")
Back to Journals » Research and Reports in Urology » Volume 15
Recent Advances in the Management of Localized and Locally Advanced Renal Cell Carcinoma: A Narrative Review
Authors Dhanji S, Wang L, Liu F , Meagher MF, Saidian A, Derweesh IH
Received 8 September 2022
Accepted for publication 28 January 2023
Published 28 February 2023 Volume 2023:15 Pages 99—108
DOI https://doi.org/10.2147/RRU.S326987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Sohail Dhanji, Luke Wang, Franklin Liu, Margaret F Meagher, Ava Saidian, Ithaar H Derweesh
Department of Urology, University of California San Diego School of Medicine, La Jolla, CA, USA
Correspondence: Ithaar H Derweesh, Department of Urology, University of California San Diego School of Medicine, 3855 Health Sciences Drive, Mail Code: 0987, La Jolla, CA, 92037, USA, Tel +1 (858) 249-0900, Fax +1 (858) 822-6188, Email [email protected]
Purpose: To review the current status of surgical and procedural treatments for renal cell carcinoma (RCC), focusing on oncological and functional outcomes, and the use of techniques for advanced disease over the last 10 years.
Findings: Partial nephrectomy (PN) has become the reference standard for most T1 and T2 masses. In cT2 RCC, PN exhibits oncological equivalence and improved functional outcomes compared to radical nephrectomy (RN). Additionally, emerging data suggest that PN may be used to treat cT3a RCC. The robot-assisted platform is increasingly used to treat locally advanced RCC. Studies suggest safety and feasibility of robotic RN and robotic inferior vena cava tumor thrombectomy. Additionally, single-port robot-assisted laparoscopic approaches are comparable to multiport approaches in select patients. Long-term data show that cryoablation, radiofrequency ablation, and microwave ablation are equipotent in management of small renal masses. Emerging data suggest that microwave may effectively treat cT1b masses.
Keywords: renal cell carcinoma, cryoablation, nephrectomy, microwave ablation, partial nephrectomy, radiofrequency ablation
Introduction
According to the World Health Organization (WHO), 431,288 new cases of renal cell carcinoma (RCC) were diagnosed in 2020. This makes RCC the 14th–most commonly diagnosed cancer and third amongst urological malignancies.1 Historically, radical nephrectomy (RN) has been the cornerstone and standard of care for treating localized RCC. Emerging data increasingly suggest that partial nephrectomy (PN) is oncologically equivalent to RN in most localized RCC and may provide benefit from nephron preservation.2–7 Furthermore, ablative strategies have emerged as a robust alternative to surgical excision in small renal masses.8–10 This review discusses advances in surgery, ablation, and minimally invasive surgery (MIS).
Methodology
We performed PubMed (http://www.ncbi.nlm.nih.gov/pubmed) searches with the keywords “partial nephrectomy”, “radical nephrectomy”, “T2”, “T3a”, “minimally invasive surgery”, “open”, “IVC tumor thrombectomy”, “nephrometry”, “single-port”, “multi-port”, “radiofrequency ablation”, “cryoablation”, “T1a”, “microwave ablation”, “T1b”, and “tumor histology” over the last 10 years. Due to limited data, we expanded our search to the past 20 years for robotic inferior vena cava (IVC) tumor thrombectomies. We selected articles that discussed oncological outcomes, functional outcomes, complication rates, and patient-satisfaction outcomes. We excluded case reports and articles not meeting these selection criteria.
Surgical Advances
Emergence of Minimally Invasive Partial Nephrectomy as Reference Standard for cT2 Tumors [Table 1]
PN has become established as the preferred definitive method of management for T1a and T1b tumors using both minimally invasive and open approaches. In recent years, emerging reports have shown that in T2 RCC, PN is equivalent to RN in oncological outcomes and superior in functional outcomes. Nonetheless, historical series and meta-analyses utilizing historical data have demonstrated significantly increased risk of complications or PN in the T2 setting when compared to RN. These data were based on primary open-approach PN.2,11–14 Contemporary analyses with robot-assisted PN (RAPN), however, suggest a decreased morbidity profile while maintaining oncological equipoise and functional benefit for PN. Bertolo et al complied a series of 298 patients with cT2a tumors who underwent PN with a median follow-up of 12 months. They reported all-cause mortality (ACM) of 3.3%, cancer-specific mortality (CSM) of 0.8%, and a recurrence rate of 10%. Functionally, these patients did have a statistically significant decrease in estimated glomerular filtration rate (eGFR) at discharge (17.5%, p<0.001). However, by 1 year, their eGFR had recovered such that there was no significant difference from the original preoperative values (p=0.2).15 Bradshaw et al performed the first study examining outcomes in a pure MIS series, performing a propensity score–matched comparison of 648 patients with cT2a tumors who underwent either RAPN (216 patients) or MIS-RN (432 patients). The authors noted that surgery type was not an independent predictor of ACM (p=0.601) or recurrence (p=0.555). Furthermore, type of surgery was not associated with a significant difference in 5-year overall survival (OS; PN 76.3% vs RN 88.0%, p=0.2221) or 5-year disease-free survival (DFS; PN 78.6% vs RN85.3%, p=0.630) for those who had pT2 masses. Nonetheless, while the authors noted that PN had a higher rate of positive surgical margins (PSMs) than RN (8.3% vs 2.6%, p=0.001), the presence of PSM was not a predictor of ACM (p=0.423) or recurrence (p=0.831). RAPN did not result in a significantly higher rate of intraoperative complications (6.9% vs 5.3%, p=0.478), major (Clavien–Dindo grade ≥III) complications (5.3% vs 2.3%, p=0.063), or 30-day readmissions (0.9% vs 2.5%, p=0.238).16 Amparore et al examined 116 patients with cT2 RCC who underwent PN (52 patients) or RN (64 patients). They found 5-year other-cause mortality (OCM) rates of 5.1% (PN) vs 6.6% (RN; p=0.9), 5-year CSM rates of 7.7% (PN) vs 16.7% (RN; p=0.08), and 5-year progression-free survival (PFS) rates of 92.2% (PN) vs 72.8% (RN; p=0.02). Surgery type was not independently associated with OCM (p=0.6), CSM (p=0.9), or PFS (p=0.7). There was no significant difference in the rates of PSM between the PN and RN cohorts (1.9% vs 3.1%, p=0.5). Furthermore, RAPN was not associated with a significantly higher rate of intraoperative transfusion (5.8% vs 4.7%, p=0.9) or major (Clavien–Dindo grade ≥III) complications (1.9% vs 0, p=0.07).17 Overall, these studies show that PN is equivalent to RN for cT2 tumors in terms of oncological outcomes and superior in terms of preserving renal function.
