")
Back to Journals » Cancer Management and Research » Volume 14
Recent Advancements in the Treatment of Rectal Gastrointestinal Stromal Tumor: In Era of Imatinib
Authors Qu H, Xu ZH, Ren YY, Gong ZZ, Ju RH , Zhang F, Kang HN, Xu Y, Chen X
Received 22 December 2021
Accepted for publication 18 February 2022
Published 16 March 2022 Volume 2022:14 Pages 1141—1152
DOI https://doi.org/10.2147/CMAR.S352860
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Hui Qu,1,2 ZhaoHui Xu,1,2 YanYing Ren,1 ZeZhong Gong,1,2 Ri Hyok Ju,1,2 Fan Zhang,1 HaoNan Kang,1,2 Yang Xu,1,2 Xin Chen1
1Department of Hernia and Colorectal Surgery, The Second Hospital of Dalian Medical University, Dalian, 116023, People’s Republic of China; 2Dalian Medical University, Dalian, People’s Republic of China
Correspondence: Xin Chen, Tel +86 17709872266, Email [email protected]
Abstract: Gastrointestinal stromal tumors (GIST) are the most common mesenchymal tumor of the gastrointestinal tract, with an annual incidence of 10– 15 cases per million. However, rectal GIST has a low incidence, accounting for approximately 0.1% of all rectal tumors. The treatment of rectal GISTs is still controversial and the relative unified guidelines and consensus opinions are inadequate. Treatment is based primarily on the clinical experience of the physician. The widespread application of neoadjuvant imatinib therapy allows diversification of treatment, especially in the choice of surgical methods. Herein, we reviewed the most recent literature and summarized the new progress in rectal tumor treatment, with the aim of providing patients with more systematic and individualized therapeutic strategies.
Keywords: gastrointestinal stromal tumors, GIST, rectum, laparoscopy, surgery, neoadjuvant imatinib
Introduction
Gastrointestinal stromal tumor (GIST), as the most common mesenchymal tumor of the gastrointestina tract, the annual incidence is 10–15 cases per million.1 GISTs are believed to originate from the pacemaker cells in the intestinal tract called Cajal interstitial cells. Activating mutations of KIT or PDGFRA oncogenes are considered the key molecular drivers of GIST pathogenesis.2 Most GISTs originate in the stomach (50–60%), followed by the small intestine (20–30%), the colon or rectum (5–10%), the esophagus (<5%), and occasionally outside the gastrointestinal tract.3 Rectal GISTs are very rare with a low incidence, accounting for approximately 0.1% of all rectal tumors.4 Given the anatomical characteristics, including a narrow, deep pelvis and the vicinity to the sphincter or invasions of other organs, these factors make surgery difficult. Surgical resection without lymph nodes resection is still the most standard method treatment for local rectal GISTs. The selection of surgical methods for rectal GIST remains controversial. Laparoscopic surgery and minimally invasive surgery for rectal GIST are both safe and feasible, not only for improving prognosis but also for preserving the patient’s quality of life. Recent studies have also focused on the efficacy of combined treatment for rectal GIST, including perioperative treatment with imatinib mesylate (IM). This article reviews the current treatment of rectal GIST.
Treatment of Rectal GISTs
Local Rectal GISTs
Resectable Rectal GISTs: Surgery
As in any other GISTs, surgical resection without lymph nodes resection is the most standard treatment method for GISTs. The achievement of histologically negative margins in the surgical management has been confirmed beneficial for resectable rectal GIST.5 Complete resection, as the key procedure in the treatment of rectal GIST, can ensure total tumor resection and avoid tumor rupture.6 However, the choice of the surgical procedure remains controversial. Low rectal GISTs are a particular challenge because radical resection is associated with significant morbidity, and when the sphincter or pelvic floor muscles become involved, abdominal perineal resection and permanent colostomy are required. Given that local GIST does not require lymph node removal and that radical excision beyond the mesentery for local GIST is associated with more complications, there is growing enthusiasm for local excision of these lesions. Several studies have also compared local resection (LR) with residual section (RE) and found the superiority of LR with a shorter operative time, less bleeding, and a rapid recovery, while oncology outcomes are similar. LR is an effective procedure for rectal GIST resection and warrants clinical endorsement.7,8 Various surgical techniques for LR have been widely described for the therapy of rectal GIST, including traditional transanal, transanal minimally invasive endoscopy,9 transacral, the perineal resection, and the transvaginal approach.
Transanal (TA) resection was first described by Parks as an alternative treatment for some rectal tumors in 1970.10 An early study revealed that traditional transanal (TA) resection can preserve anal function to the maximum extent possible in low- and mid-rectal lesions with a negative margin.11 The study compared transanal with none transanal in the treatment of rectal GIST. TA resection has a minimally invasive effect, fewer postoperative complications, a high anal sphincter preservation rate, an R0 resection rate, and a better prognosis.12 Given that local recurrence rates are high due to poor excision quality and tumor fragmentation of tumor,13 the transanal minimally invasive endoscopic excisions may lead to improved outcomes. The superiority of minimally invasive endoscopic transanal resection includes transanal minimally invasive surgery (TAMIS), transanal endoscopic microsurgery (TEM), with transanal endoscopic operation (TEO) receiving increasing attention.14
Transanal endoscopic microsurgery (TEM) is widely used in the treatment of local rectal lesions and helps avoid radical surgery. One study reported the results of 7 cases with TEM and only 1 patient experienced recurrence. Two of the 7 patients presented slight complications after surgery.15 A recent study16 reported that among 42 patients that had undergone a TEM procedure only 4 cases experienced recurrence or metastasis. Four patients presented complications after surgery and all patients recovered smoothly after conservative treatment. We summarized three larger retrospective studies in Table 1 and confirmed that the TEM is a feasible procedure for rectal GIST to maintain anal function fewer recurrences or metastases. However, TEM has been slow to become widely adopted by surgeons, and due to the high cost of highly specialized instruments.17 TAMIS, a hybrid between TEM and single-port laparoscopy, was reported in 2010 by Atallah et al. The authors concluded that TAMIS is a viable alternative to TEM at a much lower cost.18 We reviewed three larger retrospective studies of 7 cases without recurrence or metastasis, and confirmed that the TAMIS is a practicable approach for rectal GIST to preserve anal function with less recurrence or metastasis. In another approach to transanal endoscopic operation (TEO), only 1 study has reported the results of retrospective studies in detail (Table 1). The tumors of 2 patients were located in the anterior wall of the rectum and were treated with TEO. Two patients were followed up for 14 and 8 months, respectively, and no metastasis or recurrence was found. The transsacral approach (TSC) of preserving anal function can obtain a good oncological result and is particularly suitable for exogenous mid- and low-rectal GISTs. Two reports19,20 described 3 patients with transsacral procedures and neither complications no recurrence/metastasis after surgery. The adoption of the transsacral approach was considered as the treatment of choice for a rectal GIST. However, a recent study described the outcomes of 17 patients with TSC. Although all patients have a good oncological prognosis, 7 of the 17 patients experienced postoperative complications.21 Anastomotic leakage was found in 5 cases and poor wound healing in 2 cases. Two patients with anastomotic leakage recovered after conservative treatment, including without forced drainage and lavage, and one patient underwent sigmoidostomy. The TSC needs to be validated by further large-scale studies. Para-sacral approaches have also been applied in the therapy of rectal GISTs. Tokunaga et al22 showed that the para-sacral approach is simple and minimally invasive for local rectal GISTs. Matsumi23 et al showed that the para-sacral approach is effective for patients with tumors located between the urethra and the anterior wall of the low rectum in a recent study. To date, few large-scale reports demonstrate the superiority of this approach. Transsacral and transanal resection is beneficial for tumors located in the posterior wall, the areas of the middle or upper rectum.6,20 Although transanal resection is minimally invasive, tumors larger than 4 cm may be difficult to remove through the anus. When the tumor is located in the lower rectal region and is enclosed by the vaginal-rectal septum, the transvaginal approach is an alternative to a low or ultralow anterior resection surgery. However, enucleation without fragmentation may increase the risk of recurrence. We review the 4 studies associated with the transvaginal approach. Table 1 shows all of these patients had tumors of at least 5cm in size. There were no postoperative complications or tumor recurrence or metastasis at the follow-up date. The transvaginal approach is safe and feasible, especially if the tumor is large and is located in the anterior wall of the lower rectum. The perineal approach, which allows safe and effective excision of a tumor without disturbing the rectal anterior wall.24 The 4 cases included in our table were successfully resected with no perioperative complications, including metastasis or recurrence. GIST near the anterior wall of the rectum, anal sphincter, prostate, or urethra, but not invasive tumors can achieve safely and organ-preserving radical resection using the perineal approach. Robotic surgery has also been reported to have feasible and safe advantages, without morbidity or mortality, and that ISR provides bowel continuity and no need for colostomy.25 However, due to the high requirements of robotic surgery for surgical space, the difficulty of pelvic surgery has increased significantly, although there are few relevant studies in the literature.
