")
Back to Journals » Veterinary Medicine: Research and Reports » Volume 6
Recognizing and responding to cases of suspected animal cruelty, abuse, and neglect: what the veterinarian needs to know
Authors Arkow P
Received 31 July 2015
Accepted for publication 28 September 2015
Published 5 November 2015 Volume 2015:6 Pages 349—359
DOI https://doi.org/10.2147/VMRR.S87198
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Young Lyoo
Phil Arkow
National Link Coalition – The National Resource Center on The Link Between Animal Abuse and Human Violence, Stratford, NJ, USA
Abstract: The identification of a “battered pets” syndrome, which put the veterinary profession on a parallel footing with its counterparts in human medicine who respond to battered children, women, and elders, expanded the veterinarian’s role as an advocate for animals’ welfare to include the recognition of, response to, and prevention of animal abuse. Professional policies and legislation in several nations have been amended to define these responsibilities and delineate appropriate responses when animal maltreatment or other forms of family violence are suspected. This article reviews these changes, discusses abuse as a matter of animal welfare and public health, and summarizes research describing animal abuse as a possible indicator and predictor of interpersonal violence. Five steps that helped build human health care’s response to child abuse, domestic violence, and elder abuse, and that are analogous to forces in contemporary veterinary practice, are described. It familiarizes practitioners with terminology used in animal cruelty investigations. It describes clinical presentations, client profiles and behaviors, and environmental conditions that may raise a practitioner’s index of suspicion of possible animal maltreatment. It reviews protocols that practitioners may employ to respond compassionately and effectively to suspected animal abuse and enhance successful law enforcement investigations and prosecutions. Such responses can unite human and veterinary medicine in a common concern for vulnerable, victimized, and at-risk populations and position veterinarians as an essential part of public health approaches to break the cycles of violence affecting animals and human members of the family and community.
Keywords: animal cruelty, animal abuse, neglect, reporting, animal welfare, domestic violence
Introduction: the role of the veterinary professional in the prevention of abuse
An expansion of the veterinarian’s role as an advocate for animals’ welfare has emerged in recent years moving beyond the treatment of injury and disease to include the recognition of, response to, and prevention of animal abuse. Munro’s identification in 1996 of a “battered pets” syndrome1 put the veterinary medical profession on a parallel footing with its counterparts in human medicine. These counterparts recognize child abuse and neglect,2 domestic violence,3–6 and elder abuse7,8 as definable and preventable clinical conditions in which physicians have a duty and responsibility to evaluate the problem fully and strive to ensure that such trauma will not be repeated.9
Veterinarians’ responsibilities to protect animal welfare and alleviate animal suffering are embedded in policies and legislation extant in several nations. The New Zealand’s Code of Professional Conduct lists animal welfare as the first of seven fundamental principles calling it “a special responsibility” and “an over-riding professional duty”. Veterinarians must act immediately to remedy situations in which they have cause to suspect unreasonable or unnecessary pain or distress or possible breaches of animal welfare legislation. If the animal’s caregiver is a client, the veterinarian should discuss the situation and develop an action plan to relieve the concerns. The matter must be reported to an animal welfare inspector:
- if issues cannot be discussed with the caregiver;
- if the action plan’s improvements are not achieved; or
- if the case involves severe cruelty or neglect.
Valid and justifiable reasons allow disclosure of personal information. An explanatory note within the Code acknowledges research linking animal abuse with human violence and encourages veterinarians to consider whether people within the home might also be at risk. If this is the case, practitioners should use their best judgment to determine whether police or Child, Youth and Family authorities should be informed.10
Great Britain’s Royal College of Veterinary Surgeons’ Guide to Professional Conduct encourages veterinarians to include non-accidental injury (NAI) in the differential diagnosis. If the examination of the animal leads to a suspicion of abuse, the veterinarian should first attempt to discuss these concerns with the client. When this would be inappropriate or the client’s reaction increases rather than allays concerns, the veterinarian should contact the relevant authorities. Serious circumstances justify breaching obligations of client confidentiality. The Guide similarly extends veterinary response to report suspected child abuse and domestic violence.11
The Canadian Veterinary Medical Association declares that veterinarians have a “moral obligation” to report suspected cases of animal maltreatment. In return, “society has an obligation to support those veterinarians who report in good faith using their professional judgment”. Canadian Veterinary Medical Association encourages veterinary schools to train students in recognizing and reporting animal abuse. It urges veterinary associations to lobby their provincial governments to make the reporting of animal abuse mandatory with immunity from civil and criminal liability when reports are made using professional judgment and in good faith. Canadian Veterinary Medical Association likewise recognizes animal abuse as an important social issue affecting families and communities due to the link between animal abuse and human violence. Veterinarians may help break the cycle of family violence and create safe, humane communities by reporting suspected animal abuse.12 As of this writing, veterinarians in five of Canada’s 13 provinces and territories are required to report suspected cruelty. They join other professionals who are granted civil and criminal immunity for reporting animals in distress or for assisting in the enforcement of animal protection laws.
The American Veterinary Medical Association in 2010 amended the Veterinarian’s Oath to include the protection of animal welfare and the prevention of animal suffering.13 The American Veterinary Medical Association Policy on Animal Abuse and Neglect issued in 2012 recognized that veterinarians may observe cases of animal abuse or neglect as defined by laws. The Policy declares that it is their responsibility to report cases promptly to appropriate authorities to protect the health and welfare of animals and people, regardless of whether reporting is mandated by law.14 As of this writing, 20 of America’s 50 states have enacted legislation mandating or permitting veterinarians to report suspected animal maltreatment with immunity from civil and criminal liability. Two states require veterinarians to report suspected child abuse. One state mandates reporting suspected abuse of elders and vulnerable adults.15
Animal abuse as a health concern
Animal abuse is part of the spectrum of family and community violence which should be viewed as a leading worldwide public health problem.16 Two US Surgeons-General have called violence a matter best resolved through public health interventions rather than through sociological or law enforcement approaches.17,18 Family physicians in Australia have been advised that animal cruelty impacts human health in disparate ways, is an important sentinel for domestic violence and child abuse, and raises important questions about the type of society we wish to live in.19
Pets that are well cared for have long been seen as protective factors for human physiologic and behavioral health. Animal-assisted therapy programs incorporate this concept through occupational, physical, and speech therapy interventions with at-risk populations, therapeutic horseback riding, service animals to assist the disabled, and obesity control.20 While acts of animal cruelty have traditionally been considered important to the animals’ well-being but of only marginal significance to human interests, research describes animal abuse as potentially indicative and predictive of interpersonal violence and as adverse experiences impacting human health as well as animal welfare. Abuse of companion and farm animals is often a component of intimidating behaviors utilized by perpetrators of intimate partner violence and child sexual abuse. Such abuse serves to dominate, control, and induce fear and subservience in their victims and to deter battered women and their children from leaving abusive situations.20–27
In a study of Women’s Refuge clients and staff in New Zealand, Roguski27 described pets as “pawns” and animal cruelty as complex and multifaceted in households marked by domestic violence. Animal abuse:
- creates a culture of normalized violence and psychological and emotional abuse;
- is conducted purposefully by batterers who believe that police will not see animal cruelty as warranting taking action;
- occasionally includes forced use of pets as sexual objects;
- occurs as a result of the perpetrator’s jealousy of his partner’s or a child’s affections directed elsewhere; and
- is also directed against animals belonging to friends and family members who abet her escape.
