")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 11
Reducing HIV-related stigma and discrimination in healthcare settings: a systematic review of guidelines, tools, standards of practice, best practices, consensus statements and systematic reviews
Authors Feyissa GT , Lockwood C, Woldie M , Munn Z
Received 19 April 2018
Accepted for publication 31 May 2018
Published 28 August 2018 Volume 2018:11 Pages 405—416
DOI https://doi.org/10.2147/JMDH.S170720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Garumma Tolu Feyissa,1–3 Craig Lockwood,3 Mirkuzie Woldie,1,2,4 Zachary Munn3
1Department of Health, Behavior and Society, Jimma University, Jimma, Ethiopia; 2Ethiopian Evidence Based Healthcare Centre, JBI Center of Excellence, Jimma University, Jimma, Ethiopia; 3School of Public Health, The Joanna Briggs Institute, The University of Adelaide, Adelaide, SA, Australia; 4Department of Health Economics, Management and Policy, Jimma University, Jimma, Ethiopia
Introduction: Policy makers and health professionals prefer to use preappraised and summarized evidence. Stigma and discrimination (SAD) reduction activities and programs are needed to improve the quality of care delivered to people living with HIV and the success of HIV-related prevention, care and treatment programs. The objective of this review was to identify and describe systematic reviews, best practices, consensus statements, standards of practice and guidelines that addressed SAD among healthcare workers (HCWs).
Methods: All documents in the form of systematic reviews, best practices, consensus statements, standards of practice and guidelines were considered for inclusion. The search strategy aimed to find both published and unpublished studies reported in English with unlimited date range in Excerpta Medica Database from Elsevier (EMBASE), Cumulative Index to Nursing and Allied Health (CINAHL), Psychological Information (PsycINFO) database and Medical Literature Analysis and Retrieval System Online (MEDLINE). Websites of organizations and guideline databases were also searched. Two individuals independently appraised the quality of the documents using the Appraisal of Guidelines for Research and Evaluation (AGREE II) checklist and the Joanna Briggs Institute critical appraisal checklist for systematic reviews. Data extraction was done using a customized tool that was developed to record the key information of the source that is relevant to the review question.
Results: Twelve records (six guideline-related documents and six systematic reviews) were included in the review. Interventions and recommendations developed to reduce HIV-related SAD were categorized into information-based, structural, biomedical, counseling and support, skills building and contact interventions.
Conclusion: Implications for practice: Interventions that reduce HIV-related SAD are broadly categorized into information-based, structural, biomedical, counseling and support, skills building and contact interventions. Because of limited methodological description of the included documents, it was difficult to draw recommendations for policy and practice. Implications for research: Future studies need to use up-to-date instruments to measure SAD. Further studies of greater methodological quality are needed. Guidelines, tools and best practice documents that aim to reduce HIV-related SAD should be developed with the considerations of research evidence on the specific setting and specific targeted populations.
Keywords: HIV, stigma, guideline, systematic review
Introduction
Policy makers and health professionals need high-quality research evidence to make decisions on public health and clinical practice. However, they are being challenged with an overwhelmingly increasing volume of research published everyday.1 Taking the increasing volume of published research evidence into account, systematic reviews are being prioritized to make policy and practice decisions.1 Nevertheless, because of the limited time, health managers and health professionals prefer evidence in a summarized form such as guidelines and evidence summaries.2 Particularly, they prefer to use preprocessed and summarized evidence.2,3
Cognizant of this, scholars and organizations, such as the Joanna Briggs Institute (JBI), have developed a system to avail evidence at the point of care through presenting evidence in a summarized and usable format.2 Some scholars have developed a hierarchical model to search for and utilize preappraised bodies of evidence.3 The list from top down in the hierarchy includes the following: 1) systems (computerized decision support systems); 2) summaries such as evidence-based practice guidelines; 3) synopsis of syntheses; 4) syntheses of primary studies; 5) synopsis of single studies and 6) single studies.4,5 According to this model, while making a decision in healthcare practice, one always should start from the top and proceed down until one gets the best available evidence saving time and resources.5
Currently, only a few systems-level evidence are available. Hence, the highest universally available evidence for most health topics is summaries.5 As one example of summary-level evidence, guidelines are accessible worldwide through different organizational web pages and publications. Guidelines offer options for practitioners, policy makers and patients to make informed decisions to improve the outcomes of patients. Guidelines are believed to improve the quality of healthcare practice by making explicit recommendations on specific healthcare practice.6 Guidelines also reduce variations in practice.7
The lack of uniformity in handling people living with HIV (PLHIV) such as differential treatment, denial of treatment or differential or excessive use of barriers is considered as discrimination.8,9 The fear of being stigmatized discourages PLHIV from disclosing their serostatus to families, friends and healthcare workers (HCWs) and getting healthcare services and the support they need.10 To this end, globally, there has been effort to reduce stigma and discrimination (SAD) related to HIV.11,12 It has been indicated that the absence of guidelines and protocols that protect PLHIV from SAD was associated with higher levels of SAD among HCWs.13,14 Researchers recommend theory and evidence-based interventions15 and policies and guidelines14 to direct SAD reduction activities.
Evidence-based SAD reduction activities and programs are urgently needed to improve the quality of care delivered to PLHIV and the success of HIV-related prevention, care and treatment programs.14,16 There should be healthcare facility-level policies and practice that support SAD reduction activities.16 In line with this, it is imperative to identify and summarize the best available evidence to inform policy and practice on HIV-related SAD. To this end, this review aimed to identify and describe systematic reviews, best practices, consensus statements, standards of practice and guidelines that have addressed HIV-related SAD among HCWs and/or in healthcare settings.
This review sought to locate and describe international literature in the form of guidelines, tools, best practice documents, consensus statements and systematic reviews that contained recommendations and/or interventions for reducing HIV-related SAD.
Specifically, the review aimed to the following:
- To identify and describe guidelines, tools, consensus statements and best practice statements containing recommendations or interventions to reduce HIV-related SAD.
- To identify systematic reviews containing findings, conclusions and recommendations to reduce SAD related to HIV.
