")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 12
Reduced Prescription of Baloxavir After Suspected Prevalence of a Baloxavir-Resistant Influenza Virus Strain and the Emergence of SARS-CoV-2 in a Tertiary Hospital in Japan
Authors Kamioka Y, Kashiwagura S, Seki M
Received 24 June 2020
Accepted for publication 29 July 2020
Published 21 August 2020 Volume 2020:12 Pages 131—134
DOI https://doi.org/10.2147/CPAA.S268666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Yasuhiro Kamioka,1,2 Shota Kashiwagura,1,2 Masafumi Seki1
1Department of Infectious Diseases, Faculty of Medicine, Tohoku Medical and Pharmaceutical University, Sendai City, Miyagi, Japan; 2Division of Pharmacy, Tohoku Medical and Pharmaceutical University Hospital, Sendai City, Miyagi, Japan
Correspondence: Masafumi Seki
Department of Infectious Diseases, Faculty of Medicine, Tohoku Medical and Pharmaceutical University, 1-15-1 Fukumuro, Miyagino-Ku, Sendai City, Miyagi 983-8612, Japan
Tel +81-22-259-1221
Fax +81-22-290-8956
Email [email protected]
Objective: The use of baloxavir, a new anti-influenza agent, began in Japan from the 2018 to 2019 season and became the focus of attention due to its efficient viral reduction ability; therefore, we should know the prescription changes of anti-influenza agents.
Methods: We analyzed the changes in the prescription of anti-influenza agents between the 2018– 19 season and the 2019– 20 season in our hospital.
Results: The share of baloxavir was 15%, while the shares of oseltamivir and laninamivir were 42% and 31%, respectively in the 2018– 2019 season. However, in the 2019– 20 season, the share of baloxavir and laninamivir was reduced to 3% and 17%, respectively, in contrast to an increase in the share of oseltamivir (66%). The total prescription of anti-influenza agents for patients decreased in the 2019– 20 season (205 patients), compared with the 2018– 19 season (509 patients).
Conclusion: These results suggest significant changes such as a reduction in the prescription of anti-influenza agents, especially baloxavir, likely due to the suspected prevalence of a baloxavir-resistant strain of influenza virus and the emergence of SARS-CoV-2 in Japan.
Keywords: anti-influenza agents, oseltamivir, laninamivir, zanamivir, peramivir, novel coronavirus-2019, COVID-19
Introduction
Influenza virus infection is a major respiratory infectious disease that generally induces bronchitis, pneumonia,1 and acute febrile illness with malaise that can be fatal with complicating pneumonia, especially in elderly people.2–4
The neuraminidase inhibitors (NAIs) oseltamivir, zanamivir, peramivir and laninamivir are approved for therapeutic and prophylactic treatments of influenza virus infection in Japan.5 The novel cap-dependent endonuclease inhibitor (CEI) baloxavir marboxil (baloxavir; S-033188) was approved in 2018 to treat influenza and has recently become the predominant anti-influenza agent in Japan because it only requires a single oral dose.6,7
However, recent studies have associated an I38T substitution in the polymerase acidic subunit (PA) with reduced susceptibility of influenza viruses to baloxavir, and a Phase III clinical trial detected PA I38T and I38M substitutions after exposure to baloxavir in 9.7% of 370 A (H3N2) viruses related with the prolonged median amount of elapsed time to symptom alleviation although these baloxavir-resistant strain were proven to keep the susceptibility to NAIs.7–10 Therefore, we recently described the possibility of substituting and/or combining CEIs and NAIs when they have little to no effect against influenza infections, especially during the H3N2 season.11
In addition, novel SARS-CoV-2 infection spread from Wuhan, China, and a Public Health Emergency of International Concern (PHEIC) was declared by the World Health Organization (WHO) globally.
In this study, we compared the prescription of anti-influenza agents between the 2018–19 season and the 2019–20 season, and explored the effects of the emergence of COVID-19 and a suspected baloxavir-resistant strain of influenza virus.