Orchestrated harm to animals creates a level of intimidation that secures families’ obedience. It is a barrier that delays women’s leaving abusive situations for a median amount of time of 2 years. Emotional abuse involving animals is one of the first indications of escalated and broadened physical violence toward family members. In all, 32.7% of survey participants with children reported that one or more of their children had witnessed threats to injure or kill an animal. An additional 24.5% had witnessed actual killing or injury.27
Comparable findings have been reported in the US,28 Canada,29,30 Australia,31,32 the Bahamas,33 and Ireland.34,35 Partners of women living in domestic violence shelters were reported to be 11 times more likely to hurt or kill pets than were a comparison group of partners of non-abused women.36 Batterers who also abuse animals were described as more dangerous and used more forms of violence than batterers who do not harm animals.37 A history of pet abuse was reported to be one of the four most significant risk factors of becoming a batterer.38 In all, 41% of intimate partner violence offenders were reported to have committed an act of animal abuse compared to a community incidence rate of animal cruelty of 1.5%.39
Other research links histories of animal abuse with dog bite fatalities. Patronek et al reported that 21.1% of 256 canine attacks resulting in human deaths involved dogs that had been abused.40 DeViney et al reported that families under investigation for child abuse experienced 11 times more dog bites than did non-abusing households.41
Neglect of animals may be a marker for elderly persons’ co-occurring self-neglect and a variety of mental health disorders.42–44 Animal hoarders, who are statistically over-represented by older women, may live in unhealthy and squalid environments surrounded by dozens or hundreds of living and dead animals in a self-fulfilling cycle of social isolation. Three distinct types of animal hoarders have been identified.45–48
Veterinarians as sentinels: building a professional response to suspected abuse
Five steps were necessary to institutionalize human health care’s response to child abuse, domestic violence, and elder abuse. These steps, which removed personal, professional, peer, and organizational normative barriers, are analogous to forces currently active in veterinary medicine. These five steps may be summarized as follows.9
Build awareness that these are matters of significant professional interest
More than 1,000 journal and mainstream publications address animal cruelty, abuse, and neglect as linked to human health and safety and as worthy of a multidisciplinary professional response.49 Over 100 of these are specific to veterinary recognition and reporting issues.50–61 Varying findings were reported in several surveys of veterinarians’ knowledge of animal abuse and other family violence and their attitudes toward reporting suspected abuse.62–66 In one survey of New Zealand practitioners, a majority of respondents reported having seen cases of animal abuse within the previous 5 years and felt a strong ethical duty to deal with cases of animal abuse. Respondents were less comfortable about issues of human abuse even though awareness of the link between abuse of animals and abuse of humans was relatively high.67
This awareness is being augmented by training programs in colleges of veterinary medicine and continuing veterinary medical education.
Assist professionals to resolve contentious ethical dilemmas
Practitioners and their staffs often experience confounding dilemmas with cases of suspected animal cruelty, abuse, or neglect9 and an emotional block against wanting to recognize the potential of abuse.68 They need to balance economic, safety, confidentiality, legal, and management concerns with ethical principles, personal beliefs, and professional standards while attempting to respond compassionately and effectively to individual animals and society. Additional pressure is exerted when egregious or spectacular cases generate extensive news media coverage. With increasing public, legislative, and prosecutorial interest in animal welfare, failure to respond appropriately places the profession at risk of adverse criticism and litigation.69 A cruelty case can bring into question what Rollin70 called a fundamental dilemma of veterinary medicine: whether the primary responsibility is to the patient or client.
Robertson71 distinguished between ethical duties (ie, what a veterinarian should do as judged by the profession’s authorities) and legal duties (ie, what a veterinarian must do as specified by the profession and the law). While veterinarians remain divided on whether reporting suspected abuse should be mandated and numerous reasons for this division have been identified,9 it may be argued that a mandate required by law eliminates the contentious moral dilemma72 by making the decision automatic and explainable to the client. Once a decision has been made, the issue becomes how to appropriately implement a reporting process to comply with the duty.
Provide guarantees of legal protection
As noted above, many political and organizational bodies have approved mandatory or permissive reporting processes which reduce exposure to civil and/or criminal liability. This protection may be limited (in effect only if the report was made in good faith). Conversely, it may be absolute (applicable even if the report was made negligently or fraudulently).73
The confidentiality of patient records and whether they may be released to the client and/or outside agencies with or without a court order varies widely. The practitioner is advised to check with legal counsel for the most current information.73 New Zealand’s Privacy Act 1993 allows veterinarians to provide personal and private information about a client and his or her animals to an inspector if they believe the information is necessary to prevent, detect, investigate, and prosecute offenses under the Animal Welfare Act.74
Penalties for failure to report are common in laws governing physicians’ reporting of suspected child abuse. Although similar provisions might be inferred in veterinary animal abuse reporting laws,71 they have not been widely included to date. Practitioners in New Zealand who do nothing, allow unnecessary or unreasonable pain or distress to continue, or who take actions that exacerbate animal welfare issues may be investigated as a party to an offense, depending on the circumstances.74
As recognized authorities on animal health, veterinarians may be called to testify in court proceedings as a witness of fact or as an expert witness, and to issue a professional opinion as to whether an animal has been injured or is in pain.60 Training in this area is available through the International Veterinary Forensic Sciences Association (http://www.ivfsa.org). The distance education MS degree and graduate certificate in veterinary forensics at the University of Florida’s Maples Center for Forensic Medicine (http://forensics.med.ufl.edu/distance-education/) provides additional training. Such training helps practitioners to identify clinical conditions that indicate NAI and to conduct evidence-gathering and record-keeping procedures that will withstand legal scrutiny should cases result in prosecution.
