")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Reducing drug–herb interaction risk with a computerized reminder system
Authors Lin S, Tsai C, Tu C, Hsieh C
Received 25 November 2014
Accepted for publication 21 December 2014
Published 16 February 2015 Volume 2015:11 Pages 247—253
DOI https://doi.org/10.2147/TCRM.S78124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Sheng-Shing Lin,1,2 Chiu-Lin Tsai,3 Ching-Yeh Tu,3 Ching-Liang Hsieh2,4,5
1Graduate Institute of Chinese Medicine, College of Chinese Medicine, China Medical University, 2Department of Chinese Medicine, China Medical University Hospital, 3Division of Chinese Medicine, Department of Pharmacy, China Medical University Hospital, 4Graduate Institute of Integrated Medicine, College of Chinese Medicine, China Medical University, 5Research Center for Chinese Medicine and Acupuncture, China Medical University, Taichung, Taiwan
Background: Traditional Chinese medicine (TCM) and Western medicine are both popular in Taiwan. Approximately 14.1% of Taiwanese residents use Western drugs and Chinese herbs concurrently; therefore, drug–herb interaction is critical to patient safety. This paper presents a new procedure for reducing the risk of drug interactions.
Methods: Hospital computer systems are modified to ensure that drug–herb interactions are automatically detected when a TCM practitioner is writing a prescription. A pop-up reminder appears, warning of interactions, and the practitioner may adjust doses, delete herbs, or leave the prescription unchanged. A pharmacist will receive interaction information through the system and provide health education to the patient.
Results: During the 2011–2013 study period, 256 patients received 891 herbal prescriptions with potential drug–herb interactions. Three of the 50 patients who concurrently used ginseng and antidiabetic drugs manifested hypoglycemia (fasting blood sugar level ≤70 mg/dL).
Conclusion: Drug–herb interactions can cause adverse reactions. A computerized reminder system can enable TCM practitioners to reduce the risk of drug–herb interactions. In addition, health education for patients is crucial in avoiding adverse reaction by the interactions.
Keywords: Traditional Chinese medicine, Western medicine, adverse reaction
Background
Taiwan’s National Health Insurance program has covered both Western medicine (WM) and traditional Chinese medicine (TCM) since its inauguration in 1995. TCM is popular in Taiwan, and more than 60% of the people used it between 1996 and 2001.1 In 2007, approximately 14.1% of the people in Taiwan used TCM herbal products and conventional WM drug concurrently.2 Therefore, the drug–herb interaction is critical to patient safety. For example, concomitant use of danshen (Salvia miltiorrhiza) and warfarin may exaggerate the anticoagulant effect of warfarin and possibly cause bleeding.3,4 Korean/Asian ginseng (Panax ginseng) and American ginseng (Panax quinquefolius) have antidiabetic effects;5–9 using ginseng concurrently with oral hypoglycemic agents (OHAs) or insulin injections may increase the risk of hypoglycemia.10 Concomitant use of red yeast rice with cyclosporine may induce rhabdomyolysis.11
In most countries, people obtain herbal products outside of hospitals; therefore, physicians may not determine what herbs patients have consumed. Furthermore, people who sell herbal products may have insufficient knowledge about modern drugs and drug–herb interactions. In Taiwan, TCM practitioners are certified through a national board examination and have some knowledge of modern drugs.
In China Medical University Hospital, Taichung, Taiwan, the TCM department’s medical records are stored in the same database as those of the WM department. When writing a prescription, TCM practitioners and WM doctors may view previous drug and herbal prescriptions directly through the computer system. However, drug–herb interactions may not be identified because practitioners and doctors are too busy to assess previous prescriptions by another doctor, or because they lack the time to consider possible interactions.
In 2011, we modified the herb prescription process in our hospital’s TCM department. A computerized reminder system was programmed to search for drug interactions and automatically display possible interactions in a pop-up window. TCM practitioners may consider the interactions and then adjust doses or delete herbs.
