")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Recurrent respiratory papillomatosis: current and future perspectives
Authors Carifi M, Napolitano D, Morandi M, Dall'Olio D
Received 29 January 2015
Accepted for publication 5 March 2015
Published 5 May 2015 Volume 2015:11 Pages 731—738
DOI https://doi.org/10.2147/TCRM.S81825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Marco Carifi,1 Domenico Napolitano,1 Morando Morandi,1 Danilo Dall’Olio2
1Department of Otolaryngology, Azienda Ospedaliera di Rilievo Nazionale A Cardarelli, Naples, 2Department of Otolaryngology, Ospedale Maggiore CA Pizzardi, Bologna, Italy
Abstract: Although recurrent respiratory papillomatosis is a benign disease of the upper aerodigestive tract caused by infection with human papillomavirus, the disease process is unpredictable, ranging from mild disease and spontaneous remission to an aggressive disease with pulmonary spread and requirement for frequent surgical debulking procedures. It can present a protracted clinical course and cause potentially life-threatening compromise of the airways. Over recent decades, a number of alternative medical therapies to standard surgical treatment have been investigated, with modest outcomes overall. Currently, some additional therapies are being explored, together with novel surgical instrumentation that can help to avoid inevitable long-term stenotic complications, ultimately affecting quality of life. Hopefully, clinicians might soon be able to significantly improve the quality of treatment and outcomes for patients affected with recurrent respiratory papillomatosis, with human papillomavirus vaccination having a potentially important role.
Keywords: recurrent respiratory papillomatosis, laryngeal papillomatosis, adjuvant, cidofovir, bevacizumab, photodynamic therapy, microdebrider, angiolytic laser, celecoxib, HspE7
Introduction
Recurrent respiratory papillomatosis (RRP) is characterized by the development of exophytic proliferative lesions of connective tissue covered by epithelium which affect the mucosa of the airways. The condition is caused by human papillomavirus (HPV) infection, and is also termed laryngeal papillomatosis or glottal papillomatosis due to the strong predilection for the larynx,1 although papillomas may present anywhere along the respiratory tract.2 Deregulated expression of virus early genes in basal epithelial cells and genomic instability, causing secondary host genomic imbalances, are considered key events in the progression of HPV-promoted lesions.
HPVs affecting the mucosal tracts can be broadly divided into high-risk and low-risk types, based on their ability to cause malignant transformation of epithelial cells.3 High-risk types HPV-16 and HPV-18 are most commonly associated with cervical cancers as well as a subset of oropharyngeal carcinomas.4 HPV-6 and HPV-11 account for most cases of RRP and are considered low-risk subtypes, typically not associated with malignancy.5 In RRP, HPV-11 infection occurs most commonly and the disease presents an aggressive clinical course,6 followed by HPV-6. Rarely, RRP is caused by HPV types 16, 18, 31, and 33.7
A bimodal age distribution is characteristic, with young children or young adults affected. In children, vertical transmission from an infected mother during vaginal delivery8–11 or in utero12,13 has been documented. In adults, HPV infection might occur following oral sex.14,15 However, the simple presence of HPV in the upper airway tract does not necessarily cause infection of the mucosa; immunodeficiency and associated infections, particularly those associated with herpes viruses,16–18 might be determining factors. An effective immune response to viral infection involves activation of both innate and adaptive immunity, and appropriate signaling through the receptors they bind.19 Differences in HPV-specific immune responses between RRP patients and controls have been demonstrated.20–24 More recently, Hatam et al observed that the overwhelming majority of CD4+ cells in papillomas are either actively involved in immune suppression or are chronically stimulated, and are likely exhausted effector T-cells that fail to respond to HPV/tumor antigen exposure.25 A better understanding of this phenomenon could help develop novel strategies to reverse T-cell exhaustion and restore TH1-like function in RRP. A possible genetic susceptibility that would favor the development of laryngeal papillomatosis as a result of epithelial HPV infection was also suggested.26,27
In 1923, Ullmann first described the viral etiology of laryngeal papillomatosis,28 later confirmed by electron microscopy, in situ hybridization, and polymerase chain reaction techniques.29–31 The diagnosis of RRP may be challenging unless there is a high index of suspicion and awareness of the variable presentations. As previously mentioned, exophytic lesions affect the airways in RRP, and a multitude of signs and symptoms can be observed, including hoarseness, chronic cough, dyspnea, recurrent upper respiratory infections, pneumonias, dysphagia, stridor, or failure to thrive. The symptoms tend to be more severe in children because of the commonly rapid growth of the lesions, hence the condition can be potentially life-threatening in these patients despite being histologically benign.
Reeves et al investigated the clinical course of juvenile-onset RRP in a large sample representative of the USA and found young age to be the most important factor correlated with disease severity (frequency of surgery, extent of disease at diagnosis, and progression of disease).1 Children whose RRP is diagnosed at a younger age (<3 years) were found to be 3.6 times more likely to have more than four surgeries per year and almost twice as likely to have multiple anatomic sites affected than children whose RRP is diagnosed at an older age.32 In adult-onset RRP, the risk factors for an aggressive disease course appeared to be HPV-11 infection and observation time longer than 10 years.33
To date, the best estimate of the incidence and prevalence of RRP in the USA is based on a study conducted in 1995 by the RRP Task Force which projected an incidence in children of about 4.3 per 100,000 and about 1.8 per 100,000 in adults.34 However, the prevalence of the disease is likely variable depending on the age of presentation, country, and socioeconomic status.35,36 The prognosis is often good and the morbidity low in most cases, with variable clinical behavior, ie, lesions can regress, persist, or rarely malignant degeneration can occur.5,37 Clinical problems mainly arise from resistance to therapy, frequency of recurrences, and dissemination or extension of the growths to the lower airways, which is associated with a poorer prognosis.38
With regard to treatment, surgery is currently employed to secure airway patency, preserve the underlying laryngeal tissues, and maintain an acceptable quality of voice. Surgery has been traditionally performed via microscopic or endoscopic rigid laryngoscopy using a variety of lasers to debulk the papillomatous lesions. Unfortunately, lesions are generally multiple, and require multiple surgical excisions over a short period of time due to the high tendency to relapse.1,39,40
Medical treatment alone is currently unable to control or eradicate the disease. The aim of this review is to present an overview on current and future perspectives in the management of RRP.