Provide training in identification of clinical indicators of abuse as a differential diagnosis
The definitions of animal cruelty, abuse, and neglect vary widely across geographic, cultural, and professional boundaries and can shift from time to time and situation to situation. In a culture that institutionalizes such accepted practices as hunting and intensive livestock production while simultaneously revering its companion animals, achieving a universal definition of such a subjective and abstract concept as animal maltreatment is highly problematic.75
Each jurisdiction’s statutes vary in the specificity of proscribed behaviors. Most statutory language is necessarily vague: for example, a law may require that an animal have an “adequate” shelter. This allows the investigator to make a common-sense value judgment based upon ambient environmental conditions and an animal’s metabolic needs. However, a skilled defense attorney could argue that without specific criteria regarding temperature, shade, exposure to the elements, and so on, one cannot know whether cruelty actually occurred. Cruelty is frequently defined with such ambiguous language that courts may not perceive an incident to violate statutes unless it is extreme and outrageous.76
Animal cruelty, abuse, and neglect generally imply socially unacceptable actions or omissions that inflict unnecessary pain or distress. What constitutes “unnecessary” varies between countries and from time to time in each country and the prevailing standard can be determined only by the courts.77
The following terms in law enforcement investigations most commonly describe socially unacceptable conduct toward animals.75 These terms may or may not match statutory language in any given jurisdiction.
- Animal cruelty: the most prevalent term, implying a deliberate infliction of pain from which the offender derives enjoyment or amusement.
- Animal abuse: a more neutral term, modeled after the child protection field, describing willful or negligent maltreatment regardless of the perpetrator’s intent, motivation, or mental state.
- Animal neglect: an act of omission signifying a lack of care, the most common form of maltreatment.
- Animal hoarding: neglect on a significant scale involving large numbers of animals often kept in deteriorating conditions below minimal standards of nutrition, sanitation, and veterinary care.
- Animal physical abuse: a wide range of injurious acts requiring active engagement such as beating, kicking, suffocating, throwing, shaking, poisoning, and burning. The clinical presentation includes injuries to the skeleton, soft tissue, or organs sustained as a result of beating or repeated maltreatment.
- NAI: a term borrowed from the child protection field as a synonym for physical abuse.78–81
- Animal sexual abuse: abusive acts or sexual conduct with an animal involving the rectum, anus, or genitalia. The term is preferred over the more archaic bestiality (in which sexual intercourse must occur) and zoophilia (a strong erotic preference for animals).
- Emotional abuse: a concept prevalent in the lexicon of interpersonal violence generally absent from animal cruelty laws.
Detailed descriptions of clinical conditions that should raise an index of suspicion of the above conditions are too exhaustive for this limited review. They have been discussed more extensively in several key guidances.68,73,74,78–83 They may be summarized as follows.
Presenting clinical factors
- Unexplained or repetitive injuries to an animal, which may show up on examination, ultrasound or X-ray
- History of unexplained or repetitive injuries to multiple animals
- Evidence of rib injuries, either current or from previous trauma
- Low weight or low body condition scores
- Unexplained poisoning, burns, bruising, and stab wounds
- Fractures: Tong84 reported five features which should raise the index of suspicion and support a diagnosis of NAI, especially among young male dominant breeds such as Staffordshire bull terriers:
- Presence of multiple fractures
- Fractures occurring on more than one region of the body
- Transverse fractures
- Fractures presenting at a later stage of healing
- Multiple fractures at different stages of healing
- Gunshot wounds
- Ingrown collar
- Scars, wounds, and traumas consistent with animals used in dog- or cock-fighting competitions
- Obvious severe neglect: this may include heavy ectoparasite infestation, dental disease, severely matted fur, failure to treat adverse medical conditions, dehydration, emaciation, or overgrown claws, horns, or hooves
- Signs of disease, pain, distress, or injuries needing treatment, such as blood from orifices, vocalization, vomiting, lameness, shivering, or diarrhea
- Sexual abuse
- The animal displays fear of its owner or of people in general
- The animal displays an unexplained change in behavior.
Client profile factors
- The client is new to the practice or visits several clinics to avoid raising suspicion
- Discrepancies in names, addresses, and ownership of animals
- Prior history with the client has raised concerns
- History of high turnover of animals, especially with repetitive histories of behavioral problems
- Family is known to be under economic, marital, substance abuse, family violence, or other pressures
- The client’s knowledge, skills, and attitude compromise the ability for proper animal husbandry.
Client behavior factors
- History as presented by the client is inconsistent with the nature of the injuries
- Family members present changing or discrepant histories
- The Client lacks concern and is indifferent to the animal’s injuries
- The client repeatedly fails to follow-up on the treatment of serious medical conditions
- Weak emotional attachment to the animal
- Unexplained delay in seeking medical attention
- The client is argumentative or aggressive; other family members may appear intimidated, apprehensive, or deferential
- The client expresses not feeling safe at home
- The client blames someone else or unknown causes for the trauma
- The client’s methods of disciplining or housebreaking animals raise concerns
- Children’s responses to questions about their pets raise concerns
- Munchausen syndrome by proxy involving the animal81
Environmental factors
- Hoarding excessive number of animals under substandard care
- Animals’ living environment is unsuitable
- Availability, nutritional composition, and quality of feed are insufficient for animals’ metabolic needs
- High incidence of viral, bacterial, and fungal infections, heavy intestinal or heartworm burdens, or dermatitis or other skin conditions indicative of flea infestations or sarcoptic and demodectic mange
- The animal has been abandoned by owners who have departed.