Methods
Literature review
Journals from PubMed
We performed the following keyword searches in PubMed:12
- General concept: “drug herb interaction”; “herb interaction”; “traditional Chinese medicine” OR “Chinese medication” OR “herbal medicine” AND “interaction”.
- Specifying individual herb names without drug names: for example, “Panax ginseng” AND “interaction”; “American ginseng” AND “interaction”; “Danshen” AND “interaction”; “Dong Quai” AND “interaction”; and “Ma Huang” AND “interaction”.
- Specifying herb names and drug names: for example, “Panax ginseng” AND “digoxin”; “Panax ginseng” AND “warfarin”; “Panax ginseng” AND “hypoglycemic agent”; and “Danshen” AND “warfarin”.
The searches were performed in 2010 and were restricted to English-language results from 1986 to 2010. Articles were selected according to title and abstract by using the following criteria: 1) at least one herb and at least one drug were mentioned, and the interaction between the herb and drug was described; and 2) only articles about herbs that are available in Taiwan were included.
Studies in Taiwan
On Taiwan’s Government Research Bulletin (GRB) website,13 searches in Chinese language for the keyword “drug-herb interaction”, as well as individual herb names plus the keyword “drug interaction” were performed. Studies related to a single herb or to herbal combinations that were discussed with drug interactions were included; studies related to herbs unavailable at our hospital were excluded.
Theses and dissertations in Taiwan
On the Taiwan National Digital Library of Theses and Dissertations website,14 searches in traditional Chinese for the keywords “drug-herb interaction”, as well as individual herb names plus the keyword “drug interaction” were performed. Theses and dissertations related to a single herb or herbal combinations that were discussed with drug interactions were included; theses and dissertations related to herbs unavailable at our hospital were excluded.
Creating a drug–herb interaction database
We collected drug–herb interaction data from PubMed, study reports, theses, and dissertations. A database was created with columns for drug name, herb name, interaction, mechanism, symptoms, management, suggestion, severity, documentation, case number, article title, and journal title.
Severity definitions and documentation
We used the definitions in Drug Interaction Facts 2014: the Authority on Drug Interactions to identify the severity of drug–herb interactions.15
Drug–herb interaction severity categories
Major drug–herb interactions are effects that are potentially life-threatening or capable of causing permanent damage. Moderate drug–herb interactions are effects that may cause deterioration in a patient’s clinical status. Further treatment, hospitalization, or an extended hospital stay may be necessary. Minor drug–herb interactions are effects that are mild; consequences may be regarded as bothersome or may be unnoticeable and do not notably affect the therapeutic outcome. Further treatment is usually not required.
Documentation
Established drug–herb interactions are those that are proven to occur in well-controlled studies. Probable drug–herb interactions are those that are likely but not proven clinically. Suspected drug–herb interactions are those that may occur, with some good data but requiring more study. Possible drug–herb interactions are those that could occur, but data are limited. Unlikely drug–herb interactions are those that are doubtful, with no strong evidence of an altered clinical effect.
Committee conference
The Safety of Herb Usage Committee comprised three physicians (WM doctors), three TCM practitioners, four pharmacists, one nurse, and one computer programmer. The severity and documentation of drug–herb interactions were discussed at regularly held conferences. Commonly used herbs and drugs with highly significant interactions were included in the reminder system.
Programmer adds function in the hospital information system
A computer program was written to deliver warnings of potential drug interactions. The interaction data selected by the committee was entered into the hospital’s computer system. When a TCM practitioner processes a herbal prescription, the reminder program automatically searches for related drug interactions. When there is a highly substantial significant interaction, a pop-up window appears to inform the TCM practitioner, who may then adjust doses or remove problematic herbs. If the practitioner does not remove the herb/herbs related to drug interaction, the computer system will inform the pharmacist, who will explain the possible symptoms of the drug interaction to the patient. The computer system stores basic patient, drug, and herb data in a track list.
Retrospectively analyzing patient medical records
Using the track list of potential interactions, we selectively analyzed specific drugs and herbs by using retrospective medical record searches. We discussed possible drug–herb interactions with the committee to ascertain the significance and severity.