Participants and methods
Report included in this systematic review was prepared using Preferred Reporting Items for Systematic Reviews and Meta-analysis reporting guidelines for systematic reviews.17 For this review, we considered the following inclusion criteria.
Population
This review considered HCWs, health managers, PLHIV and healthcare institutions.
Interventions
Records were considered for inclusion if they contained research results or recommendations to reduce HIV-related SAD. This review considered the following interventions:
- targeting health professionals such as training and
- related to health institution policies such as institutional protocols and standards.
Comparators
Comparisons considered were as follows: no intervention or baseline intervention or one intervention compared to the other.
Outcomes
The primary outcomes considered for inclusion were HIV-related SAD among HCWs or healthcare institutions. Stigma reported in the form of fear-based stigma, value-based stigma and discrimination and internalized stigma was included. The secondary outcome considered was PLHIV-specific extra precaution.
Context
This review considered all documents and studies conducted worldwide that addressed HIV-related SAD among HCWs and in healthcare settings.
Types of studies/documents
This review considered all documents in the form of systematic reviews, consensus statements, best practice statements, standards of practice, tools and guidelines that report on the interventions or recommendations to reduce SAD related to HIV. Both published and unpublished (gray literature) studies reported in the English language were considered. Reviews that did not indicate inclusion and exclusion criteria, and an appraisal process, were not considered as systematic reviews. Guideline documents that did not indicate recommendations specific to the reduction of HIV-related SAD in healthcare settings were not included in this review. Scoping reviews, critical reviews or systematic reviews with the lack of specific focus and inclusion criteria for the inclusion of interventions or trials were excluded. Interventions such as specific treatments for PLHIV diagnosed with mental disorders were not considered. In addition, interventions beyond the scope of healthcare facilities such as financial interventions were not the focus of current review.
Search strategy
The search strategy aimed to find both published and unpublished studies. A three-step search strategy was utilized in this review. An initial limited search of Cumulative Index to Nursing and Allied Health (CINAHL) and Medical Literature Analysis and Retrieval System Online (MEDLINE) was undertaken followed by an analysis of the text words contained in the title and abstract and of the index terms used to describe the article. A second search using all identified keywords and index terms was then undertaken across all included databases. Third, the reference list of all identified reports and articles was searched for additional studies. Both published and unpublished papers reported in English language were searched with no restriction to age, country and date of publication. The databases searched included the following: Excerpta Medica Database from Elsevier (EMBASE), CINAHL, MEDLINE and Psychological Information (PsycINFO) database. The search for unpublished studies included the following: HIVinSite, AIDSinfo, HIV and AIDS clearinghouse, Communicable Diseases Control HIV publications, British HIV Association websites, Health Policy Project (HPP) website, United States Aid for International Development (USAID) experience clearinghouse, WHO guidelines and Joint United Nations Program on HIV/AIDS (UNAIDS) publications. An additional search was conducted for the existing guidelines and systematic reviews in the following websites: Turning Research into Practice (TRIP) database, Guideline International (GIN) library, National Guideline Clearinghouse (NGC), National Institute for Health and Clinical Excellence (NICE) and Task Force on Community Preventive Services. A detailed search strategy for each database is reported in Table S1.
Assessment of methodological quality
Two individuals independently appraised the quality of the guideline documents using the Appraisal of Guidelines for Research and Evaluation (AGREE II) checklist18 (Table S2). The AGREE II checklist has six domains, namely scope and purpose (three items), stakeholder involvement (three items), rigor of development (eight items), clarity of presentation (three items), appropriateness (four items) and editorial independence (two items).18 The reviews were independently assessed by two individuals using the JBI critical appraisal checklist for systematic reviews (Figure S1).
Data extraction
Data extraction was done using a format developed to record the key information of the source relevant to the review question. The data extraction instrument was developed both for systematic reviews and guideline-related documents. Relevant information such as population characteristics, publication year, authors and summary of the findings and recommendations were extracted.
Results
The search yielded a total of 1670 records. After removing duplicates, 1605 documents were retained for further analysis. Based on the analysis of the titles and abstracts, 118 records were retained for further full-text analysis. Based on predefined inclusion criteria, we retained 12 records (Figure 1). Six of the records were guideline-related documents (best practice, tools and standards of practice), and six of the records were systematic reviews.