Current management of RRP
Surgery
The traditional standard surgical treatment is performed with lasers and consists of debulking the papillomatous lesions. However, possible complications, such as respiratory tract burns, severe laryngeal scarring and stenosis, distal injuries with tracheoesophageal fistulae, have prompted a rapid conversion from use of lasers to adoption of microdebriders.41–44 In addition, the ability of the microdebrider to selectively suction the affected tissue allowing for a more precise debridement with the use of a rapidly rotating integral blade, the limited damage to the underlying tissues, and the greater preservation of normal epithelium, represent useful characteristics in light of the nature of RRP, which often necessitates multiple interventions.34
Despite the adoption of more advanced surgical equipment, laryngeal sequelae still remain frequent complications, with anterior commissure synechiae and glottic stenosis frequently observed in children who have undergone multiple procedures, particularly in advanced stages.45–47
A tracheotomy is typically included among the surgical options; however, it is reserved for the most aggressive cases with impending airway compromise, where multiple debulking surgeries have failed. When a tracheotomy is unavoidable, decannulation should be considered as early as possible once the disease process is controlled and the airway is deemed stable. In fact, tracheotomy provides an additional site for rapid colonization and serves as a conduit for distal disease spread to the tracheobronchial tree.48 Cole et al observed tracheal papillomas in more than half of patients with RRP who underwent tracheotomy.49
Nonsurgical adjuvant treatment
In light of the etiology of the condition, there have been several attempts to treat RRP medically. Unfortunately, despite some convincing theories, many treatments have proved to be ineffective, and in general medical treatment can only be considered as adjuvant to surgery.
Cidofovir
Cidofovir is an analog of cytosine and was originally developed and investigated for the treatment of cancer; its antiviral activity against DNA viruses was subsequently documented, and it is currently the antiviral most commonly used in medical adjuvant treatment for RRP.50 This treatment was first hypothesized a few decades ago, and subsequently tested in patients with severe recurrent laryngeal papillomatosis.51 The precise mechanism of action against HPV is not well understood. However, induction of apoptosis and augmentation of immune responses have been proposed as mechanisms of action.52
Some prospective studies of patients treated with intralesional injections of cidofovir at the time of surgery showed partial to complete regression of papillomas and a decrease in the frequency of debulking surgeries.52–59 In addition, it appears that intralesional administration does not produce systemic toxicity or local side effects; plasma levels are below those leading to toxicity, and are dose-dependent in children.59
There is no accepted protocol for dose, frequency of administration, or drug concentration.60 However, due to the long-lasting effect, infrequent administration of cidofovir is feasible. Pransky et al found that the greatest benefit may be had when repeated injections are performed at short time intervals (2–4 weeks) in aggressive disease.53 Naiman et al similarly reported that patients receiving injections less often than monthly had a less favorable response.59 In addition, the number of injections required to achieve a clinically relevant response is unclear. This probably points toward the variability in disease biology rather than the treatment protocol adopted, and suggests that treatment of this condition may need to be tailored to the individual patient. Cidofovir dosing is also controversial: a systematic review on published dosing regimens of cidofovir as an adjuvant in juvenile and adult RRP showed concentrations of cidofovir ranging from 0.0001 to 37.5 mg/mL, with 42% of articles reporting an adopted concentration of 5 mg/mL.61 A recent report suggested adoption of similar concentrations in children and adults, with recommended cidofovir concentrations ranging between 2.5 and 7.5 mg/mL, with the total dose not exceeding 3 mg/kg.62
Accordingly to Akst et al sequentially increased dosages of locally administered cidofovir may improve the response in pediatric patients. They described the practice of increasing the concentrations of cidofovir from 5 to 10 mg/mL during the course of treatment of RRP (stepped-dose protocol).55 Pransky et al observed the need for increasing the concentration of the drug in children, as the injectable volume can be a limiting factor in the pediatric population. In practice, submucosal injection may cause temporary swelling of the vocal folds, with the risk of airway obstruction in infants with narrow airways.63 More recently, administration of inhaled cidofovir has been reported and might offer further ground for clinical research in the immediate future.64
Other antivirals
Unlike children, co-infection with herpes simplex virus and Epstein-Barr virus in adults may lead to more aggressive RRP.16,18 This might support the use of antiviral treatments as adjuvant therapy in RRP. Ribavirin is a broad-spectrum antiviral agent that has been used systemically or topically (aerosol), but has not shown obvious efficacy in suppressing or treating RRP in clinical studies.65,66 Acyclovir has been employed in RRP, although it is not directly active against HPV and has shown poor results.67
Interferon
Interferons are proteins that are naturally produced by human leucocytes in response to a variety of stimuli, including viral infection. They bind to specific membrane receptors and alter cell metabolism, with antiviral, antiproliferative, and immunomodulatory effects. Although the exact mechanism of action of interferons in laryngeal papillomatosis is not known, they were among the first agents adopted as adjuvant therapy for laryngeal papillomatosis.68,69
There is controversial evidence regarding the clinical efficacy of interferons. Healy et al found that interferon was not curative when employed alone, and a lack of benefit in the long term was also noted when it was used as an adjunctive agent.69 However, other reports have shown a positive response in some pediatric patients.69,70
The main limitation related to intravenous administration is systemic toxicity, with a reversible increase in serum transaminase levels, and possible leucopenia and thrombocytopenia. Patients can experience transient fever, fatigue, nausea, arthralgia, and headache, along with spastic diplegia in infants.