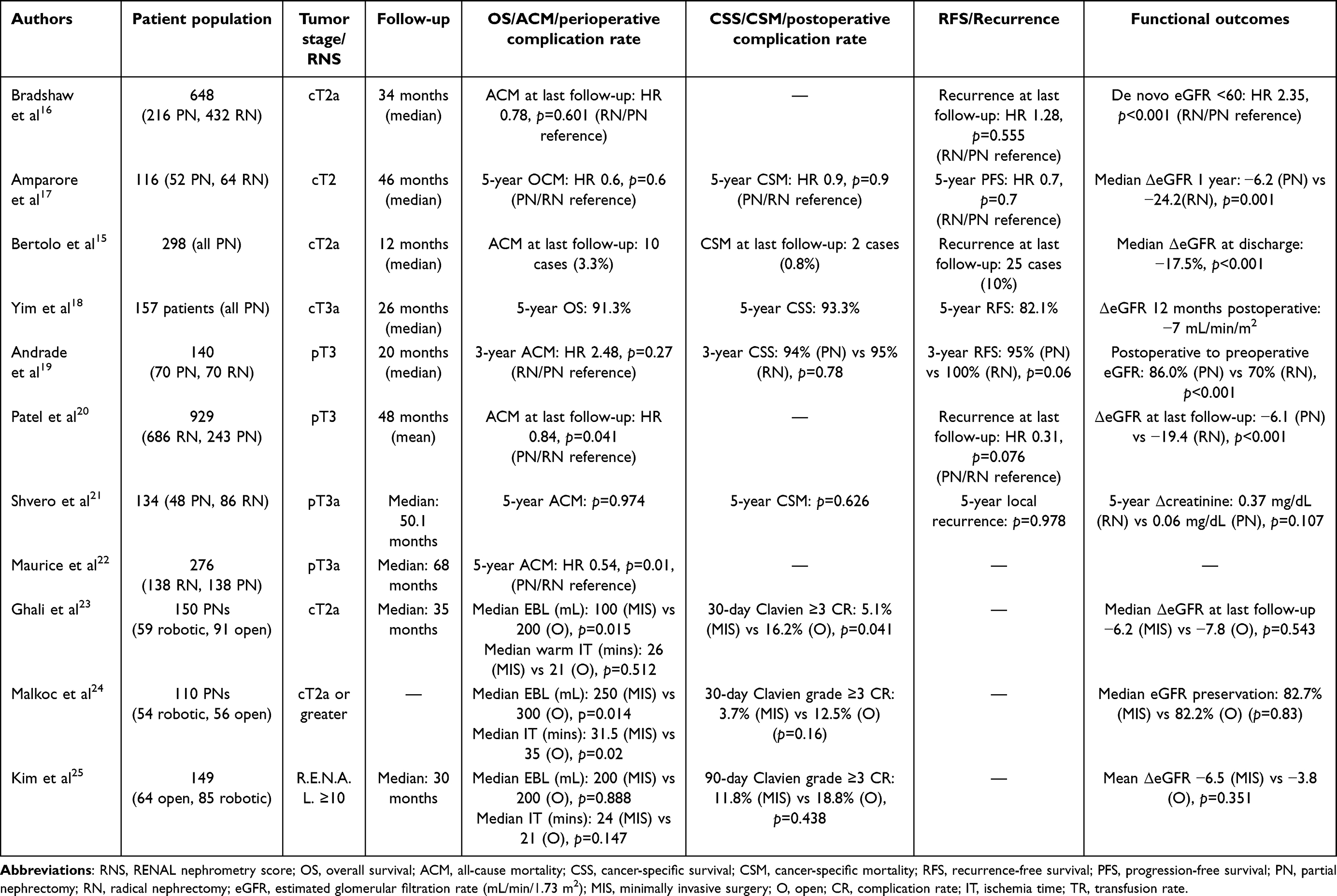 |
Table 1 Advances in minimally invasive partial nephrectomy |
Partial Nephrectomy for T3a Renal Masses [Table 1]
Extracortical extension of renal malignancy into the venous or collecting systems or perinephric or renal sinus fat (T3 RCC) have historically been viewed as a definitive indication for RN. Recent reports have examined feasibility and short-term outcomes of PN in T3a RCC. Yim et al analyzed 157 patients who underwent PN for cT3a renal masses. A total of 150 patients (95.5%) had negative margins. The 5-year recurrence-free survival (RFS), cancer-specific survival (CSS), and OS were 82.1%, 93.3%, and 91.3%, respectively. The median change in eGFR was 7 mL/min/1.72 m2, and 55.4% of patients preserved ≥90% of their eGFR. Failure to achieve the optimal outcome of negative surgical margins, warm ischemia time <25 minutes, no perioperative complications, and ≥90% eGFR preservation was associated with increasing age (OR 1.05, p<0.001), increasing BMI (OR 1.07, p=0.035), diabetes (OR 2.55, p=0.025), increasing RENAL nephrometry score (RNS) (OR 1.25, p=0.018), decreasing preoperative eGFR (OR 1.03, p=0.001), increasing operative time (OR 1.01, p=0.012), and estimated blood loss (EBL) >300 mL (OR 5.04, p=0.005).18 Additionally, Andrade et al compared patients with pT3a RCC who underwent RAPN or RARN. There were 70 patients in each cohort. Renal function preservation was significantly higher in the PN cohort (86% vs 70%, p<0.001). The estimated 3-year OS (90% vs 84%, p=0.42, CSS (94% vs 95%, p=0.78), and RFS (95% vs 100%, p=0.06) were similar in the PN and RN cohorts.19
Several studies have analyzed outcomes of patients who were pathologically upstaged from cT1–2 to pT3a. Patel et al analyzed 929 such patients who underwent either RN (n=686) or PN (n=243). Multivariate analysis showed that surgery type was not a significant predictor of recurrence. Kaplan–Meier analysis showed 5-year RFS for cT1-upstaged PN, cT1-upstaged RN, cT2-upstaged PN, and cT2-upstaged RN of 79%, 74%, 70%, and 51%, respectively (log-rank p<0.001). Five-year OS for cT1-upstaged PN, cT1-upstaged RN, cT2-upstaged PN, and cT2-upstaged RN was 64%, 65.2%, 56.4%, and 55.2%, respectively (log-rank p=0.059). Additionally, eGFR decreased less with PN than RN (6.1 vs 19.4 mL/min/1.73 m2, p<0.001).20 Shvero et al performed a similar study with 134 patients who were pathologically upstaged from cT1–2 to pT3 after PN or RN. Their multivariate analysis showed that surgery type was not a predictor of local recurrence (p=0.978), metastatic progression (p=0.972), CSM (p=0.626), or ACM (p=0.974) at 5-year follow-up. It is important to note that there was a significant difference in median tumor size between the PN and RN cohorts (4 cm vs 7 cm, p<0.001).21 Finally, Maurice et al analyzed 276 patients with tumors that were pathologically upstaged to T3a who underwent PN (138 patients) or RN (138 patients). With a median follow-up of 68 months, they found that PN was associated with significantly less risk of ACM (HR 0.54, p=0.01).22 The findings from the aforementioned studies suggest that patients with cT3 RCC with indication for PN may have acceptable short- to intermediate-term outcomes, and that PN is an appropriate option in patients with T3 tumors and with indication for nephron preservation.