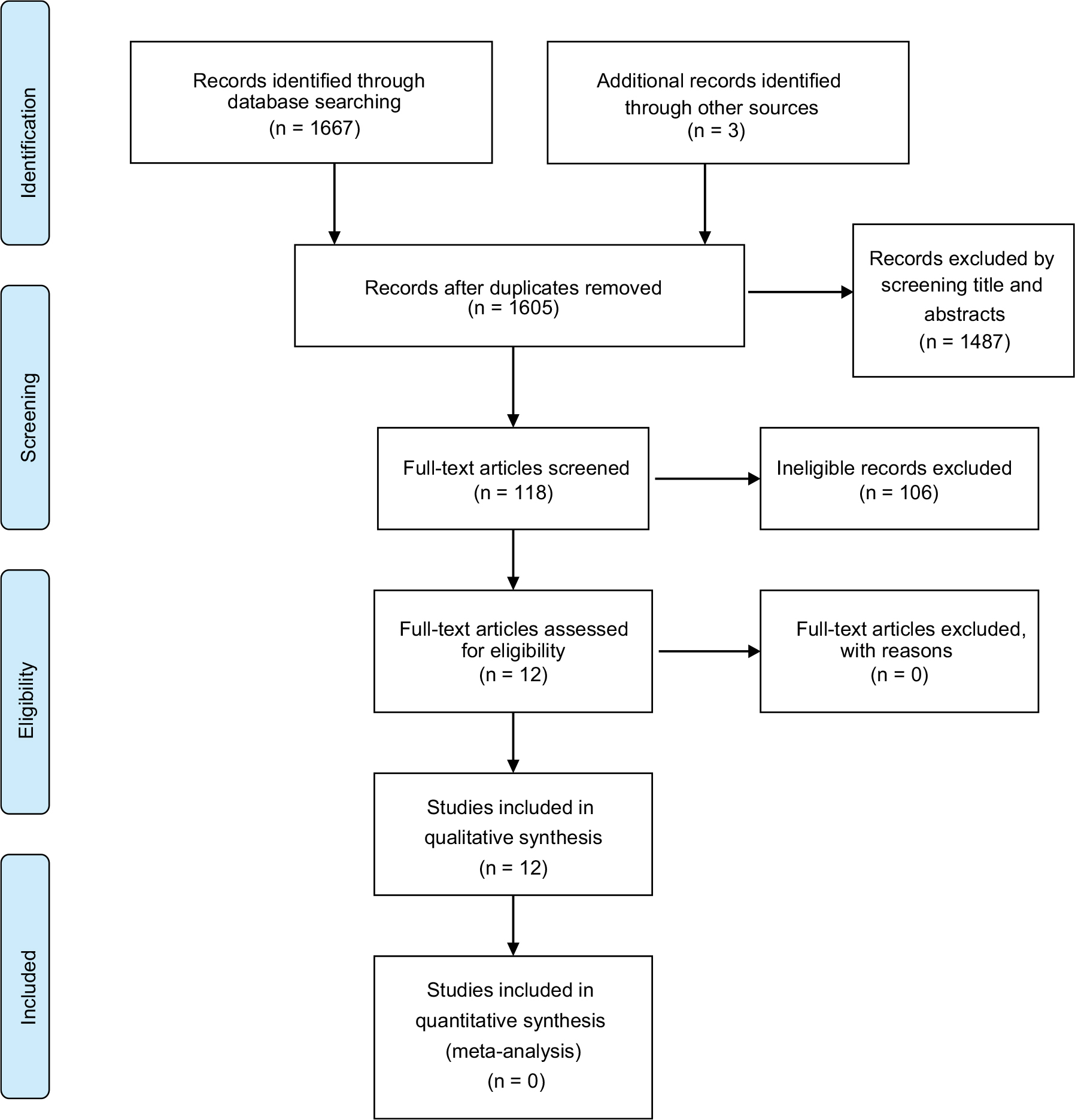 | Figure 1 Study selection process for systematic review of guidelines, best practices and systematic reviews. |
Description of the characteristics of the documents
Guidelines, best practice documents, standards of practice and tools
Among the six guideline-related documents, two were published by the USAID19,20 and one was published by the Department for International Development (DFID),21 one by Physicians for Human Rights (PHR),22 one guideline document was developed by the UNAIDS23 and one national guide24 was published by Tanzania Commission for AIDS (TCA) (Table 1). The guidelines were assessed against AGREE II reporting criteria.25
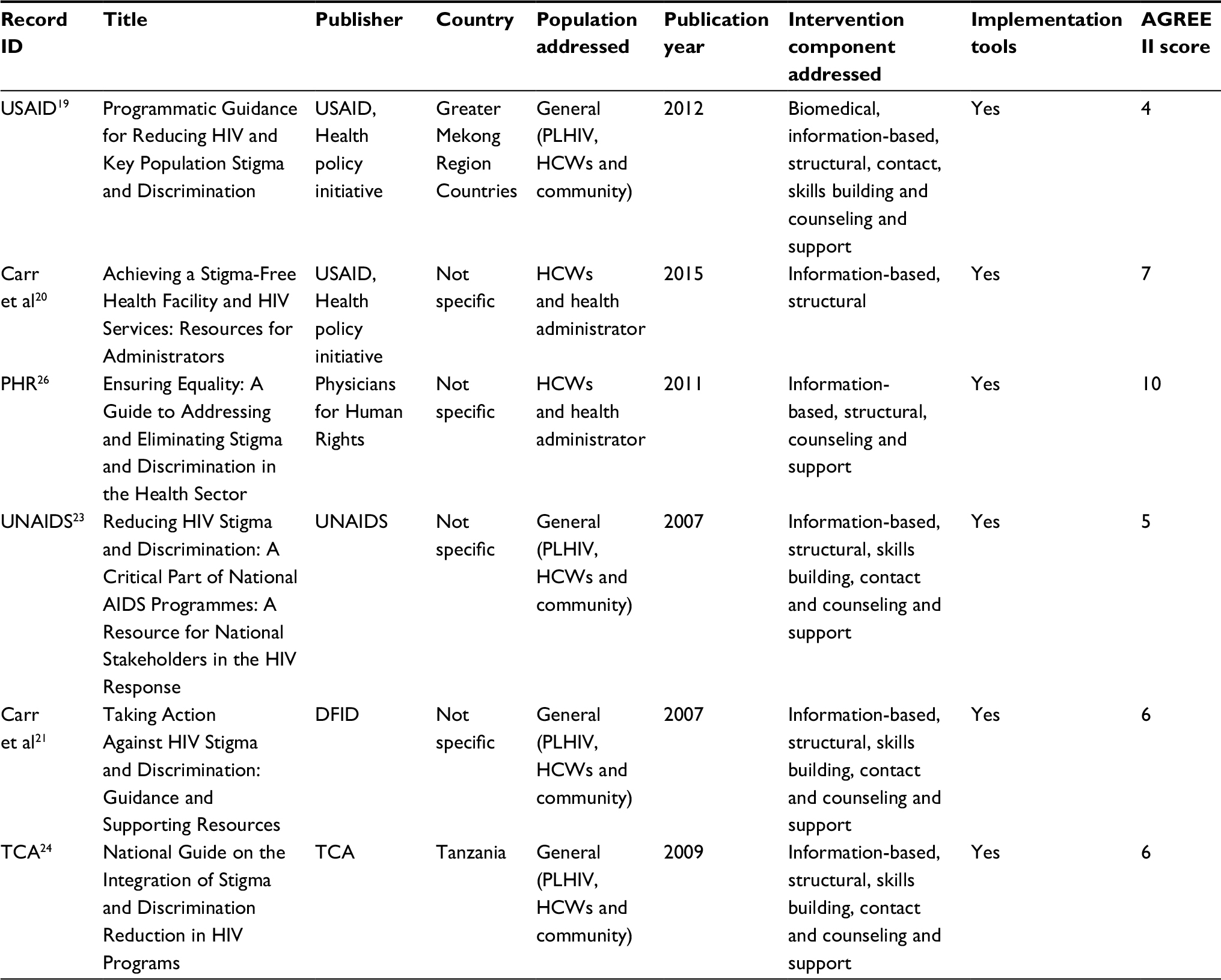 | Table 1 Summary of guideline topics and citation details Abbreviations: AGREE, Appraisal of Guidelines for Research and Evaluation; USAID, United States Aid for International Development; PLHIV, people living with HIV; HCWs, healthcare workers; PHR, Physicians for Human Rights; UNAIDS, United Nations program on HIV/AIDS; DFID, Department for International Development; TCA, Tanzanian Commission of AIDS. |
USAID (2012)
The first guide (USAID, 2012),19 which was published by the USAID health policy initiative in 2012, provided an overview of HIV epidemics and the impact of HIV-related SAD. The guide developed the recommendations under six guiding principles. This guide addressed four criteria out of the 23 criteria on AGREE II reporting checklist. It provides advice on how to implement the recommendations into practice. The guide had resources for implementation such as tool kits. Although it indicates and cites existing research evidence in the recommendations, it does not explicitly indicate the link between recommendations and research evidence. It does not provide details on how the recommendations were developed. Even though the guideline provides recommendations to be applied in healthcare settings, the target of most of the recommendations was not specifically described. The specific health questions considered the potential resource implications of the recommendations, and whether a systematic search was used to develop the recommendations were not described. Recommendations found in the guide addressed biomedical, information-based, structural, contact, skills building and counseling and support interventions.