Results
We retrieved 99 journals from PubMed and identified 648 drug–herb combinations. From Taiwan’s Government Research Bulletin website, we retrieved 44 study reports containing 76 drug–herb combinations. In addition, 46 drug–herb combinations were identified from 23 theses in Taiwan. In total, 770 drug–herb combinations and interactions were input into the database (Figure 1).
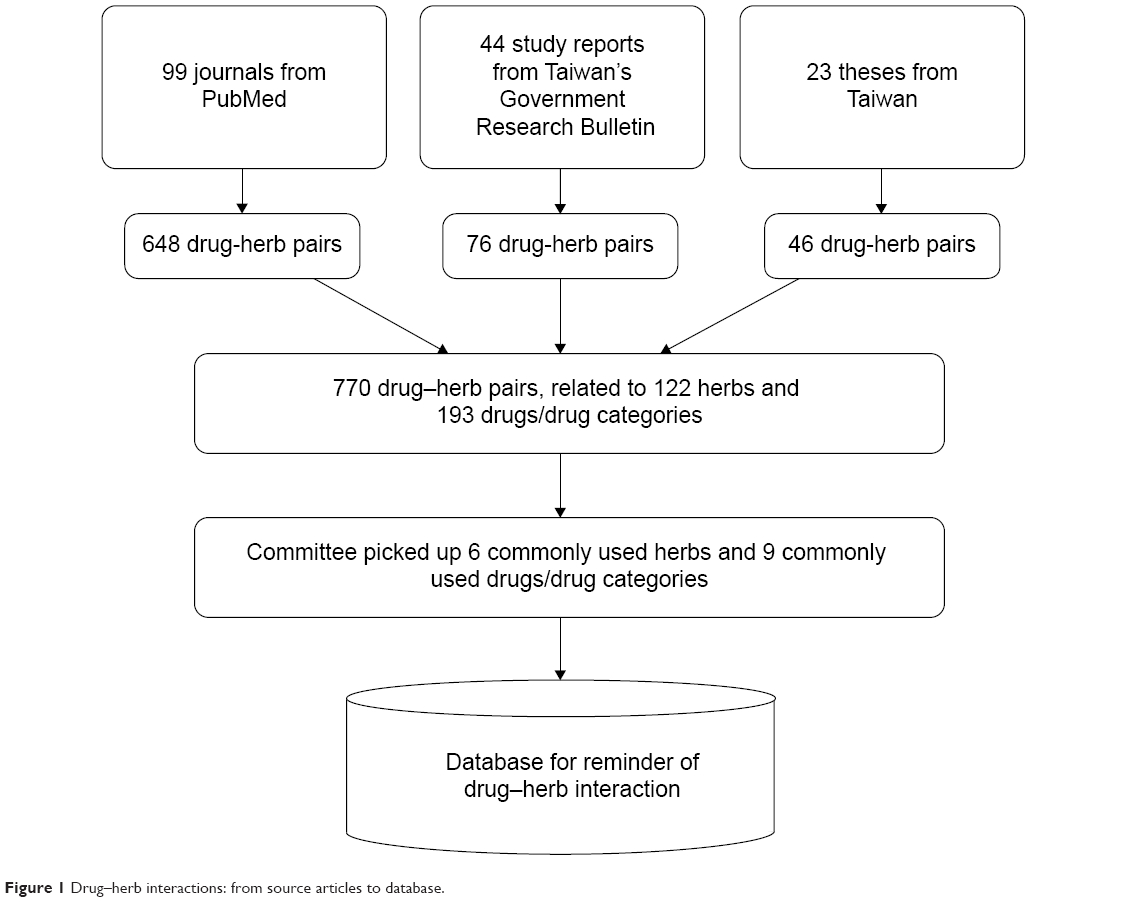 | Figure 1 Drug–herb interactions: from source articles to database. |
There were 122 herbs and 193 drugs or drug categories related in the 770 drug–herb pairs. After severity and documentation categorization, our committee selected commonly prescribed medicines, namely six herbs (American ginseng, danshen, dong quai, ma huang, Korean/Asian ginseng, and red yeast rice) and nine drug categories (insulin, OHAs, anticoagulants, antiplatelets, xanthines, QT prolongation drugs, central nervous system stimulants, HMG-CoA reductase inhibitors, and cyclosporines) for use in the reminder system (Table 1).
