")
Back to Journals » International Journal of Women's Health » Volume 10
Reconstruction of feminine identity: the strategies of women with breast cancer to cope with body image altered
Authors Zeighami Mohammadi S , Mohammad Khan Kermanshahi S , Vanaki Z
Received 26 July 2018
Accepted for publication 12 October 2018
Published 1 November 2018 Volume 2018:10 Pages 689—697
DOI https://doi.org/10.2147/IJWH.S181557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Sharareh Zeighami Mohammadi, Sima Mohammad Khan Kermanshahi, Zohreh Vanaki
Department of Nursing, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
Background: Body image altered is the most important psychosocial concern associated with breast cancer. Yet, there is a paucity of information regarding strategies for coping with this problem. This study aimed to explore Iranian breast cancer women’s strategies for coping with body image altered.
Methods: This qualitative study was conducted in 2016–2017. A purposive sample of 36 women with breast cancer was selected with maximum variation from three health care centers in Alborz Province, Iran. Data were collected by semi-structured interviews and analyzed by performing conventional qualitative content analysis.
Results: The main theme of the study was “reconstruction of feminine identity” with the six main categories of physical appearance improvement, active information seeking, self-care for managing limits, psychological self-empowerment, maintaining maternal role, and maintaining wife role.
Conclusion: Iranian breast cancer women’s strategies for coping with body image altered are multidimensional and are mainly based on personal resources. Breast cancer women use these strategies to reconstruction of their feminine identity. Health policy-makers can use the findings of the present study to develop interventions and programs for improving breast cancer women’s body image care.
Keywords: breast cancer, body image altered, coping, feminine identity, qualitative study
Introduction
Breast cancer (BC) is the most common malignancy among women in the world.1 The prevalence and the mortality rates of BC are progressively increasing. A study in Iran showed that from 1990 to 2010, these rates increased from 16 and 0.96 to 28.3 and 4.33 cases per 1,000 women, respectively.2 Increases in prevalence and decreases in onset age have turned BC into a major health problem in Iran.3
Body image altered is one of the most important psychological problems experienced by BC women.4 Body image is a subjective concept which includes perceptions, thoughts, and feelings each individual has about his/her body, appearance, sexuality, health status, wholeness, and physical functioning.5 BC and its treatments are associated with body image altered, sense of wholeness, sexual attractiveness, femininity, and satisfaction with body functioning and role performance.4–7 For instance, factors such as weight changes, surgical wounds and scars, and BC treatment side effects (chiefly nausea, fatigue, hormonal alterations, alopecia, and mastectomy) significantly contribute to BC women’s sexual dysfunction.8–10 Sexual dysfunction, in turn, threatens their sexual and marital lives.6 Moreover, psychological problems, fatigue, physical weakness, and lymphedema prevent women from effectively performing their wife, maternal, and household roles.6,10 Such ineffective role performance negatively affects women’s feminine identity, sense of worthiness, self-esteem, self-confidence, and body image.4,10–12 Besides, social stigmatization due to alopecia and mastectomy reduces BC women’s social interactions and results in their social isolation.7,13,14
Alterations in body image and changes in feminine identity are among the most principal concerns of women with BC.4,10–15 These problems are associated with low quality of life and ineffective coping with BC.10,15 Thus, BC women use different strategies to cope with body image altered.16 These strategies include breast reconstruction,13 concealment of physical defects,17,18 restriction of sexual relationships,8 deliberate social isolation,4,6 lifestyle modifications,19 and balancing of personal life and maternal role.10
Strategies women use for coping with body image altered greatly depend on their sociocultural context. Consistently, a study reported that sociocultural norms and beliefs significantly determine psycho-behavioral responses such as the selection and the use of coping strategies.20 For instance, the beauty of the body is among the most principal feminine values in Western culture,6 while in Islamic culture, modesty and chastity are more valuable and important for woman than physical beauty and attractiveness.20 Moreover, in the Iranian culture, wife and maternal role significantly contribute to women’s identity.10,20 In addition, Iranian women feel great commitment to fulfill their husbands’ sexual needs in order to protect their families21 and therefore attach great value to their patience for their probable sexual problems.22
Because of cultural differences between Western and Islamic cultures, the findings of studies into the coping strategies used by BC women in Western countries are not generalizable to Iranian BC women. Nonetheless, previous studies in Iran have provided limited information, if any, about BC women’s coping strategies for body image altered. This study sought to narrow this gap. The aim of the study was to explore strategies for coping with body image altered among Iranian BC women.
Methods
This qualitative study was conducted in 2016–2017 based on the naturalistic paradigm.