Carr et al (2015)
The second guide (Carr et al, 2015)20 was published by the USAID health policy initiative. The guide addressed seven of the AGREE II criteria for reporting guidelines. The guide was specifically developed to reduce HIV-related SAD in healthcare settings. It was developed by the synthesis of existing programs, tools and research evidence. However, details of how the developers located these sources were not described. The guide had added resources for implementation, including tool kits, health facility and provider assessment checklists. The recommendations included in the guideline were under the categories of information-based and structural interventions.
PHR (2011)
The third guide (PHR, 2011)26 was developed by physicians for PHR. This guideline addressed 10 of the criteria for AGREE II reporting standards. The recommendations in the guideline were easily identifiable. The guide indicated tools and references that supported the recommendations. The guide addressed the roles of different actors to reduce SAD in healthcare settings. The guide was based on examples and experiences of previous research and programs. Nevertheless, it did not indicate the details of the development process. Moreover, the link between the recommendations and the research evidence was not explicitly reported. While most of the citations were from the field of HIV-related stigma, it also included citations from other diseases, such as leprosy. Recommendations found in the guideline generally fell under information-based, structural, counseling and support approaches to SAD reduction.
UNAIDS (2007)
The fourth guide (UNAIDS, 2007)23 was published by UNAIDS. This guide addressed five of the 23 AGREE II criteria for reporting guidelines. It provided programmatic examples, research findings and resources for the reduction of SAD. However, the details of the retrieval of this body of evidence and the process of the development of the recommendations were not described. The guideline recommendations were under the categories of information-based, structural, skills building, contact and counseling and support approaches.
Carr et al (2007)
The fifth guide (Carr et al, 2007)21 was developed by the DFID. This document addressed six of the 23 AGREE II criteria for reporting guidelines. The guideline presented best practice and lessons learnt to tackle SAD. It provided resources for implementation. However, it did not detail the process for the development of recommendations. It was mainly developed for DFID and their partners. Moreover, the settings where recommendations were to be implemented were not clearly described. The guideline addressed recommendations that comprised information-based, structural, skills building, contact and counseling and support domains of SAD reduction interventions.
TCA (2009)
The sixth guide (TCA, 2009)24 was developed by the TCA. This guideline addressed six of the 23 AGREE II reporting criteria for guidelines. The guide focused on how to integrate SAD reduction in HIV programs. It cited some research and tool kits. The guideline mentions that it was developed based on lessons and experiences obtained in research and implementation programs. Nevertheless, the process of developing that guide was not detailed. The guideline addressed SAD reduction interventions falling under information-based, structural, skills building, contact and counseling and support interventions.
In all the documents, the expected update timeline and process were not mentioned. The results of assessment based on AGREE II reporting criteria for each guideline are given in Table S3. As none of the guidelines and tools mentioned any information on the quality of the recommendation or the design of the linked references, it was difficult to extract recommendations.
Systematic reviews
Four of the six systematic reviews12,27,28,29 scored 9/11 using the JBI critical appraisal checklist for systematic reviews. One qualitative review by Chamber et al31 scored 7/11. One quantitative review by Brown et al30 scored 4/11. All reviews did not assess the likelihood of publication bias. None of the systematic reviews combined the findings of the studies using meta-analysis. All reviews (except the one by Brown et al30) indicated clear and comprehensive search strategies and included both published and unpublished studies. However, formal assessment of risk of publication bias was not indicated in all the systematic reviews. Two of the included reviews30,31 reported the appraisal criteria, process and results explicitly (Table 2). The appraisal results for the systematic reviews are given in Table S2.