Open PN vs MIS PN for Large (T2+) and Complex Renal Masses [Table 1]
While emerging reports suggest the feasibility of MIS-PN for large and complex masses, direct comparisons of open and MIS approaches have been few. Ghali et al examined 150 patients with cT2a RCC who underwent open PN (91) or MIS PN (59). They found no significant difference in the perioperative complication rate, postoperative Clavien grade ≤2 complication rate, or median change in eGFR at follow-up. However, there was a higher rate of Clavien grade 3 or higher complications in those who underwent open PN (16.2%) than those who underwent MIS PN (5.1%; p=0.041).23 Malkoc et al reported a similar study of 110 patients with tumors ≥7 cm who underwent open PN (56) or MIS PN (54). The MIS PN cohort demonstrated lower EBL (250 mL vs 300 mL, p=0.014), median ischemia time (31.5 min vs 35 min, p=0.02), median hospitalization time (3.5 days vs 5.3 days, p<0.001), and intraoperative transfusion rate (9.4% vs 30.4%, p=0.008). However, there was no significant difference between the cohorts in intraoperative complication rate, postoperative complication rate, or eGFR preservation.24 Taken together, these reports suggest that MIS-PN has similar functional outcomes to open PN for large masses and may be associated with benefit with respect to decreased blood loss and morbidity.
Utilization of nephron-sparing surgery has historically been limited in patients with complex renal masses, with concerns about increased risk of complications and oncological risk. One method of measuring tumor complexity is through RNSs. Kim et al examined 149 patients with RNSs ≥10 who underwent open PN (64) or MIS PN (85). They found only lower median hospital stay for their MIS PN patients (5 days vs 7 days, p<0.001). They found no significant difference between the two cohorts in median EBL, median ischemia time, intraoperative complications, intraoperative transfusions, postoperative complication rates, or mean eGFR decrease.25 Although retrospective studies comparing surgical techniques are inherently susceptible to selection bias, these studies together suggest that in certain scenarios, MIS PN may confer a lower risk of intraoperative complications in patients undergoing PN for cT2 masses and those with complex renal mass. However, it remains to be determined if MIS confers a lower rate of postoperative complications for these patients and whether it is beneficial for those with RNSs ≥10 in elective circumstances.
Evolution of Robotic RN for Inferior Vena Cava Tumor Thrombi (TT) [Table 2]
RCCs may invade the renal vein and extend into the IVC cephalad into the right atrium. Tumor thrombi (TT) such as these occur in roughly 5%–15% of all RCC.26 These operations carry significant risk of major operative and postoperative complications and mortality and are considered high-risk procedures that often require an interdisciplinary team with urological oncologists, hepatobiliary surgeons, and cardiothoracic surgeons for optimal management, which has historically been an extensive multichambered abdominal and sometimes thoracic operation. However, in the last 15–20 years, minimally invasive techniques and platforms have been increasingly applied to this challenging oncological phenomenon. Abaza et al performed five robot-assisted, right-sided RNs with IVC thrombectomy (IVCTE). Two of the patients had Mayo level I (≤2 cm from the confluence of the renal vein and IVC) TT and three patients had level II (>2 cm from the confluence of the renal vein and IVC but below the hepatic veins) TT. There were no complications, transfusions, or readmissions.27 Wang et al also reported a series of 17 RARNs with IVCTE. Thirteen cases were right-sided and four left-sided. Median operating times were 131 min and 250 mins for the right and left sides, respectively. For left-sided procedures, the median warm ischemia time was 18 minutes.28 Abaza et al went on to combine his results with others in a multi-institutional case series examining 32 cases of RARN with IVCTE. Thirty of these cases were level I TT and two level II TT, and 27 were right-sided and five left-sided. All of the procedures were performed without open conversion. Three patients required 1–3 units of blood. After mean follow-up of 15.4 months, seven patients’ had tumors recurred. However, of these seven, four had node-positive disease on postlymphadenectomy pathological examination.29 Chopra et al analyzed operative success and 1-year outcomes in 24 patients with Mayo level II and III (above the hepatic veins, but below the diaphragm) IVC TT who underwent RARN with IVCTE. Sixteen cases were right-sided and seven left-sided. MIS was successful in all but one patient, who required open conversion. All tumors were excised with negative surgical margins. Five patients required intraoperative blood transfusion, and four had complications (two Clavien 2, one Clavien 3a, and one Clavien 3b). Of the 24 patients who underwent successful MIS, three had positive lymph nodes. At 1-year follow-up, eleven patients had metastatic disease and ten had received adjuvant therapy.30 Wang et al performed a similar study with 13 patients who underwent RARN with Mayo level III–IV (above the diaphragm) IVCTE. Nine cases were right-sided and four left-sided. They performed all surgeries without needing to convert to an open approach. Three patients had grade IV complications. The perioperative mortality rate was 7.7%. In the following 18 months, two patients died and one had disease progression.31 These case series have demonstrated that a minimally invasive approach is feasible for patients with RCC and level I–IV TT. However, further clinical investigations are required to delineate the role of minimally invasive versus open IVCTE in terms of short- and long-term oncological outcomes and complication rates.
