")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Recovery of a 10-year-old girl from methicillin-resistant Staphylococcus aureus sepsis in response to low-dose ceftaroline treatment
Authors Borgmann S, Rieß B, von Wernitz-Keibel T, Matthias Buehler M, Layer F, Strommenger B
Received 6 November 2015
Accepted for publication 29 January 2016
Published 11 May 2016 Volume 2016:12 Pages 749—753
DOI https://doi.org/10.2147/TCRM.S99987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Video abstract presented by Borgmann et al.
Views: 1626
Stefan Borgmann,1 Beate Rieß,1 Thomas von Wernitz-Keibel,2 Matthias Bühler,3 Franziska Layer,4 Birgit Strommenger4
1Department of Infectious Diseases and Infection Control, 2Department of Anaesthesiology and Intensive Care Medicine, 3Department of Trauma Surgery, Klinikum Ingolstadt, Ingolstadt, 4National Reference Centre for Staphylococci and Enterococci, Division Nosocomial Pathogens and Antibiotic Resistances, Department for Infectious Diseases, Robert Koch Institute, Wernigerode Branch, Wernigerode, Germany
Abstract: A 9-year-old girl was severely injured in a car accident in Afghanistan, in which both her lower legs were badly damaged. She was treated at the Hospital of Ingolstadt (Klinikum Ingolstadt) after she had undergone initial surgery at an Indian hospital. Various bacterial species were isolated from multiple wounds, and methicillin-resistant Staphylococcus aureus (MRSA) was one among them. After the amputation of her lower legs, she developed MRSA sepsis, which was successfully treated with a relatively low dosage of ceftaroline (Zinforo®/Teflaro®; 2×9 mg/kg/d), although the bacterial isolate’s minimal inhibitory concentration (1.5–4 mg/L) suggested a decreased susceptibility. In summary, ceftaroline was highly efficient and well tolerated by the patient suffering from MRSA sepsis.
Keywords: side effects, susceptibility, ceftaroline, minimal inhibitory concentration, therapy
Case report
In August 2013, a 9-year-old Afghan girl, who had been severely injured in a car accident in early 2013, was admitted to a teaching hospital in southeast Germany (Bavaria). Before her transfer to Germany, she had undergone surgery at an Indian hospital. Her left leg had been stabilized with an external fixation, which was later substituted by a femur nail.
On admission, her general condition dramatically deteriorated. She was dehydrated and undernourished (130 cm height, 25 kg body weight) as indicated by decreased serum concentration of total protein (42.3 mg/dL [normal range 66.0–83.0 mg/dL]) and creatinine (0.3 mg/dL [0.6–0.9 mg/dL]). She also suffered from anemia and several decubitus dorsal ulcers (stage 2 and 3). Both legs showed multiple wounds with extended areas of scab which secreted large amounts of yellow pus. Pus was also secreted from a fistula of her left hip joint.
Various bacteria species exhibiting extensive antibiotic resistances were isolated from swabs of the patients wounds: methicillin resistant Staphylococcus aureus (MRSA); carbapenem resistant Pseudomonas aeruginosa; and several Gram negative bacteria species with extended spectrum beta-lactamase activity (ESBL); Citrobacter sedlakii; Escherichia coli; Proteus mirabilis; Klebsiella pneumoniae. Furthermore, methicillin susceptible S. aureus, P. mirabilis (non ESBL), Enterococcus faecalis, Enterococcus hirae, Bacteroides fragilis, and peptostreptococci were identified. Bacterial identification and antibiotic susceptibility testing was performed as recently described.1
After 2 weeks of initial treatment at the intensive care unit, the patient was admitted to the pediatric surgery ward as her general condition had significantly improved. Until June 2014, she underwent 16 surgeries and approximately 60 dressing changes, each requiring general anesthetics. During her stay, she received the following antibiotics in dosages adapted to her body weight: cefazoline (1 g two times per day; 2×1 g/d), imipenem (4×0.5 g/d), meropenem (3×400 mg/d), ampicillin (3×400 mg/d) + clindamycin (3×150 mg/d) intravenously, amoxicillin (3×400 mg/d) + clindamycin (3×150 mg/d) orally, ceftazidime (3×1 g/d), ceftaroline (Zinforo® [AstraZeneca, London, UK]/Teflaro® [Allergan, Dublin, Ireland]; 2×225 mg/d), and cefuroxime (2×250 mg/d) (Figure 1A).