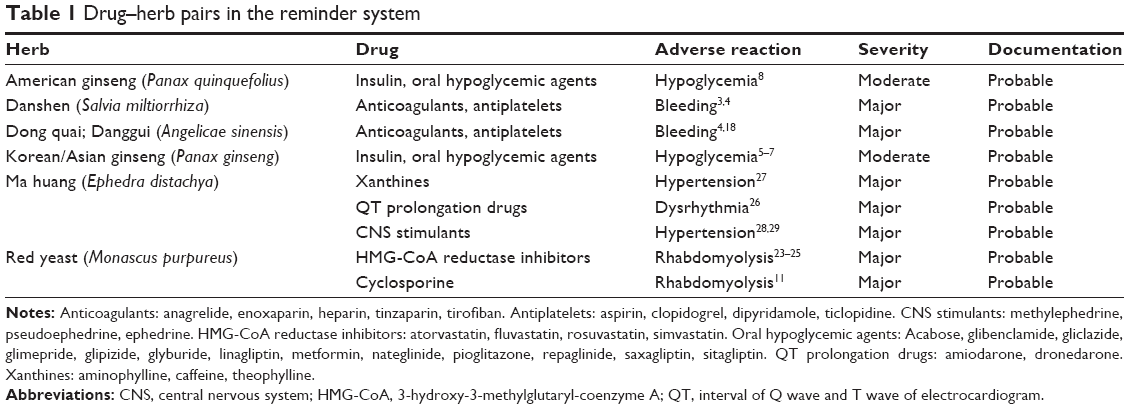 | Table 1 Drug–herb pairs in the reminder system |
A guide was created for pharmacists to educate patients about possible interactions when filling prescriptions (Table 2). TCM practitioners may also tell patients to monitor for drug-interaction symptoms, and the warnings and advice from pharmacists further emphasizes the need for vigilance against interactions.
 | Table 2 Pharmacist guide of health education on adverse reaction of drug–herb interactions |
The reminder system was inaugurated on January 1, 2011 (Figure 2), and from that day to December 31, 2013, it identified 891 herbal prescriptions (for 256 patients) with possible drug interactions to which no adjustments were made by the TCM practitioner. The system recorded 227 prescriptions (for 50 patients) in which the interaction of ginseng (Korean/Asian ginseng or American ginseng) and hypoglycemic agents was possible. We retrospectively reviewed medical records in a pilot study and determined that three of the 50 patients manifested hypoglycemia (fasting blood sugar level ≤70 mg/dL) during concurrent use of ginseng and a hypoglycemic agent. Only one of those three patients displayed symptoms of hypoglycemia. More time is required to evaluate the clinical course of other drug–herb combinations, and further analysis is required to gain a deeper understanding of drug–herb interactions.