Recently, alternative topical delivery of interferon alpha via biphasic vesicles has been investigated.71,72 Topical application of biphasic vesicles containing interferon alpha resulted in sustained local delivery of biologically active interferon alpha with minimal systemic exposure,73 but further studies in RRP patients are necessary.
Indole-3-carbinol
Indole-3-carbinol is derived from cruciferous vegetables (eg, sprouts, broccoli, cabbage) and is known to affect papilloma growth in vitro through its effect on estrogen metabolism. While no adverse events in children were noted in a small case series of patients treated with oral administration of indole-3-carbinol, doubts regarding its clinical efficacy persist.74 No further studies of this agent have been planned.
Cis-retinoic acid
Adjunctive use of cis-retinoic acid as treatment for laryngeal lesions caused by HPV was investigated in clinical studies over 2 decades ago.75,76 The hypothesis was that its antiproliferative action on epithelial tissues could be used to halt or delay recurrent growth of papillomatous lesions. Due to its lack of efficacy, experiments with cis-retinoic acid are no longer being undertaken in patients with RRP. Currently, it is used to treat epithelial acne.
Mumps vaccine
The use of intralesional mumps vaccine as adjuvant therapy was considered to be an intriguing hypothesis in need of further investigation.77,78 A recent, prospective, randomized controlled interventional study was planned on the basis that the measles-mumps-rubella vaccine might either prevent further recurrences of RRP or prolong its remission.79 All of the 26 enrolled patients underwent surgical excision of their lesions and 13 patients in the study group were prospectively randomized to receive a topical coating of the measles-mumps-rubella vaccine at the site of the excised lesion.79 Although showing a prolonged remission period, it did not appear to be significantly better.
HspE7
HspE7 is a recombinant fusion protein of Mycobacterium bovis heat shock protein 65 and E7 protein from HPV-16. In an open-label study, 27 patients were given 500 μg of subcutaneous HspE7 monthly for three doses over 3 months, and followed for up to 5 years. A promising decrease in frequency of surgery was reported, with mild reactions at the site of injection.80
Control of gastroesophageal reflux disease
The presence of laryngopharyngeal reflux disease has been associated with worsening manifestations of RRP and increased treatment complications. Irritation of the epithelium of the aerodigestive tract caused by laryngopharyngeal reflux disease, either through acid or gastric enzyme interaction, may produce mucosal damage or an inflammatory response that could potentially trigger proliferation or spread of papilloma disease. Effective disease management may result in improved control of RRP and possibly complete remission.81–84
Studies have shown that treatment with cimetidine or a proton pump inhibitor may result in improved control or complete remission of RRP.82,84 Following remission, papillomatous disease requiring surgery recurred in the event of discontinuation of antireflux therapy in a study reported by McKenna et al.84 After these early observations, further larger controlled studies might be required to establish the role of antireflux therapy in the treatment algorithm for RRP.
Photodynamic therapy
Photodynamic therapy (PDT) looks promising in the treatment of RRP. It requires an injectable photosensitizer and promotes apoptosis after laser excitation of the agent. The photosensitizer is activated by light and interacts with molecular oxygen to produce an excited state (reactive singlet oxygen); its direct cytotoxic activity and microvascular damage contribute to the destruction of proliferating cells, which is manifested as swelling and formation of necrotic tissue. In conventional PDT, the photosensitized tissue is exposed to intense light for seconds to minutes, which results in short-term production of powerful oxidants; in a novel approach, a longer interstitial light delivery system leads to prolonged or repeated photoactivation of the photosensitizing agents, resulting in a larger number of cytocidal oxygen molecules in individual cells, increased cell death, and increased volume and depth of PDT-induced tissue necrosis. The benefit of this approach lies in its ability to selectively treat the abnormally proliferating cells without damaging healthy tissue.85,86 PDT has been approved for use in lung cancer, esophageal cancer, and Barrett’s esophagus, and might prove beneficial in RRP in light of its common characteristics, including the superficial area of disease and high cell turnover.
In RRP, PDT may also alter the immune response and increase the reactivity to even low concentrations of viral proteins.87,88 Current evidence regarding the efficacy of PDT in RRP is controversial.89–91 To date, there is insufficient evidence from high-quality, randomized controlled trials to determine whether PDT alters the course of RRP or provides an added benefit to surgery in patients with the disease. Certainly, PDT remains an area for future study.
Future treatment possibilities
Surgery
Angiolytic lasers precisely target hemoglobin within the microcirculation of papillary lesions, and adoption of this technology in RRP would have obvious advantages.92 In fact, such lasers allow for a more precise removal, thus easier preservation of the delicate laryngeal tissues can be guaranteed. Early clinical studies have investigated the efficacy of clinical application of this novel technology in RRP and reported promising results.93 In the near future, we will likely move toward a further change in trends for the surgical treatment of RRP, with angiolytic lasers taking the place of microdebriders (Table 1).
