")
Back to Journals » Clinical Interventions in Aging » Volume 18
Recurrence of Local Kyphosis After Percutaneous Kyphoplasty: The Neglected Injury of the Disc–Endplate Complex
Authors Wang JN, Xie W , Song DW , Zou J, Yan Q, Feng T, Jin SY, Yang C , Luo ZP, Niu JJ
Received 19 March 2023
Accepted for publication 8 May 2023
Published 18 May 2023 Volume 2023:18 Pages 827—834
DOI https://doi.org/10.2147/CIA.S410992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Jin-ning Wang,1,* Wei Xie,2,* Da-Wei Song,1,* Jun Zou,1 Qi Yan,1 Tao Feng,1 Sheng-yang Jin,1 Chao Yang,1 Zong-ping Luo,1,3 Jun-jie Niu1
1Department of Orthopaedic Surgery, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Department of Orthopaedics, Suzhou Ninth People’s Hospital, Suzhou, Jiangsu, People’s Republic of China; 3Orthopedic Institute, Department of Orthopaedic Surgery, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zong-ping Luo, Orthopedic Institute, Department of Orthopaedic Surgery, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China, Tel +86-512-67781351, Email [email protected] Jun-jie Niu, Department of Orthopaedic Surgery, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China, Tel +86-512-67780111, Email [email protected]
Background: Recurrent of local kyphosis after percutaneous kyphoplasty (PKP) is rarely reported and discussed. Literatures reported that re-kyphosis is usually a consequence of refractures of augmented or adjacent vertebra. However, whether re-kyphosis should be considered as a complication of refractures and has an impact on clinical efficacy of PKP during follow-up time is unknown. The purpose of this study is to evaluate the related risk factors and clinical significance of the recurrent of local kyphosis in osteoporotic vertebral fracture (OVF) patients without refractures.
Patients and Methods: A total of 143 patients who underwent single-level PKP were recruited and assigned into the re-kyphosis group and non-re-kyphosis group. Clinical and radiographic data were collected and compared between the two groups. Then, multivariate logistic regression analyses were conducted to identify the related risk factors.
Results: During follow-up, 16 of the 143 patients presented postoperative re-kyphosis. The average local kyphosis angle increased from 11.81± 8.60° postoperatively to 25.13± 8.91° at the final follow-up which showed a statistically significant difference (p< 0.05). Both groups had significant improvements in postoperative visual analogue scale (VAS) and Oswestry Disability Index (ODI) scores compared to their preoperative values (p< 0.05). However, in the re-kyphosis group at final follow-up, the VAS and ODI scores showed worsening compared to the postoperative scores. Logistic regression analysis showed that disc–endplate complex injury (OR=17.46, p=0.003); local kyphosis angle correction (OR=1.84, p< 0.001); and vertebral height restoration (OR=1.15, p=0.003) were risk factors for re-kyphosis.
Conclusion: Re-kyphosis is not rare in patients with osteoporotic vertebral fracture and tends to have an inferior prognosis following PKP surgery. Patients with disc–endplate complex injury and more correction of vertebral height and kyphosis angle are at a higher risk for re-kyphosis after PKP surgery than others.
Keywords: percutaneous kyphoplasty, risk factors, re-kyphosis, disc–endplate complex injury, clinical efficacy
Introduction
Osteoporotic vertebral fracture (OVF) is a common disease in older persons, and it is an important medical problem due to the increasing aging population worldwide. Percutaneous kyphoplasty (PKP), one of the vertebral augmentation techniques, has been shown to relieve back pain, restore vertebral height, and correct the kyphotic deformity.1,2
As the number of patients undergoing PKP increases, an increasing number of researchers and orthopedic practitioners have started to focus on surgery-related complications, among which postoperative refracture (also known as subsequent vertebral fracture) is considered the most common complication.3–5 However, the commonly neglected postoperative re-kyphosis has long been regarded as imaging findings of postoperative refracture.