Methods
We used data from the prescription database maintained by the department of pharmacy in Tohoku Medical and Pharmaceutical University Hospital (600 beds).
The patients were diagnosed as influenza by rapid antigen tests (rapid influenza diagnosed kit: RIDTs), and/or clinically signs, such as temperature >38.0°C with cough or sore throat with an onset of symptoms within 7 days after close contact with influenza patients. More than 90% patients were diagnosed as influenza by both RIDTs and clinical symptoms and the other were diagnosed by clinically. Both inpatient and outpatient were registered, and the anti-influenza agents were prescribed and used. The rates of inpatient and outpatient were 14% and 86%, respectively.
This study was complied with declaration of Helsinki and approved by the Committee for Clinical Scientific Research of Tohoku Medical and Pharmaceutical University Hospital in Feb, 2020 as No. ID2019-2-028. Written informed consent was provided by the patients to use their data in this study.
Results
In the 2018–19 season, in which both A/H1N1pdm09 and H3N2 influenza virus infections were prevalent, a total of 509 patients received anti-influenza agents. In contrast, Only 205 patients received anti-influenza agents in the 2019–20 season, in which A/H1N1pdm09 infections were most prevalent. However, novel corona virus infection 2019 (COVID-19) has become a much larger cause for concern than influenza in 2019–20 season. Five anti-influenza agents, oseltamivir, laninamivir, baloxavir, zanamivir, and peramivir, were prescribed in both the 2018–19 season and the 2019–20 season although the total prescription of the anti-influenza agents decreased in the 2019–20 season (Figure 1).
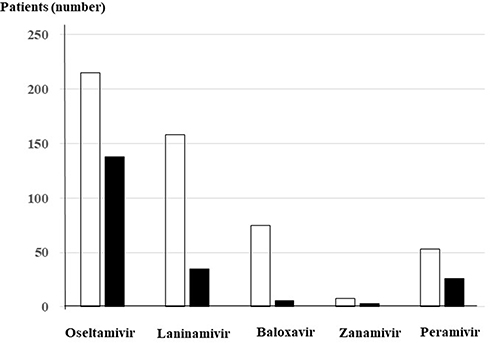 |
Figure 1 Total prescription of anti-influenza agents in Tohoku Medical and Pharmaceutical University Hospital in the 2018–19 season (white bars) and the 2019–20 season (black bars), respectively. |
Figure 2 shows the share and ratio of each anti-influenza agent in the 2018–19 season (Figure 2A) and the 2019–20 season (Figure 2B). Among the five anti-influenza agents, the ratio and share of baloxavir and laninamivir significantly decreased from 15% to 3% and from 31% to 17%, respectively. In contrast, oseltamivir increased from 42% to 66%. Zanamivir remained constant, while peramivir showed a slight increase.