Participants included 36 Iranian BC women who were purposively recruited from Alborz Clinic, Rajaei Hospital, and Hashtgerd Hospital in Alborz Province, Iran. Selection criteria were providing written informed consent for participation and ability to verbally communicate in Persian. Sampling was performed with maximum variation in order to access different experiences and promote transferability of the findings. Sampling was ended after reaching data saturation. Table 1 shows participants’ characteristics.
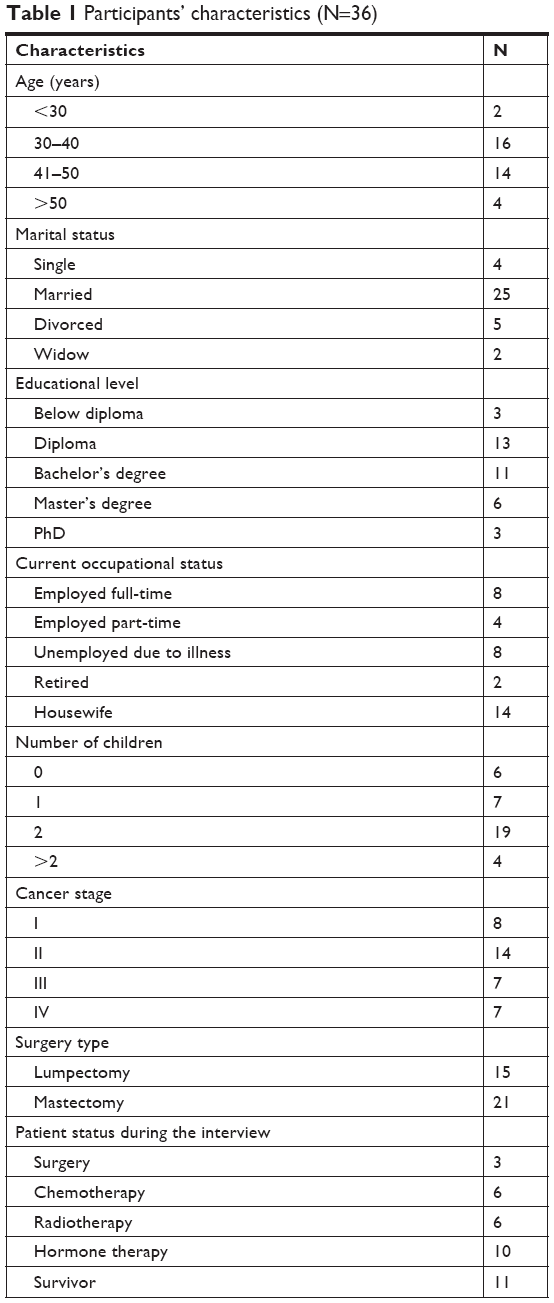 | Table 1 Participants’ characteristics (N=36) |
Data gathering
The first author collected data from March 2016 to October 2017 through 46 in-depth semi-structured interviews. Each interview was started using the following broad questions: “What are changes about your body since your cancer treatments?” Throughout interviews, pointed and probing questions were asked to collect more in-depth data. These questions included, “How do you manage this change in your body?”, “What actions did you take?”, “Can you explain it more?”, “Can you provide an example about this?”, “Do you want to add anything else?” Interviews were conducted in a private calm environment and recorded using a sound recorder application on a smart phone. After 43 interviews, we did not obtain any new data, denoting the saturation of the data. Yet, three more interviews were conducted to ensure data saturation. The duration of each interview depended on the interviewee’s preferences and was 50 minutes, on average, with the range of 30–120 minutes. After each interview, the Microsoft Office Word was employed to type the interview content word by word together with the interviewee’s nonverbal signals during the interview (such as sigh, silence, cry, or laugh).
Data analysis
Data were analyzed concurrently with data collection based on the content analysis approach proposed by Graneheim and Lundman. The unit of analysis was each whole interview. Each interview transcript was reviewed several times in order to grasp its main ideas. Then, meaning units were identified and labeled with primary codes. Simultaneously, the codes were sorted into larger categories, and finally, the main theme of the study was generated.23
Trustworthiness
The rigor of the study was maintained via the criteria proposed by Lincoln and Guba (1994). Our prolonged engagement with the data added to the depth of the data and ensured the credibility. Three interview transcripts with codes and categories were returned to the same patients who reviewed and confirmed. During the regular meetings of the research team, codes and categories were confirmed and agreed upon by the second and the third authors in order to confirm ability. External peer check approved the accuracy of data analysis. Maximum variation sampling promotes the transferability.24
Ethical considerations
The present study obtained ethical approval from the Ethics Committee of Tarbiat Modares University, Tehran, Iran (approval code: 52D8050). Before inclusion in the study, eligible participants were provided with detailed information about the study, its advantages and disadvantages, data collection methods, confidential data management, their role in the study, and their right to unilaterally withdraw from the study. Afterward, verbal and written consents for participation were obtained from each of them. This study was conducted in accordance with the Declaration of Helsinki.