Studies have reported that spinal local kyphosis has significant negative effects on patients’ daily life, resulting in persistent back pain, a higher incidence of adjacent vertebral fractures, decreased lung function, and increased mortality.6,7 In our clinical practice, we found that although several patients with OVF developed recurrent local kyphosis after PKP surgery during the follow-up period, no refractures of augmented or adjacent vertebrae were detected. This suggests the existence of other factors leading to re-kyphosis; that is, apart from refractures, there may be other unknown risk factors related to re-kyphosis. Therefore, it should be clarified whether re-kyphosis has an impact on the clinical efficacy of PKP. This study aimed to identify the related risk factors and evaluate the clinical significance of re-kyphosis after PKP surgery.
Materials and Methods
Patient Selection
The inclusion criteria of this study were as follows: (1) single-level bone marrow edema within vertebral body on fat-suppressed sequences and (2) patients suffered from severe back pain caused by mild-to-moderate injury, and the symptoms could not be relieved by conservative treatment for at least 1 week. The exclusion criteria were as follows: (1) non-osteoporotic vertebral fracture, including fractures secondary to malignancy or infection; (2) patients with neurologic deficit and needing decompression surgery; (3) patients with spinal surgery history; and (4) refractures of augmented vertebrae or new vertebrae fractures during the follow-up period.
According to the inclusion and exclusion criteria, 143 patients who underwent PKP surgery during December 2019 and January 2021 were included. The local kyphosis angle (LKA) change was calculated as the difference between the first postoperative day and the final follow-up. The occurrence of re-kyphosis was defined as more than 10° aggravation in LKA change.8–11 According to this criterion, the included patients were divided into a re-kyphosis group and a non-re-kyphosis group. The location of the fractured vertebrae was classified into the non-thoracolumbar zone (T5–T10 and L3–L5) and thoracolumbar zone (T11–L2).
Surgical Procedure
Patients were placed in the prone position under general anesthesia. Two puncture needles were used to access the fractured vertebral body and establish the working channels. Then, inflatable balloon tamps were placed into the fractured vertebral body to reduce the fracture and correct the local kyphosis. Next, polymethylmethacrylate (PMMA) cement was injected under fluoroscopic guidance, and the total volume of injected cement was recorded. After PKP surgery, calcium, vitamin D3, and bisphosphonates were routinely prescribed for all included patients. Radiological and clinical evaluation were performed preoperatively, on the first postoperative day, and at the final follow-up visit.
Radiological Evaluations
Radiological assessments were independently performed by two senior radiologists through the picture archiving and communication system (PACS).
The LKA was determined by measuring the angle between the superior endplate of the vertebra above the fractured vertebra and the inferior endplate of the vertebrae below the fractured vertebra.12 Vertebral height was measured in lateral radiographs according to the method described by a previous study.9 Vertebral height was calculated as follows: (fractured vertebral height/normal height) × 100%.
LKA correction (LKAC) and vertebral height restoration (VHR) were acquired by calculating the difference between the preoperative LKA and the first postoperative day LKA. The vertebral body wedge angle was measured according to the method described in a previous study.13 The height of the anterior, middle, and posterior intervertebral disc space was measured by a method previously described.14
The shape of the fractured vertebrae on radiographs was observed to determine the fracture type, which was divided into two types: wedge fracture and non-wedge (biconcave or crush) fracture.15 The cement distribution pattern was evaluated on postoperative radiographs as follows: (1) solid lump patterns, and (2) comparatively diffused pattern.16 According to previous literature, disc–endplate complex injury (EDCI) was identified by the presence of endplate edema or fluid collection, cortical discontinuity, or angulation injury, and the presence of disk edema, morphologic alteration, annular tears, or herniation into the endplate.17 If contact was observed between the PMMA bone cement and either the superior or inferior endplate, then PMMA endplate contact (PEC) was recorded; otherwise, non-PMMA endplate contact (NPEC) was recorded.
Clinical Evaluations
Clinical evaluation was performed preoperatively, 1 day postoperatively, and at the final follow-up visit. The assessments included visual analogue scale (VAS) and Oswestry Disability Index (ODI). The VAS score used a scoring system ranging from 0 to 10 and was mounted on a card, with 0 indicating no pain and 10 indicating the maximum pain. The ODI score consists of nine sections of questions (sexual function was excluded) and is used to assess limitations of various daily activities; the ODI score ranges from 0 to 90, with a higher score reflecting greater disability.