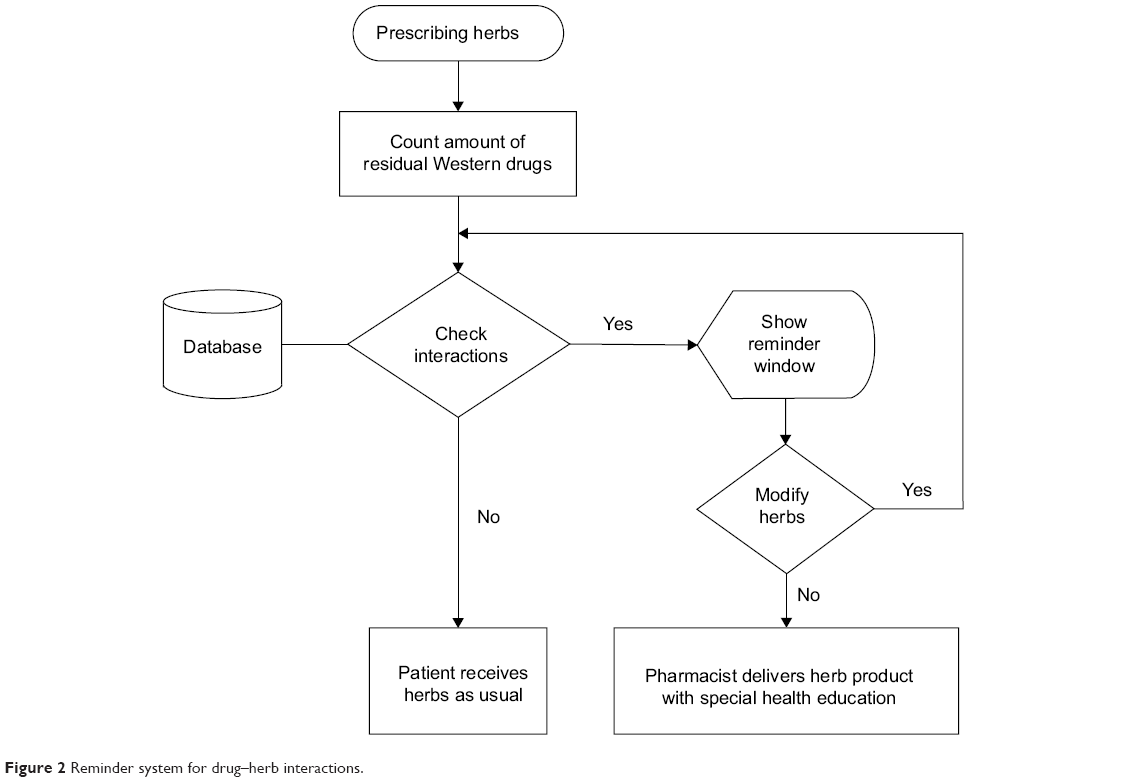 | Figure 2 Reminder system for drug–herb interactions. |
The interaction of danshen or dong quai with anticoagulants, such as warfarin, or with antiplatelets, such as aspirin or Plavix, as well as the interaction of red yeast rice with statins can be life-threatening. The interaction of American ginseng or P. ginseng with an OHA or insulin injection can cause clinical deterioration and require hospitalization.
Discussion
We effectively designed and implemented a computerized drug–herb reminder system that identified 891 herbal prescriptions posing possible major or moderate interactions with WM drugs in our hospital from January 1, 2011 to July 31, 2013.15 Pharmacists were prompted by the system to warn patients of possible interactions and interaction symptoms, and followed-up with the patients. Three patients were discovered to have hypoglycemia (fasting blood sugar level ≤70 mg/dL), but no other adverse clinical reactions were reported by other patients. The system is simple, rapid, and convenient to use, providing immediate drug–herb interaction information upon prescription input.