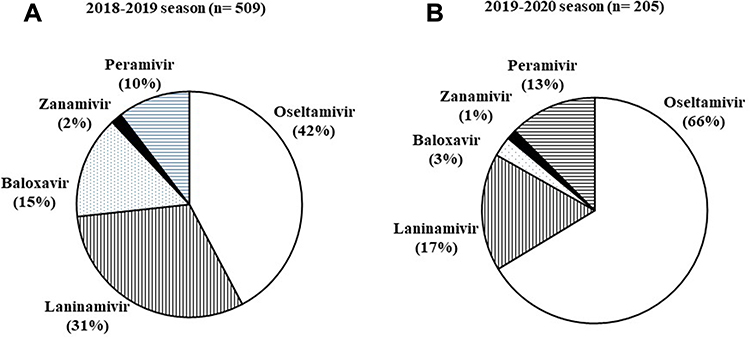 |
Figure 2 The ratio and shares of prescribed anti-influenza agents in the 2018–19 season (A) and the 2019–20 season (B), respectively. White area: oseltamivir, vertical line area: laninamivir, dot area: baloxavir, black area: zanamivir, and horizontal line area: peramivir, respectively. |
Discussion
In Japan, many NAIs have been available and recently the use of a new CEI, baloxavir marboxil, began. Baloxavir is reported to be equally clinically effective, have a better viral reduction ability and only require a single oral dose to be effective when compared with oseltamivir, which must be administered twice per day for five days to be effective.7
In this study, we observed a large ratio of baloxavir prescription among the anti-influenza agents in our hospital with a relatively high share of 15% even though the 2018–19 season was the novel year of prescription. However, the clinical efficiency of baloxavir is reduced in patients with an I38 substitution of PA regions, which is consistent with drug susceptibility, and these substitutions have been found in 1.5% and 9.5% of influenza virus types H1N1 and H3N2, respectively, suggesting that the low efficiency of baloxavir, especially against H3N2 in its seasonal peak, should be considered after the 2018–19 season.6,8-10
Furthermore, viruses with I38 substitutions suggest human-to-human transmission because these viruses were isolated from patients who had not been treated with baloxavir but had siblings who were.6 NAI-resistant viruses, for instance, NA H275Y mutation confers resistance to oseltamivir and peramivir although laninamivir might be still relatively susceptible, and it is also well confirmed human-to human transmission of NAI-resistant viruses.12,13 These data suggest that appropriate treatment to avoid selecting mutant viruses should be performed, since treatment for the whole household is impractical. Therefore, careful use of baloxavir might become the trend among Japanese clinicians in the 2019–20 season. As an effect, we found a significant reduction in the prescription of baloxavir from a 15% to 3% share among anti-influenza agents in our hospital. We did not find actual large number of baloxavir–resistant strain in 2019–2020 because H1N1 strain, which considered low-resistant for baloxavir, was dominant in this season, however, the informative support and education for the appropriate use of antimicrobial agents by the infectious diseases physicians and pharmacists, such as one of the antimicrobial stewardship program may result the improvement of the anti-influenza agents use, especially for use of baloxavir.14,15
In addition, the total prescription of the anti-influenza agents significantly decreased in our hospital in the 2019–20 season, compared to the 2018–19 season. This might be an effect of the COVID-19 pandemic.16 The general population has been very cautious about the transmission and infection of the virus in Japan, with masks and proper hygiene procedures being strongly recommended. Therefore, influenza virus transmission and infection may also reduce, and the total use of anti-influenza drugs, including laninamivir were reduced although prevalence of laninamivir-resistant strain have not been reported and shown continuously clinical effects in contrast to baloxavir.17 The share of osertamivir alone increased clearly because it was considered as the most standard anti-influenza agent globally,18 but the total amount of osertamivir use also reduced in 2019–2020 seasons, compared with 2018–2019 seasons. Further studies and clinical observation of anti-influenza agents and emergence of resistant strains and novel viruses are needed.
In summary, we analyzed the prescription of anti-influenza agents and compared their shares in the 2018–19 season and the 2019–20 season. We found a significant decrease in the total prescription of anti-influenza agents, especially of the new CEI baloxavir, in our hospital in Japan. The suspected prevalence of the baloxavir-resistant influenza strain and emergence of SARS-CoV-2 might have affected the use of anti-influenza agents in the 2019–20 season. This could be in line with the antiviral stewardship and infection control philosophy; however, more comprehensive and nationwide data analysis will be needed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mandell LA, Wunderink RG, Anzueto A; Infectious Diseases Society of America, American Thoracic Society, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44:S27–S72.