Statistical Analysis
SPSS 26.0 software (IBM Corporation, Armonk, NY, USA) was used for analysis. Continuous variables, between groups or within the same group at different time points, were compared using t-test or Mann–Whitney U-test. Categorical variables were assessed using chi-square test. Univariate and multivariate logistic regression analysis were performed to identify related risk factors. p<0.05 was considered to indicate statistically significant differences.
Results
Overall, 143 patients (28 men and 115 women) were included in this study. Sixteen of the 143 patients developed re-kyphosis during follow-up and were classified as the re-kyphosis group (3 men and 13 women, mean age: 69.06±7.79 years). The remaining 127 patients were assigned into the non-re-kyphosis group (25 men and 102 women, mean age: 66.17±8.25 years). The demographic data of all 143 included patients are summarized and presented in Table 1.
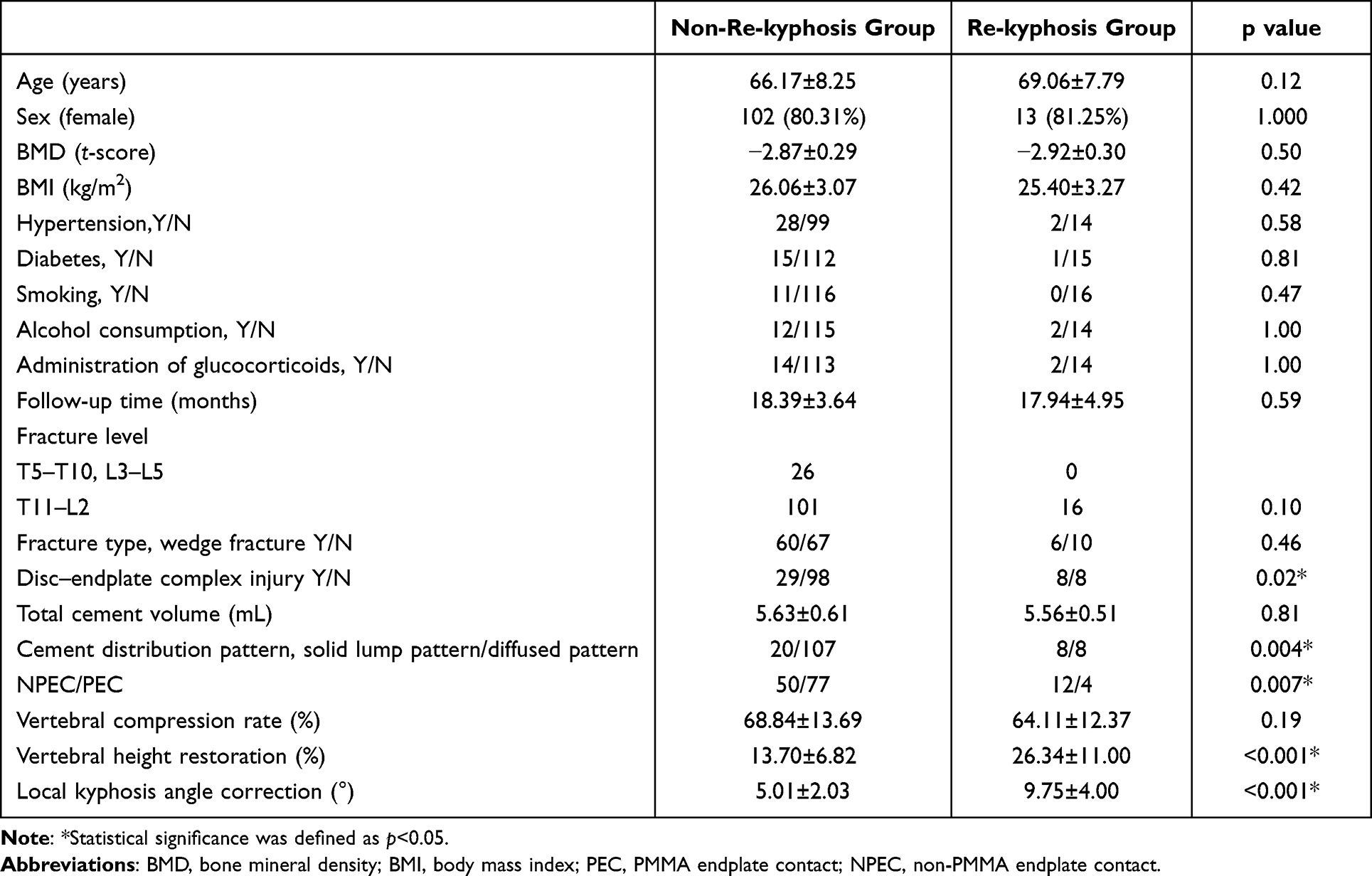 |
Table 1 Characteristics of the Included Patients |
In the re-kyphosis group, the LKA significantly decreased from 19.44±9.79° preoperatively to 11.81±8.60° on the first postoperative day; however, it significantly increased to 25.13±8.91° at the final follow-up visit, which was statistically significant in terms of exacerbation when compared to the LKA of the first postoperative day (Figure 1). In the non-re-kyphosis group, the LKA showed no significant difference between the first postoperative day and the final follow-up (10.12±7.24° vs 11.56±7.18°, p>0.05). The vertebral wedge angles in both groups were significantly decreased postoperatively, and the improvement was maintained until the final follow-up (Figure 1). In the re-kyphosis group, the anterior and middle disc heights significantly decreased at the final follow-up compared to the first postoperative day, but these values did not significantly decrease at the final follow-up in the non-re-kyphosis group. Posterior