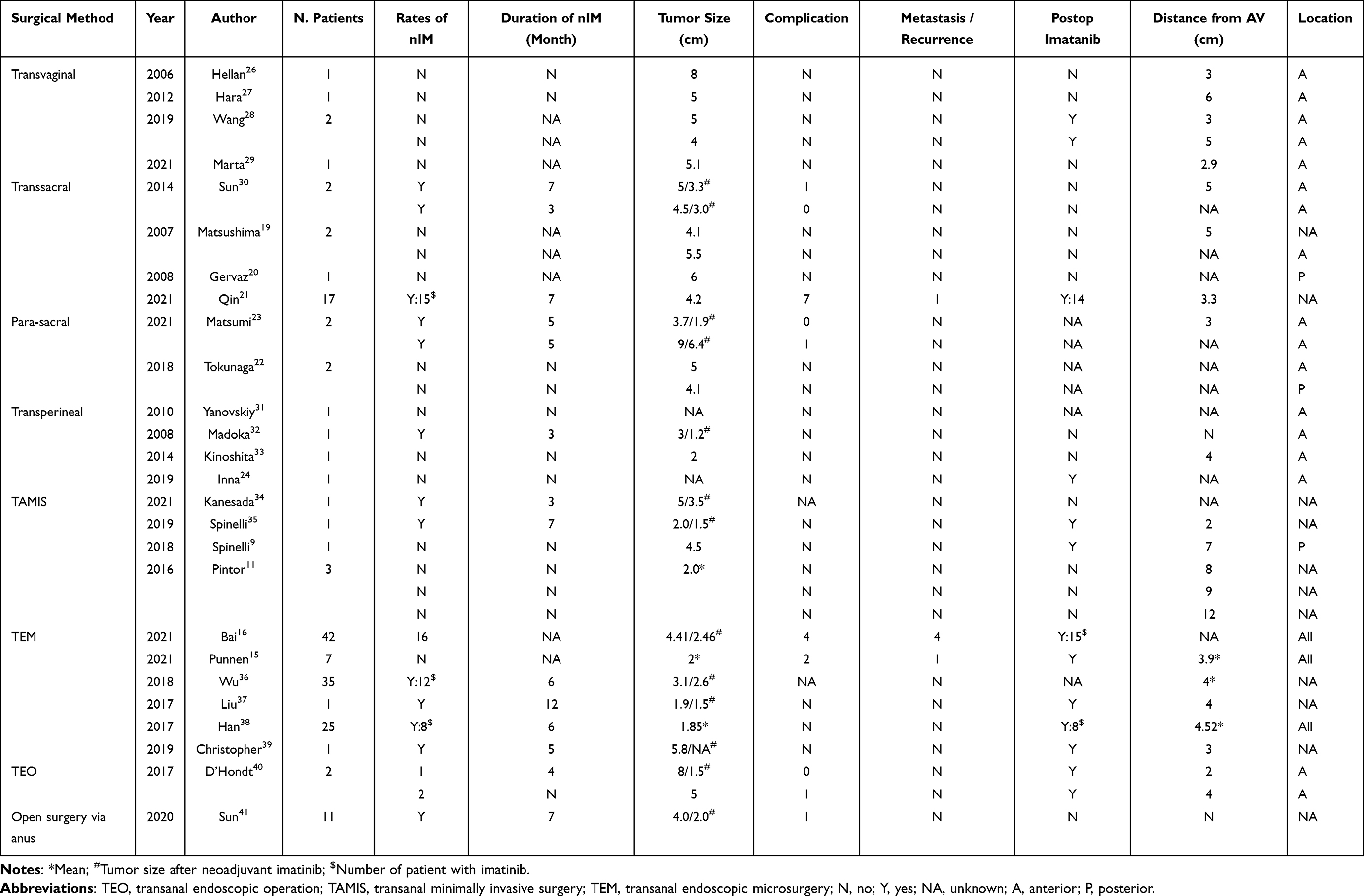 |
Table 1 Local Resection for Rectal GISTs |
Several recent approaches of endoscopic resection for rectal GISTs including the submucosal tunneling endoscopic resection (STER) technique, endoscopic submucosal dissection (ESD), and laparoscopic and endoscopic cooperative surgery (LECS) have been reported as the treatment of choice for local GISTs. Ishida et al described 88-year-old anemic woman with a 5 cm rectal submucosal tumor, the tumor was successfully resected by ESD with a negative margin.26 The STER technique successfully removed a 1.5-cm tumor arising from the inherent muscularis layer.27 LECS for rectal GI stromal tumors in patients with GISTs originating in the upper rectum may be a feasible procedure that achieves R0 resection while preserving the rectal function.28 Therefore, endoscopic resection for patients with rectal GIST is also a suitable method and worthy of further investigation.