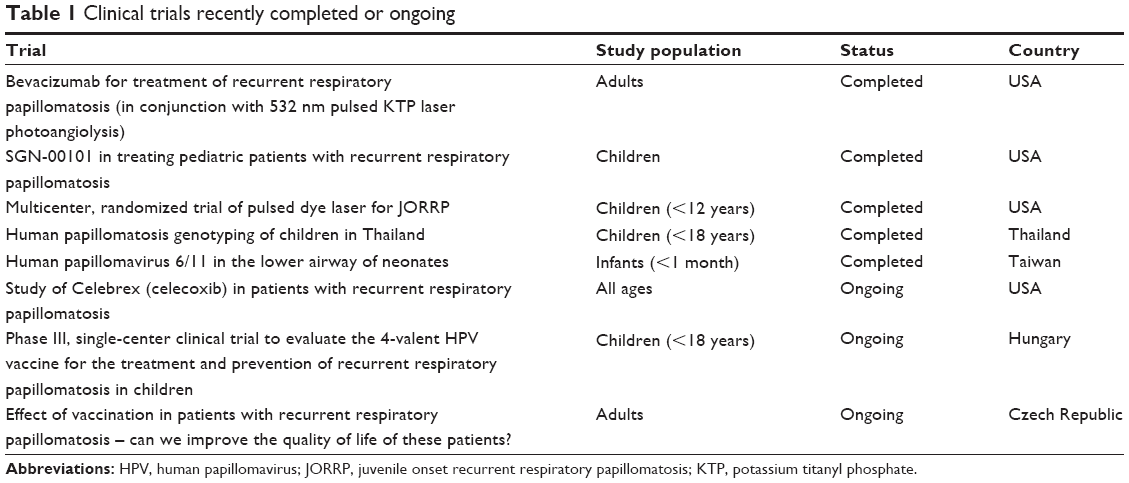 | Table 1 Clinical trials recently completed or ongoing |
Adjuvants
Bevacizumab
Bevacizumab is a recombinant humanized monoclonal immunoglobulin G1 antibody that binds to and inhibits the biologic activity of human vascular endothelial growth factor in vitro and in vivo, by preventing receptor activation. Based on the evidence that vascular endothelial growth factor is an important factor in the development of RRP, there have been some recent reports of promising results achieved with relatively high dosing (up to 45–50 mg) of bevacizumab in all patients treated.94–96 The dose approved by the US Food and Drug Administration is 12.5 mg. This adjuvant therapy would increase the time interval between surgical procedures, with a simultaneous reduction in number of procedures required per year, and it also seems that improvements in voice quality can be achieved.95
The favorable clinical results of bevacizumab and KTP laser reported within the last 2 years and the lack of complications after over 200 laryngeal injections of bevacizumab have brought this therapeutic approach to the top of the list of RRP treatment options.97,98
Celecoxib
Celecoxib is a cyclooxygenase-2-selective nonsteroidal anti-inflammatory drug, commonly used to treat signs and symptoms of osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, acute pain in adults, painful menstruation, and juvenile rheumatoid arthritis. Limsukon et al successfully treated a patient with RRP using a combination of erlotinib and celecoxib, arguing that papillomas overexpress the epidermal growth factor receptor, and show increased expression of cyclooxygenase-2 and prostaglandin E2.99 While they found their approach effective in controlling papilloma growth, more research is necessary to determine the long-term safety and effectiveness of such therapies for individuals with RRP, and is currently ongoing (Table 1).
HPV vaccine
Currently, two HPV vaccines are available, ie, a bivalent vaccine designed against the L1 capsid proteins of HPV-16 and HPV-18, and a prophylactic quadrivalent vaccine with activity against HPV-6, HPV-11, HPV-16, and HPV-18. Although vaccination against HPV-16 and HPV-18 may help prevent cervical cancer, the bivalent vaccine does not address HPV-6 and HPV-11, which are the most common causes of RRP. The quadrivalent vaccine is approved for administration in young female teenagers as well as young boys. HPV infection seems to be as common in men as in women but is often asymptomatic, which contributes to the high rate of transmission between sexual partners. While both, males and females benefit from vaccination,100 it is uncertain what effect this will have on neonatal transmission of HPV or on the overall incidence of RRP. Although further research is necessary, it is possible that vaccines might eventually be useful in neonates for two reasons: via transmission of immunity through maternal antibodies and through direct vaccination of neonates similar to neonatal vaccination for hepatitis B. Currently, HPV vaccines are not approved for routine use in neonates, hence this application also requires further research. Theoretically, mass HPV vaccination could provide the community with immunity against the disease, and if such a community status exists, there will be a consequent decrease in incidence of RRP disease.
A direct effect of vaccination in patients already affected by RRP has also been observed. In 2008, Förster et al reported the case of a 2-year-old with aggressive laryngeal papillomatosis.101 After three shots of tetravalent HPV injection, the patient’s condition was stabilized without surgery. In 2011, Mudry et al reported the case of a 5-year-old with frequently recurring papillomas submitted to multiple procedures, who entered a remission period lasting 17 months after administration of the tetravalent HPV vaccine.102 A study by Hočevar-Boltežar et al pointed out that vaccination with the quadrivalent HPV vaccine can favorably influence the course of RRP in patients with rapid growth of papillomas, with significantly prolonged intervals between surgical procedures and reduction of the number of procedures needed in the majority of patients observed.103 Although promising, these isolated positive experiences need to be validated by multicenter trials that might be able to ascertain the true benefits of vaccination as a treatment of RRP (Table 1).
Author contributions
The authors contributed equally to the study design and conduct, and preparation of the manuscript.
Disclosure
The authors have no financial or proprietary interest in any material or method mentioned in this paper and did not receive any relevant financial support.