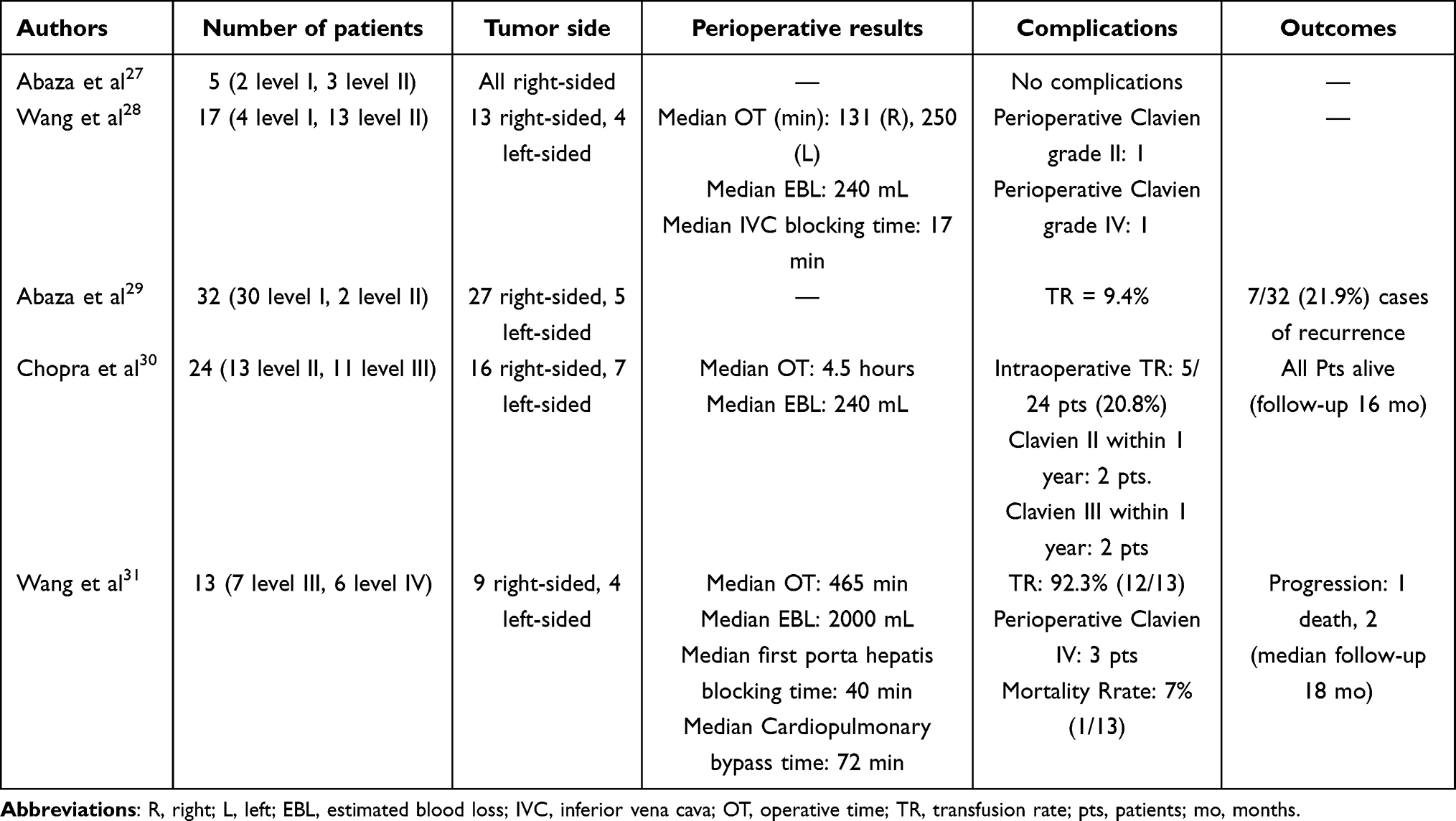 |
Table 2 Evolution of robotic radical nephrectomy with inferior vena cava tumor thrombectomy |
Single-Port vs Multiport MIS PN [Table 3]
Single-port (SP) laparoscopic surgery emerged in the last 15 years as a potential minimally invasive alternative to traditional multiport approaches that may further reduce incisional morbidity and promote improved cosmesis.32 Patients undergoing SP nephrectomy have similar operative outcomes with higher cosmetic satisfaction than those who underwent a multiport (MP) nephrectomy, with cosmetic benefit derived by consolidation of working ports and extraction incision into a discrete periumbilical or Pfannenstiel incision.33,34 Nonetheless, adoption of pure laparoscopic platforms has been hindered by a technology gap with respect to robust and wristed instrumentation and the difficulty of training surgeons in this approach.35 Development of the DaVinci SP robotic platform (Intuitive, Sunnyvale, USA) has led to renewed interest in and application of SP robotic approaches for a variety of procedures, including PN and RN. Harrison et al set out to determine if there was a tangible benefit to either technology using propensity score–matched cohorts of 48 patients who underwent SP or MP MIS PN for renal tumors ≤4 cm. They found no significant difference in median operative time, median EBL, intraoperative complications, or postoperative complications. However, they did find that those who underwent SP PN had significantly shorter median hospital stay (1.4 days vs 1.6 days, p=0.0045) and lower median opioid use on postoperative day 1 (4.6 MME vs 9.8 MME, p=0.0209).36 Glaser et al also attempted to establish whether one technique was preferable when they examined 78 patients who underwent either SP PN (26) or MP PN (52). They found no significant differences between the two cohorts in mean operative time, rate of EBL >500 mL, complication rates, rate of discharge on postoperative day 1, or rates of opioid prescriptions being filled.37 Currently, there seems to be little tangible benefit to using an SP in lieu of MP technique when performing PN. SP PN may lead to shorter hospital stays and less opioid dependence, but further investigation is warranted.
