")
Back to Journals » Clinical Ophthalmology » Volume 16
Reasons for the Late Presentation of Diabetic Retinopathy in Saudi Arabia: A Survey of Patients Who Presented with Advanced Proliferative Diabetic Retinopathy to a Tertiary Eye Hospital
Authors Al-Shehri AM, Aldihan KA , Aljohani S
Received 20 October 2022
Accepted for publication 20 December 2022
Published 28 December 2022 Volume 2022:16 Pages 4323—4333
DOI https://doi.org/10.2147/OPTH.S394146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdulaziz Mohammed Al-Shehri,1,2 Khalid Abdulaziz Aldihan,3 Saud Aljohani4
1Vitreoretinal Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 2Surgery Department, Taif University, Taif, Saudi Arabia; 3Fellowship and Residency Training Program, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 4Ophthalmology Department, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Abdulaziz Mohammed Al-Shehri, Vitreoretinal Division, King Khaled Eye Specialist Hospital, 2867 Al Urubah Road, 8247, Riyadh, 26524, Saudi Arabia, Tel +966569974474, Email [email protected]
Purpose: This study aimed to understand the barriers that contribute to diagnostic and therapeutic delays in patients with advanced proliferative diabetic retinopathy (PDR).
Patients and Methods: This cross-sectional study targeted patients with advanced PDR who never received any ocular intervention at King Khaled Eye Specialist Hospital in Saudi Arabia. An Arabic-language questionnaire was used to interview the participants over a period of 6 months. The questionnaire comprised sociodemographic questions followed by several sections to assess the causes of delay in diagnosis and management. Variables were analyzed descriptively and reported as numbers and percentages using SPSS 22.
Results: A total of 338 patients were included in the study. Most patients were older than 50 years (60.4%), and decreased vision was the main complaint at presentation (81%). Vitreous hemorrhage was the most common diagnosis (46%). Patients’ lack of knowledge about the importance of DR screening programs and problems with healthcare system screenings were the most frequent causes of delay in diabetic retinopathy (DR) diagnosis and management.
Conclusion: DR is still a major cause of permanent blindness that is treatable with regular follow-up and timely management. Even though DR screening and treatment in Saudi Arabia have improved drastically over the last years, socioeconomic and health system factors remain barriers to the improvement of outcomes of DR.
Keywords: diabetic retinopathy, proliferative diabetic retinopathy, vitreous hemorrhage
Introduction
Diabetes mellitus (DM) is a significant, global public health challenge that affected approximately 415 million people worldwide in 2015, and this is expected to increase to 642 million in 2040.1 In 2015, Saudi Arabia had the highest prevalence (17.6%) of DM in the Middle East and North Africa Region.2
Diabetic retinopathy (DR) is the primary cause of vision loss in adults and may have a severe impact on the patient’s quality of life and impose a financial burden on health systems.3–5 The overall global prevalence of DR is estimated to be around 34.6%, accounting for 4.8% of blindness in the world.2,3 In Saudi Arabia, the prevalence of DR was found to be 19.7%, with 53% of them reported to have proliferative diabetic retinopathy (PDR).5 Other studies from different regions of Saudi Arabia have reported a high prevalence of DR ranging from 27.8% to 36%.6,7
The prognosis of DR is strongly correlated with the stage of the disease at presentation; barriers in access to DR screening could delay diagnosis and management, leading to progression of the disease and, consequently, poorer prognosis.3 In Saudi Arabia, despite advancements in DR treatment, well-established screening services, and the availability of free health coverage, there are still a considerable number of patients presenting late with advanced DR and no previous treatment. These patients require more medical and surgical interventions, with guarded prognosis that lead to socioeconomic burdens on the patient and healthcare system. To ensure optimal DR care and improve patient compliance with screening programs, our goal was to understand the barriers (demographic, patient, and healthcare system factors), from the patient perspective, that contribute to DR diagnostic and therapeutic delays among population-based samples of advanced PDR patients at King Khaled Eye Specialist Hospital (KKESH) in Riyadh, Saudi Arabia.
Materials and Methods
This was a cross-sectional questionnaire-based study conducted at a specialized eye hospital in Saudi Arabia, over a 6-month period (December 2020 to May 2021). The study was approved by the Institutional Review Board and Ethics Committee of King Khaled Eye Specialist Hospital (approval number: RD/26001/IRB/0212-20) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all the participants.
Adult patients with advanced PDR (diabetic vitreous hemorrhage, tractional retinal detachment, PDR with corrected distance visual acuity (CDVA) < 20/50, and neovascular glaucoma) who had never been treated with laser photocoagulation or anti-vascular endothelial growth factors were deemed eligible for the study. Only the patients who met the inclusion criteria and signed the consent form were included. The exclusion criteria were DR not reaching an advanced stage, advanced PDR with prior treatment, or advanced proliferative retinopathy not caused by diabetes.