Findings
In total, 36 BC women with a mean age of 24–64 years were studied. Their strategies for coping with BC-related body image altered were sorted into 21 subcategories and the six main categories of physical appearance improvement, active information seeking, self-care for managing limits, psychological self-empowerment, maintaining maternal role, and maintaining wife role. These subcategories and categories came under the main theme of “reconstruction of feminine identity” (Table 2).
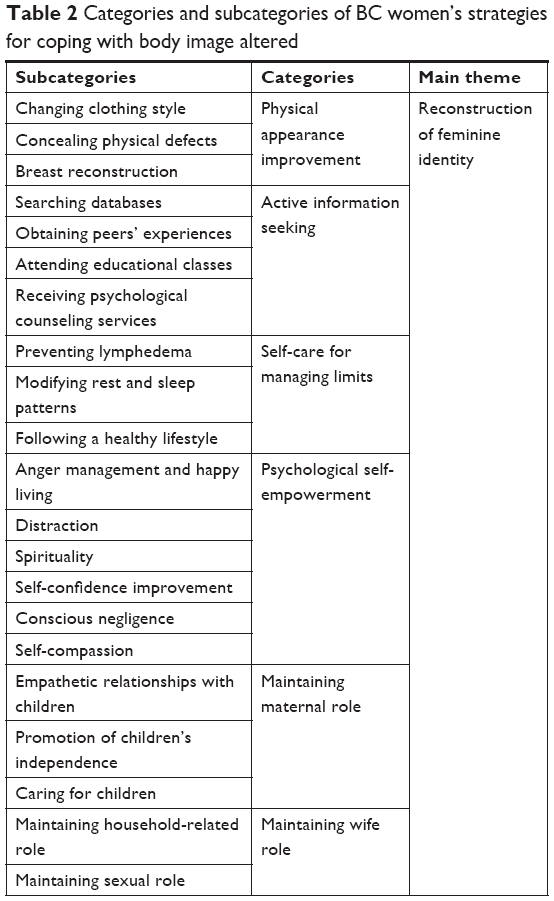 | Table 2 Categories and subcategories of BC women’s strategies for coping with body image altered |
Physical appearance improvement
Participants attempted to improve their physical appearance in order to win social acceptance. One of their strategies for such improvement was to change their clothing style to conceal their physical defects. For instance, they wore long-sleeve, loose-fitting, or high-necked dresses or used cupped swimsuit in pools in order to conceal their lymphedema, deformities, or breast absence. In addition, they filled the empty space in their brassiere with pieces of towel, cotton, or prosthesis or wore padded brassiere in order to conceal breast absence or breast size asymmetry.
Previously, I frequently colored my hair with different dyes and used different clothing styles. But, since hair loss, I started to use Islamic veil. I even wear scarf if I have hairpiece. [P15]
They also attempted to use some tricks to conceal chemotherapy-induced changes in their physical appearance such as alopecia or yellow or pale face. For instance, they used thick makeup to conceal their pallor or used full-head scarf, hairpiece, knitted hat, false eyelash, or tattoo to repair their alopecia.
Before chemotherapy, I tattooed my eyelashes and eyebrows. [P26]
Breast reconstruction was another strategy for improving their physical appearance. Their main motives for breast reconstruction were to regain their feminine identity, protect their sexual relationships, restore their physical attractiveness, and have a normal appearance in front of their children.
I want to undergo breast reconstruction because I greatly value my appearance and like to be a complete woman. A woman is more beautiful and natural with breasts. [P12]
Active information seeking
Participants actively sought for information about healthy lifestyle, stress management, appearance improvement strategies, and methods for complication and side-effect management. Their main sources for obtaining information were books, magazines, Internet, and peer groups in real and virtual worlds. The latter was their most commonly used source of information which they used to obtain information about the management of treatment side effects (such as physical pain, nausea and vomiting, vaginal dryness, lymphedema) and also about different types of hairpieces, breast prostheses, and breast reconstruction. They had greater confidence in information obtained from their peers compared with information obtained from health care providers.
I had vaginal dryness. Thus, I asked my cancer-afflicted friends and searched the internet. Finally, I found its treatment and now, effectively manage it. [P23]
A small number of participants attended educational programs and used counseling services offered to BC women in non-governmental organizations. They went to such settings to receive information and counseling about stress management, sexual functioning, life skills, healthy eating, and physical activity from attending psychologists, sexologists, nutritionists, oncologists, music therapists, yoga specialists, and lymph therapists. Of course, not all participants had access to these services.