Local Advanced GISTs: Neoadjuvant Imatinib Therapy with Surgery
IM, a specific tyrosine kinase receptor inhibitor (TKI), was approved by the US Food and Drug Administration (FDA) as the first-line treatment for advanced GIST in February 2002.29 IM is also the only TKI currently available for neoadjuvant therapy (nIM), and the standard dose is 400 mg/day.30,31 However, a case report also showed that sunitinib was selected for neoadjuvant therapy for gastrointestinal stromal tumors firstly. First-line neoadjuvant therapy with sunitinib produced good clinical outcomes in 2 patients with very large rectal GISTs adjacent to the prostate and bladder.32 The inclusion criteria for neoadjuvant therapy remain not well defined. Some studies have suggested a tumor size cut-off of 5 cm to start nIM while other studies recommend starting treatment in high-risk tumors.5,33–35 The European Society for Medical Oncology (ESMO) guidelines suggested that when R0 resection is not feasible, or the tumor can be removed with minor surgery through reduced cells,36 nIM will help reduce tumor size before surgery, preserving the sphincter in most cases. Rutkowski et al collected 161 local advanced GIST patients treated with nIM and showed nIM combining surgery with a good long-term result.37 Neoadjuvant treatment of rectal GISTs with IM was first reported in 2005 to achieve negative resection margins and preservation of the anal sphincter.38 When considering neoadjuvant therapy, diagnosis by biopsy is generally standard practice. One study39 suggested that for larger locally advanced lesions, a biopsy should be performed, preferably with an endoscope-guided fine needle puncture, to confirm the diagnosis before neoadjuvant therapy. When nIM is considered for GISTs, a molecular analysis should also be performed at the same time. However, we should avoid using nIM for wild-type GISTs.40 Most GISTs had a KIT mutation, including exon 11 (90%) or exon 9 (8%) and, less in exon 13 or exon 17.41 The mutant genotype of the rectal stromal tumor is unknown. Kameyama et al described several studies and found a proportion (59–100%) with exon 11 mutations in rectal GISTs.42 We have summarized all published studies including gene analyses since the article was published, all results in Table 2. The gene mutations of rectal GIST include KIT exon 11, KIT exon 9, KIT exon 13, PDGFR-a12, and wild type. We identified a higher proportion (71–90%) of rectal GISTs carrying c-KIT exon 11 mutations. Therefore, the exon mutations of rectal GISTs are similar to GISTs in other sites. For rectal GIST with exon 11 mutations, IM also obtained good therapeutic results. Heinrich et al43 showed that the ratio of objective response is 71.7% for rectal GIST with exon 11 mutations after nIM therapy. Yang et al44 also found the benefits which partial response occurred in 23 of 25 patients with c-KIT exon 11 after nIM therapy.
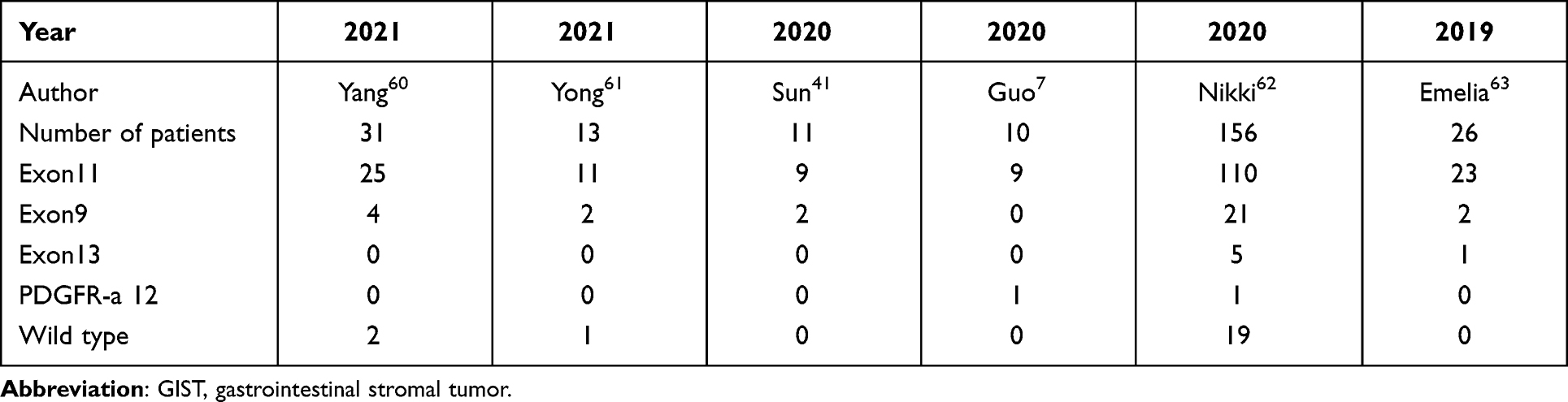 |
Table 2 Larger Scale Genotypes in Rectal GISTs |
IM, as a first-line nIM of rectal GISTs, was widely accepted. Similarly, the dose of IM with 400mg/d is most effective for patients with rectal GISTs. However, the optimal duration of nIM is still controversial. If the maximal response appears in the GISTs, IM should be discontinued. The maximal response is considered that when the tumor does not shrink further after two sequential computed tomography scans. The guidelines of the National Comprehensive Cancer Network (NCCN) guidelines suggested that the duration of maximum response may be at least 6 months.45 However, a recent larger study reported that treatment for GISTs located in the rectum seemed to have a longer median duration of 10.0 months.46
In locally advanced or unresectable cases, nIM can improve resectability or may reduce the incidence of complications and improve relapse-free survival.34 The study reported that recurrence rate after surgery was >25%, and the average survival time was less than 34 months.47 Neoadjuvant therapy generally prevents local recurrence and improves overall survival (OS), regardless of tumor size and risk stratification. Yong et al48 compared the patients receiving neoadjuvant therapy with patients undergoing surgery alone. They concluded the conclusion that neoadjuvant TKI has the benefit of downsizing unresectable rectal GIST to benefit from the sphincter-sparing procedure and also confers protection against local recurrence and improves OS. The application of nIM significantly decreased tumor size in large localized rectal GIST, allowing LR to preserve the sphincter and has maintained satisfactory anal function. Bai et al, reported that 16 patients were treated with nIM, resulted in 16 patients undergoing sphincter-sparing surgery that would otherwise require abdominal peritonectomy or pelvic tumor removal.16 However, another study reported LR for 7 patients without nIM and 4 cases of 7 patients with a positive margin. Previous studies have also confirmed that tumor size reduction by preoperative neoadjuvant IM was significantly reduced and improved the preservation rate of the anus. After IM treatment, the anal retention rate increased from 14.2% to 33.0–94.9%.42 Laparoscopic surgery with the advantage of adequate visualization for deep pelvic lesions has been used successfully in rectal GISTs.49–51 The effectiveness of nIM combining laparoscopic surgery has been described in several recent articles with an advanced and larger tumor.52,53 Although there are limited data on the treatment of rectal stromal tumors by laparoscopic surgery, this approach appears to be feasible, especially for locally advanced tumors. We summarized the laparoscopic resection of rectal GISTs nearly 10 years of articles in Table 3. From the results, we determined that most of the patients selected preoperative neoadjuvant therapy because they refused permanent stoma or serious invasive surgery. Neoadjuvant therapy was found to reduce tumor size in most tumors, complete R0 resection, and provided patients with the opportunity to choose surgery to preserve anal function. Furthermore, no recurrence or metastasis was found in all patients counted by the follow-up date. Although the rate of local recurrence of laparoscopic surgery is low, most patients are treated with laparoscopic surgery plus temporary transverse colostomy, which may affect patient quality of life and increase the possibility of ostomy complications. Further studies are needed. These results provide strong evidence that laparoscopic surgery is effective and safe for patients with rectal GISTs.