The most frequent drug–herb interaction reminders were for ginseng plus OHA or insulin injections; danshen or dong quai plus warfarin, aspirin, or clopidogrel; and red yeast rice plus statin. Ginseng may increase insulin sensitivity, reduce insulin resistance, and increase insulin secretion, yielding hypoglycemic effects.5,16 In addition, ginsenoside, a component of ginseng, increases glucagon-like peptide-1 secretion, thereby reducing blood glucose levels.5 In Taiwan, Liu Wei Di Huang Wan is the most frequently prescribed formula by TCM doctors for diabetes patients.17 The interactions between Liu Wei Di Huang Wan and antidiabetic WM drugs need more study for further evaluation. Ginseng is often prescribed for other purpose such as improving energy rather than reducing blood sugar. Dong quai contains coumarin derivatives, which can potentiate warfarin, elevating prothrombin time and the international normalized ratio.18 Danshen increased the absorption of warfarin in rats and reduced the protein binding of warfarin in serum.19 Moreover, danshen increased the international normalized ratio from 3.0 to more than 8.4 and was reported to cause the activated partial thromboplastin time to increase to more than 120 seconds in a cardiac valve operation patient.20 Consuming 10 mg of monacolins from red yeast rice (Monascus purpureus) for 4 weeks reduced the total cholesterol and low-density lipoprotein (LDL) cholesterol levels substantially in hypercholesterolemia patients.21 In addition, red yeast rice was demonstrated to reduce the effects of LDL cholesterol in statin-intolerant hyperlipidemia patients with or without type 2 diabetes.22 Therefore, red yeast rice, like statins, can reduce the effects of LDL cholesterol. The combination use of statin with red yeast rice may increase the risk of rhabdomyolysis.23–25 There are also other TCM herbs with hypolipidemic effect, such as Zexie (Alismatis rhizoma), Huang lian (Coptidis rhizoma), and hawthorn (Crataegi fructus).24 The interactions between hypolipidemic drugs with those herbs require further study to confirm clinical influence.
Ephedra may have an additive effect with drugs that prolong the QT interval, eg, amiodarone, dronedarone, and quinidine. This may increase the risk of ventricular arrhythmias.26 Use of ephedra with caffeine or other methylxanthines such as theophylline might increase the risk of stimulatory adverse effects.27 Drugs with central nervous system stimulant properties, such as phenylpropanolamine, pseudoephedrine, and diethylpropion, might increase the risk of hypertension and adverse cardiovascular effects of ephedra.28,29
Some items have not yet been included in the reminder system, eg, licorice, ginger, and ginkgo. Licorice may induce pseudoaldosteronism with hypokalemia, and increase the toxicity of digoxin.30 Concurrent use of ginger with warfarin may increase the risk of bleeding.31,32 Ginkgo and ginger at recommended doses do not significantly affect clotting status, or the pharmacokinetics or pharmacodynamics of warfarin in healthy subjects.33 The use of licorice and ginger is very common in TCM prescriptions and the dose is often small. The severity of interaction is related to the dose but the reminder system checks only the herb name without the dosage. We selected highly significant interactions initially to avoid too many annoying pop-up windows. In the future, more items such as licorice and ginger will be included after the discussion in committee.
Ginkgo biloba is made to be a drug and is prescribed by WM doctors in Taiwan. There may be possible interactions with monoamine oxidase inhibitors, alprazolam, haloperidol, warfarin, and nifedipine.34 Ginkgo biloba is not an item for TCM use, hence our TCM reminder system does not include it. However, ginkgo biloba is included in another reminder system of drug–drug interaction for WM doctors in our hospital.
This study’s limitations were as follows:
- The reminder system was used only in our hospital, and drug–herb interactions could not be observed if patients visited other hospital or clinics; therefore, the system will be expanded to all hospitals and local clinics in Taiwan.
- The system issued warnings for all possible drug–herb interactions from among those in the database, and indicated whether the interaction was minor, moderate, or major. This resulted in excess information on the computer screen, interfering with the work of the TCM practitioners. This limitation raises the critical concern of deciding which possible interactions should be included in the system.
- Drug–herb interactions are largely dependent on the doses and formulas involved, and although animal studies of interactions investigated exact doses, the effects of different doses in humans is unclear.
Despite these limitations, the computerized reminder system improves drug and patient safety because it alerts TCM practitioners to interactions and enables them to change herbs or formulas, modify doses, or take no action when writing prescriptions.
Drug safety will improve if TCM practitioners pay more attention to the system’s warnings. However, too many pop-up windows may disturb the thinking process of the doctors; we should achieve a balance between safety and convenience. Our committee selected commonly used herbs and drugs for inclusion in the reminder system. TCM practitioners will be familiar with the prescription process, and pharmacists will be acquainted with providing supplemental health education. We will add more interactions into the reminder system after regularly held conferences.