References
Reeves WC, Ruparelia SS, Swanson KI, Derkay CS, Marcus A, Unger ER. National registry for juvenile-onset recurrent respiratory papillomatosis. Arch Otolaryngol Head Neck Surg. 2003;129(9):976–982. | ||
Gélinas JF, Manoukian J, Côté A. Lung involvement in juvenile onset recurrent respiratory papillomatosis: a systematic review of the literature. Int J Pediatr Otorhinolaryngol. 2008;72(4):433–452. | ||
Michaud DS, Langevin SM, Eliot M, et al. High-risk HPV types and head and neck cancer. Int J Cancer. 2014;135(7):1653–1661. | ||
D’Souza G, Gross ND, Pai SI, et al. Oral human papillomavirus (HPV) infection in HPV-positive patients with oropharyngeal cancer and their partners. J Clin Oncol. 2014;32(23):2408–2415. | ||
Hartley C, Hamilton J, Birzgalis AR, et al. Recurrent respiratory papillomatosis – the Manchester experience, 1974–1992. J Laryngol Otol. 1994;108(3):226–229. | ||
Wiatrak BJ, Wiatrak DW, Broker TR, Lewis L. Recurrent respiratory papillomatosis: a longitudinal study comparing severity associated with human papilloma viral types 6 and 11 and other risk factors in a large pediatric population. Laryngoscope. 2004;114(11 Pt 2 Suppl 104):1–23. | ||
Venkatesan NN, Pine HS, Underbrink MP. Recurrent respiratory papillomatosis. Otolaryngol Clin North Am. 2012;45(3):671–694. | ||
Silverberg MJ, Thorsen P, Lindeberg H, Grant LA, Shah KV. Condyloma in pregnancy is strongly predictive of juvenile-onset recurrent respiratory papillomatosis. Obstet Gynecol. 2003;101(4):645–652. | ||
Shah KV, Stern WF, Shah FK, Bishai D, Kashima HK. Risk factors for juvenile onset recurrent respiratory papillomatosis. Pediatr Infect Dis J. 1998;17(5):372–376. | ||
Hallden C, Majmudar B. The relationship between juvenile laryngeal papillomatosis and maternal condylomata acuminata. J Reprod Med. 1986;31(9):804–807. | ||
Bennett RS, Powell KR. Human papillomaviruses: associations between laryngeal papillomas and genital warts. Pediatr Infect Dis J. 1987;6(3):229–232. | ||
Kosko JR, Derkay CS. Role of cesarean section in prevention of recurrent respiratory papillomatosis – is there one? Int J Pediatr Otorhinolaryngol. 1996;35(1):31–38. | ||
Winckworth LC, Nichol R. Question 2: do caesarean sections reduce the maternal-fetal transmission rate of human papillomavirus infection? Arch Dis Child. 2010;95(1):70–73. | ||
Kashima HK, Shah F, Lyles A, et al. A comparison of risk factors in juvenile-onset and adult-onset recurrent respiratory papillomatosis. Laryngoscope. 1992;102(1):9–13. | ||
Ruiz R, Achlatis S, Verma A, et al. Risk factors for adult-onset recurrent respiratory papillomatosis. Laryngoscope. 2014;124(10):2338–2344. | ||
Rimell FL, Shoemaker DL, Pou AM, Jordan JA, Post JC, Ehrlich GD. Pediatric respiratory papillomatosis: prognostic role of viral typing and cofactors. Laryngoscope. 1997;107(7):915–918. | ||
DeVoti J, Hatam L, Lucs A, et al. Decreased Langerhans cell responses to IL-36γ: altered innate immunity in patients with recurrent respiratory papillomatosis. Mol Med. 2014;20:372–380. | ||
Pou AM, Rimell FL, Jordan JA, et al. Adult respiratory papillomatosis: human papillomavirus type and viral coinfections as predictors of prognosis. Ann Otol Rhinol Laryngol. 1995;104(10):758–762. | ||
Steinman L. A brief history of T(H)17, the first major revision in the T(H)1/T(H)2 hypothesis of T cell-mediated tissue damage. Nat Med. 2007;13(2):139–145. | ||
Bonagura VR, Siegal FP, Abramson AL, et al. Enriched HLA-DQ3 phenotype and decreased class I major histocompatibility complex antigen expression in recurrent respiratory papillomatosis. Clin Diagn Lab Immunol. 1994;1(3):357–360. | ||
Vambutas A, Bonagura VR, Reed EF, et al. Polymorphism of transporter associated with antigen presentation 1 as a potential determinant for severity of disease in recurrent respiratory papillomatosis caused by human papillomavirus types 6 and 11. J Infect Dis. 2004;189(5):871–879. | ||
DeVoti JA, Steinberg BM, Rosenthal DW, et al. Failure of gamma interferon but not interleukin-10 expression in response to human papillomavirus type 11 E6 protein in respiratory papillomatosis. Clin Diagn Lab Immunol. 2004;11(3):538–547. | ||
Bonagura VR, Hatam L, DeVoti J, Zeng F, Steinberg BM. Recurrent respiratory papillomatosis: altered CD8(+) T-cell subsets and T(H)1/T(H)2 cytokine imbalance. Clin Immunol. 1999;93(3):302–311. | ||
Bonagura VR, Hatam LJ, Rosenthal DW, et al. Recurrent respiratory papillomatosis: a complex defect in immune responsiveness to human papillomavirus-6 and -11. APMIS. 2010;118(6–7):455–470. | ||
Hatam LJ, Devoti JA, Rosenthal DW, et al. Immune suppression in premalignant respiratory papillomas: enriched functional CD4+Foxp3+ regulatory T cells and PD-1/PD-L1/L2 expression. Clin Cancer Res. 2012;18(7):1925–1935. | ||