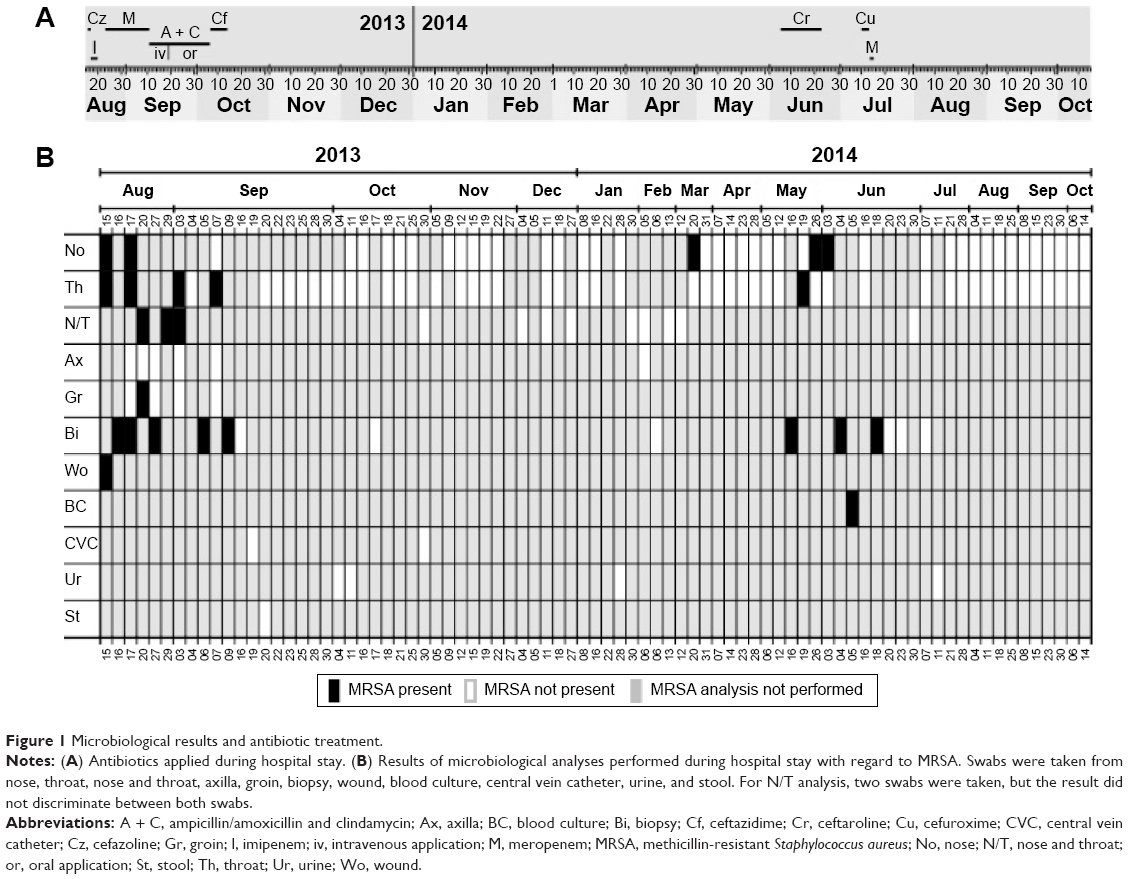 | Figure 1 Microbiological results and antibiotic treatment. |
MRSA was frequently isolated from various body sites within the first 3 weeks after admission (Figure 1B). Following two decolonization cycle, MRSA was not found in several swabs taken from the nose and throat nor isolated from the biopsy specimen taken from September 16, 2013 to March 20, 2014. There was no further proof of MRSA over this time, except for a nose swab taken on March 20, 2014, leading to decolonization measures for seven additional days.
On May 16, 2014, MRSA was found in a biopsy sample and it was also found afterwards in swabs taken from the nose and throat. On June 3, 2014, the patient underwent amputation of her lower legs (knee disarticulation) and MRSA was detected in a biopsy of the infected limb. After surgery, the patient was treated for 9 days in the intensive care unit due to a deterioration in her general condition. As shown in Figure 2, systemic inflammatory response syndrome was present, as indicated by an increased heart rate (140/bpm), white blood cell count (>24,200/mm3), and decreased blood pressure (systolic arterial pressure 80–100 mmHg).2 Body temperature rose to 40.3°C and C-reactive protein concentration increased to 265.5 mg/L. MRSA was found in a blood culture, indicating septic infection.