Conclusion
The computerized reminder system automatically informs TCM practitioners who are writing prescriptions of potential drug–herb interactions. TCM practitioners may choose to adjust herbs or doses to avoid or reduce the risk of drug–herb interactions. Pharmacists may then use information provided by the system to educate patients about possible drug–herb interactions and resulting symptoms. This combination of reminders and education can improve patient safety.
Acknowledgments
This study was supported by China Medical University under the Aim for Top University Plan of the Ministry of Education, Taiwan, and by the Taiwan Ministry of Health and Welfare’s Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002). The authors thank computer programmer Zi-Rong Yen, who designed the reminder system.
Disclosure
The authors report no conflicts of interest in this work.
References
Chen FP, Chen TJ, Kung YY, et al. Use frequency of traditional Chinese medicine in Taiwan. BMC Health Serv Res.2007;7:26. | ||
Chen MC, Lai JN, Chen PC, Wang JD. Concurrent Use of Conventional Drugs with Chinese Herbal Products in Taiwan: A Population-based Study. J Tradit Complement Med.2013;3(4):256–262. | ||
Chan TY. Interaction between warfarin and danshen (Salvia miltiorrhiza). Ann Pharmacother.2001;35(4):501–504. | ||
Tsai HH, Lin HW, Lu YH, Chen YL, Mahady GB. A review of potential harmful interactions between anticoagulant/antiplatelet agents and Chinese herbal medicines. PloS One.2013;8(5):e64255. | ||
Liu Z, Li W, Li X, et al. Antidiabetic effects of malonyl ginsenosides from Panax ginseng on type 2 diabetic rats induced by high-fat diet and streptozotocin. J Ethnopharmacol.2013;145(1):233–240. | ||
Jeon WJ, Oh JS, Park MS, Ji GE. Anti-hyperglycemic effect of fermented ginseng in type 2 diabetes mellitus mouse model. Phytother Res.2013;27(2):166–172. | ||
Xie JT, Mchendale S, Yuan CS. Ginseng and diabetes. Am J Chin Med.2005;33(3):397–404. | ||
Sen S, Querques MA, Chakrabarti S. North American Ginseng (Panax quinquefolius) prevents hyperglycemia and associated pancreatic abnormalities in diabetes. J Med Food.2013;16(7):587–592. | ||
Kim DH. Chemical Diversity of Panax ginseng, Panax quinquifolium, and Panax notoginseng. J Ginseng Res.2012;36(1):1–15. | ||
Brazier NC, Levine MA. Drug-herb interaction among commonly used conventional medicines: a compendium for health care professionals. Am J Ther.2003;10(3):163–169. | ||
Prasad GV, Wong T, Meliton G, Bhaloo S. Rhabdomyolysis due to red yeast rice (Monascus purpureus) in a renal transplant recipient. Transplantation.2002;74(8):1200–1201. | ||
PubMed.gov [database on the Internet]. Bethesda, MD: National Center for Biotechnology Information, US Library of Medicine. Available from: http://www.ncbi.nlm.nih.gov/pubmed/ Accessed July 1, 2010. | ||
GRB [database on the Internet]. Taipei, Taiwan: Government Research Bulletin. [Updated 2014 Dec 18; cited 2015 Jan 20]. Available from: http://grbsearch.stpi.narl.org.tw/GRB_Search/grb/. Accessed July 1, 2010. | ||
National Digital Library [database on the Internet]. Taipei, Taiwan: National Digital Library of Theses and Dissertations. [Updated 2015 Jan 16; cited 2015 Jan 20]. Available from: http://ndltd.ncl.edu.tw/cgi-bin/gs32/gsweb.cgi. Accessed July 1, 2010. | ||
Tatro DS. Drug Interaction Facts 2014: the Authority on Drug Interactions. St Louis: Lippincott Williams & Wilkins; 2013. | ||