Aaltonen LM, Rihkanen H, Vaheri A. Human papillomavirus in larynx. Laryngoscope. 2002;112(4):700–707. | ||
Buchinsky FJ, Derkay CS, Leal SM, Donfack J, Ehrlich GD, Post JC. Multicenter initiative seeking critical genes in respiratory papillomatosis. Laryngoscope. 2004;114(2):349–357. | ||
Ullmann EV. On the etiology of laryngeal papilloma. Acta Otolaryngol. 1923;5(4):317–334. | ||
Duggan MA, Lim M, Gill MJ, Inoue M. HPV DNA typing of adult-onset respiratory papillomatosis. Laryngoscope. 1990;100(6):639–642. | ||
Maisel R, Rimell F, Dayton V. In situ hybridization and laryngeal papillomas. Ann Otol Rhinol Laryngol. 1992;101(2):119–126. | ||
Multhaupt HAB, Fessler JN, Warhol MJ. Detection of human papillomavirus in laryngeal lesions by in situ hybridization. Hum Pathol. 1994;25(12):1302–1305. | ||
Derkay CS. Recurrent respiratory papillomatosis. Laryngoscope. 2001;111(1):57–69. | ||
Omland T, Akre H, Lie KA, Jebsen P, Sandvik L, Brøndbo K. Risk factors for aggressive recurrent respiratory papillomatosis in adults and juveniles. PLoS One. 2014;9(11):e113584. | ||
Armstrong LR, Derkay CS, Reeves WC. Initial results from the national registry for juvenile-onset recurrent respiratory papillomatosis. RRP Task Force. Arch Otolaryngol Head Neck Surg. 1999;125(7):743–748. | ||
Leung R, Hawkes M, Campisi P. Severity of juvenile onset recurrent respiratory papillomatosis is not associated with socioeconomic status in a setting of universal health care. Int J Pediatr Otorhinolaryngol. 2007;71(6):965–972. | ||
Marsico M, Mehta V, Chastek B, Liaw KL, Derkay C. Estimating the incidence and prevalence of juvenile-onset recurrent respiratory papillomatosis in publicly and privately insured claims databases in the United States. Sex Transm Dis. 2014;41(5):300–305. | ||
Gorgoulis V, Rassidakis G, Karameris A, et al. Expression of p53 protein in laryngeal squamous cell carcinoma and dysplasia: possible correlation with human papillomavirus infection and clinicopathological findings. Virchows Arch. 1994;425(5):481–489. | ||
Doyle JD, Gianoli JG, Espinola T, Miller RH. Recurrent respiratory papillomatosis: juvenile versus adult forms. Laryngoscope. 1994;104(5):523–527. | ||
Soldatski IL, Onufrieva EK, Steklov AM, Schepin NV. Tracheal, bronchial, and pulmonary papillomatosis in children. Laryngoscope. 2005;115(10):1848–1854. | ||
Silverberg MJ, Thorsen P, Lindeberg H, Ahdieh-Grant L, Shah KV. Clinical course of recurrent respiratory papillomatosis in Danish children. Arch Otolaryngol Head Neck Surg. 2004;130(6):711–716. | ||
El-Bitar MA, Zalzal GH. Powered instrumentation in the treatment of recurrent respiratory papillomatosis: an alternative to the carbon dioxide laser. Arch Otolaryngol Head Neck Surg. 2002;128(4):425–428. | ||
Patel N, Rowe M, Tunkel D. Treatment of recurrent respiratory papillomatosis in children with the microdebrider. Ann Otol Rhinol Laryngol. 2003;112(1):7–10. | ||
Pasquale K, Wiatrak B, Woolley A, Lewis L. Microdebrider versus CO2 laser removal of recurrent respiratory papillomas: a prospective analysis. Laryngoscope. 2003;113(1):139–143. | ||
Dedo HH, Yu KC. CO(2) laser treatment in 244 patients with respiratory papillomas. Laryngoscope. 2001;111(9):1639–1644. | ||
Hermann JS, Pontes P, Weckx LL, Fujita R, Avelino M, Pignatari SS. [Laryngeal sequelae of recurrent respiratory papillomatosis surgery in children]. Rev Assoc Med Bras. 2012;58(2):204–208. Portuguese. | ||
Derkay CS, Malis DJ, Zalzal G, et al. A staging system for assessing severity of disease and response to therapy in recurrent respiratory papillomatosis. Laryngoscope. 1998;108(6):935–937. | ||
Derkay CS, Hester RP, Burke B, et al. Analysis of a staging assessment system for prediction of surgical interval in recurrent respiratory papillomatosis. Int J Pediatr Otorhinolaryngol. 2004;68(12):1493–1498. | ||
Tasca RA, Clarke RW. Recurrent respiratory papillomatosis. Arch Dis Child. 2006;91(8):689–691. | ||
Cole RR, Myer CM III, Cotton RT. Tracheotomy in children with recurrent respiratory papillomatosis. Head Neck. 1989;11(3):226–230. | ||
De Clercq E, Descamps J, De Somer P, Holyacute A. (S)-9-(2,3-dihydroxypropyl) adenine: an aliphatic nucleoside analog with broad-spectrum antiviral activity. Science. 1978;200(4341):563–565. | ||
Snoeck R, Wellens W, Desloovere C, et al. Treatment of severe laryngeal papillomatosis with intralesional injections of cidofovir. J Med Virol. 1998;54(3):219–225. | ||
Shehab N, Sweet B, Hogikyan ND, et al. Cidofovir for the treatment of recurrent respiratory papillomatosis: a review of the literature. Pharmacotherapy. 2005;25(7):977–989. | ||
Pransky SM, Albright JT, Magit AE. Long-term follow-up of pediatric recurrent respiratory papillomatosis managed with intralesional cidofovir. Laryngoscope. 2003;113(9):1583–1587. | ||