The structured questionnaire used in the study was prepared after a thorough literature review of papers relevant to barrier for diabetic retinopathy screening. The regional and local contexts were also considered to better fit the questionnaire with the study population and objectives.
In the preliminary stage of the questionnaire modification, the patients who presented late with advanced PDR were asked open-ended questions about the reasons for the delay. These responses plus the literature review and input of patients’ health-care providers, including the physicians, counselors, nurses, and patient care coordinators, were collected to create a modified questionnaire.
The modified questionnaire was distributed to 15 patients for questionnaire validation. Additional modifications were made based on this pilot questionnaire and were integrated into the final questionnaire distributed to the study participants by trained paramedic staff.
All the participants were examined by retina specialists. The questionnaire consisted of five sections. Section A included clinical findings from the recent visit. Ophthalmic status was documented at the time of patient recruitment, including patient complaints, time frame from noticing the visual symptoms to being seen by the ophthalmologist, CDVA, type of DM, duration of DM, and stage of DR. Section B detailed baseline demographics such as age, sex, marital status, place of living, level of education, occupation, and income. Section C consisted of three parts; the first part included 5 questions assessing the patient’s knowledge about DR, annual screening programs, source of his/her knowledge, and if the patient was compliant with regular DR screening. The second part included 7 reasons explaining his/her poor compliance to DR screening with an agree/disagree response option for each item (participants were permitted to answer agree to all reasons that applied). Participants’ other reasons which were not included in the questionnaire were included in a comments section. The third part consisted of targeting patient attitude and practice regarding self-care and management towards illness when they first noticed “something was wrong with their vision.” People who answered “I did not go immediately to the nearest hospital to get eye care” were asked five questions explaining their attitude for seeking help when they noticed that their vision was affected, with agree/disagree responses.
Section D consisted of three questions on the type of Health-Care Practitioner (HCP) the patient followed, if he/she had a regular follow-up, and whether some advice or referral for DR screening program had been given. Section E consisted of five questions about the types of health-care facility the patient can access, appointment accessibility, retina service availability, referral process issues, and insurance status. The questionnaire was created in English but distributed to the patients in their language (Arabic). Section A was completed by the retina specialist while the remaining sections were completed by the patient with the help of paramedic staff and relatives or those accompanying them.
In Saudi Arabia, Ministry of Health (MOH) is the major provider of health services followed by other government agencies (eg, army forces medical services, National Guard health affairs, Ministry of Higher Education hospitals) and private sector. Public health-care services provide at three levels: primary, secondary, and tertiary care.
In terms of diabetic retinopathy care, DR screening usually performed in primary care centers or local hospitals followed by referral to higher center if needed. There is minimal variation in some region in terms of the presence, scope and quality of screening programs, access to specialized providers, and affordability of service.
Statistical Analysis
For the purpose of analysis, CDVA was transferred to the logarithm as minimum angle of resolution. Quantitative data are summarized with mean and standard deviation. Categorical data are summarized with percentages. The analysis of variance (ANOVA) test was used to study associations among different variables, with a p-value <0.05 set as a statistically significant result. All statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). All figures were created using the Microsoft Excel (2019, Microsoft Corp.).
Results
Three hundred and thirty-eight patients with advanced DR meeting the inclusion criteria were interviewed and responded to the questionnaire. The majority of patients were >50 years old (mean age 50.54 ± 13.22 years), had type II DM (73.2%), had a mean duration of diabetes of 17.30 ± 8.60 years, had a high school or general equivalency diploma or higher education (>50%), and had no income (28.6%); 61.5% of the patients came from a central region of Saudi Arabia. Table 1 shows the characteristics of the patients in this study.