disc height showed no statistically significant difference at any follow-up time point between the two groups (Figure 1). These results indicated that along with the aggravation of local kyphosis, the disc height collapsed while the vertebral height was maintained at the final follow-up in the re-kyphosis group. Images of the typical case in the re-kyphosis group are shown in Figure 2.
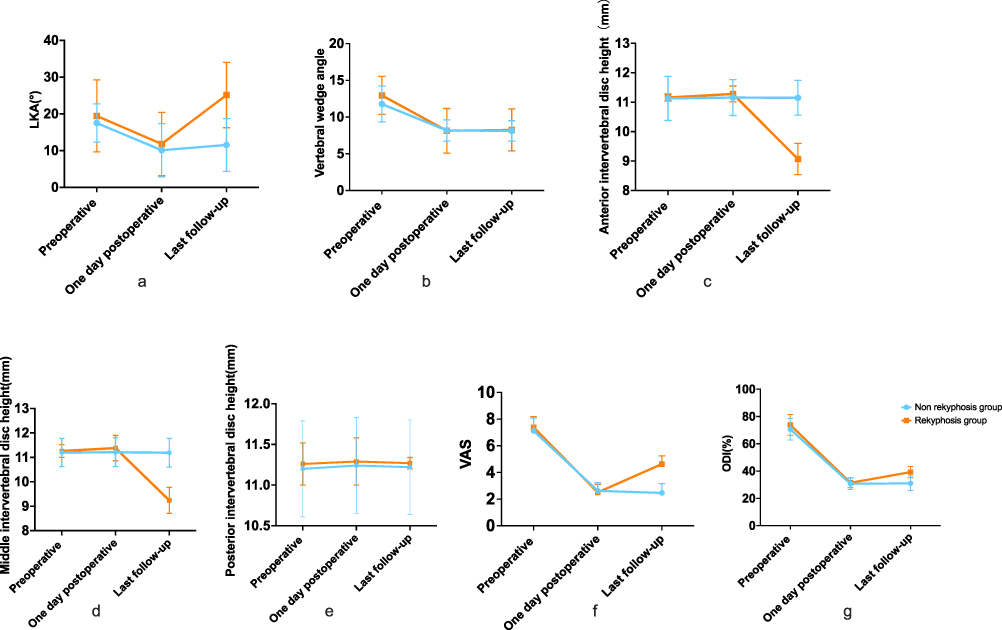 |
Figure 1 Variation trends of radiographic and clinical indices in both the re-kyphosis and non-re-kyphosis group. Line graphs showing the changes in local kyphosis angle (LKA) (a), vertebral wedge angle (b), anterior intervertebral disc height (c), middle intervertebral disc height (d), posterior intervertebral disc height (e), visual analogue scale (VAS) scores (f) and Oswestry Disability Index (ODI) scores (g) of the two groups at three different time points. |
 |
Figure 2 Typical case in the re-kyphosis group. A 67-year-old male patient complained of back pain for 10 days. T1-weighted (a), T2 -weighted (b) and fat-suppressed (c) MRI images showed bone marrow edema signal and disc–endplate complex injury of L1 vertebra(red arrow). Preoperative lateral X-ray image (d) showed multiple degenerative changes of lumbar spine. Lateral X-ray image 1 day after surgery (e) showed the vertebral height was restored and local kyphotic angle was corrected. Lateral X-ray image at the last follow-up (f) showed the occurrence of re-kyphosis. |
The changes in VAS and ODI scores were consistent with the changes of local kyphosis angle (Figure 1). In both the re-kyphosis and non-re-kyphosis groups, the postoperative VAS and ODI scores improved significantly compared to the preoperative scores, indicating that PKP could relieve symptoms and improve daily activity function. However, at the final follow-up in the re-kyphosis group, the VAS and ODI scores worsened compared to the scores of the first postoperative day (p<0.05).
