacement surgery. Pharmacotherapy. 2013;33(12):1333–1340. | ||
Amin A, Jing Y, Trocio J, Lin J, Lingohr-Smith M, Graham J. Evaluation of medical costs associated with use of new oral anticoagulants compared with standard therapy among venous thromboembolism patients. J Med Econ. 2014;17(11):763–770. | ||
Bauersachs RM. Guidelines for the management of cancer and thrombosis – special aspects in women. Thromb Res. 2015;135 Suppl 1:S13–S22. | ||
Vinereanu D, Stevens SR, Alexander JH, et al. Clinical outcomes in patients with atrial fibrillation according to sex during anticoagulation with apixaban or warfarin: a secondary analysis of a randomized controlled trial. Eur Heart J. 2015;36(46):3268–3275. | ||
Dentali F, Ageno W, Pomero F, Fenoglio L, Squizzato A, Bonzini M. Time trends and case fatality rate of in-hospital treated pulmonary embolism during 11 years of observation in Northwestern Italy. Thromb Haemost. Epub 2015 Sep 17. | ||
Zhang J, Chen Z, Zheng J, Breusch SJ, Tian J. Risk factors for venous thromboembolism after total hip and total knee arthroplasty: a meta-analysis. Arch Orthop Trauma Surg. 2015;135(6):759–772. | ||
Blanco-Molina A, Enea I, Gadelha T, et al. Sex differences in patients receiving anticoagulant therapy for venous thromboembolism. Medicine (Baltimore). 2014;93(17):309–317. | ||
Martín-Martos F, Trujillo-Santos J, Barrón M, et al. Gender differences in cancer patients with acute venous thromboembolism. Thromb Res. 2015;135 Suppl 1:S12–S15. | ||
Lapner S, Cohen N, Kearon C. Influence of sex on risk of bleeding in anticoagulated patients: a systematic review and meta-analysis. J Thromb Haemost. 2014;12(5):595–605. | ||
Dentali F, Sironi AP, Gianni M, et al. Gender difference in efficacy and safety of nonvitamin K antagonist oral anticoagulants in patients with nonvalvular atrial fibrillation or venous thromboembolism: a systematic review and a meta-analysis of the literature. Semin Thromb Hemost. 2015;41(7):774–787. | ||
Kneeland PP, Fang MC. Current issues in patient adherence and persistence: focus on anticoagulants for the treatment and prevention of thromboembolism. Patient Prefer Adherence. 2010;4:51–60. | ||
Nilsson H, Grove EL, Larsen TB, et al. Sex differences in treatment quality of self-managed oral anticoagulant therapy: 6,900 patient-years of follow-up. PLoS One. 2014;9(11):e113627. | ||
Forslund T, Ettermark B, Hjiemdahl P. Comparison of treatment persistence with different oral anticoagulants in patients with atrial fibrillation. Eur J Clin Pharmacol. Epub 2015 Nov 27. | ||
Castellucci LA, Shaw J, van der Salm K, et al. Self-reported adherence to anticoagulation and its determinants using the Morisky medication adherence scale. Thromb Res. 2015;136(4):727–731. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.