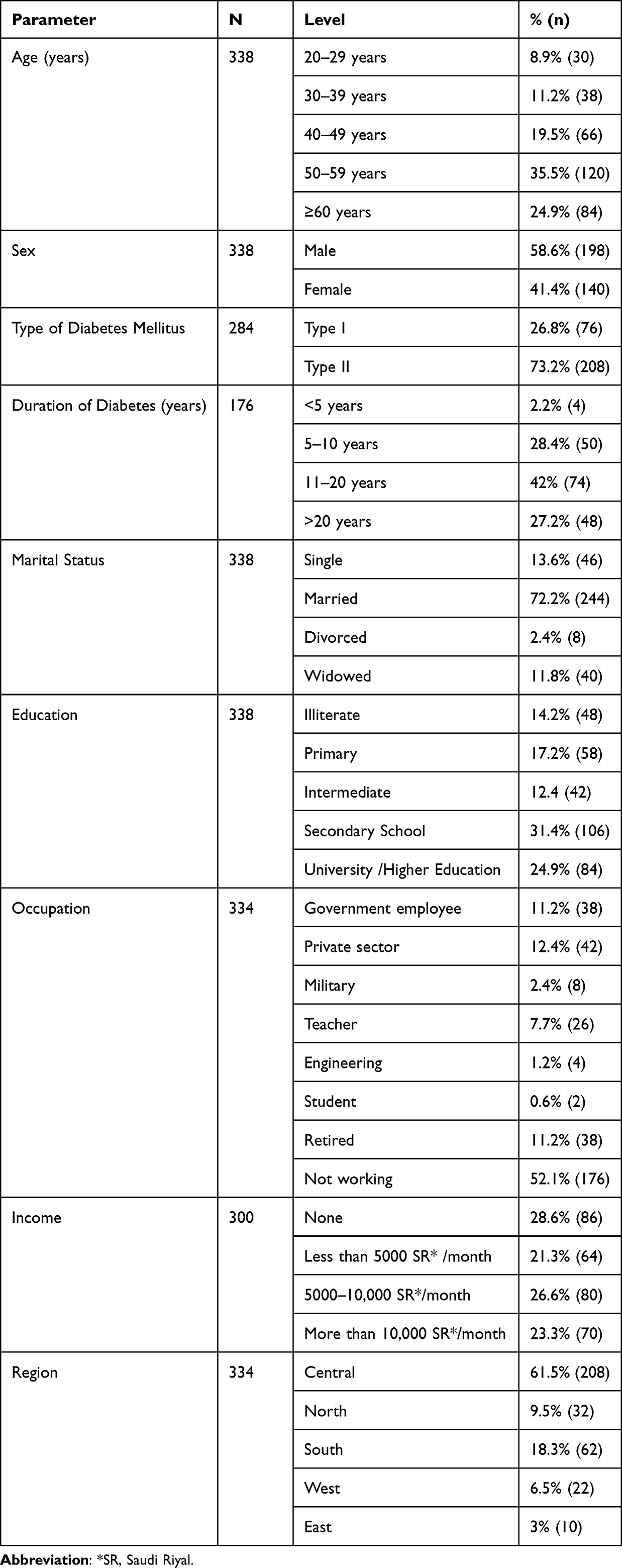 |
Table 1 Demographic Characteristics of Participants |
The mean CDVA (n = 334) was 1.04±0.97 LogMAR (0 to 5 LogMAR) (20/200) in the right eye and 1.15±1.04 LogMAR (0 to 5 LogMAR) (20/300) in the left eye. The most frequent and important complaints were decreased vision (81.7%) and floaters (40.8%) (Table 2). Vitreous hemorrhage was the most common diagnosis (46.4%), followed by tractional retinal detachment (33.9%). The frequency of diagnosis is summarized in Table 3.
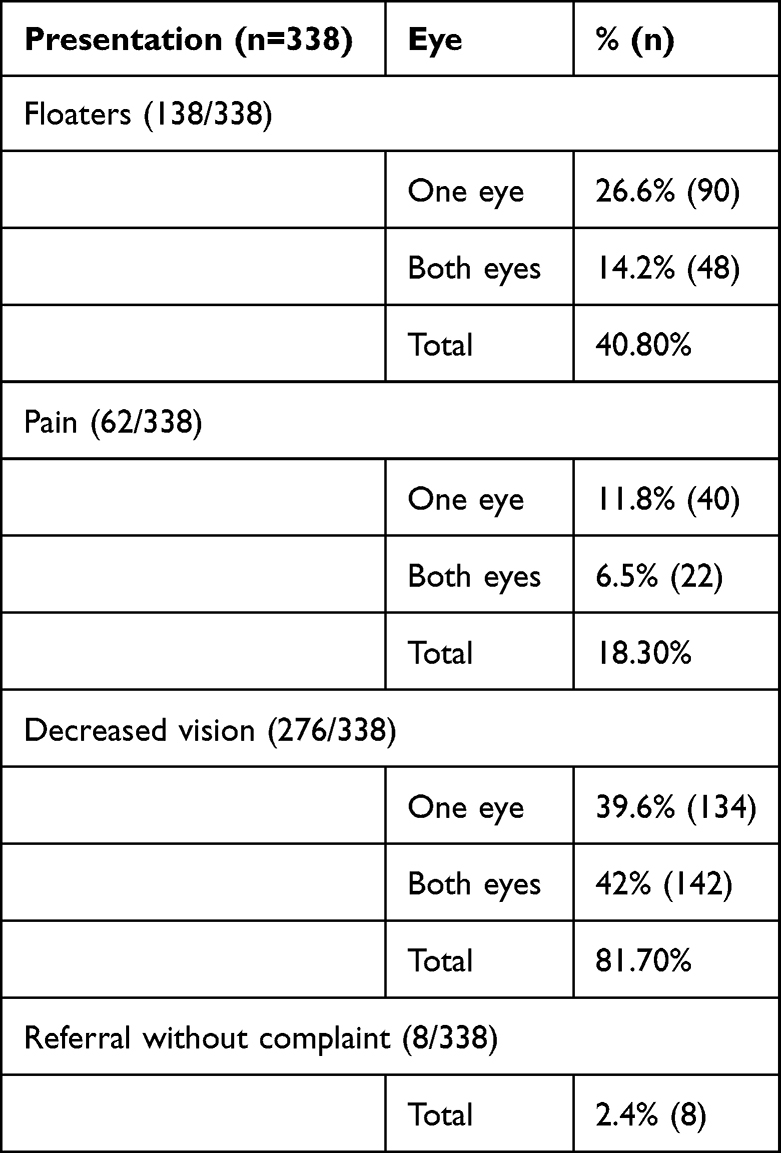 |