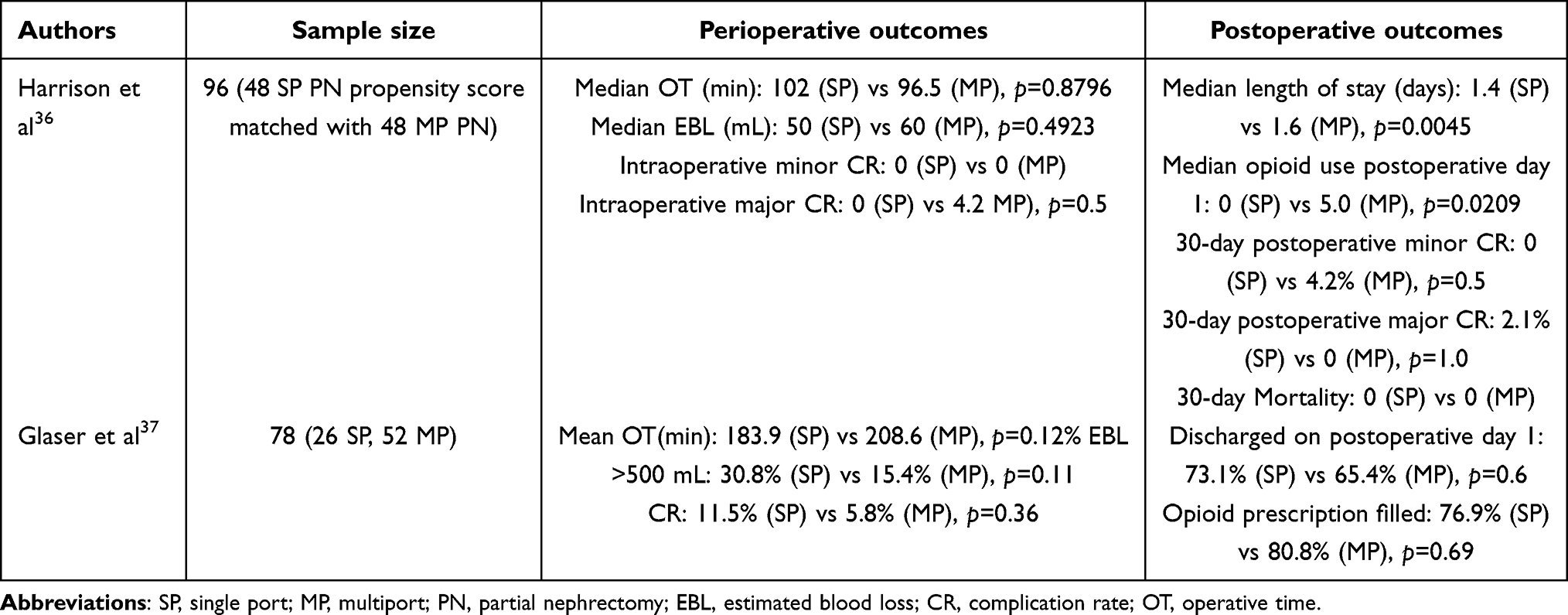 |
Table 3 Emergence of robotic single-port partial nephrectomy |
Advances in Thermal Ablation
Long-Term Functional and Oncological Outcomes for Cryoablation and Radiofrequency Ablation [Table 4]
In recent years, ablative techniques, including radiofrequency ablation (RFA) and cryoablation (CA), have become established options for patients with select small renal masses who are not optimal surgical candidates or who prefer a minimally invasive nonsurgical approach, with reports demonstrating oncological efficacy. Psutka et al examined 185 patients (143 T1a and 42 T1b) treated with RFA. On follow-up, there were 12 cases of recurrence (6.5%) with a median time to recurrence of 2.5 years. T1b masses were significantly more likely to recur than T1a masses (14.3% vs 4.2%, p=0.0196).38 Takaki et al analyzed 60 patients with T1b renal masses treated with RFA (21) or RN (39). The patients in the RFA cohort had significantly higher age, rate of chronic kidney disease, and American Society of Anesthesiologists scores, while the RN cohort had significantly larger tumors. Despite this, there was no significant difference between the two cohorts in 10-year RFS or 10-year CSS. In the RFA cohort, there was no significant difference between baseline eGFR and eGFR at last follow-up. In the RN cohort, there was a significant decrease in eGFR (88.4 mL/min/1.73 m2 vs 59.6 mL/min/1.73 m2, p<0.001). It is important to note that the RFA cohort had significantly lower 10-year OS (48% vs 97%, p<0.009), although it is unclear how much of that difference was due to patient selection bias.39 Ma et al analyzed 58 T1a renal tumors treated with RFA, and 5- and 10-year RFS was 94.2%. Three (5.1%) patients died during the follow-up, which translates to 5- and 10-year OS of 95.7% and 91.1%.40 Knox et all analyzed 234 biopsy-proven T1a/T1b RCCs that were treated with CA. Complete response to CA occurred following one session in 195 of 204 tumors and following two sessions in 200 of 204 tumors. There were three cases of recurrence in the 200 cases followed up (1.5%) and ten cases of metastatic progression out of the 193 eligible cases (5.2%). Variables associated with metastatic progression were tumor size, prior kidney surgery, and clear-cell histology. The ACM rate was 2.7%. With regard to functional preservation, there was a significant difference in eGFR at baseline and follow-up (70.32 vs 68.17 mL/min/1.73 m2, p=0.01).41 Pecoraro et al utilized the SEER (Surveillance, Epidemiology, and End Results) database to analyze 5763 patients with T1b RCC, 5521 of whom were treated with PN and 242 with CA. They found that CA was a significant predictor of CSM (HR 2.50, p=0.03) and a relative risk factor of OCM (HR 1.45, p=0.12).42 The current state of the literature supports utilization of CA and RFA for management of T1a tumors with durable outcomes in patients with tumors <3.5 cm in size that are comparable with surgical excision; however, outcomes in T1b RCC are significantly worse with ablative modalities and utilization of CA, and RFA for T1b tumors should only be considered in circumstances where excisional therapy is contraindicated due to significant systemic risk to the patient.