The cement distribution pattern (p=0.004), EDCI (p=0.02), NPEC (p=0.007), VHR (p<0.001), and LKAC (p<0.001) showed statistically significant differences between the two groups (Table 1). Increased solid lump pattern (8/16, 50% vs 20/127, 15.75%), EDCI (8/16, 50% vs 29/127, 22.83%), VHR (26.34±11.00% vs 13.70±6.82%), LKAC (9.75±4.00° vs 5.01±2.03°), and NPEC (12/16, 75.00% vs 50/127, 9.37%) were detected in the re-kyphosis group than the non-re-kyphosis group.
The above-mentioned factors were selected into the final multivariate regression analysis model (Table 2). The results showed that the EDCI (OR=17.46, p=0.003), LKAC (OR=1.84, p<0.001), and VHR (OR=1.15, p=0.003) were positively associated with the recurrence of re-kyphosis after PKP.
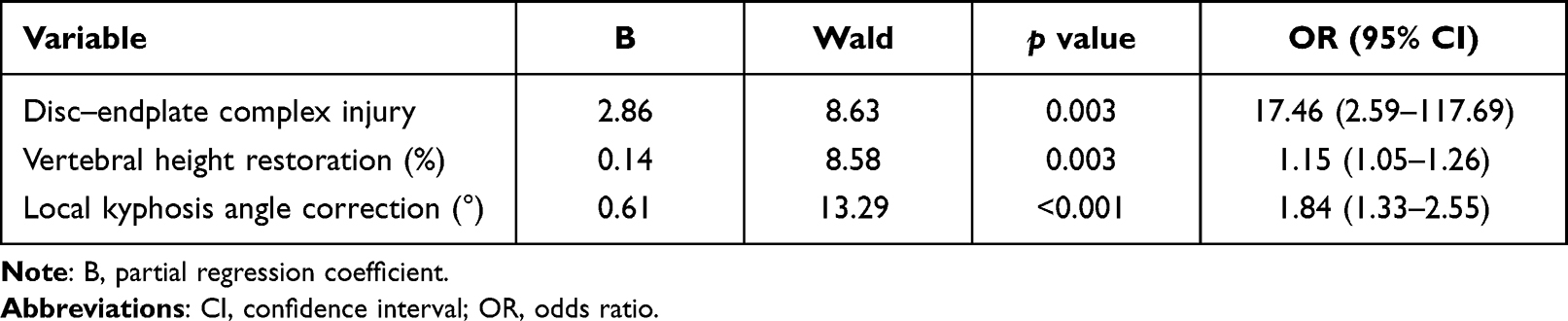 |
Table 2 Multivariate Logistic Regression Analysis |
Discussion
In aging societies, osteoporosis is considered a growing medical and social problem, affecting approximately 30% of the post-menopausal women according to a previous report.18 PKP was considered an appropriate approach for managing OVF, which led to immediate pain relief and stable recovery of fractured vertebrae. With the increasing number of cases, researchers have begun paying more attention to refractures of augmented vertebrae or adjacent new fractures after PKP, which can lead to recurrent refractory pain, compromise patients’ quality of life, and even increase mortality risk.