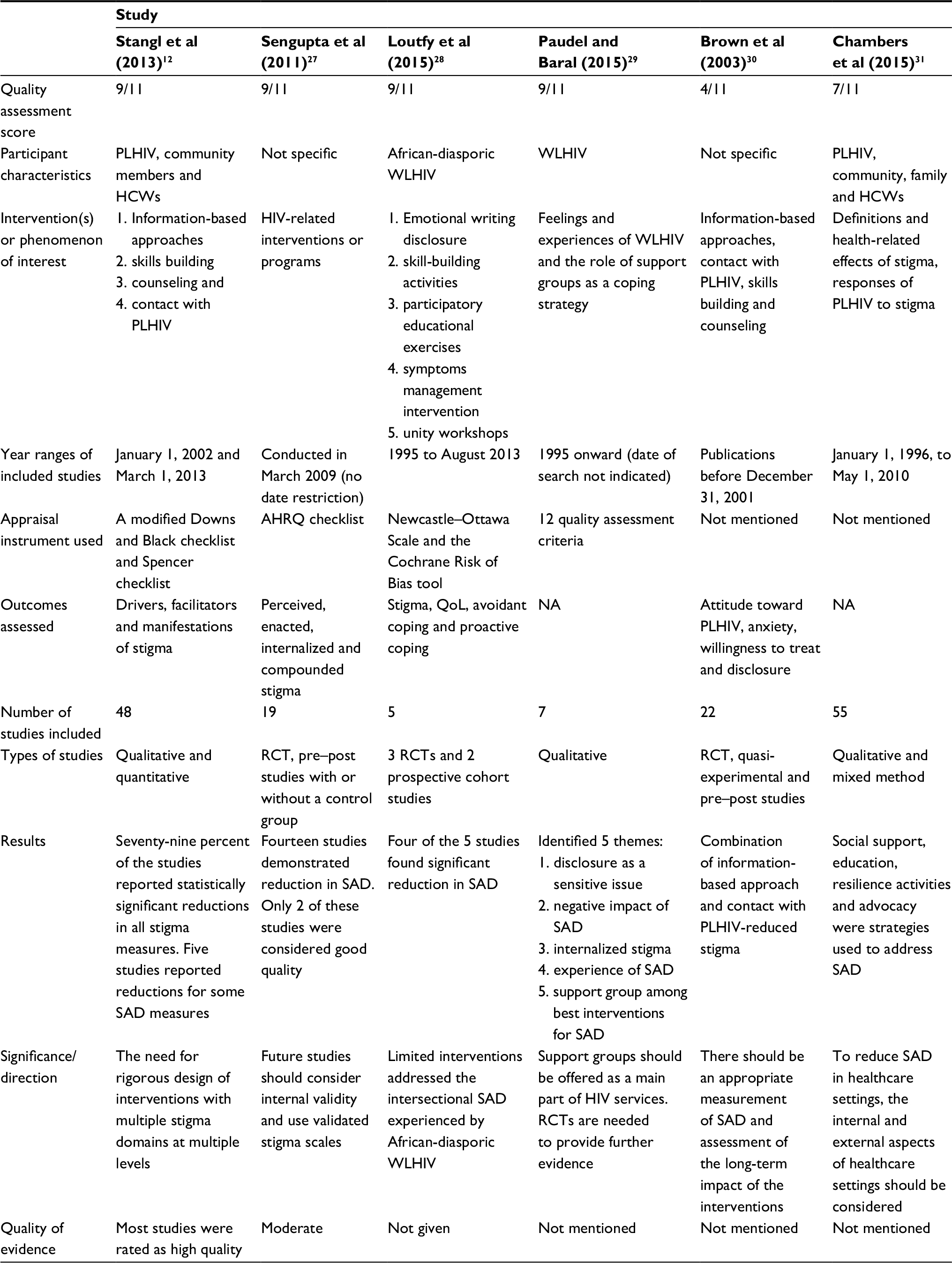 | Table 2 Description of systematic reviews Abbreviations: PLHIV, people living with HIV; HCWs, healthcare workers; WLHIV, women living with HIV; AHRQ, Agency for Healthcare Research and Quality; QoL, quality of life; NA, not applicable; RCT, randomized controlled trial; SAD, stigma and discrimination. |
Stangl et al (2013)
The systematic review by Stangl et al12 aimed to obtain a complete picture of intervention efforts in interrupting SAD and included 48 studies. The included studies were randomized controlled trials (RCTs), quasi-experimental designs with and without control groups, repeated cross-sectional surveys, qualitative studies and mixed method studies.12 The review conceptualized domains of SAD and stigma reduction approaches as follows:
- Domains of HIV-related SAD: the authors categorized HIV-related stigma domains into drivers, facilitators and manifestation domains. Drivers are individual-level factors that negatively influence the stigmatization process.12 Manifestations of stigma include how stigma is executed or experienced.12
- HIV-related SAD reduction approaches: the authors categorized the interventions into information-based, skills building, counseling and support, contact, structural and biomedical interventions.12
As indicated in the review, most programs used information-based approaches, but some used a combination of two or more of these approaches. The information-based approaches were both written and verbal information to increase the understanding of HIV and of SAD. These were provided in the form of leaflets, brochures and other methods.12 The structural approaches to SAD reduction employed in healthcare settings were availing supplies for standard precautions, revision and development of standard operating procedures (SOPs), policies and regulations and putting a grievance addressing system in place.12 Biomedical approaches are interventions such as universal access to care and treatment.12 Contact strategies are activities such as testimonials of PLHIV and activities that encourage interaction between HCWs and PLHIV. Counseling and support approaches are activities that aid in minimizing the negative psychosocial impact of HIV-related SAD on clients and their families.12
The review conceptualized levels and targets of SAD reduction interventions as follows:
- Levels of HIV-related SAD reduction interventions: the review considered a range of interventions at the individual, interpersonal, organizational and community and public policy levels. At the individual level, interventions were targeted to influence how individuals feel about HIV and how they respond to it. At the interpersonal level, interventions addressed stigma between individuals, including family and friends. At the organizational level, interventions addressed stigma within institutions, such as schools and hospitals. At the public policy level, interventions addressed stigma that was reflected in public laws or policies.12
- Targets of SAD reduction interventions: the review comprised interventions that targeted various population groups, including HCWs, PLHIV, female sex workers and men who have sex with men.12
In this review, 38 (79%) of the included studies reported statistically significant reductions in all stigma measures. Five studies reported reductions in some stigma measures. The review, however, did not pool the findings from the primary studies because of heterogeneity of the interventions and measures used in the primary studies. The authors called for more rigor and improved quality studies and future interventions to address intersectional stigma (multiple prejudices experienced by clients both because of their disease status and their other attributes such as sexual activity or orientation).12
Sengupta et al (2011)
The review by Sengupta et al27 assessed the effectiveness of HIV-related interventions to reduce HIV-related SAD. The review included 19 studies. The designs of the included studies were RCTs and pre–post study designs with and without control groups. This review identified interventions that targeted a range of population groups such as students, HCWs, working women and the general community. The included studies addressed information-based approaches, PLHIV testimonials, skills building, support groups and a combination of these approaches.27 Outcomes reported were perceived, enacted, internalized and compounded stigma. Fourteen of the included studies demonstrated a reduction in HIV-related SAD. Only two of these studies were considered good quality by the reviewers. The reviewers called for further studies with good internal validity and employing validated measures of stigma.27
Loutfy et al (2015)
The review Loutfy et al28 identified studies addressing interventions to reduce HIV-related SAD among African diasporic women living with HIV (WLHIV). The review included three RCTs and two prospective cohort studies. The included studies measured internalized stigma (holding negative attitude against oneself) and perceived stigma (awareness of social devaluation, social rejection, diminished social identity and limited social opportunity attributed to stigma). Four of the studies demonstrated a positive effect in the reduction of HIV-related SAD among WLHIV. The reviewer concluded that the included studies addressed interpersonal and intrapersonal stigma. The authors recommended further research to address SAD at community, institutional or structural levels. They also concluded that there was a lack of research evidence addressing intersectional SAD experienced by African diasporic WLHIV.28
Paudel and Baral (2015)
The review by Paudel and Baral29 examined the feelings, experiences and perceptions of WLHIV and assessed the role of support groups as a coping strategy from seven qualitative studies. The review identified the following five themes: 1) disclosure is a sensitive issue for WLHIV; 2) WLHIV have physical, social, emotional and spiritual difficulties in dealing with SAD from family, friends, community and health professionals; 3) internalized or self-stigma affects WLHIV more than the actual experience of stigma; 4) WLHIV are rejected, shunned and treated differently by physicians, family and close friends and 5) support groups are among the best interventions for HIV-related SAD. Based on the findings, the authors recommended that support group interventions should constitute the main approach for HIV programs. They also recommended additional RCTs to demonstrate the effectiveness of support group interventions.29