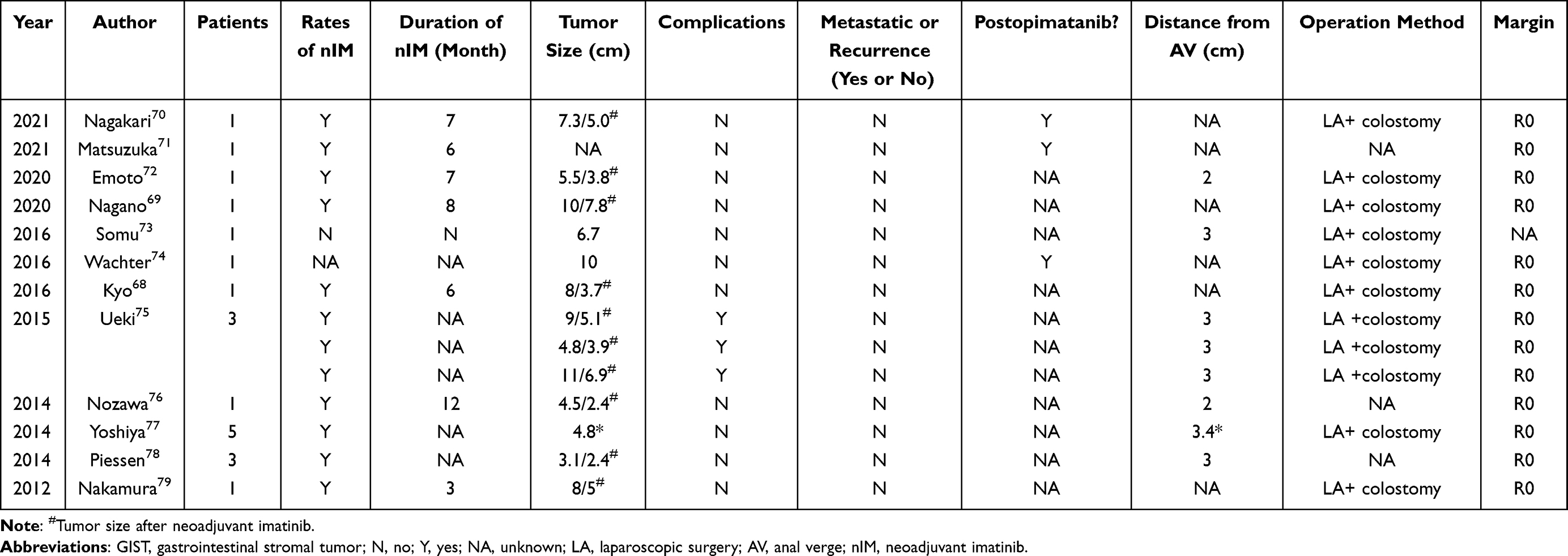 |
Table 3 Laparoscopic Surgery for Rectal GIST |
Adjuvant IM After Surgery
The 15 years of recurrence-free survival (RFS) and overall survival (OS) time were found to be 59.9% and 12.4 years with surgery alone respectively.3 Although R0 resection was complete, nearly one-third of the patients experienced relapse after surgery.33 Therefore, for patients at high risk of recurrence, it is necessary to use adjuvant IM after surgery. In a Phase III trial, patients with primary GIST who had a complete resection of at least 3 cm were randomized to receive placebo or IM for 1 year after surgery. The 12-month IM group had significantly better RFS than the placebo group. Based on these data, IM has been approved by the US Food and Drug Administration (FDA) as a postoperative adjuvant therapy. The SSG XVIII trial also included tumors at high risk of recurrence, with 36 months of adjuvant IM significantly improving RFS compared to 12 months of adjuvant therapy. Furthermore, the guidelines recommend that adjuvant therapy should continue for three years in high-risk patients. For intermediate-risk patients, there is still controversy. The consensus in China suggests that patients with moderate risk of small bowel or rectal stromal tumor should receive adjuvant IM for 3 years, while patients with moderate risk of gastric stromal tumor only need 1 year of adjuvant therapy.54,55 Recent studies have confirmed that approximately 50% of deaths during the first 10 years of postoperative follow-up can be avoided in high-risk patients who are treated with adjuvant IM for a longer period of time.56 Therefore, long-term adjuvant IM therapy is recommended for patients at high risk of recurrence.
Treatment for Advanced/Metastatic Rectal GIST
Conventional Medical Therapy
IM was approved by the FDA as a first-line treatment for advanced GIST in February 2002.29 Two-phase III trials determined that 400 mg daily was the optimal dose of IM in advanced GIST. In the trials of S0033 and phase III European Cancer Research and Treatment Group 62,005 trials, both trials demonstrated a significant clinical benefit of IM 400mg/ day. This result was first reported in the B222257 study, which also reported longer progression-free survival (PFS) with IM 800mg/ day, but no difference in OS. Based on these data, the standard dose of adjuvant IM is 400mg/ day.29,58 The BFR1459 trial evaluated patients with advanced GIST whose tumors responded to IM or were in a stable state. At 1, 3, or 5 years after discontinuing IM treatment, patients who stopped treatment had shorter PFS compared to those who continued treatment. No significant differences were found in OS time when treatment resumed. Therefore, in the event of metastasis/recurrence of the disease, the medication should be continued indefinitely.
Second-line sunitinib malate therapy is typically initiated for advanced GIST in which the disease progresses or is not tolerated after first-line IM therapy. A phase III trial also showed significant improvements in PFS and OS in patients treated with sunitinib compared to those treated with placebo.59 Based on these data, sunitinib was approved by US FDA as a second-line treatment for advanced GIST.60
A Phase III study (GRID study)61 in patients with metastatic and/or unresectable GIST who progressed after IM and sunitinib treatment showed that regorafenib significantly improved median disease-free survival, but no statistically significant differences were found in the median survival between the two groups. Regorafenib is approved to treat patients with GIST who had previously failed treatment with IM and sunitinib.61,62 Regorafenib has a similar effect to sunitinib, benefiting mutations in KIT exons 11 or 9 in patients with primary tumors.
A report published in September 2020 revealed that all patients who received ripretinib as second-, third-, or fourth-line therapy significantly prolonged PFS by increasing the dose of ripretinib. The subsequent INVICTUS III study63 confirmed 6.3 and 1.0 months of m PFS, 15.1 and 6.6 months of m OS, respectively, compared to ripretinib and placebo. Based on these results, in May 2020, the US FDA approved ripretinib inclusion as the standard fourth-line treatment for advanced GIST patients who have failed three lines of TKI therapy, including IM. A Phase III trial is currently underway to test the efficacy of lapatinib versus sunitinib in advanced GIST patients who progress in a second-line setting or are intolerant to IM.64
The use of ripretinib for advanced rectal GIST was firstly presented in China.65 The tumor size did not improve further after the initial first to third-line treatments. However, tumors started to shrink after 3 courses of ripretinib treatment. Therefore, the use of mutation inhibitors at an early stage may be more precise and rational.
Of the exon 18 mutations, D842Y was sensitive to IM but resistant to sunitinib,66 most of the mutations, especially D842V, were not sensitive to IM. A Phase II trial reported that a GIST patient harboring a D842V mutation had a good response to dasatinib. Due to these initial therapeutic results, the NCCN added dasatinib to the treatment list of this molecular subtype.67 In a recent NAVIGATOR68 study of 56 advanced patients with the D842V mutation, avapritinib reduced tumors in the majority (98%) of patients. Thus, in January 2020, the US FDA approved avapritinib for the treatment of advanced or metastatic GISTs carrying PDGFRA exon 18 mutations. Avapritinib also received approval from the European Medicines Agency (EMA) on 24 September 2020.69 However, more cognition-related and intracranial hemorrhage adverse events should be closely monitored in clinical application. Therefore, patients with PDGFRA exon 18 mutations must receive avapritinib as first-line therapy.