Studies have demonstrated that spinal kyphosis leads to persistent back pain, decreased lung function, and increased mortality. A crucial advantage of kyphoplasty is the superior efficacy of local kyphosis correction by expandable balloon or posture reduction. However, aggravation of kyphosis after kyphoplasty was observed in several OVF patients, which has rarely been discussed in the literature. The researchers tended to associate re-kyphosis with the refracture of augmented or adjacent segments.19–21 Ha et al reported the presence of thick fibrous tissue around the cement after PKP and considered peri-cement bone resorption as one of the main causes of re-kyphosis after PKP. They believed that the peri-cement bone resorption could cause refracture of the augmented vertebral body, thereby causing re-kyphosis.22 Yang et al reported that the diffusion pattern of bone cement was also regarded as one of the risk factors for recompression of augmented vertebrae, which can lead to local re-kyphosis. Furthermore, the distribution pattern of bone cement could be divided into solid lump pattern and diffused pattern; the solid lump pattern of bone cement indicated no or rare cement spiculation into bone trabeculae, while the hard lump cement could cause compression in the peri-cement bones.23
The endplate-disc complex (EDC) is located between two adjacent vertebral bodies. Recent literature reported that the EDC plays an important role in maintaining the stability of the spine and transferring the axial load.24,25 Injury to the EDC can be easily neglected. Ortiz et al reported that EDCI is often accompanied by OVF in elderly patients; however, most surgeons tend to pay more attention to OVF and neglect EDC.17 The results of our logistic regression analysis showed that EDCI is one of the most important risk factors for re-kyphosis after PKP. A possible explanation is that injury to the EDC may directly accelerate the degenerative process of the intervertebral disc and narrow the intervertebral space, which could be a critical factor to increase local kyphosis. Another possible reason may be the nutrition supply of the intervertebral disc, which mainly relies on the micropore channels located on the endplate. Hence, injury to the endplate may decrease the number of channels and lead to metabolic dysfunction of the disc.26 Furthermore, the cement augmentation reduce the deformation of augmented endplate, increasing the pressure of adjacent intervertebral disc and ultimately resulting in disc degeneration, which may also be related to recurrent local kyphosis.
Vertebral body restoration and LKAC were also identified as risk factors related to re-kyphosis after PKP. Increased restoration of the vertebral height and LKA may decrease the density of the local bony trabeculae within the augmented vertebrae and lead to recompression susceptibility of local bone trabeculae in non-cement augmented areas.27 However, in the re-kyphosis group, the augmented vertebral wedge angle at the final follow-up presented no statistical difference when compared to the postoperative angle (p>0.05), suggesting that the re-kyphosis may not be associated with recompression of local trabeculae. Therefore, we proposed that restoration of vertebral height and LKA may increase the tension of surrounding soft tissue, thereby increasing the mechanical loading of intervertebral discs adjacent to the augmented vertebrae, further accelerating the disc degeneration process, and finally increasing the LKA.
The changing trends of VAS and ODI scores presented a similar pattern, with both the non-re-kyphosis group and re-kyphosis group exhibiting significant pain relief and functional improvement after PKP. However, at the final follow-up, the VAS and ODI scores in the re-kyphosis group deteriorated when compared to the non-re-kyphosis group. These results show that re-kyphosis should not be neglected, as the symptoms seem to progress gradually during follow-up. We speculate that the changed sagittal balance after occurrence of re-kyphosis may be the reason for the aggravated symptoms after PKP surgery. Further studies should be performed to elucidate the relationship between changed sagittal balance and aggravated symptoms in re-kyphosis patients.
There were several limitations in this study. First, postoperative MRI was not a routine examination in this study, so the Pifrrmann grading system could not be used to evaluate the degree of intervertebral disc degeneration and its relationship with the aggravation of local kyphosis in included patients. Second, in this study, the reason of the aggravated symptoms after the occurrence of re-kyphosis remained unclear and needed to elucidate in further studies. Third, the follow-up time of this study was relatively short and the sample size was relatively small. Further studies are still needed to explore the risk factors and the clinical significance of re-kyphosis after PKP surgery.