Chambers et al (2015)
The review by Chambers et al31 analyzed and presented the findings of 55 qualitative studies into three categories. These included the conceptualization of HIV-related SAD, which included dimensions of stigma, experiences of stigma and managing stigma. The review also showed that healthcare practice was negatively affected by personal stigmatizing perceptions of practitioners. The reviewers also found that feeling stigmatized negatively influenced health services utilization, adherence to treatment and overall health and well-being of PLHIV. In addition, the review reported that HIV-related SAD in healthcare settings was interlinked with other forms of marginalization due to sexual behavior or orientation, race, gender and other factors. This is called intersectional or double stigma. The review identified social support, education, self-efficacy, resilience activities and advocacy as major strategies to address HIV-related SAD.31
Brown et al (2003)
The review by Brown et al30 included 22 studies that reported on interventions to reduce SAD related to HIV. Among the included studies, 14 reported on interventions aimed to reduce SAD toward PLHIV among the general population, and five studies included interventions aimed at increasing the willingness of HCWs to treat PLHIV. Three studies aimed to improve coping strategies to deal with HIV-related stigma using counseling and information-based approaches. Most studies included in this review found that information combined with a skill-building approach was more effective than the information-only approach to reduce HIV-related SAD in the general population. The studies also found that contact with PLHIV was more effective in reducing HIV-related SAD when combined with information provision than a contact-only approach. Taking the limitations of the included studies into account, the authors recommended for the utilization of validated scales of measurement to aid appropriate measurement of HIV-related SAD and assessment of the long-term impact of the interventions. The settings, population characteristics and summarized findings extracted from the systematic reviews are shown in Table 2. None of the systematic reviews reported a meta-analysis or a summary of findings (SoF) table.
Discussion
In this review, we attempted to locate documents in the form of guidelines, consensus statements, best practice statements, standards of practice and systematic reviews indicating directions on how to tackle SAD. In this project, we searched both published and gray literature to locate the evidence on SAD related to HIV. Acknowledging SAD as a significant barrier to HIV prevention and control programs32 and its negative impact on clients,10 for more than 3 decades, organizations have been working to reduce SAD related to HIV,33 and through time, implementers and researchers are improving practice, based on the lessons they learn from their experiences.33
In addition to the interventions and primary studies conducted so far, researchers have tried to identify the global evidence to reduce SAD related to HIV and present the evidence in the form of guidelines, best practice statements and systematic reviews.12 Through these efforts, they have understood and conceptualized the interventions falling under the following general categories: information-based interventions, structural interventions, biomedical interventions, counseling and support, skills building and contact strategies.12
The quality of the five of the systematic reviews included in this review was generally good. Nevertheless, in this review, we could not obtain evidence in a usable form. Systematic reviews are supposed to facilitate the guideline development and knowledge translation process.34 The following were missing from the reviews included in the current project: indication of the quality of the findings and pooling the results of the primary studies or presenting SoF tables to inform policy and practice. There were no meta-analyses conducted on interventions to reduce HIV-related SAD. Hence, it was very difficult to draw conclusions from the findings of the systematic reviews. One of the reasons that contributed to these gaps was the fact that stigma measures were not always uniform across different studies.12,27,30 The other reason was that the interventions, most of which were behavioral in nature, were not always similar across different studies in mode of delivery, duration of delivery and type of population they addressed.12,27 Public health interventions are often complex and this makes the systematic review challenging.35 In circumstances where the interventions were found to be similar, the study designs or the populations varied.12,27 In addition, programs and policy implementers also need to consider other factors such as the degree to which the interventions described in the protocols were implemented (intervention fidelity).35
As was recommended in most of the systematic reviews, it is vital to focus on the design of the studies which includes paying attention to internal validities and using validated instruments to measure SAD.12,27,28,30 Future studies may fill these gaps as stigma instruments have been evolving over time. This, however, will be possible only if the researchers are aware of the recent developments in measurements and scales. The other limitation that the reviews had was that some did not report the findings specifically within different population subgroups and settings.12,27
Different guidelines and best practice documents were developed worldwide based on the lessons learnt from primary studies and implementation programs.19,21,24,26 Efforts were made to develop standard tools and instruments to reduce HIV-related SAD and to monitor these efforts.20 Nonetheless, most of these guideline-related documents did not indicate the details of how they developed the recommendations and the scientific rigor of their methods. The guidelines and best practice documents for addressing HIV-related SAD were developed based on the experiences of implementers and best practices in tackling SAD. In most of these documents, however, detailed information on how these best practice documents were located, selected, appraised and created was missing.