Other Medicines Treatment
Selective TKIs of targeting secondary KIT mutations, including PLX3397, PLX9486, and AZD3229 are being studied. The integral combination treatment with PLX9486 with sunitinib, improving the median PFS for 2 months.70,71 AZD3229, a pan-KIT/PDGFRα inhibitor, showed good preclinical activity in gastrointestinal stromal tumor models and was deemed worthy of a clinical study. Preclinical studies have confirmed the effects of immune agents on KIT-mutated GIST. Balachandran et al verified the combination of IM and ipilimumab in animal models with KIT-mutated GIST. Compared to treatment alone, combination therapy exhibited synergistic effects and significantly reduced tumor size.72 ETV1 may also be the key to the resistance observed to IM treatment inherent in GIST, KIT-independent stem cell/progenitor cell survival and maintenance, demonstrated that this may be a potential therapeutic target to be considered in wild-type GIST.71 The study showed the benefits of the combination of IM and pinitinib for patients with advanced GIST with all genotypes. In particular, for 9 patients who have an unresectable tumor, the percentage of patients who switched to excision was 88.9%.73 These results confirm the advantages of the combination treatment compared to IM alone. Sirolimus has also been shown to be safe when added to sorafenib or sunitinib in the treatment of advanced tumor.74
Treatment Beyond Medicines: Radiotherapy
Palliative surgery is not considered necessary for recurrent or metastatic GISTs.75,76 However, radiotherapy is usually well-tolerated and the use of IM enhances sensitivity to radiotherapy.77 This limited use can be attributed to GIST’s shifting pattern and radiotherapy has been imposed restrictions on palliative intent.78,79 Radiotherapy can be an effective treatment for patients who cannot tolerate TKIs, are resistant to TKI, or exhibit unresectable tumors. Radiotherapy for rectal GIST alone is very rare. Pollock at al. reported a case rectal GIST with radiotherapy and reported a total treatment plan, treatment field in rectal GIST radiotherapy.80
Conclusions
The treatment of rectal stromal tumors is still dominated by surgery, and the specific surgical method is still controversial. The use of neoadjuvant IM provides better treatment feasibility. Local resection, including transanal, transacral, parasacral, perineal, and transvaginal resection can obtain a good oncological outcome and prevent the appearance of genitourinary and anal dysfunction. Laparoscopic surgery is a safe surgical technique that prevents the appearance of genitourinary and anal dysfunctions and completely resects the tumor, and is especially useful for advanced and larger tumors. Endoscopic resection for rectal GISTs arising from the inherent muscularis layer is also a suitable method and worthy of further investigation.
Acknowledgment
The authors acknowledge the support of the Liaoning province science and Technology Agency (No. 2014023034).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Søreide K, Sandvik OM, Søreide JA, et al. Global epidemiology of gastrointestinal stromal tumours (GIST): a systematic review of population-based cohort studies. Cancer Epidemiol. 2016;40:39–46. doi:10.1016/j.canep.2015.10.031
2. Corless CL, Barnett CM, Heinrich MC. Gastrointestinal stromal tumours: origin and molecular oncology. Nat Rev Cancer. 2011;11:865–878. doi:10.1038/nrc3143
3. Joensuu H, Vehtari A, Riihimäki J, et al. Risk of recurrence of gastrointestinal stromal tumour after surgery: an analysis of pooled population-based cohorts. Lancet Oncol. 2012;13:265–274. doi:10.1016/s1470-2045(11)70299-6
4. Baik SH, Kim NK, Lee CH, et al. Gastrointestinal stromal tumor of the rectum: an analysis of seven cases. Surg Today. 2007;37:455–459. doi:10.1007/s00595-006-3424-1
5. Jakob J, Mussi C, Ronellenfitsch U, et al. Gastrointestinal stromal tumor of the rectum: results of surgical and multimodality therapy in the era of imatinib. Ann Surg Oncol. 2013;20:586–592. doi:10.1245/s10434-012-2647-1
6. Miettinen M, Furlong M, Sarlomo-Rikala M, et al. Gastrointestinal stromal tumors, intramural leiomyomas, and leiomyosarcomas in the rectum and anus: a clinicopathologic, immunohistochemical, and molecular genetic study of 144 cases. Am J Surg Pathol. 2001;25:1121–1133. doi:10.1097/00000478-200109000-00002
7. Guo W, Yang Z, Wei Y, et al. Radical excision versus local resection for primary rectal gastrointestinal stromal tumors cohort study. Int J Surg. 2020;77:190–197. doi:10.1016/j.ijsu.2020.03.068
8. Watanabe Y, et al. Clinical outcomes of different therapeutic modalities for rectal gastrointestinal stromal tumor: summary of 14-year clinical experience in a single center. Cancer Sci. 2020;77:1–7. doi:10.1111/cas.1420210.1016/j.ijsu.2020.03.007
9. Nepal P, Mori S, Kita Y, et al. Management of a case of high-risk gastrointestinal stromal tumor in rectum by transanal minimal invasive surgery. World J Surg Oncol. 2018;16:165. doi:10.1186/s12957-018-1463-x
10. Parks AG, Stuart AE. The management of villous tumours of the large bowel. Br J Surg. 1973;60:688–695. doi:10.1002/bjs.1800600908
11. Pintor-Tortolero J, García JC, Cantero R. Transanal minimally invasive surgery approach for rectal GIST. Tech Coloproctol. 2016;20:321–322. doi:10.1007/s10151-016-1438-2
12. Yang Z, et al. Transanal versus nontransanal surgery for the treatment of primary rectal gastrointestinal stromal tumors: a 10-year experience in a high-volume center. World J Surg Oncol. 2020;8:201. doi:10.1186/s12957-018-1427-110.21037/atm.2020.01.55
13. Paty PB, Nash GM, Baron P, et al. Long-term results of local excision for rectal cancer. Ann Surg. 2002;236(4):
14. Eldamshety O, Metwally IH, Ghoneem E, Elkashef WF. Resection of rectal GIST using a novel technique: a report of two cases. Ecancermedicalscience. 2017;11:760. doi:10.3332/ecancer.2017.760
15. Punnen S, Karimuddin AA, Raval MJ, Phang PT, Brown CJ. Transanal Endoscopic Microsurgery (TEM) for rectal GI stromal tumor. J Surg Oncol. 2021;221:183–186. doi:10.1002/jso.2562110.1016/j.amjsurg.2020.07.013
16. Bai X, Zhou W, Li Y, Lin G. Transanal endoscopic microsurgery with alternative neoadjuvant imatinib for localized rectal gastrointestinal stromal tumor: a single center experience with long-term surveillance. Surgical endoscopy. 2021;35:3607–3617. doi:10.1007/s00464-020-07837-5
17. Maslekar S, Pillinger SH, Sharma A, Taylor A, Monson JR. Cost analysis of transanal endoscopic microsurgery for rectal tumours. Colorectal Dis. 2007;9:229–234. doi:10.1111/j.1463-1318.2006.01132.x
18. Atallah S, Albert M, Larach S. Transanal minimally invasive surgery: a giant leap forward. Surg Endosc. 2010;24:2200–2205. doi:10.1007/s00464-010-0927-z
19. Matsushima K, Kayo M. Transsacral approach to resect a gastrointestinal stromal tumor in the rectum: report of two cases. Surg Today. 2007;37:698–701. doi:10.1007/s00595-006-3466-4
20. Gervaz P, Huber O, Bucher P, Sappino P, Morel P. Trans-sacral (Kraske) approach for gastrointestinal stromal tumour of the lower rectum: old procedure for a new disease. Colorectal Dis. 2008;10:951–952. doi:10.1111/j.1463-1318.2008.01489.x
21. Qin X, Li C, Yang Z, et al. Transsacrococcygeal approach in rectal gastrointestinal stromal tumour resection: 10-year experience at a single centre. Ann Transl Med. 2021;9:341. doi:10.21037/atm-20-8204
22. Tokunaga R, Sakamoto Y, Nakagawa S, et al. Para-sacral approach for large gastrointestinal stromal tumor of the lower rectum. Int Cancer Conf J. 2018;7:40–42. doi:10.1007/s13691-017-0314-x
23. Matsumi Y, Hamada M, Sakaguchi T, Sekimoto M, Kurokawa H, Kinoshita H. Para-sacral approach followed by laparoscopic low anterior resection of a gastrointestinal stromal tumour at the anterior wall of the lower rectum. Colorectal Dis. 2021;23:1579–1583. doi:10.1111/codi.15597
24. Tulina I, Kitsenko Y, Lukyano A, Bergamaschi R, Tsarkov P. Transperineal Excision of Rectal Gastrointestinal Stromal Tumor. Surg Technol Int. 2019;34:195–198.