After surgery, I went to lymph therapy classes, where they taught us how to facilitate lymphatic circulation through massage. [P33]
Self-care for managing limits
Participants performed self-care to overcome their physical and functional limits. They attempted to manage and reduce the symptoms of fatigue and weakness. For instance, they used nutritious and iron-based foods to provide energy and anemia treatment, and increased their sleep and rest periods to save and conserve energy. In addition, our participants used light sport exercise (walking, yoga, and swimming) to increase their physical capacity and ability to perform the tasks of housekeeping and taking care of the children.
After radiotherapy, when I went a little way, I suffering from a heart palpitations and extreme fatigue. I walk at a slow, my pulmonary volume low, I had a severe weakness and felt cold, but I fight. I ran yoga and stretching exercises. Every day I am doing 4–5 stretching exercises. My blood hemoglobin low, I ate grilled meat, and every day ate a little walnut, hazelnuts and pistachios. By doing this, treated my body’s weakness and anemia. [P23]
By maintaining the range of motion and by controlling arm lymphedema, participants try to keep physical function for doing everyday activities. They used physiotherapy, swimming, and yoga to decrease the swelling and increase the range of motion of the arm. BC women also prevent lymphedema by using healthy hand, lightweight cooking dishes, and get support from spouse and children to do their household chores. Women adhere to a low-sodium diet, raise their arms, avoid pulling and lifting of heavy objects, perform lymphatic drainage massage, avoid wearing tight-fitting clothes, and use hand and arm stretch compression bandages during swelling.
Because lymphedema may occur every time, I take many cares and caution. I do not lift heavy and raise my hand every time. The heavy and slow digestion food, consuming much meat and rice, lead to swollen arm, so, I eat more vegetarian and low-salt foods. [P14]
Participants cared for their physical appearance through skin, hair, and nails care and keep normal weight and fitness. Participants use several strategies for skin care such as Rejuderm cream to reduce surgery scar and skin massage with olive oil to reduce darkness and increase skin elasticity after radiotherapy. BC women also avoid direct sun exposure and use of moisturizer, hydration, and anti-spot face cream to prevent skin dryness and hyperpigmentation, and by increasing fluid intake and eating fresh colored fruits to maintain the color and texture of the skin. Participants use hair strengthening shampoos, natural herbal hair color, ammonia-free permanent hair color, and traditional medicine for care of hair following chemotherapy and also use nail moisturizer for reducing dry nails. Participants changed their health behaviors and followed a healthy lifestyle. They attempted to use more fresh vegetables and fruits, fish, and shrimp, and reduced the intake of high-fat, high-salt and sweet foods, fast foods, and remaining foods. They also used light physical exercises, such as walking, swimming, and yoga, to reduce overweight because of chemotherapy and to maintain fitness and body health.
I knew would become obese if I were eating much food during the chemotherapy, and cortisone injection. So I tried to eat low-calorie and healthy food. I had a great desire to eat sweets, but I tried to eat nuts instead of sweets. I washed and prepared celery, carrots and cabbage and I ate them when I wanted to eat something. I ate wheat germ, water and colored fruits, like carrots, watermelon so my skin did not hurt and pale. [P33]
Psychological self-empowerment
In order to cope with the psychological tensions and negative thoughts and feelings associated with their physical changes, participants used different strategies such as anger management, happy living, distraction, spirituality, self-confidence development, conscious negligence, and self-compassion. Accordingly, when they felt sad about their physical defects and dysfunction, they calmed themselves by praying, saying prayers, reciting the Holy Quran, and going to holy places. They also managed their anger by shouting in the mountains, going to anger management classes, consulting with psychologists, doing meditation, and expressing their emotions in peer groups in real and virtual worlds. Moreover, they boosted their morale and kept themselves happy by listening to happy music, dancing, distancing from bad news, joining joke-telling and happiness peer groups, and going to parties. They also attempted to push aside their disturbing thoughts and live in the moment by erasing alopecia-related memories and pictures, getting involved in outdoor and indoor activities, and performing artistic works (such as doll making, musical instrument playing, and singing). Furthermore, they had chosen to be indifferent to others’ curiosity about or reactions to changes in their physical appearance.
Sometimes, I start thinking about the reality that I’m not like before, have deformities in my hand or breast, or don’t have hair. In these cases, I attempt to perform my favorite activities such as travelling, attending praying or Quran recitation sessions, or going to the central market. In the market, I watch people and forget that I have some physical defects. [P21]
Another strategy for their psychological self-empowerment was self-compassion through establishing empathetic relationships with self instead of unconstructive self-criticism. To do so, they engaged in private self-talk with their bodies, treated their bodies with kindness, gently touched or kissed their bodies, or commiserated with the missed limb.
I attempt to be kind to my body and give it positive energy. I talk to my body very much. It gives me good feelings. When I give it positive energy and console it, I think it become more powerful. I kiss my right hand for the injections in it and apologize to it for my delay in seeking medical help. [P7]
Participants also attempted to boost their self-confidence by taking an optimistic view toward life, taking on a powerful appearance in parties or peer groups, avoiding comparison of themselves with others, and establishing purposeful interactions with caring people.