The systematic reviews included in this review did not give conclusion on direction regarding the specific nature, content and duration of an ideal psychological intervention to help HCWs living with HIV cope with stigma or secondary stigma.36 One of the strengths of the guideline documents on the reduction of HIV-related SAD included in this review was that implementers of stigma reduction programs in the field of HIV had good networks and collaborations20,21 and most of these implementers developed the guidelines based on their work worldwide.23,33 This might have been because the funding organizations were working worldwide.
Because of the limitations in the transparency of how the reviews and the guideline-related documents were developed, putting them into practice and setting priorities for specific intervention is challenging. While drawing conclusions from the reviews and guideline documents available to date, it is very important to consider the details of the primary studies linked to these documents. The context in which the primary studies linked to these documents were conducted (healthcare settings, community, media and faith-based organizations) and the target beneficiaries involved in the original primary studies must be examined. The intervention might have been effective or not effective, simply because of preexisting contextual factors.35,37 In addition, details of the intervention characteristics such as the providers of the intervention and the fidelity of the intervention are worthy of consideration.37,38
In healthcare settings, additional factors exist, which fuel SAD related to HIV. Some of these factors are specific to the practice of HCWs, such as fear of casual transmission, and limited knowledge of what stigma is and its negative consequences. Hence, these factors should be addressed through skills building and infrastructural interventions such as availing universal precaution supplies.9 This makes the stigma related to HIV in healthcare settings different from HIV-related SAD in other settings. However, some of the guideline-related documents included in this review have extrapolated community-based findings to healthcare settings.26 It is therefore essential to develop context- and population-specific recommendations and guidelines that help to improve accountability for monitoring and evaluation, as well as those that support efficient delivery of audience-specific recommendations.
It is critical to consider the specific nature of SAD related to HIV. Stigma related to HIV results from associating HIV with immoral or unacceptable behaviors.9 However, only two of the guideline-related documents identified in this review were specific with respect to the setting or population or the disease condition they addressed.19,23 In some of the guideline-related documents, although most of the evidence was drawn from HIV-related SAD, the guidelines also drew recommendations based on interventions that were found effective in addressing stigma related to other disease conditions such as leprosy.26 Hence, organizations or programs working on SAD reduction should consider the settings and specific population for which each of these interventions should be applied.
On the other hand, it is encouraging to see some of the guidelines mentioning the roles of different stakeholders in reducing SAD in healthcare settings.19 As clearly indicated in the guidelines, it is imperative to consider that stigma in healthcare settings is affected by the factors and actors beyond healthcare settings.19,26
Conclusion
Implications for practice: SAD reduction interventions are framed as information-based, skills building, structural, biomedical, counseling and support and contact-based approaches. Currently existing systematic reviews and guideline-related documents are not transparent enough to provide details of the quality of evidence supporting the recommendations. Implications for research: Although good-quality systematic reviews exist, they were not presented in a usable form. Future systematic reviews should address this by including SoF tables. Future studies need to use up-to-date stigma instruments to measure HIV-related SAD. Studies with rigorous designs, such as RCTs, are needed.
Acknowledgments
The authors are grateful to Siang Tay for editing the report. This study was conducted as part of GTF’s PhD project, which was supported by the Adelaide Scholarship International (ASI) granted by the University of Adelaide. The authors did not receive any funding for this research.
Author contributions
GTF performed the formal analysis, was responsible for project administration, and wrote the original draft of the manuscript. All authors contributed to conception of the study, methodology, data curation, validation, visualization, data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interests in this work.
References
Bastian H, Glasziou P, Chalmers I. Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PLoS Med. 2010;7(9):e1000326. | ||
Munn Z, Lockwood C, Moola S. The development and use of evidence summaries for point of care information systems: a streamlined rapid review approach. Worldviews Evid Based Nurs. 2015;12(3):131–138. | ||
Windish D. Searching for the right evidence: how to answer your clinical questions using the 6S hierarchy. Evid Based Med. 2013;18(3):93–97. | ||
Robeson P, Dobbins M, DeCorby K, Tirilis D. Facilitating access to pre-processed research evidence in public health. BMC Public Health. 2010;10(1):95. | ||
DiCenso A, Bayley L, Haynes RB. Accessing pre-appraised evidence: fine-tuning the 5S model into a 6S model. Evid Based Nurs. 2009;12(4):99–101. | ||
Woolf SH, Grol R, Hutchinson A, Eccles M, Grimshaw J. Potential benefits, limitations, and harms of clinical guidelines. Br Med J. 1999;318(7182):527. | ||
Harrison M, Van Den Hoek J. CAN-IMPLEMENT: A Guideline Adaptation and Implementation Planning Resource. Kingston: Queen’s University School of Nursing and Canadian Partnership Against Cancer; 2012. | ||