25. Du JL, Chen CC, Chao HM, Kuo LJ. Robot-assisted intersphincteric resection for rectal submucosal tumour. Int J Surg Pathol. 2016;12:478–482. doi:10.1177/106689691877317710.1002/rcs.1667
26. Hellan M, Maker VK. Transvaginal excision of a large rectal stromal tumor: an alternative. Am J Surg. 2006;191:121–123. doi:10.1016/j.amjsurg.2005.10.013
27. Hara M, Takayama S, Arakawa A, et al. Transvaginal resection of a rectal gastrointestinal stromal tumor. Surg Today. 2012;42:909–912. doi:10.1007/s00595-012-0215-8
28. Shizhuo W, Nannan L, Sha N, et al. Transvaginal excision of rectal stromal tumors: case reports and a literature review. World J Surg Oncol. 2019;17:164. doi:10.1186/s12957-019-1703-8
29. Ferreira MM, Guimaraes N, Monica IB, et al. Transvaginal resection of a rectal gastrointestinal stromal tumor: a case report. J Med Cases. 2021;12:57–60. doi:10.14740/jmc3615
30. Sun LF, He JJ, Yu S-J, et al. Transsacral excision with pre-operative imatinib mesylate treatment and approach for gastrointestinal stromal tumors in the rectum: a report of two cases. Oncol Lett. 2014;8:1455–1460. doi:10.3892/ol.2014.2406
31. Yanovskiy M, Saddig C, Ommer A, Pahnke JM, Kröpfl D. [Gastrointestinal stromal tumor (GIST) of the anterior rectal wall. R0 resection with simultaneous radical retropubic prostatectomy]. Der Urologe. 2010;49:271–274. German. doi:10.1007/s00120-009-2186-y
32. Hamada M, Ozaki K, Horimi T, et al. Recurrent rectal GIST resected successfully after preoperative chemotherapy with imatinib mesylate. Int J Clin Oncol. 2008;13:355–360. doi:10.1007/s10147-007-0735-1
33. Kinoshita H, Sakata Y, Umano Y, Iwamoto H, Mori K. Perineal approach for a gastrointestinal stromal tumor on the anterior wall of the lower rectum. World J Surg Oncol. 2014;12:62. doi:10.1186/1477-7819-12-62
34. Kanesada K, et al. [A case of gastrointestinal stromal tumor of the lower rectum that enabled minimally invasive surgery with imatinib mesylate as neoadjuvant chemotherapy]. Gan To Kagaku Ryoho. 2021;48:269–272. Japanese.
35. Spinelli A, Carvello M, Sacchi M, et al. Transanal minimally invasive surgery (TAMIS) for anterior rectal GIST. Tech Coloproctol. 2019;23:501–502. doi:10.1007/s10151-019-01979-y
36. Wu X, Lin G, Qiu H, Zhou J, Xu J. [Transanal endoscopic microsurgery for local excision of rectal gastrointestinal stromal tumors]. Zhonghua wei Chang Wai Ke Za Zhi. 2018;21:1296–1300. Chinese.
37. Liu Q, Zhong G, Zhou W, Lin G. Initial application of transanal endoscopic microsurgery for high-risk lower rectal gastrointestinal stromal tumor after imatinib mesylate neoadjuvant chemotherapy: a case report. Medicine. 2017;96:e7538. doi:10.1097/md.0000000000007538
38. Han X, Xu J, Qiu H, Lin G. A novel curative treatment strategy for patients with lower grade rectal gastrointestinal stromal tumor: chemoreduction combined with transanal endoscopic microsurgery. J Laparoendosc Adv Surg Tech A. 2017;27:579–585. doi:10.1089/lap.2017.0051
39. Kane WJ, Friel CM. Diagnosis and treatment of rectal gastrointestinal stromal tumors. Dis Colon Rectum. 2019;62:537–540. doi:10.1097/dcr.0000000000001376
40. D’Hondt M, Yoshihara E, Dedrye L, et al. Transanal endoscopic operation for benign rectal lesions and T1 carcinoma. J Soc Laparoendosc Surg. 2017;21. doi:10.4293/jsls.2016.00093
41. Sun Q, Su N, Li X, Hu Z, Wang W. Open transanal resection of low rectal stromal tumor following neoadjuvant therapy of imatinib mesylate: report of 11 cases and review of literature. Asia Pac J Clin Oncol. 2020;16:123–128. doi:10.1016/j.amjsurg.2020.07.01310.1111/ajco.13292
42. Ishida T, Furumatsu K, Kado T. Endoscopic submucosal dissection of a rectal gastrointestinal stromal tumor close to the dentate line. Dig Endosc. 2020;32:e49–e51. doi:10.1111/den.13605
43. Wallenhorst T, et al. Endoscopic resection of a rectal gastrointestinal stromal tumor using the submucosal tunneling endoscopic resection (STER) technique. Endoscopy. 2021. doi:10.1055/a-1508-5241
44. Hiyoshi Y, Yamasaki A, Shono T, et al. Laparoscopic and endoscopic cooperative surgery for rectal GI stromal tumor. Dis Colon Rectum. 2020;63:116. doi:10.21037/atm.2020.01.5510.1097/dcr.0000000000001514
45. Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002;347:472–480. doi:10.1056/NEJMoa020461
46. Corless CL, Ballman KV, Antonescu CR, et al. Pathologic and molecular features correlate with long-term outcome after adjuvant therapy of resected primary GI stromal tumor: the ACOSOG Z9001 trial. J clin oncol. 2014;32:1563–1570. doi:10.1200/jco.2013.51.2046
47. Casali PG, Le Cesne A, Poveda Velasco A, et al. Time to definitive failure to the first tyrosine kinase inhibitor in localized GI stromal tumors treated with imatinib as an adjuvant: a European Organisation for research and treatment of cancer soft tissue and bone sarcoma group intergroup randomized trial in collaboration with the Australasian Gastro-Intestinal Trials Group, UNICANCER, French Sarcoma Group, Italian Sarcoma Group, and Spanish Group for research on sarcomas. J clin oncol. 2015;33:4276–4283. doi:10.1200/jco.2015.62.4304