I had a yellow skin and had lost my eyelashes and eyebrows during the course of chemotherapy; however, I didn’t quit my job. Rather, I wore a headband and presented myself as a powerful person whose value and respect don’t depend on her appearance. [P14]
Maintaining maternal role
This category describes participants’ strategies for maintaining their paternal role. These strategies included empathetic interactions with children, concealment of the disease and its associated physical problems from them, suppression of negative feelings and thoughts, and promotion of their independence in doing their daily activities in order to protect them against psychological damages associated with their mothers’ BC.
I never wore sleeveless clothes in front of my children because I didn’t like them to see the sutures. I want them to see me as a real and perfect mother. [P27]
Moreover, they, individually or with the help of others, attempted to care for their children, maintain their morale, create a normal living condition for them, and assist them in their educational activities.
With the help of my sister, I prevented my children from experiencing depression or academic failure. After several chemotherapy sessions, I took my children outdoor to prevent damages to their morale. I did whatever I could for them. However, when I was too weak, my sister used to immediately came and take children to school. [P18]
Maintaining wife role
Maintaining wife role was the other strategy our participants used for coping with body image altered. This role included both housekeeping-related and sexual role. Our participants attempted to maintain household-related role (cleaning, cooking, shopping, and laundry) either independently or with the help of other family members. They changed doing household chores to keep their housekeeping role. They used a dishwasher instead of washing dishes with their hands. Instead of preparing, washing, and chopping vegetables, they used chopped and ready to cook vegetables. To ease cooking, they used lightweight pot and pan. They were doing their housework without hurry and with rest periods. Also, they shared responsibility for some of their housework between their spouses and their children.
Do not putting pressure on myself, with the help of my children; we do all the work of the house. In the first days, I planned and trained them for them. But after that, they themselves were skill. [P12]
They attempted to protect their wife role by maintaining sexual role. They fulfilled their husbands’ sexual needs and attempted to play sexual role against their husbands. Participants remind themselves of the sex desire. Before sex, they prepared themselves by watching porn movies. To increase sexual satisfaction, they used lubricant, olive oil, and sesame oil for reducing vaginal dryness. They are sexually self-sacrificing by expressing the desire to perform sex and initiating sex with their husbands and pretending to enjoy sex, despite having no sexual desire. BC women feel feminine through sex and attempted to keep their spouse’s support for themselves.
When I was on chemotherapy, I had limited sexual desire. Yet, I attempted, even more than before, to help my husband gain his pleasure. [P13]
In bed, I want my husband to sex with me. After each sex, I feel recharged. When we reach sexual satisfaction, I am feeling still a woman. [P10]
Discussion
This study aimed to explore Iranian BC women’s strategies for coping with body image altered. Findings showed that in order to cope with such alterations and reconstruction of feminine identity, BC women used the six strategies of physical appearance improvement, active information seeking, self-care for managing limits, psychological self-empowerment, maintaining maternal role, and maintaining wife role.
Physical appearance improvement was one of the main strategies used by participants. Previous studies also reported that BC women use makeup, prosthesis, hairpiece, scarf, veil, tattoo, and breast reconstruction in order to conceal or correct their physical defects.17,18 Changes in the body make BC women feel limited control over their physical appearance,20 and hence cause them depression and anxiety and undermine their self-confidence.9 Therefore, appearance management is an effective strategy to maintain body wholeness and to look better and normal.25,26 It reduces BC women’s sense of being different from others, decreases their vulnerability,27 protects them against social stigmatization,13,14 helps them have normal social interactions,25,26 gives them greater control over their appearance, boosts their maternal and sexual role performance,25 increases their self-confidence, enhances their body image,4 and protects their feminine identity.26,27 Therefore, appearance improvement strategies should be taught to BC women in order to improve their body image.4,26 An important point is that despite the significant role of breast reconstruction in reducing the emotional and psychological burdens of mastectomy, it is still considered as a plastic surgery in Iran, and hence is not covered by adequate insurance.28
Active information seeking was another strategy by our participants for coping with body image altered. In line with this finding, previous studies showed that BC women seek health-related information from different sources such as health care providers, Internet, and peer groups.29,30 Health-related information or knowledge promotes patients’ self-efficacy,29,30 while self-efficacy increases their self-confidence, gives them more control over their bodies, and improves their body image.20 Consequently, educational interventions can be used to promote patients’ self-efficacy and improve their body image.4 However, although health care providers are the most reliable source of health-related information, their failure to provide patients with quality education makes patients rely on other sources of information.29 These findings highlight the necessity of nurses’ greater attention to their educational and counseling role in order to fulfill patients’ educational needs.