Milczuk HA. Intralesional cidofovir for the treatment of severe juvenile recurrent respiratory papillomatosis: long-term results in 4 children. Otolaryngol Head Neck Surg. 2003;128(6):788–794. | ||
Akst LM, Lee W, Discolo C, et al. Stepped-dose protocol of cidofovir therapy in recurrent respiratory papillomatosis in children. Arch Otolaryngol Head Neck Surg. 2003;129(8):841–846. | ||
Lee AS, Rosen CA. Efficacy of cidofovir injection for the treatment of recurrent respiratory papillomatosis. J Voice. 2004;18(4):551–556. | ||
Peyton SW, Wiatrak B. Is cidofovir a useful adjunctive therapy for recurrent respiratory papillomatosis in children? Int J Pediatr Otorhinolaryngol. 2004;68(4):413–418. | ||
Mandell DL, Arjmand EM, Kay DJ, et al. Intralesional cidofovir for pediatric recurrent respiratory papillomatosis. Arch Otolaryngol Head Neck Surg. 2004;130(11):1319–1323. | ||
Naiman AN, Ceruse P, Coulombeau B, et al. Intralesional cidofovir and surgical excision for laryngeal papillomatosis. Laryngoscope. 2003;113(12):2174–2181. | ||
Derkay C; Multi-Disciplinary Task Force on Recurrent Respiratory Papillomas. Cidofovir for recurrent respiratory papillomatosis (RRP): a re-assessment of risks. Int J Pediatr Otorhinolaryngol. 2005;69(11):1465–1467. | ||
Clamp PJ, Saunders MW. Systematic review of intralesional cidofovir dosing regimens in the treatment of recurrent respiratory papillomatosis. Int J Pediatr Otorhinolaryngol. 2013;77(3):323–328. | ||
Derkay CS, Volsky PG, Rosen CA, et al. Current use of intralesional cidofovir for recurrent respiratory papillomatosis. Laryngoscope. 2013;123(3):705–712. | ||
Pransky SM, Magit AE, Kearns DB, Kang DR, Duncan NO. Intralesional cidofovir for recurrent respiratory papillomatosis in children. Arch Otolaryngol Head Neck Surg. 1999;125(10):1143–1148. | ||
Ksiazek J, Prager JD, Sun GH, et al. Inhaled cidofovir as an adjuvant therapy for recurrent respiratory papillomatosis. Otolaryngol Head Neck Surg. 2011;144(4):639–641. | ||
Chadha NK, James AL. Antiviral agents for the treatment of recurrent respiratory papillomatosis: a systematic review of the English-language literature. Otolaryngol Head Neck Surg. 2007;136(6):863–869. | ||
Morrison GA, Kotecha B, Evans JN, et al. Ribavarin treatment for juvenile respiratory papillomatosis. J Laryngol Otol. 1993;107(5):423–426. | ||
Endres DR, Bauman NM, Burke D, Smith RJ. Acyclovir in the treatment of recurrent respiratory papillomatosis. A pilot study. Ann Otol Rhinol Laryngol. 1994;103(4 Pt 1):301–305. | ||
Leventhal BG, Kashima HK, Weck PW, et al. Randomized surgical adjuvant trial of interferon alfa-n1 in recurrent papillomatosis. Arch Otolaryngol Head Neck Surg. 1988;114(10):1163–1169. | ||
Healy GB, Gelber RD, Trowbridge AL, Grundfast KM, Ruben RJ, Price KN. Treatment of recurrent respiratory papillomatosis with human leukocyte interferon. Results of a multicenter randomized clinical trial. N Engl J Med. 1988;319(7):401–407. | ||
Nodarse-Cuní H, Iznaga-Marín N, Viera-Alvarez D, et al. Interferon alpha-2b as adjuvant treatment of recurrent respiratory papillomatosis in Cuba: National Programme (1994–1999 report). J Laryngol Otol. 2004;118(9):681–687. | ||
Foldvari M, Badea I, Kumar P, et al. Biphasic vesicles for topical delivery of interferon alpha in human volunteers and treatment of patients with human papillomavirus infections. Curr Drug Deliv. 2011;8(3):307–319. | ||
King M, Kumar P, Michel D, Batta R, Foldvari M. In vivo sustained dermal delivery and pharmacokinetics of interferon alpha in biphasic vesicles after topical application. Eur J Pharm Biopharm. 2013;84(3):532–539. | ||
Foldvari M, Kumar P. Recent progress in the application of nanotechnology for prevention and treatment of human papillomavirus infection. Ther Deliv. 2012;3(8):1005–1017. | ||
Rosen CA, Bryson PC. Indole-3-carbinol for recurrent respiratory papillomatosis: long-term results. J Voice. 2004;18(2):248–253. | ||
Bell R, Hong WK, Itri LM, McDonald G, Strong MS. The use of cis-retinoic acid in recurrent respiratory papillomatosis of the larynx: a randomized pilot study. Am J Otolaryngol. 1988;9(4):161–164. | ||
Lippman SM, Donovan DT, Frankenthaler RA, et al. 13-Cis-retinoic acid plus interferon-alpha 2a in recurrent respiratory papillomatosis. J Natl Cancer Inst. 1994;86(11):859–861. | ||
Pashley NR. Can mumps vaccine induce remission in recurrent respiratory papilloma? Arch Otolaryngol Head Neck Surg. 2002;128(7):783–786. | ||
Lieu JE, Molter DW. Another potential adjuvant therapy for recurrent respiratory papillomatosis. Arch Otolaryngol Head Neck Surg. 2002;128(7):787–788. | ||