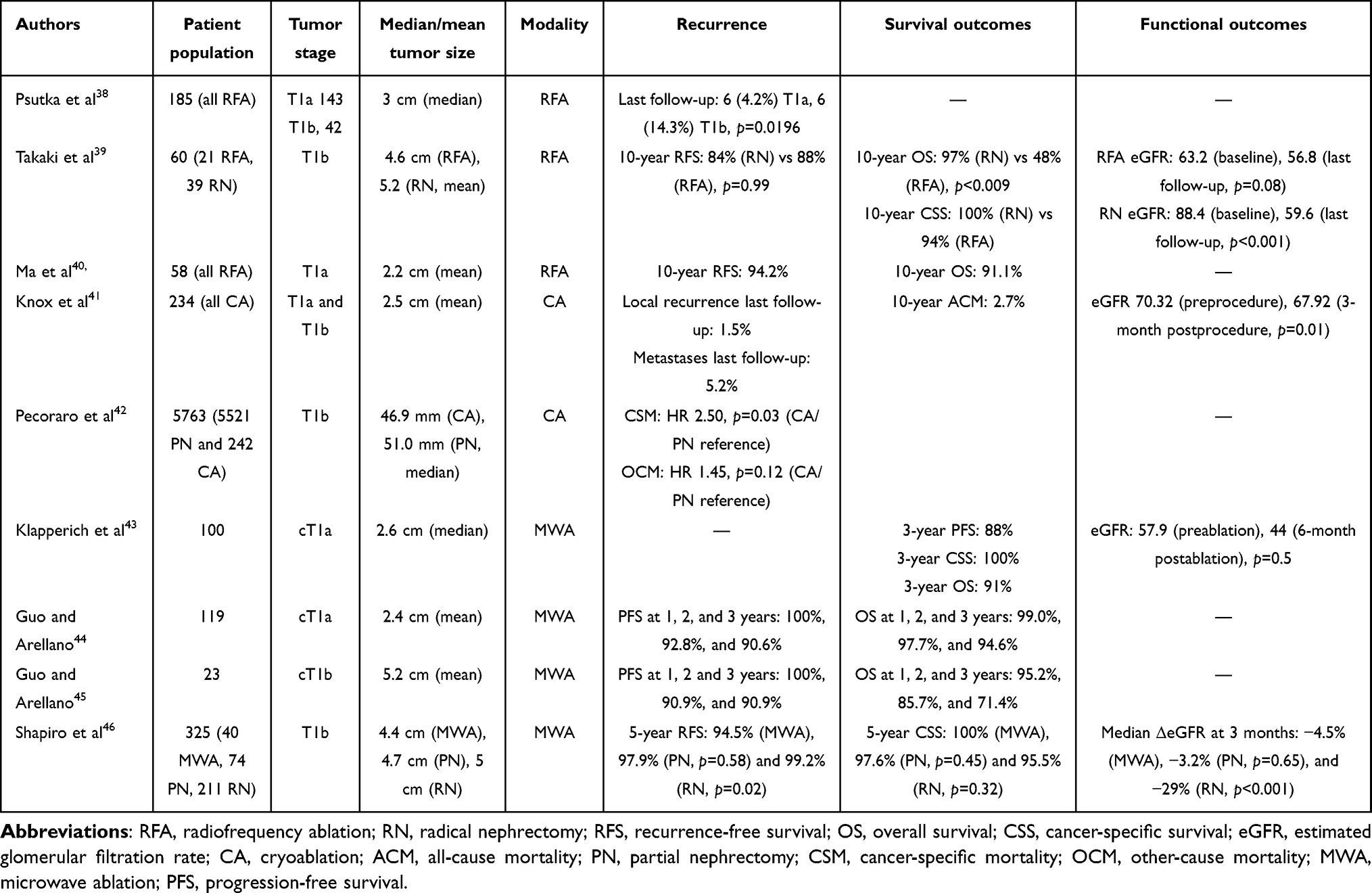 |
Table 4 Advances in ablation |
Emergence of Microwave Therapy [Table 4]
Microwave ablation (MWA) has emerged as an alternative ablative platform to RFA and CA, with promising short- and intermediate-term outcomes in T1 RCC. Klapperich et al analyzed 100 patients with T1a masses who underwent MWA. Technical success was achieved in all patients, and 3-year RFS was 99%. Three-year PFS, CSS, and OS was 88%, 100, and 91%, respectively. Additionally, there was no significant difference in eGFR at baseline and postablation (57.9 mL/min/1.73 m2 vs 44 mL/min/1.73 m2, p=0.5).43 Guo and Arellano performed two studies that analyzed the outcomes of patients with T1a and T1b masses following MWA. In their first study, they analyzed 119 patients with cT1a masses and found a complete response to MWA in 95.3% of cases. Additionally, they reported PFS of 100%, 92.8%, and 90.6% at 1, 2, and 3 years and OS of 99.0%, 97.7% and 94.6% at 1, 2, and 3 years, respectively.44 In their second study, they analyzed 23 patients with cT1b masses. Complete response was achieved in 87% of patients on the first attempt and 100% of patients on the second attempt. At 1, 2, and 3 years, PFS was 100%, 90.9%, and 90.9% and OS 95.2%, 85.7%, and 71.4%, respectively.45 Shapiro et al analyzed a group of 325 patients with T1b RCC who underwent RN (211), PN (74), or MWA (40). The 5-year RFS for MWA (94.5%) was noninferior when compared to PN (97.9%, p=0.58), but significantly lower than RN (99.2%, p=0.02). Nonetheless, the 5-year CSS for the MWA cohort (100%) was not significantly different from the PN (97.6%, p=0.45) or RN one (95.5%, p=0.32).46 Taken together, the current state of the literature reflects short- to intermediate-term outcomes in MWA that are promising for T1 RCC, suggesting efficacy in the T1b and T1a cohorts of patients. Nonetheless, longer-term follow-up data are required to confirm durability of outcomes.
Conclusion
In this review, we discussed advances in the surgical and ablative treatment of RCC. RAPN has become the reference standard for most T2 masses because of its oncological equipoise and functional preservation when compared to RN. PN may also be utilized for selected clinical T3a renal masses with imperative indication for functional preservation. Additionally, a robotic approach to PN has been shown to have improved morbidity when compared to open PN, which is comparable to the morbidity profile of RN for large and complex masses. Emerging reports suggest that RARN with IVC TT is feasible for select patients, with benefits of MIS and acceptable short-term oncological outcomes. Robotic SP PN has been shown to demonstrate improved cosmesis with the possibility of shorter hospital stays and improved postoperative pain, although this must be confirmed with further investigation. In the field of thermal ablation, different energy approaches, such as CA, RFA, and MWA, have demonstrated acceptable efficacy for tumors <3 cm, while only MWA has shown acceptable short-term outcomes in larger (T1b) masses. Further investigation is necessary to establish the role of MWA for management for T1b masses. These data reflect the current state of the art of the field, though the analyses are limited by their retrospective nature and selection bias, and in the case of the surgical series, the analyses were conducted in high-volume centers of excellence by experienced surgeons, and as such, the applicability of the data may be limited, but serve as the starting point for further investigation.
Summary
Nephron-sparing and minimally invasive surgery has become increasingly effective for management of large renal masses. Ablative techniques are now feasible alternatives in select patients.
Future Directions
Future studies should be aimed at establishing the extent of disease that can be sufficiently treated with PN vs RN, which is best carried out via a randomized clinical trial.47 It remains unclear whether PN for patients beyond T2 disease confers a functional and mortality benefit compared to RN. Additionally, it is unclear whether an MIS approach for tumors with IVC extension is adoptable beyond centers of excellence. SP MIS for RCC should be further investigated to examine any potential differences in complication rates and satisfaction outcomes. With regard to ablation, MWA must be further explored before being deemed a safe alternative treatment for T1b RCC. Further investigation is needed to establish how tumor histology and complexity affects response to different ablation techniques.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Kidney: Intenational Agency for Research on Cancer ; 2020. Available from: https://gco.iarc.fr/today/data/factsheets/cancers/29-Kidney-fact-sheet.pdf.