Our participants also attempted adherence to self-care to manage their appearance and physical limits. Other studies also reported the same finding.4,17,20,31 Physical function plays an important role in body image. Fatigue is the most common complaint in BC women that affects physical function. Fatigue management through energy conservation, changing activity and rest rhythm, light physical exercise, listening to music, massage, eating nourishing meals, and treating anemia can improve the patient’s physical function and self-efficacy.31,32 Lymphedema causes pain, swelling, disfigurement, and changes in limb motility that affect self-esteem, interpersonal relationship, and body image. Lymphedema and limited movement of arm and shoulder affect daily activities, role, and function. Engagement in self-care can help restore motion of the arm and shoulder and control of lymphedema, which lead to better physical function and improved body image.33 Adhering to the healthy diet and regular physical exercise is one of the health-promoting behaviors and an important aspect of self-care behaviors. Evidence suggests that following healthy diet and exercise helps in creating healthy feeling, increasing physical activity, controlling weight, and increasing physical fitness in BC women. These, in turn, can increase self-efficacy, control over the body, and self-confidence, thus improving body image.4,17,31 Therefore, patient empowerment for self-care should be considered as an effective strategy for body image improvement among BC women.
Psychological self-empowerment was another main strategy used by BC women in the present study for coping with body image altered. BC women manage their psychological problems using different strategies such as acceptance, spiritual coping, distraction, suppression of negative thoughts, self-control, release of emotions,34 and self-respect and self-confidence improvement.35 Expression of feelings, adequate support, communication skills, self-confidence improvement, and stress management strategies have positive effects on self-esteem and body image.4,20 Our findings revealed that BC women rarely referred to psychologists and counselors for promoting their psychological self-empowerment. Similarly, a study reported that although body image altered were among the most important concerns of BC women, they rarely referred to psychologists for managing this concern.36 BC women avoid talking with others about their concerns over their bodies and femininity or seeking their help in order to protect themselves against social stigmatization.6 These findings highlight the importance of paying special attention to BC women’s psychological well-being in order to improve their body image.
Study findings also showed maintaining maternal role as another strategy used by BC women for coping with body image altered. Similarly, several earlier studies reported that BC women maintained their maternal role in order to protect their feminine identity.10,37 BC women maintain their maternal role through creating a normal condition in the house, paying attention to their children’s academic affairs, caring for their children, concealing their own feelings and discomfort,37,38 and performing household activities.39 Iranian BC women greatly focus on their maternal role, have grater emotional involvement with their children, and effectively cope with their maternal role.10 Such an attempt for maintaining maternal role improves women’s self-efficacy12 and gives them sense of self-confidence and control over life, which in turn positively affect their body image.6,12,40 Therefore, supporting BC women in maintaining and performing their maternal role can improve their body image.
Maintaining wife role was the other main strategy used by BC women for coping with body image altered. Two earlier studies also reported the same finding.6,8,27 Maintaining the family life has a valuable place in the culture and religion of Iranians; hence, ability to housekeeping and sexual role are important for a wife role in Iranian culture.8,10 Housekeeping disability and sexual dysfunction lead to helplessness, vulnerability, decreased self-worth, and threatening marital life.6,8,10 Accordingly, BC women attempt to maintain the family through resuming housekeeping and effective sexual role performance despite the lack of sexual desire.8,10 Performing housekeeping and sexual roles helps to have a feeling of control over life,15 increases their self-confidence, promotes their self-efficacy, and rebuilds their body image and feminine identity.6,12 Sexual problems are caused by psychological and hormonal disorders, and drug’s side effects. Thus, interdisciplinary collaborations among psychologists, sexologists, physicians, and nurses are required to diagnose and manage BC women’s sexual problems.41,42 However, Iranian women avoid from seeking professional health care services despite having sexual problems. Because talking about sexual issues is a matter of great cultural sensitivity and is considered as a cultural taboo in Iran.43 Also, sexual history taking is not routinely performed by clinicians.41 Thus, nurses and clinicians need to learn the communication skills to discuss about patients’ sexual problems. They should also consider continuous screening of women’s sexual problems during cancer treatment and defining the referral pathways.41,42
Limitations
Participants were selected purposively, and hence those who agreed to participate in the study might have had greater motivation for body image improvement. This fact can limit the transferability of the findings. Moreover, this study was conducted only on women and addressed just body image altered among patients with BC. Further studies on patients with different types of cancer and among both gender groups are recommended to produce more evidence regarding cancer patients’ strategies for coping with body image altered. Also, the coping strategies adopted and the outcomes were influenced by various conditions, such as context, individual, and the social facilitators and barriers, which are not mentioned in this article. Study on the facilitators and inhibitors of coping in women with breast cancer is recommended for future study.