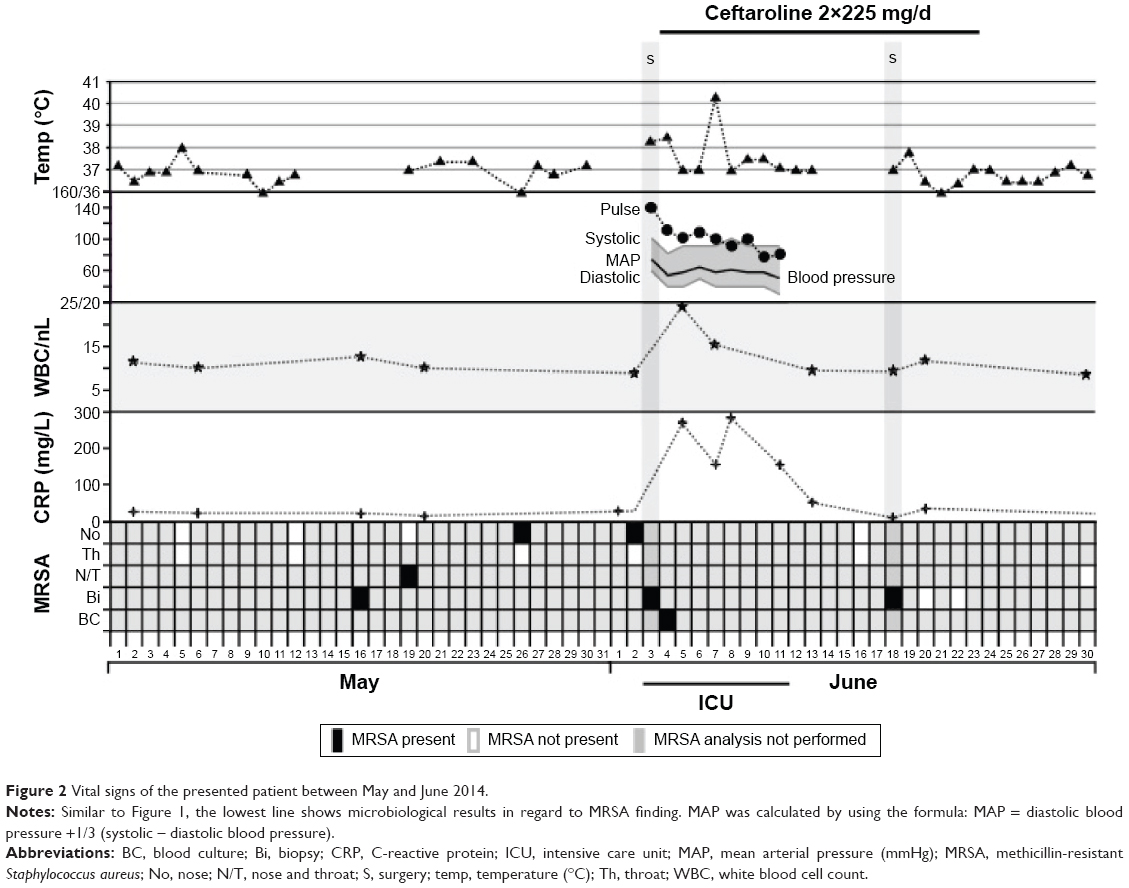 | Figure 2 Vital signs of the presented patient between May and June 2014. |
In the following days, antibiotic treatment with ceftaroline (2×225 mg/d) led to a continuous improvement of her general condition. On June 18, 2014, she underwent a final revision surgery of her right thigh wound, including removal of the condylar cartilage and debridement of necrotic tissue. Although MRSA was detected in a biopsy specimen removed during this surgery, there was no increase of inflammation parameters nor was the circulation impaired. Ceftaroline application was stopped after a treatment period of 19 days. No further MRSA was found in any of the swabs taken from the nose and throat and she was discharged from the hospital in October 2014.