2. Mir MC, Derweesh I, Porpiglia F, Zargar H, Mottrie A, Autorino R. Partial nephrectomy versus radical nephrectomy for clinical T1b and T2 renal tumors: a systematic review and meta-analysis of comparative studies. Eur Urol. 2017;71(4):606–617. doi:10.1016/j.eururo.2016.08.060
3. Campell SC, Clark PE, Chang SS, et al. Renal mass and localized renal cancer: evaluation, management, and follow-up: AUA Guideline Part I. J Urol. 2021;206:199. doi:10.1097/JU.0000000000001911
4. Campbell SC, Uzzo RG, Karam JA, et al. Renal mass and localized renal cancer: evaluation, management, and follow-up: AUA Guideline: part II. J Urol. 2021;206:209. doi:10.1097/JU.0000000000001912
5. Ljungberg B, Albiges L, Abu-Ghanem Y, et al. European association of urology guidelines on renal cell carcinoma: the 2022 update. Eur Urol. 2022;82(4):399–410. doi:10.1016/j.eururo.2022.03.006
6. Miller DC, Schonlau M, Litwin MS, Lai J, Saigal CS. Urologic Diseases in America Project. Renal and cardiovascular morbidity after partial or radical nephrectomy. Cancer. 2008;112(3):511–520. doi:10.1002/cncr.23218
7. Kim SP, Thompson RH, Boorjian SA, et al. Comparative effectiveness for survival and renal function of partial and radical nephrectomy for localized renal tumors: a systematic review and meta-analysis. J Urol. 2012;188(1):51–57. doi:10.1016/j.juro.2012.03.006
8. McCarthy CJ, Gervais DA. Decision Making: thermal Ablation Options for Small Renal Masses. Semin Intervent Radiol. 2017;34(2):167–175. doi:10.1055/s-0037-1602708
9. Pierorazio PM, Johnson MH, Patel HD, et al. Management of Renal Masses and Localized Renal Cancer: systematic Review and Meta-Analysis. J Urol. 2016;196(4):989–999. doi:10.1016/j.juro.2016.04.081
10. Alam R, Patel HD, Osumah T, et al. Comparative effectiveness of management options for patients with small renal masses: a prospective cohort study. BJU Int. 2019;123(1):42–50. doi:10.1111/bju.14490
11. Klett DE, Tsivian M, Packiam VT, et al. Partial versus radical nephrectomy in clinical T2 renal masses. Int J Urol. 2021;28(11):1149–1154. doi:10.1111/iju.14664
12. Kopp RP, Mehrazin R, Palazzi KL, et al. Survival outcomes after radical and partial nephrectomy for clinical T2 renal tumours categorised by R.E.N.A.L. nephrometry score. BJU Int. 2014;114(5):708–718. doi:10.1111/bju.12580
13. Breau RH, Crispen PL, Jimenez RE, Lohse CM, Blute ML, Leibovich BC. Outcome of stage T2 or greater renal cell cancer treated with partial nephrectomy. J Urol. 2010;183(3):903–908. doi:10.1016/j.juro.2009.11.037
14. Long CJ, Canter DJ, Kutikov A, et al. Partial nephrectomy for renal masses ≥ 7 cm: technical, oncological and functional outcomes. BJU Int. 2012;109(10):1450–1456. doi:10.1111/j.1464-410X.2011.10608.x
15. Bertolo R, Autorino R, Simone G, et al. Outcomes of Robot-assisted Partial Nephrectomy for Clinical T2 Renal Tumors: a Multicenter Analysis (ROSULA Collaborative Group). Eur Urol. 2018;74(2):226–232. doi:10.1016/j.eururo.2018.05.004
16. Bradshaw AW, Autorino R, Simone G, et al. Robotic partial nephrectomy vs minimally invasive radical nephrectomy for clinical T2a renal mass: a propensity score-matched comparison from the ROSULA (Robotic Surgery for Large Renal Mass) Collaborative Group. BJU Int. 2020;126(1):114–123. doi:10.1111/bju.15064
17. Amparore D, Pecoraro A, Piramide F, et al. Comparison between minimally-invasive partial and radical nephrectomy for the treatment of clinical T2 renal masses: results of a 10-year study in a tertiary care center. Minerva Urol Nephrol. 2021;73(4):509–517. doi:10.23736/S2724-6051.21.04390-1
18. Yim K, Aron M, Rha KH, et al. Outcomes of Robot-assisted Partial Nephrectomy for Clinical T3a Renal Masses: a Multicenter Analysis. Eur Urol Focus. 2021;7(5):1107–1114. doi:10.1016/j.euf.2020.10.011
19. Andrade HS, Zargar H, Akca O, et al. Is Robotic Partial Nephrectomy Safe for T3a Renal Cell Carcinoma? Experience of a High-Volume Center. J Endourol. 2017;31(2):153–157. doi:10.1089/end.2016.0622
20. Patel SH, Uzzo RG, Larcher A, et al. Oncologic and Functional Outcomes of Radical and Partial Nephrectomy in pT3a Pathologically Upstaged Renal Cell Carcinoma: a Multi-institutional Analysis. Clin Genitourin Cancer. 2020;18(6):e723–e729. doi:10.1016/j.clgc.2020.05.002
21. Shvero A, Nativ O, Abu-Ghanem Y, et al. Oncologic Outcomes of Partial Nephrectomy for Stage T3a Renal Cell Cancer. Clin Genitourin Cancer. 2018;16(3):e613–e617. doi:10.1016/j.clgc.2017.10.016
22. Maurice MJ, Zhu H, Kim S, Abouassaly R. Survival after partial and radical nephrectomy for high-risk disease: a propensity-matched comparison. Can Urol Assoc J. 2016;10(9–10):E282–E289. doi:10.5489/cuaj.3707
23. Ghali F, Elbakry AA, Hamilton ZA, et al. Robotic partial nephrectomy for clinical T2a renal mass is associated with improved trifecta outcome compared to open partial nephrectomy: a single surgeon comparative analysis. World J Urol. 2020;38(5):1113–1122. doi:10.1007/s00345-019-02994-2
24. Malkoc E, Ramirez D, Kara O, et al. Robotic and open partial nephrectomy for localized renal tumors larger than 7 cm: a single-center experience. World J Urol. 2017;35:781–787. doi:10.1007/s00345-016-1937-9