As shown in Table 1, the Colorado Veterinary Medical Association85 summarized suspicious patterns of NAI. More detailed descriptions of these and similar traumas may be found in several textbooks that review veterinary pathology, crime scene investigation, evidence collection, and recording techniques employed in forensic animal cruelty investigations.86–90
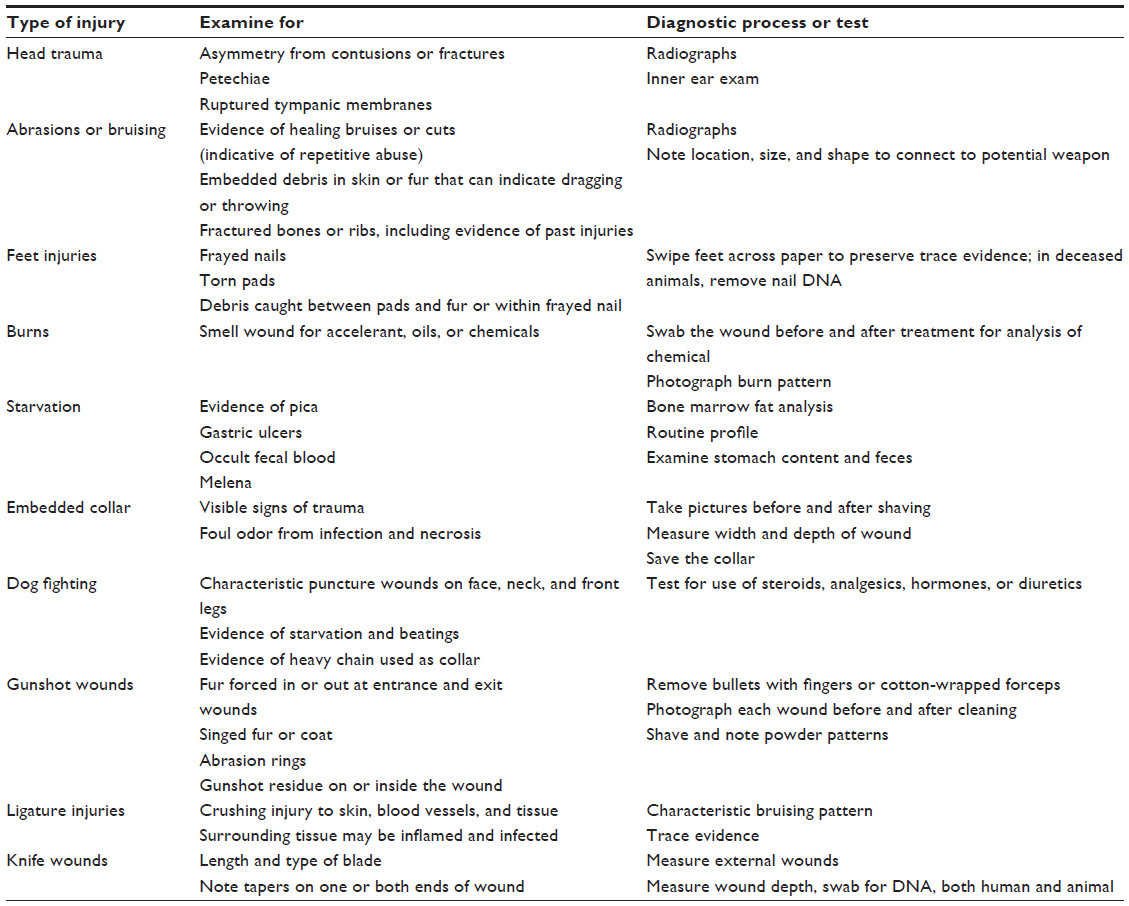 | Table 1 Patterns of non-accidental injury |
The practitioner is reminded that it is not necessarily a single incident that leads to a raised index of suspicion, but rather a variable combination of factors, pattern of actions, and behaviors, or injuries which are not clearly or adequately explained. The person presenting the animal may not be the perpetrator or may be under some coercion from the person who caused the injury.
Develop standardized protocols for responses that balance the interests of the practice, clients, patients, and other animals in the household
The complexities of animal cruelty cases and their inherent ethical dilemmas are challenging, particularly for junior members of the clinical team, nurses, receptionists, and technicians if the senior members do not believe abuse has occurred. A practice-specific decision-making protocol should be established in advance. This must protect the interests of the patient, other animals, the veterinary staff and practice, the client, and other family members whenever a staff member is concerned for an animal’s welfare.
Administering a client questionnaire73 that describes family members’ relationships with and attitudes toward their animals may uncover patterns of abusive behaviors and inability to provide proper animal husbandry. This questionnaire could be administered when welcoming a new client to the practice or whenever an abusive etiology is suspected.
A victim may be presented by a perpetrator, another family member (who may be a victim himself/herself), or a third party. The situation is best handled by an experienced clinician with a firm policy in place. It is important to remain calm, polite, and objective, indicating that the inquiries are in the animal’s best interests. If the suspicions are allayed, brief notes should be kept in the clinical file. If the inquiry suggests that a second opinion, further examination, or possible reporting to authorities is indicated, comprehensive, contemporaneous, and accurate note-taking or tape recording is essential especially if the case will lead to a formal investigation. Explanations from the owner or presenter should be recorded as fully as possible. If no explanation is offered, this should be noted as well.68
The assessment of the animals and their environment is essential for potential prosecution. This will enhance the veterinarian’s credibility with the client, animal welfare investigators, police, and the courts.74 Notes should be signed and dated. If possible, another veterinarian should conduct a second, documented examination, which may support or contradict the findings. If a report is made to law enforcement, it is not realistic to expect to remain anonymous. Nor will the veterinarian be expected to make a determination of cruelty: the investigating authority will make this determination.85
When writing notes for the client’s file, consider how you would describe the scene and the animal’s condition to best portray the scale of the incident and severity of the animals’ pain and distress to a third party several months hence. The notes should include the following.74,85
Base information
- Who engaged you
- Date, location, time, and duration of visit(s)
- Other parties present
- Number, class, species, breed, and sex of the animal(s)
- Chief complaint by the client
- Statements made by the client or others, which may include incriminating conduct: try to write down exactly what is said
- Document the timeliness of seeking veterinary care and how the animal was presented (walking on own, limping, carried in)
- Identifiable risk factors, including the client’s financial issues, client’s decision-making authority, physical environment, nutrition type and availability, and animal husbandry concerns.