Typing of two MRSA isolates was performed by the National Reference Centre for Staphylococci and Enterococci at the Robert Koch Institute, Wernigerode, Germany and the results are summarized in Table 1. Informed consent was given by the patients legal representative. Ethics approval was not deemed necessary by the Institutional Review Board of Klinikum Ingolstadt as only standard treatment procedures were carried out and no additional samples were taken for scientific purposes.
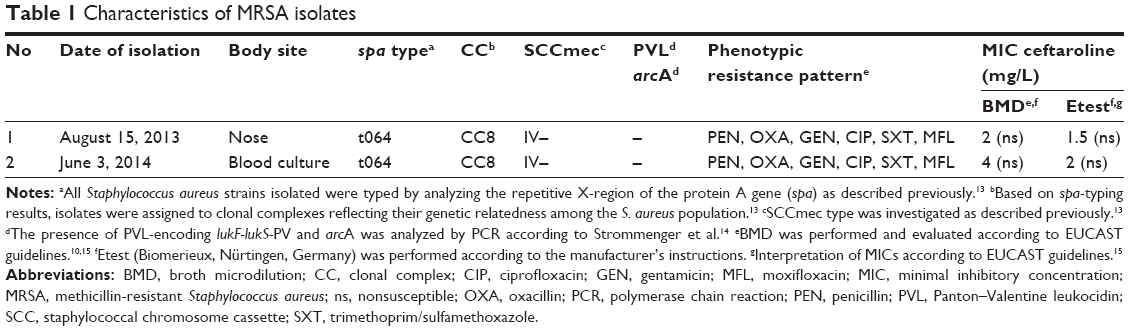 | Table 1 Characteristics of MRSA isolates |
Discussion
In this report, we present a young patient with severe infection of both legs, caused by a multitude of (multiresistant) bacteria. Bacteriologic analyses intermittently revealed the presence of MRSA, and after amputation surgery, the patient developed sepsis caused by this particular bacterial species. Typing results indicated an endogenous MRSA infection, although screening results had suggested successful prior MRSA decolonization. Screening and decolonization of S. aureus in orthopedic patients is an effective measure to prevent endogenous infection and subsequent bacteremia.3 However, in this case, it is questionable whether decolonization measures proved efficient, due to the underlying conditions of the patient. Moreover, the screening results presented demonstrate the risk of MRSA recolonization in high-risk patients, which underlines the importance of continuous MRSA monitoring.
The infection was successfully treated with ceftaroline. This antibiotic was chosen because a greater efficiency in comparison to vancomycin and linezolid was anticipated. Despite the promising reports on the use of daptomycin in pediatric patients, we forewent usage of this drug due to limited treatment experiences in children at our hospital.4
Since ceftaroline is not approved for use in children, information about appropriate ceftaroline dosage, safety, and efficacy in children is scarce.5,6 A study examining the safety of 3×12 mg/kg/d ceftaroline for pediatric patients of <33 kg body weight has recently been completed, but its results have not been published yet.7 In a recent case report on ceftaroline treatment of MRSA pneumonia in a 6-year-old boy, a comparable initial dose of 2×9.7 mg/kg/d had been applied. During the course of treatment, the dosage was increased to 3×10.8 mg/kg/d and it did not produce any side effects.8
With respect to body weight and the general condition of the patient described herein, initial therapy was started with a relatively low dosage (2×9 mg/kg/d).9 As the postoperative course was satisfactory, the low-dose treatment was continued.
Within 4 days of treatment, the patient’s circulation stabilized and body temperature decreased, while C-reactive protein concentration and white blood cell count remained increased for another week, which was probably due to the extended wounds on her thighs. The patient’s temperature rose once again to 40.3°C, probably caused by dissemination of bacteria from the remaining infected tissue into circulation. After a final revision surgery, inflammation parameters remained low.
In vitro analysis displayed an increased minimal inhibitory concentration (MIC) of 1.5–4 mg/L for MRSA from blood culture, suggesting reduced antibiotic susceptibility to ceftaroline. Reduced preuse susceptibility to ceftaroline has been reported worldwide, predominantly in MRSA belonging to certain clonal lineages (ST228 and ST239).10 The strains isolated in this case belong to a different clonal lineage (CC8); however, their isolation demonstrates that ceftaroline resistance might occur in MRSA in general.