2. Glezen WP, Greenberg S, Atmar RL, Piedra PA, Couch RB. Impact of respiratory virus infections on persons with chronic underlying conditions. JAMA. 2000;283:499–505. doi:10.1001/jama.283.4.499
3. Seki M, Kosai K, Yanagihara K, et al. Disease severity in patients with simultaneous influenza and bacterial pneumonia. Intern Med. 2007;46(13):953–958. doi:10.2169/internalmedicine.46.6364
4. Esposito S, Molteni CG, Daleno C, et al. Impact of pandemic A/H1N1/2009 influenza on children and their families: comparison with seasonal A/H1N1 and A/H3N2 influenza viruses. J Infect. 2011;63(4):300–307. doi:10.1016/j.jinf.2011.07.015
5. Oikawa N, Seki M. Clinical differences in hospitalized adult influenza patients between the A (H1N1) pdm09 and the A (H3N2) seasons in Japan. J Infect Dis Ther. 2018;6:1–6. doi:10.4172/2332-0877.1000353
6. Takashita E, Ichikawa M, Morita H, et al. Human-to-human transmission of influenza A(H3N2) virus with reduced susceptibility to baloxavir, Japan, February 2019. Emerg Infect Dis. 2019;17:25.
7. Baloxavir Marboxil Investigators Group, Hayden FG, Sugaya N, Hirotsu N, et al. Baloxavir marboxil for uncomplicated influenza in adults and adolescents. N Engl J Med. 2018;379(10):913–923. doi:10.1056/NEJMoa1716197.
8. Takashita E, Morita H, Ogawa R, et al. Susceptibility of influenza viruses to the novel cap-dependent endonuclease inhibitor baloxavir marboxil. Front Microbiol. 2018;9:3026. doi:10.3389/fmicb.2018.03026
9. Takashita E, Kawakami C, Morita H, et al. On behalf of the influenza virus surveillance group of Japan. Detection of influenza A(H3N2) viruses exhibiting reduced susceptibility to the novel cap-dependent endonuclease inhibitor baloxavir in Japan, December 2018. Euro Surveill. 2019;24(3). doi:10.2807/1560-7917.ES.2019.24.3.1800698.
10. Takashita E, Kawakami C, Ogawa R, et al. Influenza A(H3N2) virus exhibiting reduced susceptibility to baloxavir due to a polymerase acidic subunit I38T substitution detected from a hospitalised child without prior baloxavir treatment, Japan, January 2019. Euro Surveill. 2019;24:12. doi:10.2807/1560-7917.ES.2019.24.12.1900170
11. Seki M, Sakai-Tagawa Y, Yasuhara A, Watanabe Y. Adult influenza A (H3N2) with reduced susceptibility to baloxavir or peramivir cured after switching anti-influenza agents. IDCases. 2019;18:e00650. doi:10.1016/j.idcr.2019.e00650
12. Lee N, Hurt AC. euraminidase inhibitor resistance in influenza: a clinical perspective. Curr Opin Infect Dis. 2018;31:520–526. doi:10.1097/QCO.0000000000000498
13. Sugaya N, Ohashi Y. Long-acting neuraminidase inhibitor laninamivir octanoate (CS-8958 versus oseltamivir as treatment for children with influenza virus infection. Antimicrob Agents Chemother. 2010;54:2575–2582. doi:10.1128/AAC.01755-09
14. Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the infectious diseases society of America and the society for healthcare epidemiology of America. Clin Infect Dis. 2016;62:e51–77. doi:10.1093/cid/ciw118
15. Dellit TH, Owens RC, McGowan JE
16. Huang C, Huang C, Wang Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
17. Ikematsu H, Kawai N, Iwaki N, et al. Duration of fever and other symptoms after the inhalation of laninamivir octanoate hydrate in the 2016/17 Japanese influenza season; comparison with the 2011/12 to 2015/16 seasons. J Infect Chemother. 2018;24:718–724. doi:10.1016/j.jiac.2018.04.013
18. Uyeki TM, Bernstein HH, Bradley JS, et al. Clinical practice guidelines by the infectious diseases society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenzaa. Clinical Infect Dis. 2019;68:895–902. doi:10.1093/cid/ciy874
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.