The assessment undertaken
- Nature and number of physical examination(s), radiographs, and laboratory tests noting any abnormalities or unusual findings
- Description of injuries: a wound diagram using a silhouette drawing may be helpful
- Body condition: be specific as to which score scale you use and be very descriptive
- Coat condition, including suspected parasites or foreign material
- Dental condition
- Observations of normal/abnormal behavior
- Discussion of levels of pain and distress
- Photographs or videos taken, including “before and after”, full-body shots, and close-ups; remember that fur or feathers may conceal injuries.
Diagnosis, advice, and treatment
- All steps that lead up to the diagnosis
- Processes or considerations adopted to rule out all other possible contributing factors
- Details of all advice given to the client
- Treatment(s) administered
- Outcome achieved for the animal(s)
- Details of subsequent follow-up examinations and treatments
- Specific literature or other materials used to support your opinions.
If euthanasia is indicated, document the reasons for this decision (eg, “in extreme pain and suffering” or “injured past recovery”). Take care to maintain all records and notes as a “chain of evidence” for potential prosecution. Keep a chronological record of the movement or transfer of any sample (ante- or post-mortem) or physical evidence from the diagnostic processes (eg, X-rays, ultrasound, photographs, laboratory results), including any courier services utilized, from the time it was taken until the production of the evidence in a courtroom. Such materials must be securely and appropriately packaged and stored, including storing the body in a freezer or refrigerator for necropsy by a forensic pathologist so as to not contaminate or deteriorate the evidence.
Several factors determine whether the most appropriate course of action is to educate the client, monitor the situation further, or report to an animal welfare inspector or law enforcement agency. These include the following.68,73,74,83
- Statutory mandates or permissions to report with protection from exposure to civil or criminal liability
- Number of problems, severity, frequency, and duration of injuries
- The client’s intentionality, motivations, and attitude regarding the injuries, and willingness and ability to correct adverse situations
- Whether the situation is normal and acceptable under applicable laws and contemporary standards
- Medical histories of the patient and the client’s other animals
- Appearance and attitude of other family members and witnesses
- Availability of procedures for follow-up on questionable cases
- Indications of co-occurring domestic violence or child abuse.
The flowchart in Figure 1,10 developed in New Zealand, may serve as a model adaptable in other nations to guide practitioners to an appropriate response.
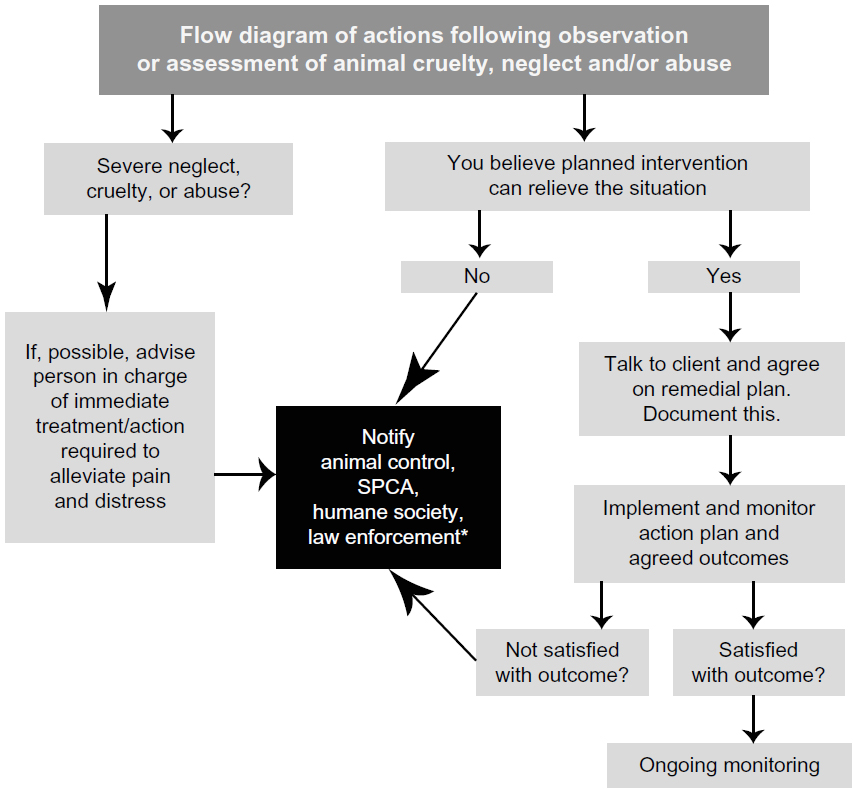 | Figure 1 A flow diagram of actions following observation of an animal welfare case. |
When in doubt, seek clarification from your veterinary association or legal counsel. Whichever decision is made, staff members should be fully briefed on the situation and understand the implications for the clients’ future visits. Remember that it is not up to the veterinarian to establish any offense, but to report the situation to those who have the legal power to investigate. They will make a determination whether filing of criminal charges is warranted.
Conclusion
Animal maltreatment is one of the most challenging diagnoses in clinical work requiring time, experience, emotional energy, sensitivity, tact, and not a small measure of courage. Practitioners may be reluctant to admit that a client would present abused animals for treatment. Nevertheless, most practitioners will be presented at some time in their careers with cruelty cases.63,78–81,91–95 While such cases may not be seen regularly, they are invariably problematic and difficult to resolve.52
Veterinarians’ reluctance to report suspected maltreatment is outweighed by the profession’s sense of responsibility to animal welfare, satisfaction of helping abused animals, and opportunity to stop escalation into interpersonal violence. A proactive response has the potential to save human lives and reduce animal suffering.
Animal cruelty cases are being treated with more respect than at any time in the past. With 99% of Americans perceiving animals as close companions or family members,96 animal abuse should be described as a form of family violence. We are witnessing increased public concern for animals, a proliferation of university courses in human–animal studies and animal law, a growing number of animal-assisted therapy programs, and extensive empirical evidence for animal abuse as a precursor to human violence. These are generating a renaissance of interest in animal well-being as an indicator of human health.
This increased attention is helping veterinarians to address animal welfare more fully and to fulfill the oath to use their skills for the betterment of society. Veterinarians are ideally placed as sentinels to identify and treat abuse and to report it to appropriate authorities as necessary. Practitioners can be an essential part of public health approaches to break the cycles of violence affecting animals and human members of the family and community.