Increased ceftaroline MICs reported in literature remain relatively low (1.5–4 mg/L) and it is not yet clear whether these MICs influence treatment efficiency. Therefore, changing the susceptibility interpretive criteria to an MIC of ≤2.0 mg/L was suggested recently based on pharmacokinetic and pharmacodynamic in vitro analyses.11 However, due to diagnostic challenges in susceptibility testing, ceftaroline MIC of 1.0 mg/L remains an important and conservative breakpoint to sensitize clinicians for putative treatment failure and to preserve ceftaroline as a potent antibiotic for serious infections caused by broadly resistant MRSA.10,12
Disclosure
SB received speaker’s honorarium from AstraZeneca. The authors report no other conflicts of interest in this work.
References
Steger S, Demetz F, Schmidt C, Borgmann S. Low percentage of asylum seekers colonized with multi-resistant bacteria treated at a German hospital. J J Epidemiol Prevent. 2016;1(2):21. | ||
Goldstein B, Giroir B, Randolph A; International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. | ||
Chen AF, Wessel CB, Rao N. Staphylococcus aureus screening and decolonization in orthopaedic surgery and reduction of surgical site infections. Clin Orthop Relat Res. 2013;471(7):2383–2399. | ||
Principi N, Caironi M, Venturini F, Pani L, Esposito S. Daptomycin in paediatrics: current knowledge and the need for future research. J Antimicrob Chemother. 2015;70(3):643–648. | ||
Gostelow M, Gonzalez D, Smith PB, Cohen-Wolkowiez M. Pharmacokinetics and safety of recently approved drugs used to treat methicillin-resistant Staphylococcus aureus infections in infants, children and adults. Expert Rev Clin Pharmacol. 2014;7(3):327–340. | ||
Mpenge MA, MacGowan AP. Ceftaroline in the management of complicated skin and soft tissue infections and community acquired pneumonia. Ther Clin Risk Manag. 2015;11:565–579. | ||
Forest Laboratories. Safety and efficacy study of ceftaroline versus a comparator in pediatric subjects with community acquired bacterial pneumonia (CABP) [updated January 12, 2015]. Available from: https://clinicaltrials.gov/ct2/show/NCT01530763/. ClinicalTrials.gov Identifier: NCT01530763. Accessed August 11, 2015. | ||
Molloy L, Snyder AH, Srivastava R, Rybak MJ, McGrath E. Ceftaroline fosamil for methicillin-resistant Staphylococcus aureus pulmonary exacerbation in a pediatric cystic fibrosis patient. J Pediatr Pharmacol Ther. 2014;19(2):135–140. | ||
Jain R, Chan JD, Rogers L, Dellit TH, Lynch JB, Pottinger PS. High incidence of discontinuations due to adverse events in patients treated with ceftaroline. Pharmacotherapy. 2014;34(7):758–763. | ||
Strommenger B, Layer F, Klare I, Werner G. Pre-use susceptibility to ceftaroline in clinical Staphylococcus aureus isolates from Germany: Is there a non-susceptible pool to be selected? PLoS One. 2015;10(5): e0125864. | ||
Van Wart SA, Ambrose PG, Rubino CM, et al. Pharmacokinetic-pharmacodynamic target attainment analyses to evaluate in vitro susceptibility test interpretive criteria for ceftaroline against Staphylococcus aureus and Streptococcus pneumoniae. Antimicrob Agents Chemother. 2014;58(2):885–891. | ||
Livermore DM, Mushtaq S, Warner M, James D, Woodford N. Susceptibility testing challenges with ceftaroline, MRSA and a 1 mg/L breakpoint. J Antimicrob Chemother. 2015;70(12):3259–3266. | ||
Strommenger B, Braulke C, Heuck D, et al. spa Typing of Staphylococcus aureus as a frontline tool in epidemiological typing. J Clin Microbiol. 2008;46(2):574–581. | ||
Strommenger B, Braulke C, Pasemann B, Schmidt C, Witte W. Multiplex PCR for rapid detection of Staphylococcus aureus isolates suspected to represent community-acquired strains. J Clin Microbiol. 2008;46(2):582–587. | ||
EUCAST: The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 5.0; 2015 [updated January 26, 2015]. Available from: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_5.0_Breakpoint_Table_01.pdf. Accessed August 11, 2015. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.