Implications of the study for policy and practice
Health policy-makers can use the findings of the present study to develop interventions and programs for improving BC women’s body image care. These interventions may include beauty care for improving physical appearance, broadening health-related knowledge, promoting self-care, screening, triage of mental and sexual distress, and referral to specialists for receiving supportive and therapeutic interventions. Moreover, this study showed paucity in external resources and support for BC women. Thus, developing efficient social support systems and organizations is recommended in order to provide BC women with informational psychological counseling and insurance support.
Conclusion
This study concludes that Iranian BC women’s strategies for coping with body image altered are multidimensional, are mainly based on personal resources, and are used for both personal and interpersonal benefits. These strategies include physical appearance improvement, active information seeking, self-care for managing limits, psychological self-empowerment, and maintaining maternal and wife roles. Women use these strategies for reconstruction of their feminine identity.
Acknowledgments
This study was part of a PhD dissertation in nursing in Tarbiat Modares University, Tehran, Iran. The authors would like to thank all women who shared their experiences as well as the Research Administration of Tarbiat Modares University for its financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
Tao Z, Shi A, Lu C, Song T, Zhang Z, Zhao J. Breast cancer: epidemiology and etiology. Cell Biochem Biophys. 2015;72(2):333–338. | ||
Sharifian A, Pourhoseingholi MA, Emadedin M, et al. Burden of breast cancer in Iranian women is increasing. Asian Pac J Cancer Prev. 2015;16(12):5049–5052. | ||
Asadzadeh Vostakolaei F, Broeders MJ, Mousavi SM, Kiemeney LA, Verbeek AL. The effect of demographic and lifestyle changes on the burden of breast cancer in Iranian women: a projection to 2030. Breast. 2013;22(3):277–281. | ||
Fingeret MC, Teo I, Epner DE. Managing body image difficulties of adult cancer patients: lessons from available research. Cancer. 2014;120(5):633–641. | ||
Fobair P, Stewart SL, Chang S, D’Onofrio C, Banks PJ, Bloom JR. Body image and sexual problems in young women with breast cancer. Psychooncology. 2006;15(7):579–594. | ||
Martinez-Ramos G. Body image and femininity of Latina breast cancer survivors. Camino Real. 2009;1(1):89–109. | ||
Choi EK, Kim IR, Chang O, et al. Impact of chemotherapy-induced alopecia distress on body image, psychosocial well-being, and depression in breast cancer patients. Psychooncology. 2014;23(10):1103–1110. | ||
Khajehaminian F, Ebrahimi M, Kamali M, Dolatshahi B, Younesi S. [Sexual functioning after mastectomy surgery – A qualitative study]. Iranian Journal of Breast Disease. 2014;7(3):50–58. Persian. | ||
Rezaei M, Elyasi F, Janbabai G, Moosazadeh M, Hamzehgardeshi Z. Factors influencing body image in women with breast cancer: a comprehensive literature review. Iran Red Crescent Med J. 2016;18(10):e39465. | ||
Vaziri S, Lotfi Kashani F, Akbari M, Ghorbani Ashin Y. [Comparing the motherhood and spouse role in women with breast cancer and healthy women]. Iranian Journal of Breast Disease. 2014;7(2):76–83. Persian. | ||
Garrusi B, Faezee H. How do Iranian women with breast cancer conceptualize sex and body image? Sex Disabil. 2008;26(3):159–165. | ||
Pedram Razi S, Satiyarvand A, Tabari F, et al. The effect of education and telephone counseling on the self- efficacy of women with breast cancer undergoing radiotherapy. Iranian Journal of Nursing Research. 2018;13(1):64–72. | ||
Fang SY, Shu BC, Chang YJ. The effect of breast reconstruction surgery on body image among women after mastectomy: a meta-analysis. Breast Cancer Res Treat. 2013;137(1):13–21. | ||
Harcourt D, Frith H. Women’s experiences of an altered appearance during chemotherapy: an indication of cancer status. J Health Psychol. 2008;13(5):597–606. | ||
Taleghani F, Yekta ZP, Nasrabadi AN, Käppeli S. Adjustment process in Iranian women with breast cancer. Cancer Nurs. 2008;31(3):E32–E41. | ||
Grogan S. Femininity and body image: promoting positive body image in the “culture of slenderness”. In: Hörschelmann K, Colls R, editors. Contested Bodies of Childhood and Youth. London: Palgrave Macmillan; 2010. | ||
Brunet J, Sabiston CM, Burke S. Surviving breast cancer: women’s experiences with their changed bodies. Body Image. 2013;10(3):344–351. | ||