Animal cruelty is a crime. Specialized veterinary pathology and veterinary forensics laboratories are being established in more developed areas. Elsewhere, the services of human forensic specialists are being utilized to help document animal cruelty. This improved capability to document and present clinical findings, combined with increased awareness of the impact of animal abuse on human well-being, has led to more aggressive prosecution of animal cruelty cases. Recognizing and reporting suspected animal abuse are the first steps to resolve unhealthy situations and make communities safer for all. In so doing, veterinarians can work within a One Health approach that unites human and veterinary medicine in a common concern for the vulnerable, victimized, and at-risk.
Disclosure
The author reports no conflicts of interest in this work.
References
Munro HMC. Battered pets. Ir Vet J. 1996;(49):712–713. | |
Kempe CH, Silverman FN, Steele BF, Droegenmuller W, Silver HK. The battered-child syndrome. JAMA. 1984;251(24):3288–3294. | |
Walker LA. The Battered Woman. New York: Harper and Row; 1979. | |
Salber PR, Taliaferro E. Physician’s Guide to Domestic Violence: How to Ask the Right Questions and Recognize Abuse. Volcano (CA): Volcano Press; 1995. | |
Schornstein SL. Domestic Violence and Health Care: What Every Professional Needs to Know. Thousand Oaks (CA): Sage Publications; 1997. | |
Jordan CE, Nietzel M, Walker R, Logan TK. Intimate Partner Violence: Clinical Training Guide for Mental Health Professionals. New York: Springer; 2004. | |
National Center on Elder Abuse. 15 Questions and Answers about Elder Abuse. Washington: The Center; 2005. | |
Hildreth CJ, Burke AE, Golub RM. Elder abuse. JAMA. 2011;306(5):568–568. | |
Arkow P, Munro, H. The veterinary profession’s roles in recognizing and preventing family violence: The experiences of the human medicine field and the development of diagnostic indicators of non-accidental injury. In: Ascione FR, editors. The International Handbook of Animal Abuse and Cruelty: Theory, Research and Application. West Lafayette (IN): Purdue University Press; 2008:31–58. | |
Veterinary Council of New Zealand. Code of Professional Conduct: Animal Welfare. Wellington: The Council; 2012. | |
Royal College of Veterinary Surgeons. Guide to Professional Conduct for Veterinary Surgeons: Animal Abuse, Child Abuse, Domestic Violence. London: The College; 2003. | |
Animal abuse – position statement, 2011, Canadian Veterinary Medical Association Web Site. Available from: http://www.canadianveterinarians. net/documents/animal-abuse. Accessed July 29, 2015. | |
Nolen RS. Veterinarian’s Oath revised to emphasize animal welfare commitment. J Am Vet Med Assoc. 2011;238(1):15–16. | |
American Veterinary Medical Association. Resolution #1 – 2012 Regular Winter Session: Policy on Animal Abuse and Animal Neglect. Schaumburg (IL): The Association; 2012. | |
The National Link Coalition. Is veterinary reporting of abuse being taught in states where reporting is mandated? LINK-Letter. 2015;8(4):7. | |
Gullone E. Animal Cruelty, Antisocial Behaviour, and Aggression: More than a Link. Basingstoke (UK): Palgrave Macmillan; 2012. | |
Koop CE, Lundberg GD. Violence in America: A public health emergency: Time to bite the bullet back. JAMA. 1992;267(22):3075–3076. | |
Novello AC, Shosky J, Froehlke R. From the Surgeon General, US Public Health Service: A medical response to violence. JAMA. 1992; 267(22):3007–3007. | |
Sherley M. Why doctors should care about animal cruelty. Aust Fam Physician. 2007;36(1–2):61–63. | |
Arkow P. A Link Across the Lifespan: Animal Abuse as a Marker for Traumatic Experiences in Child Abuse, Domestic Violence and Elder Abuse. Shakopee (MN): Academy on Violence and Abuse; 2015. | |
Ascione FR, Arkow P, editors. Child Abuse, Domestic Violence and Animal Abuse: Linking the Circles of Compassion for Prevention and Intervention. West Lafayette, (IN): Purdue University Press; 1999. | |
Arkow P. Breaking the Cycles of Violence: A Guide to Multi-Disciplinary Interventions. A Handbook for Child Protection, Domestic Violence and Animal Protection Agencies. Alameda (CA): Latham Foundation; 2003. | |
Becker F, French L. Making the links: Child abuse, animal cruelty, and domestic violence. Child Abuse Rev. 2004;13(6):399–414. | |
Merz-Perez L, Heide KM. Animal Cruelty: Pathway to Violence Against People. Walnut Creek (CA): AltaMira Press; 2004. | |
DeGue S, DiLillo D. Is animal cruelty a “red flag” for family violence? Investigating co-occurring violence toward children, partners, and pets. J Interpers Violence. 2009;24(6):1036–1056. | |
Randour ML. What Every Clinician Should Know About the Link Between Pet Abuse and Family Violence. Washington: American Psychological Association; 2011. | |
Roguski M. Pets as Pawns: The Co-existence of Animal Cruelty and Family Violence. Auckland: Royal New Zealand Society for the Prevention of Cruelty to Animals; 2012. | |
Goodman PE. The relationship between intimate partner violence and other forms of family and societal violence. Emerg Med Clin North Am – Emergency Medicine and the Public’s Health. 2006;24(4):889–903. | |
McIntosh S. Exploring the links between animal abuse and domestic violence: Calgary research results. The Latham Letter. 2001;22(4):14–16. | |
Doherty D, Hornosty J. Exploring the Links: Firearms, Family Violence and Animal Abuse in Rural Communities. Fredericton (NB): University of New Brunswick Family Violence on the Farm and in Rural Communities Project; 2007. | |
Fawcett N, Gullone E, Johnson J. Domestic violence and animal abuse: Encouraging collaborative relations between animal welfare and human welfare agencies in Australia. InPsych: Bull Aust Psychol Soc. 2002;24(2):36–38. | |