Conclusion
The recurrent local kyphosis after PKP is not rare in OVF patients without refractures of augmented or adjacent segments. The clinical symptoms deteriorate during follow-up in patients with the recurrent local kyphosis which indicate that re-kyphosis tends to lead to a poor prognosis after PKP surgery and should be taken seriously. Patients with disc–endplate complex injury, more correction of vertebral height and kyphosis angle are at a higher risk for re-kyphosis after PKP surgery.
Abbreviations
OVF, osteoporotic vertebral fracture; PKP, percutaneous kyphoplasty; LKA, local kyphosis angle; LKAC, local kyphotic angle correlation; PEC, PMMA endplate contact; NPEC, non-PMMA endplate contact; VHR, vertebral height restoration; VAS, visual analogue Scale; ODI, Oswestry Disability Index; EDCI, endplate–disc complex injury.
Data Sharing Statement
The data that support the results of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent for Publication
This study was approved by the institutional ethics committee of First Affiliated Hospital of Soochow University (Ethics Number: 2023021). Informed consent was obtained from all participants enrolled in this study. We certify that the study was performed in accordance with the declaration of Helsinki. All authors agree with the version of the manuscript submitted for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Du J, Li X, Lin X. Kyphoplasty versus vertebroplasty in the treatment of painful osteoporotic vertebral compression fractures: two-year follow-up in a prospective controlled study. Acta Orthop Belg. 2014;80(4):477–486.
2. Wang B, Zhao CP, Song LX, Zhu L. Balloon kyphoplasty versus percutaneous vertebroplasty for osteoporotic vertebral compression fracture: a meta-analysis and systematic review. J Orthop Surg Res. 2018;13(1):264. doi:10.1186/s13018-018-0952-5
3. Farrokhi MR, Alibai E, Maghami Z. Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J Neurosurg Spine. 2011;14(5):561–569. doi:10.3171/2010.12.Spine10286
4. Pflugmacher R, Schroeder RJ, Klostermann CK. Incidence of adjacent vertebral fractures in patients treated with balloon kyphoplasty: two years’ prospective follow-up. Acta Radiol. 2006;47(8):830–840. doi:10.1080/02841850600854928
5. Shi C, Zhang M, Cheng AY, Huang ZF. Percutaneous kyphoplasty combined with zoledronic acid infusion in the treatment of osteoporotic thoracolumbar fractures in the elderly. Clin Interv Aging. 2018;13:853–861. doi:10.2147/cia.S146871
6. Lombardi I, Oliveira LM, Mayer AF, Jardim JR, Natour J. Evaluation of pulmonary function and quality of life in women with osteoporosis. Osteoporos Int. 2005;16(10):1247–1253. doi:10.1007/s00198-005-1834-3
7. Silverman SL. The clinical consequences of vertebral compression fracture. Bone. 1992;13(Suppl 2):S27–231. doi:10.1016/8756-3282(92)90193-z
8. Chou KN, Lin BJ, Wu YC, Liu MY, Hueng DY. Progressive kyphosis after vertebroplasty in osteoporotic vertebral compression fracture. Spine. 2014;39(1):68–73. doi:10.1097/brs.0000000000000042
9. Kanezaki S, Miyazaki M, Ishihara T, Notani N, Tsumura H. Magnetic resonance imaging evaluation of intervertebral disc injuries can predict kyphotic deformity after posterior fixation of unstable thoracolumbar spine injuries. Medicine. 2018;97(28):e11442. doi:10.1097/md.0000000000011442
10. Oner FC, van Gils AP, Faber JA, Dhert WJ, Verbout AJ. Some complications of common treatment schemes of thoracolumbar spine fractures can be predicted with magnetic resonance imaging: prospective study of 53 patients with 71 fractures. Spine. 2002;27(6):629–636. doi:10.1097/00007632-200203150-00012
11. Seo DK, Kim CH, Jung SK, Kim MK, Choi SJ, Park JH. Analysis of the risk factors for unfavorable radiologic outcomes after fusion surgery in thoracolumbar burst fracture: what amount of postoperative thoracolumbar kyphosis correction is reasonable? J Korean Neurosurg Soc. 2019;62(1):96–105. doi:10.3340/jkns.2017.0214
12. Grelat M, Madkouri R, Comby PO, Fahed E, Lemogne B, Thouant P. Mid-term clinical and radiological outcomes after kyphoplasty in the treatment of thoracolumbar traumatic vertebral compression fractures. World Neurosurg. 2018;115:e386–e392. doi:10.1016/j.wneu.2018.04.060
13. Ohyama S, Hoshino M, Takahashi S, et al. Presence of sarcopenia does not affect the clinical results of balloon kyphoplasty for acute osteoporotic vertebral fracture. Sci Rep. 2021;11(1):122. doi:10.1038/s41598-020-80129-z
14. Zhao C, Zhang H, Wang Y, et al. Nomograms for predicting recurrent herniation in PETD with preoperative radiological factors. J Pain Res. 2021;14:2095–2109. doi:10.2147/jpr.S312224
15. De Kong L, Meng LC, Shen Y, Wang LF, Wang P, Shang ZK. Effect of shape and severity of vertebral fractures on the outcomes of kyphoplasty. Acta Orthop Belg. 2013;79(5):565–571.