Jassim GA, Whitford DL. Understanding the experiences and quality of life issues of Bahraini women with breast cancer. Soc Sci Med. 2014;107:189–195. | ||
Falavigna M, Lima KM, Giacomazzi J, et al. Effects of lifestyle modification after breast cancer treatment: a systematic review protocol. Syst Rev. 2014;3:72. | ||
Cohen M, Mabjish AA, Zidan J. Comparison of Arab breast cancer survivors and healthy controls for spousal relationship, body image, and emotional distress. Qual Life Res. 2011;20(2):191–198. | ||
Pakseresht S, Jafarzadeh-Kenarsari F, Rafat F, Rahebi SM. Qualitative study of married women’s perception on the meaning of sexual-marital activity. J Qual Res Health Sci. 2017;6(1):78–88. | ||
Foroutan SK, Jadid Milani M. The prevalence of sexual dysfunction among divorce requested. Daneshvar Medicine Journal. 2009;16(78):39–44. | ||
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | ||
Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2014. | ||
McKean LN, Newman EF, Adair P. Feeling like me again: a grounded theory of the role of breast reconstruction surgery in self-image. Eur J Cancer Care (Engl). 2013;22(4):493–502. | ||
Kim IR, Cho J, Choi EK, et al. Perception, attitudes, preparedness and experience of chemotherapy-induced alopecia among breast cancer patients: a qualitative study. Asian Pac J Cancer Prev. 2012;13(4):1383–1388. | ||
Klaeson K, Sandell K, Berterö CM. To feel like an outsider: focus group discussions regarding the influence on sexuality caused by breast cancer treatment. Eur J Cancer Care (Engl). 2011;20(6):728–737. | ||
Manafi A, Ahmadi Moghadam M, Mirfakhraee AM. Breast reconstruction after mastectomy, necessity or luxury? Iranian Journal of Surgery. 2007;15(2):78–83. | ||
Namkoong K, Shah DV, Han JY, et al. Expression and reception of treatment information in breast cancer support groups: how health self-efficacy moderates effects on emotional well-being. Patient Educ Couns. 2010;81(Suppl 1):S41–S47. | ||
Latifi M, Barahmand N, Fahimnia F. Post-mastectomy Barriers for Information Seeking in Women with Breast Cancer. Health Inf Manage. 2016;13(5):326–332. | ||
Foster C, Breckons M, Cotterell P, et al. Cancer survivors’ self-efficacy to self-manage in the year following primary treatment. J Cancer Surviv. 2015;9(1):11–19. | ||
Chan R, Yates P, McCarthy AL. Fatigue self-management behaviors in patients with advanced cancer: a prospective longitudinal survey. Oncol Nurs Forum. 2016;43(6):762–771. | ||
Fu MR. Breast cancer survivors’ intentions of managing lymphedema. Cancer Nurs. 2005;28(6):446–457; quiz 458–459. | ||
Kvillemo P, Bränström R. Coping with breast cancer: a meta-analysis. PLoS One. 2014;9(11):112733. | ||
Berterö CM. Affected self-respect and self-value: the impact of breast cancer treatment on self-esteem and QoL. Psychooncology. 2002;11(4):356–364. | ||
Figueiredo MI, Fries E, Ingram KM. The role of disclosure patterns and unsupportive social interactions in the well-being of breast cancer patients. Psychooncology. 2004;13(2):96–105. | ||
Tavares R, Brandão T, Matos PM. Mothers with breast cancer: A mixed-method systematic review on the impact on the parent-child relationship. Psychooncology. 2018;27(2):367–375. | ||
Cho OH, Yoo YS, Hwang KH. Comparison of parent-child communication patterns and parental role satisfaction among mothers with and without breast cancer. Appl Nurs Res. 2015;28(2):163–168. | ||
Cheng T, Jackman M, McQuestion M, Fitch M. “Knowledge is power”: perceived needs and preferred services of male partners of women newly diagnosed with breast cancer. Support Care Cancer. 2014;22(12):3175–3183. | ||
Hajian S, Mehrabi E, Simbar M, Houshyari M. Coping strategies and experiences in women with a primary breast cancer dagnosis. Asian Pacific Journal of Cancer Prevention: APJCP. 2017;18(1):215–224. | ||
Vaziri Sh, Lotfi Kashani F. Sexuality after breast cancer: need for guideline. Iranian Journal of Cancer Prevention. 2012;5(1):10–15. | ||
de Morais FD, Freitas-Junior R, Rahal RM, Gonzaga CM. Sociodemographic and clinical factors affecting body image, sexual function and sexual satisfaction in women with breast cancer. J Clin Nurs. 2016;25(11–12):1557–1565. | ||
Fouladi N, Pourfarzi F, Dolattorkpour N, Alimohammadi S, Mehrara E. Sexual life after mastectomy in breast cancer survivors: a qualitative study. Psychooncology. 2018;27(2):434–441. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.