Tiplady CM, Walsh DB, Phillips, CJC. Intimate partner violence and companion animal welfare. Aust Vet J. 2012;90(1–2):48–53. | |
Fielding, WJ. Domestic violence and dog care in New Providence, The Bahamas. Soc Anim. 2010;18(2):183–203. | |
Allen M, Gallagher, B, Jones B. Domestic violence and the abuse of pets: Researching the link and its implications in Ireland. Practice: Soc Work Action. 2006;18(3):167–181. | |
Gallagher B, Allen M, Jones B. Animal abuse and intimate partner violence: Researching the link and its significance in Ireland – a veterinary perspective. Ir Vet J. 2008;61(10):658–667. | |
Ascione FR. Emerging research on animal abuse as a risk factor for intimate partner violence. In: Kendall-Tackett K, Giacomoni S, editors. Intimate Partner Violence. Kingston (NJ): Civic Research Institute; 2007:3.1–3.17. | |
Simmons CA, Lehmann P. Exploring the link between pet abuse and controlling behaviors in violent relationships. J Interpers Violence. 2007;22(9):1211–1222. | |
Walton-Moss BJ, Manganello J, Frye U, Campbell JC. Risk factors for interpersonal violence and associated injury among urban women. J Community Health. 2005;30(5):377–389. | |
Febres J, Brasfield H, Shorey RC. et al. Adulthood animal abuse among men arrested for domestic violence. Violence Against Women. 2014; 20(9):1059–1077. | |
Patronek GJ, Sacks JJ, Delise KM, Cleary DV, Marder AR. Co-occurrence of potentially preventable factors in 256 dog bite-related fatalities in the United States (2000–2009). J Am Vet Med Assoc. 2013; 243(12):1726–1736. | |
DeViney E, Dickert J, Lockwood R. The care of pets within child abusing families. Int J Study Anim Probl. 1983;(4):321–329. | |
Cooke-Daniels L. The connection between animals and elder abuse. Victimization Elder Disabl. 1999;2(3):37–47. | |
Boat BW, Knight JC. Experiences and needs of Adult Protective Services case managers when assisting clients who have companion animals. J Elder Abuse Negl. 2000;12(3–4):145–155. | |
Lockwood R. Making the connection between animal cruelty and abuse and neglect of vulnerable adults. The Latham Letter. 2002;23(1):10–11. | |
Hoarding of Animals Research Consortium. Health implications of animal hoarding. Health Soc Work. 2002;27(2):125–136. | |
Patronek GJ, Loar L, Nathanson JN, editors. Animal Hoarding: Structuring Interdisciplinary Responses to Help People, Animals and Communities at Risk. North Grafton (MA): Hoarding of Animals Research Consortium; 2006. | |
Kuehn BM. Animal hoarding: A public health problem veterinarians can take a lead role in solving. J Am Vet Med Assoc. 2002;221(8): 1087–1089. | |
Frost RO, Patronek G, Arluke A, Steketee G. The hoarding of animals: An update. Psychiatr Times [webpage on the Internet]. New York: UBM Medica LLC, 2015 [updated April 30, 2015; cited July 30, 2015]. Available from: http://www.psychiatrictimes.com/addiction/hoarding-animals-update/page/0/1. Accessed September 16, 2015. | |
animaltherapy.net [webpage on the Internet]. Bibliography of the Link between Animal Abuse, Domestic Violence, Child Abuse and Elder Abuse. Stratford (NJ): Animal Therapy.net; 2015 [cited July 30, 2015]. Available from: http://animaltherapy.net/animal-abuse-human-violence/bibliography/. Accessed September 16, 2015. | |
Arkow P. The correlations between cruelty to animals and child abuse and the implications for veterinary medicine. Can Vet J. 1992;33(8):518–521. | |
Arkow P. Child abuse, animal abuse, and the veterinarian. J Am Vet Med Assoc. 1994;204(7):1004–1007. | |
Crook A. The CVMA animal abuse position – how we got here. Can Vet J. 2000:41(8):631–633. | |
Lockwood R. Animal cruelty and human violence: The veterinarian’s role in making the connection – the American experience. Can Vet J. 2000;41(11):876–878. | |
McGuinness K, Allen M, Jones BR. Non-accidental injury in companion animals in the Republic of Ireland. Ir Vet J. 2005;58(7):392–396. | |
Lofflin J. Animal abuse: What practitioners need to know. DVM360 [serial on the Internet]. Lenexa: UBM Life Sciences, Veterinary; 2006 [cited August 1, 2006] Available from: http://veterinarymedicine.dvm360.com/animal-abuse-what-practitioners-need-know. Accessed July 29, 2015. | |
Whiting TL, Brennan SC, Wruck GC. The veterinary profession’s role in policing animal welfare. Can Vet J. 2006;47(11):1065–1072. | |
Arkow P. The veterinarian’s responsibility in family violence. Amer Assoc Hum-Anim Bond Vet. 2006;(17):4. | |
Canadian Veterinary Medical Association. Animal Abuse: What Veterinarians Can Do. Ottawa: The Association; 2009. | |
Yoffe-Sharp BL, Loar LM. The veterinarian’s responsibility to recognize and report animal abuse. J Am Vet Med Assoc. 2009;234(6):732–737. | |
Benetato MA, Reisman R, McCobb E. The veterinarian’s role in animal cruelty cases. J Am Vet Med Assoc. 2011;238(1):31–34. | |
Arkow P. A ‘one health’ approach to ending family violence: The responsibilities of veterinary professionals in recognizing and reporting animal abuse, domestic violence, child abuse and elder abuse. In: Tiplady C, editor. Animal Abuse: Helping Animals and People. Boston (MA): CAB International; 2013:83–92. | |
Stolt LB, Johnson YJ, Kaneene JB. Attitudes of veterinarians, animal control directors, and county prosecutors in Michigan regarding enforcement of state cruelty legislation. J Am Vet Med Assoc. 1997; 211(12):1521–1523. | |
Donley L, Patronek GJ, Luke C. Animal abuse in Massachusetts: A summary of case reports at the MSPCA and attitudes of Massachusetts veterinarians. J Appl Anim Welf Sci. 1999;2(1):59–73. | |
Green PC, Gullone E. Knowledge and attitudes of Australian veterinarians to animal abuse and human interpersonal violence. Aust Vet J. 2005;83(10):619–625. | |