16. Yu W, Liang D, Yao Z, et al. Risk factors for recollapse of the augmented vertebrae after percutaneous vertebroplasty for osteoporotic vertebral fractures with intravertebral vacuum cleft. Medicine. 2017;96(2):e5675–e5675. doi:10.1097/MD.0000000000005675
17. Ortiz AO, Bordia R. Injury to the vertebral endplate-disk complex associated with osteoporotic vertebral compression fractures. Am J Neuroradiol. 2011;32(1):115–120. doi:10.3174/ajnr.A2223
18. Melton LJ, Chrischilles EA, Cooper C, Lane AW, Riggs BL. Perspective. How many women have osteoporosis? J Bone Miner Res. 1992;7(9):1005–1010. doi:10.1002/jbmr.5650070902
19. Huang D, Ying J, Xu D, et al. Comparison of percutaneous kyphoplasty with or without pedicle screw fixation in osteoporotic thoracolumbar vertebral fractures: a retrospective study. Dis Markers. 2021;2021:4745853. doi:10.1155/2021/4745853
20. Zhao C, Liu X, Wang Y, et al. The effects of biomechanical factors on adjacent vertebral compression fractures after percutaneous kyphoplasty: a propensity score matching analysis. Osteoporos Int. 2022;33(8):1795–1806. doi:10.1007/s00198-022-06428-5
21. Zhu J, Zhang K, Luo K, et al. Mineralized collagen modified polymethyl methacrylate bone cement for osteoporotic compression vertebral fracture at 1-year follow-up. Spine. 2019;44(12):827–838. doi:10.1097/brs.0000000000002971
22. Ha KY, Kim KW, Kim YH, Oh IS, Park SW. Revision surgery after vertebroplasty or kyphoplasty. Clin Orthop Surg. 2010;2(4):203–208. doi:10.4055/cios.2010.2.4.203
23. Yang SC, Chen WJ, Yu SW, Tu YK, Kao YH, Chung KC. Revision strategies for complications and failure of vertebroplasties. Eur Spine J. 2008;17(7):982–988. doi:10.1007/s00586-008-0680-3
24. Chen WJ, Kao YH, Yang SC, Yu SW, Tu YK, Chung KC. Impact of cement leakage into disks on the development of adjacent vertebral compression fractures. J Spinal Disord Tech. 2010;23(1):35–39. doi:10.1097/BSD.0b013e3181981843
25. Fujiwara T, Akeda K, Yamada J, Kondo T, Sudo A. Endplate and intervertebral disc injuries in acute and single level osteoporotic vertebral fractures: is there any association with the process of bone healing? BMC Musculoskelet Disord. 2019;20(1):336. doi:10.1186/s12891-019-2719-5
26. Che YJ, Guo JB, Liang T, et al. Assessment of changes in the micro-nano environment of intervertebral disc degeneration based on Pfirrmann grade. Spine J. 2019;19(7):1242–1253. doi:10.1016/j.spinee.2019.01.008
27. Lin WC, Lee YC, Lee CH, et al. Refractures in cemented vertebrae after percutaneous vertebroplasty: a retrospective analysis. Eur Spine J. 2008;17(4):592–599. doi:10.1007/s00586-007-0564-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.