48. Kajiura S, Hosokawa A, Nanjyo S, et al. [A case of a gastrointestinal stromal tumor of the rectum effectively treated with continuously-administered regorafenib after failure of imatinib and sunitinib]. Nihon Shokakibyo Gakkai zasshi. 2016;113:655–661. Japanese. doi:10.11405/nisshoshi.113.655
49. Liu H, Yan Z, Liao G, Yin H. Treatment strategy of rectal gastrointestinal stromal tumor (GIST). J Surg Oncol. 2014;109:708–713. doi:10.1002/jso.23562
50. Wilkinson MJ, Fitzgerald JEF, Strauss DC, et al. Surgical treatment of gastrointestinal stromal tumour of the rectum in the era of imatinib. Br J Surg. 2015;102:965–971. doi:10.1002/bjs.9818
51. Hawkins AT, Wells KO, Krishnamurty DM, et al. Preoperative chemotherapy and survival for large anorectal gastrointestinal stromal tumors: a national analysis of 333 cases. Ann Surg Oncol. 2017;24:1195–1201. doi:10.1245/s10434-016-5706-1
52. Casali PG, Jost L, Reichardt P, Schlemmer M, Blay JY. Gastrointestinal stromal tumors: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2008;19(Suppl 2):ii35–ii38. doi:10.1093/annonc/mdn080
53. Rutkowski P, Gronchi A, Hohenberger P, et al. Neoadjuvant imatinib in locally advanced gastrointestinal stromal tumors (GIST): the EORTC STBSG experience. Ann Surg Oncol. 2013;20:2937–2943. doi:10.1245/s10434-013-3013-7
54. Lo SS, Papachristou GI, Finkelstein SD, et al. Neoadjuvant imatinib in gastrointestinal stromal tumor of the rectum: report of a case. Dis Colon Rectum. 2005;48:1316–1319. doi:10.1007/s10350-004-0922-3
55. Alavi K. Expert commentary on the diagnosis and treatment of rectal GI tumors. Dis Colon Rectum. 2019;62:540–541. doi:10.1097/dcr.0000000000001375
56. Heinrich MC, Corless CL, Demetri GD, et al. Kinase mutations and imatinib response in patients with metastatic gastrointestinal stromal tumor. J clin oncol. 2003;21:4342–4349. doi:10.1200/jco.2003.04.190
57. Joensuu H, Rutkowski P, Nishida T, et al. KIT and PDGFRA mutations and the risk of GI stromal tumor recurrence. J clin oncol. 2015;33:634–642. doi:10.1200/jco.2014.57.4970
58. Kameyama H, Kanda T, Tajima Y, et al. Management of rectal gastrointestinal stromal tumor. Transl Gastroenterol Hepatol. 2018;3:8. doi:10.21037/tgh.2018.01.08
59. Heinrich MC, Owzar K, Corless CL, et al. Correlation of kinase genotype and clinical outcome in the North American intergroup Phase III trial of imatinib mesylate for treatment of advanced gastrointestinal stromal tumor: CALGB 150105 study by cancer and leukemia group B and Southwest Oncology Group. J clin oncol. 2008;26:5360–5367. doi:10.1200/jco.2008.17.4284
60. Yang W, Liu Q, Lin G. The effect of neoadjuvant imatinib therapy on outcome and survival in rectal gastrointestinal stromal tumors: a multiinstitutional study. J Surg Oncol. 2021;124(7):1128–1135. doi:10.1002/jso.26628
61. Yong ZZ, et al. Neoadjuvant tyrosine kinase inhibitors in rectal gastrointestinal stromal tumours: a provision for enhanced oncological and functional outcomes. Int J Clin Oncol. 2021;26:913–921. doi:10.1007/s10147-021-01867-2
62. IJzerman NS, Mohammadi M, Tzanis D, et al. Quality of treatment and surgical approach for rectal gastrointestinal stromal tumour (GIST) in a large European cohort. Eur j Surg Oncol. 2020;46:1124–1130. doi:10.1016/j.ejso.2020.02.033
63. Tatsuoka T, et al. Frequent rectal gastrointestinal stromal tumor recurrences in the imatinib era: retrospective analysis of an International Patient Registry. World J Surg Oncol. 2019;120:715–721. doi:10.1186/s12957-017-1231-310.1002/jso.25621
64. von Mehren M, Randall RL, Benjamin RS, et al. Soft Tissue Sarcoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Netw. 2018;16:536–563. doi:10.6004/jnccn.2018.0025
65. Qi J, Liu H-L, Ren F, et al. Preoperative adjuvant therapy for locally advanced and recurrent/metastatic gastrointestinal stromal tumors: a retrospective study. World J Surg Oncol. 2020;18:70. doi:10.1186/s12957-020-01840-9
66. Zanwar S, Ostwal V, Sahu A, et al. Rectal GIST-Outcomes and viewpoint from a tertiary cancer center. Indian j Gastroenterol. 2016;35:445–449. doi:10.1007/s12664-016-0710-8
67. Akiyoshi T, Ueno M, Fukunaga Y, et al. Laparoscopic local excision and rectoanal anastomosis for rectal gastrointestinal stromal tumor: modified laparoscopic intersphincteric resection technique. Dis Colon Rectum. 2014;57:900–904. doi:10.1097/dcr.0000000000000146
68. Kyo K, Azuma M, Okamoto K, et al. Neoadjuvant imatinib treatment and laparoscopic anus-preserving surgery for a large gastrointestinal stromal tumor of the rectum. World J Surg Oncol. 2016;14:68. doi:10.1186/s12957-016-0837-1
69. Nagano S, Miyoshi N, Takahashi T, et al. Preoperative imatinib and laparoscopic intersphincteric resection for large rectal gastrointestinal stromal tumor: a case report. Int J Surg Case Rep. 2020;71:235–239. doi:10.1016/j.ijscr.2020.05.031
70. Nagakari K, Matoba S, Toda S, et al. Hybrid resection of massive rectal gastrointestinal stromal tumor using laparoscopic and transanal approaches. Asian J Endosc Surg. 2021;14:102–105. doi:10.1111/ases.12824
71. Matsuzuka S, et al. [A case of the large rectal GIST treated by laparoscopic anus preserving operation after neoadjuvant therapy with imatinib mesylate]. Gan To Kagaku Ryoho. 2021;48:385–387. Japanese.