McKerchar H. Survey of veterinary practitioner awareness of non-accidental injury in companion animals. Soc Comp An Stud J. 2005;17(3):8–13. | |
Enns A. MVMA Public Awareness and Attitude Survey, Final Report. Winnipeg (MB): Manitoba Veterinary Medical Association; 2006. | |
Williams VM, Dale AR, Clarke N, Garrett, NKG. Animal abuse and family violence: Survey on the recognition of animal abuse by veterinarians in New Zealand and their understanding of the correlation between animal abuse and human violence. N Z Vet J. 2008;56(1):21–28. | |
The Links Group. Recognizing Abuse in Animals and Humans: Guidance for Veterinary Surgeons and Other Veterinary Employees. Milton Keynes (UK): The Group; 2013. | |
Robertson IA. Legally protecting and compelling veterinarians in issues of animal abuse and domestic violence. N Z Vet J. 2010;58(3):114–120. | |
Rollin BE. Veterinary and animal ethics. In: Wilson JF, editor. Law and Ethics of the Veterinary Profession. Yardley (PA): Priority Press; 1988:24–49. | |
Robertson I. A legal duty to report suspected animal abuse: Are veterinarians ready? In: Linzey A, editor. The Link Between Animal Abuse and Human Violence. Eastbourne (UK): Sussex Academic Press; 2009:263–272. | |
Rollin BE. Veterinary medical ethics. Can Vet J. 2007;48(5):459–462. | |
Arkow P, Boyden P, Patterson-Kane E. Practical Guidance for the Effective Response by Veterinarians to Suspected Animal Cruelty, Abuse and Neglect. Schaumburg (IL): American Veterinary Medical Association; 2011. | |
New Zealand Veterinary Association. The Veterinarians Animal Welfare Toolkit. Wellington: The Association; 2011. | |
Arkow P, Lockwood R. Definitions of animal cruelty, abuse, and neglect. In: Brewster MP, Reyes CL, editors. Animal Cruelty: A Multidisciplinary Approach to Understanding. Durham (NC): Carolina Academic Press; 2013:3–24. | |
Lacroix CA. Another weapon for combating family violence: Prevention of animal abuse. In: Ascione FR, Arkow P, editors. Child Abuse, Domestic Violence, and Animal Abuse: Linking the Circles of Compassion for Prevention and Intervention. West Lafayette (IN): Purdue University Press; 1999:62–80. | |
Blood DC, Studdert VP. Saunders Comprehensive Veterinary Dictionary. 2nd ed. London: W.B. Saunders; 1999. | |
Munro HMC, Thrusfield MV. Battered pets: features that raise suspicion of non-accidental injury. J Small Anim Pract. 2001;42(5):218–226. | |
Munro HMC, Thrusfield MV. Battered pets: non-accidental physical injuries found in dogs and cats. J Small Anim Pract. 2001;42(6):279–290. | |
Munro HMC, Thrusfield MV. Battered pets: sexual abuse. J Small Anim Pract. 2001;42(7):333–337. | |
Munro HMC, Thrusfield MV. Battered pets: Munchausen syndrome by proxy. J Small Anim Pract. 2001;42(8):385–389. | |
Tiplady C. Animal abuse case studies and treatment. In: Tiplady C, editor. Animal Abuse: Helping Animals and People. Boston (MA): CAB International; 2013:147–163. | |
Veterinary Council of New Zealand. Guidance for Veterinarians Dealing with Cases of Suspected or Actual Animal Abuse and Family Violence. Wellington: The Council; 2013. | |
Tong LJ. Fracture characteristics to distinguish between accidental injury and non-accidental injury in dogs. Vet J. 2014;199(3):392–398. | |
Colorado Veterinary Medical Association. Issue Briefing: Mandatory Reporting of Cruelty to Animals and Animal Fighting. Denver: The Association; 2007. | |
Miller L, Zawistowski S, editors. Shelter Medicine for Veterinarians and Staff. Ames (IA): Blackwell; 2004. | |
Sinclair L, Merck M, Lockwood R. Forensic Investigation of Animal Cruelty: A Guide for Veterinary and Law Enforcement Professionals. Washington: Humane Society of the United States; 2006. | |
Cooper J, Cooper M. Introduction to Veterinary and Comparative Forensic Medicine. Ames (IA): Blackwell; 2007. | |
Munro R, Munro HMC. Animal Abuse and Unlawful Killing: Forensic Veterinary Pathology. Philadelphia: Saunders; 2008. | |
Merck M. Veterinary Forensics: Animal Cruelty Investigations. 2nd ed. Ames (IA): Blackwell; 2013. | |
American Humane Association. Non-accidental Injury in Dogs and Cats in Colorado: Final Report to Animal Assistance Fund. Englewood (CO): The Association; 2003. | |
Gullone E, Johnson J, Volant A. The Link Between Animal Abuse and Family Violence: A Victoria-wide Study. Canberra: Australian Veterinary Association; 2004. | |
Patronek GJ. Animal cruelty, abuse and neglect. In: Miller L, Zawistowski S, editors. Shelter Medicine for Veterinarians and Staff. Ames (IA): Blackwell; 2004:427–452. | |
Landau R. The veterinarian’s role in recognizing and reporting abuse. In: Ascione FR, Arkow P, editors. Child Abuse, Domestic Violence, and Animal Abuse: Linking the Circles of Compassion for Prevention and Intervention. West Lafayette, (IN): Purdue University Press; 1999: 241–249. | |
Sharpe MS. A survey of veterinarians and a proposal for intervention. In: Ascione FR, Arkow P, editors. Child Abuse, Domestic Violence, and Animal Abuse: Linking the Circles of Compassion for Prevention and Intervention. West Lafayette, (IN): Purdue University Press; 1999: 250–256. | |
American Veterinary Medical Association. US Pet Ownership and Demographics Sourcebook. Schaumburg (IL): The Association; 2012. | |
Colorado Veterinary Medical Association. Issue Briefing: Mandatory Reporting of Cruelty to Animals and Animal Fighting. Denver: The Association; 2007. Available from: http://www.colovma.org/?57. | |
Veterinary Council of New Zealand, Code of Professional Conduct (2012). Available from: http://www.vetcouncil.org.nz/CPC/AnimalWelfare/CPC_AnimalWelfare_FlowChart.php. Accessed November 21, 2015. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.