Kim HY, Kim K. Regulation of signaling molecules associated with insulin action, insulin secretion and pancreatic β-cell mass in the hypoglycemic effects of Korean red ginseng in Goto-Kakizaki rats. J Ethnopharmacol.2012;142(1):53–58. | ||
Huang CY, Tsai YT, Lai JN, Hsu FL. Prescription pattern of chinese herbal products for diabetes mellitus in taiwan: a population-based study. Evid Based Complement Alternat Med.2013;2013:201329. | ||
Page RL 2nd, Lawrence JD. Potentiation of warfarin by dong quai. Pharmacotherapy.1999;19(7):870–876. | ||
Zhang Z, Ge B, Zhou L, Lam TN, Zuo Z. Induction of liver cytochrome P450s by Danshen-Gegen formula is the leading cause for its pharmacokinetic interactions with warfarin. J Ethnopharmacol.2014;154(3):672–686. | ||
Izzat MB, Yim AP, El-Zufari MH. A taste of Chinese medicine! Ann Thorac Surg.1998;66(3):941–942. | ||
Cicero AF, Derosa G, Parini A, et al. Red yeast rice improves lipid pattern, high-sensitivity C-reactive protein, and vascular remodeling parameters in moderately hypercholesterolemic Italian subjects. Nutr Res.2013;33(8):622–628. | ||
Sartore G, Burlina S, Ragazzi E, Ferraresso S, Valentini R, Lapolla A. Mediterranean Diet and Red Yeast Rice Supplementation for the Management of Hyperlipidemia in Statin-Intolerant Patients with or without Type 2 Diabetes. Evid Based Complement Alternat Med.2013;2013:743473. | ||
Harper CR, Jacobson TA. The broad spectrum of statin myopathy: from myalgia to rhabdomyolysis. Curr Opin Lipidol.2007;18(4):401–408. | ||
Sham TT, Chan CO, Wang YH, Yang JM, Mok DK, Chan SW. A review on the traditional Chinese medicinal herbs and formulae with hypolipidemic effect. Biomed Res Int.2014;2014:925302. | ||
Mueller PS. Symptomatic myopathy due to red yeast rice. Ann Intern Med.2006;145(6):474–475. | ||
McBride BF, Karapanos AK, Krudysz A, Kluger J, Coleman CI, White CM. Electrocardiographic and hemodynamic effects of a multicomponent dietary supplement containing ephedra and caffeine: a randomized controlled trial. JAMA.2004;291(2):216–221. | ||
Weinberger M, Bronsky E, Bensch GW, Bock GN, Yecies JJ. Interaction of ephedrine and theophylline. Clin Pharmacol Ther.1975;17(5):585–592. | ||
White LM, Gardner SF, Gurley BJ, Marx MA, Wang PL, Estes M. Pharmacokinetics and cardiovascular effects of ma-huang (Ephedra sinica) in normotensive adults. J Clin Pharmacol.1997;37(2):116–122. | ||
Haller CA, Benowitz NL. Adverse cardiovascular and central nervous system events associated with dietary supplements containing ephedra alkaloids. N Engl J Med.2000;343(25):1833–1838. | ||
Harada T, Ohtaki E, Misu K, Sumiyoshi T, Hosoda S. Congestive heart failure caused by digitalis toxicity in an elderly man taking a licorice-containing chinese herbal laxative. Cardiology.2002;98(4):218. | ||
Lesho EP, Saullo L, Udvari-Nagy S. A 76-year-old woman with erratic anticoagulation. Cleve Clin J Med.2004;71(8):651–656. | ||
Shalansky S, Lynd L, Richardson K, Ingaszewski A, Kerr C. Risk of warfarin-related bleeding events and supratherapeutic international normalized ratios associated with complementary and alternative medicine: a longitudinal analysis. Pharmacotherapy.2007;27(9):1237–1247. | ||
Jiang X, Williams KM, Liauw WS, et al. Effect of ginkgo and ginger on the pharmacokinetics and pharmacodynamics of warfarin in healthy subjects. Br J Clin Pharmacol.2005;59(4):425–432. | ||
Diamond BJ, Bailey MR. Ginkgo biloba: indications, mechanisms, and safety. Psychiatr Clin North Am.2013;36(1):73–83. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.