Feyissa GT, Abebe L, Girma E, Woldie M. Stigma and discrimination against people living with HIV by healthcare providers, Southwest Ethiopia. BMC Public Health. 2012;12:522. | ||
Nyblade L, Stangl A, Weiss E, Ashburn K. Combating HIV stigma in health care settings: what works? J Int AIDS Soc. 2009;12:15. | ||
Vanable PA, Carey MP, Blair DC, Littlewood RA. Impact of HIV-related stigma on health behaviors and psychological adjustment among HIV-positive men and women. AIDS Behav. 2006;10(5):473–482. | ||
Stangl AL, Grossman CI. Global action to reduce HIV stigma and discrimination. J Int AIDS Soc. 2013;16(3 Suppl 2):18934. | ||
Stangl AL, Lloyd JK, Brady LM, Holland CE, Baral S. A systematic review of interventions to reduce HIV-related stigma and discrimination from 2002 to 2013: how far have we come? J Int AIDS Soc. 2013;16(3 Suppl 2):18734. | ||
Salih MH, Tessema GA, Cherkos EA, Ferede AJ, Zelalem Anlay D. Stigma towards people living on HIV/AIDS and associated factors among nurses’ working in Amhara region referral hospitals, Northwest Ethiopia: a cross-sectional study. Adv Nurs. 2017;2017:1–7. | ||
Wodajo BS, Thupayagale-Tshweneagae G, Akpor OA. Stigma and discrimination within the Ethiopian health care settings: views of inpatients living with human immunodeficiency virus and acquired immune deficiency syndrome. Afr J Prim Health Care Fam Med. 2017;9(1):1314. | ||
Bos AE, Schaalma HP, Pryor JB. Reducing AIDS-related stigma in developing countries: the importance of theory- and evidence-based interventions. Psychol Health Med. 2008;13(4):450–460. | ||
Jain A, Nyblade L. Scaling up Policies, Interventions, and Measurement for Stigma-Free HIV Prevention, Care and Treatment Services. Washington, DC: The Health Policy Project; 2012. | ||
Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. | ||
NCCMT. Critically Appraising Practice Guidelines: The AGREE II Instrument. Hamilton: McMaster University; 2011 [updated November 1, 2013]. Available from: http://www.nccmt.ca/registry/view/eng/100.html. Accessed July 13, 2018. | ||
USAID. Health Policy Initiative. Programmatic Guidance for Reducing HIV and Key Population Stigma and Discrimination: For the Greater Mekong Region Countries of Thailand, Lao PDR and Myanmar. Bangkok: USAID; 2012. | ||
Carr D, Kidd R, Nyblade L. Achieving a Stigma-Free Health Facility and HIV Services: Resources for Administrators. Washington, DC: Futures Group, Health Policy Project; 2015. | ||
Department for International Development. Taking Action Against HIV Stigma and Discrimination: Guidance Document and Supporting Resources; 2007. Available from: https://www.icrw.org/wp-content/uploads/2016/10/DFID-Taking-Action-Against-HIV-Stigma-and-Discrimination.pdf. Accessed August 13, 2018. | ||
Peugh L, Friedman E. Ensuring Equality: A Guide to Addressing and Eliminating Stigma and Discrimination in the Health Sector. Cambridge, MA, Washington, DC: Physicians for Human Rights; 2011. | ||
UNAIDS; Joint United Nations Programme on HIV/AIDS. Reducing HIV Stigma and Discrimination: A Critical Part of National AIDS Programmes: A Resource for National Stakeholders in the HIV Response. UNAIDS; 2007. Available from: http://data.unaids.org/pub/report/2008/jc1521_stigmatisation_en.pdf. Accessed August 13, 2018. | ||
Jamhuri ya Muungano wa Tanzania; Ofisi ya Waziri Mkuu [Tanzania Commision for AIDS]. Mwongozo wa kitaifa wa Kuhusisha kupunguza Unyanyapaa na Ubaguzi katika Programu za Virusi Vya UKIMWI [National Guide on the Integration of Stigma and Discrimination Reduction in HIV Programs]; 2009. Available from: https://www.icrw.org/sites/default/files/images/National-Guide-on-the-Integration-of-Stigma-and-Discrimination-Reduction-in-HIV-Programs-Kiswahili.pdf. Accessed August 14, 2018. Kiswali. | ||
Brouwers MC, Kerkvliet K, Spithoff K, Consortium ANS. The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. BMJ. 2016;352:i1152. | ||
PHR. Guide to Reducing Stigma and Discrimination in the Health Sector. 2011. Available from: http://physiciansforhumanrights.org/library/other/stigma-reduction-guide.html. Accessed July 13, 2018. | ||
Sengupta S, Banks B, Jonas D, Miles MS, Smith GC. HIV interventions to reduce HIV/AIDS stigma: a systematic review. AIDS Behav. 2011;15(6):1075–1087. | ||
Loutfy M, Tharao W, Logie C, et al. Systematic review of stigma reducing interventions for African/Black diasporic women. J Int AIDS Soc. 2015;18:19835. | ||
Paudel V, Baral KP. Women living with HIV/AIDS (WLHA), battling stigma, discrimination and denial and the role of support groups as a coping strategy: a review of literature. Reprod Health. 2015;12:53. | ||
Brown L, Macintyre K, Trujillo L. Interventions to reduce HIV/AIDS stigma: what have we learned? AIDS Educ Prev. 2003;15(1):49–69. | ||
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health. 2015;15(1):848. | ||
Turan JM, Nyblade L. HIV-related stigma as a barrier to achievement of global PMTCT and maternal health goals: a review of the evidence. AIDS Behav. 2013;17(7):2528–2539. | ||
Pulerwitz J, Michaelis A, Weiss E, Brown L, Mahendra V. Reducing HIV-related stigma: lessons learned from Horizons research and programs. Public Health Rep. 2010;125(2):272–281. | ||
Shekelle P, Woolf S, Grimshaw JM, Schünemann HJ, Eccles MP. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci. 2012;7(1):62. | ||
Jackson N, Waters E. The challenges of systematically reviewing public health interventions. J Public Health (Oxf). 2004;26(3):303–307. | ||
Sikkema KJ, Dennis AC, Watt MH, Choi KW, Yemeke TT, Joska JA. Improving mental health among people living with HIV: a review of intervention trials in low-and middle-income countries. Glob Ment Health (Camb). 2015;2:e19. | ||
Montgomery P, Underhill K, Gardner F, Operario D, Mayo-Wilson E. The Oxford Implementation Index: a new tool for incorporating implementation data into systematic reviews and meta-analyses. J Clin Epidemiol. 2013;66(8):874–882. | ||
Armstrong R, Waters E, Jackson N. Systematic Reviews of Health Promotion and Public Health Interventions. Melbourne: University of Melbourne; 2007. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.