72. Emoto S, Akiyoshi T, Fukata K, Nagasaki T, Fukunaga Y. Laparoscopic transabdominal dissection and transection of the distal rectum followed by local excision through the anus for rectal gastrointestinal stromal tumor. Dis Colon Rectum. 2020;63:e542. doi:10.1097/dcr.0000000000001814
73. Somu K, Dashore AR, Shah AR, Anandh R. Laparoscopic excision of large lower rectal gastrointestinal stromal tumour (GIST): a case report. J Minim Access Surg. 2016;12:283–285. doi:10.4103/0972-9941.181311
74. Wachter N, Wörns M-A, Dos Santos D, et al. Transanal minimally invasive surgery (TAMIS) approach for large juxta-anal gastrointestinal stromal tumour. J Minim Access Surg. 2016;12:289–291. doi:10.4103/0972-9941.181306
75. Ueki T, Nagayoshi K, Manabe T, et al. Laparoscopic en bloc excision of gastrointestinal stromal tumors of the rectum after neoadjuvant imatinib therapy: anteriorly extended intersphincteric resection combined with partial resection of the prostate. Tech Coloproctol. 2015;19:247–251. doi:10.1007/s10151-014-1261-6
76. Nozawa H, Kanazawa T, Tanaka T, et al. Laparoscopic resection of a gastrointestinal stromal tumor of the lower rectum in a patient with coronary artery disease following long-term neoadjuvant imatinib treatment and anticoagulation therapy. World J Surg Oncol. 2014;12:211. doi:10.1186/1477-7819-12-211
77. Fujimoto Y, Akiyoshi T, Konishi T, et al. Laparoscopic sphincter-preserving surgery (intersphincteric resection) after neoadjuvant imatinib treatment for gastrointestinal stromal tumor (GIST) of the rectum. Int J Colorectal Dis. 2014;29:111–116. doi:10.1007/s00384-013-1769-7
78. Piessen G, et al. Laparoscopic local excision and rectoanal anastomosis for rectal gastrointestinal stromal tumor: modified laparoscopic intersphincteric resection technique. J Surg Oncol. 2014;57:900–904. doi:10.1002/jso.2621510.1097/dcr.0000000000000146
79. Nakamura T, Mitomi H, Onozato W, et al. Laparoscopic resection of a gastrointestinal stromal tumor of the rectum after treatment with imatinib mesylate: report of a case. Surg Today. 2012;42:1096–1099. doi:10.1007/s00595-012-0134-8
80. Wu X, Li J, Xu W, et al. Postoperative imatinib in patients with intermediate risk gastrointestinal stromal tumor. Future Oncol. 2018;14:1721–1729. doi:10.2217/fon-2017-0691
81. Fu Y, Hao H, Guo L, Yang G, Zhang X. Retrospective analysis of 85 cases of intermediate-risk gastrointestinal stromal tumor. Oncotarget. 2017;8:10136–10144. doi:10.18632/oncotarget.14359
82. Joensuu H, Eriksson M, Sundby Hall K, et al. Survival outcomes associated with 3 years vs 1 year of adjuvant imatinib for patients with high-risk gastrointestinal stromal tumors: an analysis of a randomized clinical trial after 10-year follow-up. JAMA oncol. 2020;6:1241–1246. doi:10.1001/jamaoncol.2020.2091
83. Gastrointestinal Stromal Tumor Meta-Analysis Group. Comparison of two doses of imatinib for the treatment of unresectable or metastatic gastrointestinal stromal tumors: a meta-analysis of 1,640 patients. J clin oncol. 2010;28:1247–1253. doi:10.1200/jco.2009.24.2099
84. Ben-Ami E, Barysauskas CM, von Mehren M, et al. Long-term follow-up results of the multicenter Phase II trial of regorafenib in patients with metastatic and/or unresectable GI stromal tumor after failure of standard tyrosine kinase inhibitor therapy. Ann Oncol. 2016;27:1794–1799. doi:10.1093/annonc/mdw228
85. Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368:1329–1338. doi:10.1016/s0140-6736(06)69446-4
86. Ozols RF, Herbst RS, Colson YL, et al. Clinical cancer advances 2006: major research advances in cancer treatment, prevention, and screening–a report from the American Society of Clinical Oncology. J clin oncol. 2007;25:146–162. doi:10.1200/jco.2006.09.7030
87. Demetri GD, Reichardt P, Kang Y-K, et al. Efficacy and safety of regorafenib for advanced gastrointestinal stromal tumours after failure of imatinib and sunitinib (GRID): an international, multicentre, randomised, placebo-controlled, Phase 3 trial. Lancet. 2013;381:295–302. doi:10.1016/s0140-6736(12)61857-1
88. Demetri GD, Heinrich MC, Fletcher JA, et al. Molecular target modulation, imaging, and clinical evaluation of gastrointestinal stromal tumor patients treated with sunitinib malate after imatinib failure. Clin Cancer Res. 2009;15:5902–5909. doi:10.1158/1078-0432.ccr-09-0482
89. Blay JY, Serrano C, Heinrich MC, et al. Ripretinib in patients with advanced gastrointestinal stromal tumours (INVICTUS): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2020;21:923–934. doi:10.1016/s1470-2045(20)30168-6
90. Clinicaltrials.gov. A study of DCC-2618 vs. sunitinib in advanced gist patients after treatment with imatinib (intrigue); 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT03673501.
91. Wu C, Zhang J, Wu X. Ripretinib in treatment of repeatedly relapsing rectal gastrointestinal stromal tumor: a case report. Ann Palliat Med. 2021;10:4994–4998. doi:10.1002/rcs.166710.21037/apm-21-722
92. Heinrich MC, Maki RG, Corless CL, et al. Primary and secondary kinase genotypes correlate with the biological and clinical activity of sunitinib in imatinib-resistant gastrointestinal stromal tumor. J clin oncol. 2008;26:5352–5359. doi:10.1200/jco.2007.15.7461
93. Network NCC. NCCN guidelines version 2.2017 soft tissue sarcoma; 2017. Available from: https://www.nccn.org/professionals/physician_gls/pdf/sarcoma.pdf.
94. Heinrich MC, Jones RL, von Mehren M, et al. Avapritinib in advanced PDGFRA D842V-mutant gastrointestinal stromal tumour (NAVIGATOR): a multicentre, open-label, Phase 1 trial. Lancet Oncol. 2020;21:935–946. doi:10.1016/s1470-2045(20)30269-2
95. Trullas-Jimeno A, Delgado J, Garcia-Ochoa B, et al. The EMA assessment of avapritinib in the treatment of gastrointestinal stromal tumours harbouring the PDGFRA D842V mutation. ESMO open. 2021;6:100159. doi:10.1016/j.esmoop.2021.100159
96. Clinicaltrials.gov. PLX9486 as a single agent and in combination with PLX3397 or PLX9486 with sunitinib in patients with advanced solid tumors; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT02401815?term=NCT02401815&draw=2&rank=1.
97. Trent J, Chugh R, Tsiatis AC, et al. The potent and selective KIT inhibitor PLX9846 dosed in combination with sunitinib demonstrates promising PFS in patients with advanced GIST: final results of phase I/II study.
98. Balachandran VP, Cavnar MJ, Zeng S, et al. Imatinib potentiates antitumor T cell responses in gastrointestinal stromal tumor through the inhibition of Ido. Nat Med. 2011;17:1094–1100. doi:10.1038/nm.2438
99. Chi P, Qin L-X, Kelly CM, et al. A phase II study of MEK162 (binimetinib [BINI]) in combination with imatinib in patients with untreated advanced gastrointestinal stromal tumor (GIST). J Clin Oncol. 2020;38(15_suppl):11508. doi:10.1200/JCO.2020.38.15_suppl.11508
100. Vincenzi B, Nannini M, Badalamenti G. Imatinib rechallenge in patients with advanced gastrointestinal stromal tumors following progression with imatinib, sunitinib and regorafenib. Ther Adv Med Oncol. 2018;10:1758835918794623. doi:10.1177/1758835918794623
101. Shen C, Chen H, Yin Y, et al. Preoperative imatinib for patients with primary unresectable or metastatic/recurrent gastrointestinal stromal tumor. Clinics. 2014;69:758–762. doi:10.6061/clinics/2014(11)09\\
102. Bischof DA, Kim Y, Blazer DG, et al. Surgical management of advanced gastrointestinal stromal tumors: an international multi-institutional analysis of 158 patients. J Am Coll Surg. 2014;219:439–449. doi:10.1016/j.jamcollsurg.2014.02.037
103. Choudhury A, Zhao H, Jalali F, et al. Targeting homologous recombination using imatinib results in enhanced tumor cell chemosensitivity and radiosensitivity. Mol Cancer Ther. 2009;8(1):203–213. doi:10.1158/1535-7163.mct-08-0959
104. Di Scioscio V, Greco L, Pallotti MC, et al. Three cases of bone metastases in patients with gastrointestinal stromal tumors. Rare Tumors. 2011;3(2):e17. doi:10.4081/rt.2011.e17
105. Tezcan Y, Koç M. Gastrointestinal stromal tumor of the rectum with bone and liver metastasis: a case study. Med Oncol. 2011;28(Suppl 1):S204–S206. doi:10.1007/s12032-010-9697-7
106. Pollock J, Morgan D, Denobile J, Williams J. Adjuvant radiotherapy for gastrointestinal stromal tumor of the rectum. Dig Dis Sci. 2001;46:268–272. doi:10.1023/a:1005581000712
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.