25. Kim JK, Lee H, Oh JJ, et al. Comparison of robotic and open partial nephrectomy for highly complex renal tumors (RENAL nephrometry score ≥10). PLoS One. 2019;14(1):e0210413. doi:10.1371/journal.pone.0210413
26. Chiappini B, Savini C, Marinelli G, et al. Cavoatrial tumor thrombus: single-stage surgical approach with profound hypothermia and circulatory arrest, including a review of the literature. J Thorac Cardiovasc Surg. 2002;124(4):684–688. doi:10.1067/mtc.2002.124295
27. Abaza R. Initial series of robotic radical nephrectomy with vena caval tumor thrombectomy. Eur Urol. 2011;59(4):652–656. doi:10.1016/j.eururo.2010.08.038
28. Wang B, Li H, Ma X, et al. Robot-assisted Laparoscopic Inferior Vena Cava Thrombectomy: different Sides Require Different Techniques. Eur Urol. 2016;69(6):1112–1119. doi:10.1016/j.eururo.2015.12.001
29. Abaza R, Shabsigh A, Castle E, et al. Multi-Institutional Experience with Robotic Nephrectomy with Inferior Vena Cava Tumor Thrombectomy. J Urol. 2016;195(4 Pt 1):865–871. doi:10.1016/j.juro.2015.09.094
30. Chopra S, Simone G, Metcalfe C, et al. Robot-assisted Level II-III Inferior Vena Cava Tumor Thrombectomy: step-by-Step Technique and 1-Year Outcomes. Eur Urol. 2017;72(2):267–274. doi:10.1016/j.eururo.2016.08.066
31. Wang B, Huang Q, Liu K, et al. Robot-assisted Level III-IV Inferior Vena Cava Thrombectomy: initial Series with Step-by-step Procedures and 1-yr Outcomes. Eur Urol. 2020;78(1):77–86. doi:10.1016/j.eururo.2019.04.019
32. Huang MM, Schwen ZR, Biles MJ, et al. A comparative analysis of surgical scar cosmesis based on operative approach for radical prostatectomy. J Endourol. 2021;35:138–143. doi:10.1089/end.2020.0649
33. Kopp RP, Silberstein JL, Derweesh IH. Laparo-endoscopic single-site (LESS) radical nephrectomy with renal vein thrombectomy: initial report. BMC Urol. 2010;10:8. doi:10.1186/1471-2490-10-8
34. Richstone L, Rais-Bahrami S, Waingankar N, et al. Pfannenstiel laparoendoscopic single-site (LESS) vs conventional multiport laparoscopic live donor nephrectomy: a prospective randomized controlled trial. BJU Int. 2013;112(5):616–622. doi:10.1111/bju.12202
35. Derweesh IH. Whither the long march of LESS. J Urol. 2012;187(5):1531–1532. doi:10.1016/j.juro.2012.02.010
36. Harrison R, Ahmed M, Billah M, et al. Single-port versus multiport partial nephrectomy: a propensity-score-matched comparison of perioperative and short-term outcomes. J Robot Surg. 2022. doi:10.1007/s11701-022-01415-8
37. Glaser ZA, Burns ZR, Fang AM, et al. Single- versus multi-port robotic partial nephrectomy: a comparative analysis of perioperative outcomes and analgesic requirements. J Robot Surg. 2022;16(3):695–703. doi:10.1007/s11701-021-01271-y
38. Psutka SP, Feldman AS, McDougal WS, McGovern FJ, Mueller P, Gervais DA. Long-term oncologic outcomes after radiofrequency ablation for T1 renal cell carcinoma. Eur Urol. 2013;63(3):486–492. doi:10.1016/j.eururo.2012.08.062
39. Takaki H, Soga N, Kanda H, et al. Radiofrequency ablation versus radical nephrectomy: clinical outcomes for stage T1b renal cell carcinoma. Radiology. 2014;270(1):292–299. doi:10.1148/radiol.13130221
40. Ma Y, Bedir S, Cadeddu JA, Gahan JC. Long-term outcomes in healthy adults after radiofrequency ablation of T1a renal tumours. BJU Int. 2014;113(1):51–55. doi:10.1111/bju.12366
41. Knox J, Kohlbrenner R, Kolli K, et al. Intermediate to Long-Term Clinical Outcomes of Percutaneous Cryoablation for Renal Masses. J Vasc Interv Radiol. 2020;31(8):1242–1248. doi:10.1016/j.jvir.2020.02.021
42. Pecoraro A, Palumbo C, Knipper S, et al. Cryoablation Predisposes to Higher Cancer Specific Mortality Relative to Partial Nephrectomy in Patients with Nonmetastatic pT1b Kidney Cancer. J Urol. 2019;202(6):1120–1126. doi:10.1097/JU.0000000000000460
43. Klapperich ME, Abel EJ, Ziemlewicz TJ, et al. Effect of Tumor Complexity and Technique on Efficacy and Complications after Percutaneous Microwave Ablation of Stage T1a Renal Cell Carcinoma: a Single-Center, Retrospective Study. Radiology. 2017;284(1):272–280. doi:10.1148/radiol.2016160592
44. Guo J, Arellano RS. Percutaneous Microwave Ablation of Category T1a Renal Cell Carcinoma: intermediate Results on Safety, Technical Feasibility, and Clinical Outcomes of 119 Tumors. AJR Am J Roentgenol. 2021;216(1):117–124. doi:10.2214/AJR.20.22818
45. Guo J, Arellano RS. Percutaneous Microwave Ablation of Stage T1b Renal Cell Carcinoma: short-Term Assessment of Technical Feasibility, Short-Term Oncologic Outcomes, and Safety. J Endourol. 2020;34(10):1021–1027. doi:10.1089/end.2020.0382
46. Shapiro DD, Wells SA, Best SL, et al. Comparing Outcomes for Patients with Clinical T1b Renal Cell Carcinoma Treated With Either Percutaneous Microwave Ablation or Surgery. Urology. 2020;135:88–94. doi:10.1016/j.urology.2019.09.024
47. Weight CJ, Miller DC, Campbell SC, Derweesh IH, Lane BR, Messing EM. The management of a clinical t1b renal tumor in the presence of a normal contralateral kidney. J Urol. 2013;189(4):1198–1202. doi:10.1016/j.juro.2013.01.030
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.