Lei J, Yu W, Yuexin L, Qi C, Xiumin S, Tianyu Z. Topical measles-mumps-rubella vaccine in the treatment of recurrent respiratory papillomatosis: results of a preliminary randomized, controlled trial. Ear Nose Throat J. 2012;91(4):174–175. | ||
Derkay CS, Smith RJ, McClay J, et al. HspE7 treatment of pediatric recurrent respiratory papillomatosis: final results of an open-label trial. Ann Otol Rhinol Laryngol. 2005;114(9):730–737. | ||
Borkowski G, Sommer P, Stark T, Sudhoff H, Luckhaupt H. Recurrent respiratory papillomatosis associated with gastroesophageal reflux disease in children. Eur Arch Otorhinolaryngol. 1999;256(7):370–372. | ||
Harcourt JP, Worley G, Leighton SE. Cimetidine treatment for recurrent respiratory papillomatosis. Int J Pediatr Otorhinolaryngol. 1999;51(2):109–113. | ||
Holland BW, Koufman JA, Postma GN, McGuirt WF Jr. Laryngopharyngeal reflux and laryngeal web formation in patients with pediatric recurrent respiratory papillomas. Laryngoscope. 2002;112(11):1926–1929. | ||
McKenna M, Brodsky L. Extraesophageal acid reflux and recurrent respiratory papilloma in children. Int J Pediatr Otorhinolaryngol. 2005;69(5):597–605. | ||
Dolmans DE, Fukumura D, Jain RK. Photodynamic therapy for cancer. Nat Rev Cancer. 2003;3(5):380–387. | ||
Dougherty TJ, Gomer CJ, Henderson BW, et al. Photodynamic therapy. J Natl Cancer Inst. 1998;90(12):889–905. | ||
Shikowitz MJ, Abramson AL, Steinberg BM, et al. Clinical trial of photodynamic therapy with mesotetra (hydroxyphenyl) chlorin for respiratory papillomatosis. Arch Otolaryngol Head Neck Surg. 2005;131(2):99–105. | ||
Lee RG, Vecchiotti MA, Heaphy J, et al. Photodynamic therapy of cottontail rabbit papillomavirus-induced papillomas in a severe combined immunodeficient mouse xenograft system. Laryngoscope. 2010;120(3):618–624. | ||
Abramson AL, Shikowitz MJ, Mullooly VM, Steinberg BM, Amella CA, Rothstein HR. Clinical effects of photodynamic therapy on recurrent laryngeal papillomas. Arch Otolaryngol Head Neck Surg. 1992;118(1):25–29. | ||
Abramson AL, Shikowitz MJ, Mullooly VM, Steinberg BM, Hyman RB. Variable light-dose effect on photodynamic therapy for laryngeal papillomas. Arch Otolaryngol Head Neck Surg. 1994;120(8):852–855. | ||
Lieder A, Khan MK, Lippert BM. Photodynamic therapy for recurrent respiratory papillomatosis. Cochrane Database Syst Rev. 2014;6:CD009810. | ||
Burns JA, Zeitels SM, Akst LM, Broadhurst MS, Hillman RE, Anderson R. 532 nm pulsed potassium-titanyl-phosphate laser treatment of laryngeal papillomatosis under general anesthesia. Laryngoscope. 2007;117(8):1500–1504. | ||
Kuet ML, Pitman MJ. Photoangiolytic laser treatment of recurrent respiratory papillomatosis: a scaled assessment. J Voice. 2013;27(1):124–128. | ||
Sidell DR, Nassar M, Cotton RT, Zeitels SM, de Alarcon A. High-dose sublesional bevacizumab (Avastin) for pediatric recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol. 2014;123(3):214–221. | ||
Best SR, Friedman AD, Landau-Zemer T, et al. Safety and dosing of bevacizumab (Avastin) for the treatment of recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol. 2012;121(9):587–593. | ||
Rogers DJ, Ojha S, Maurer R, Hartnick CJ. Use of adjuvant intralesional bevacizumab for aggressive respiratory papillomatosis in children. JAMA Otolaryngol Head Neck Surg. 2013;139(5):496–501. | ||
Zeitels SM, Barbu AM, Landau-Zemer T, et al. Local injection of bevacizumab (Avastin) and angiolytic KTP laser treatment of recurrent respiratory papillomatosis of the vocal folds: a prospective study. Ann Otol Rhinol Laryngol. 2011;120(10):627–634. | ||
Ramet J, van Esso D, Meszner Z; European Academy of Paediatrics Scientific Working Group on Vaccination. Position paper – HPV and the primary prevention of cancer: improving vaccine uptake by paediatricians. Eur J Pediatr. 2011;170(3):309–321. | ||
Limsukon A, Susanto I, Hoo GW, Dubinett SM, Batra RK. Regression of recurrent respiratory papillomatosis with celecoxib and erlotinib combination therapy. Chest. 2009;136(3):924–926. | ||
Villa LL, Costa RL, Petta CA, et al. Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: a randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol. 2005;6(5):271–278. | ||
Förster G, Boltze C, Seidel J, Pawlita M, Müller A. [Juvenile laryngeal papillomatosis – immunisation with the polyvalent vaccine Gardasil]. Laryngorhinootologie. 2008;87(11):796–799. German. | ||
Mudry P, Vavrina M, Mazanek P, Machalova M, Litzman J, Sterba J. Recurrent laryngeal papillomatosis: successful treatment with human papillomavirus vaccination. Arch Dis Child. 2011;96(5):476–477. | ||
Hočevar-Boltežar I, Matičič M, Sereg-Bahar M, et al. Human papilloma virus vaccination in patients with an aggressive course of recurrent respiratory papillomatosis. Eur Arch Otorhinolaryngol. 2014;271(12):3255–3262. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.