Table 2 Participant Presentations |
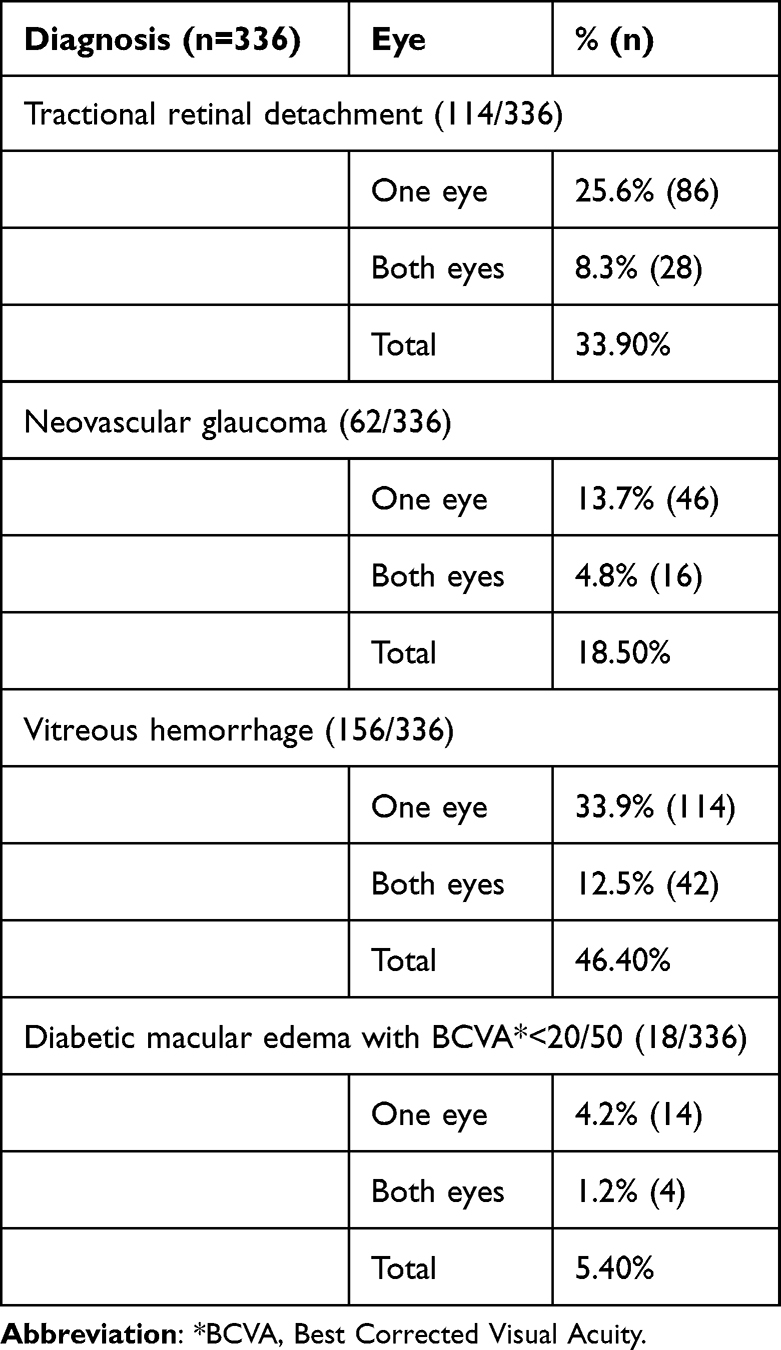 |
Table 3 Participant Diagnosis at Presentation |
Barriers at an Individual Level
Although two-thirds of the patients (65.7%) in our study had heard at least once in their lives about DR and had known that DR can cause visual loss, only 42.6% knew about the importance of annual DR screening exam. Moreover, only 27% of the patients underwent a routine DR annual exam. Physicians and family members were the main source of DR awareness in our study (Table 4).
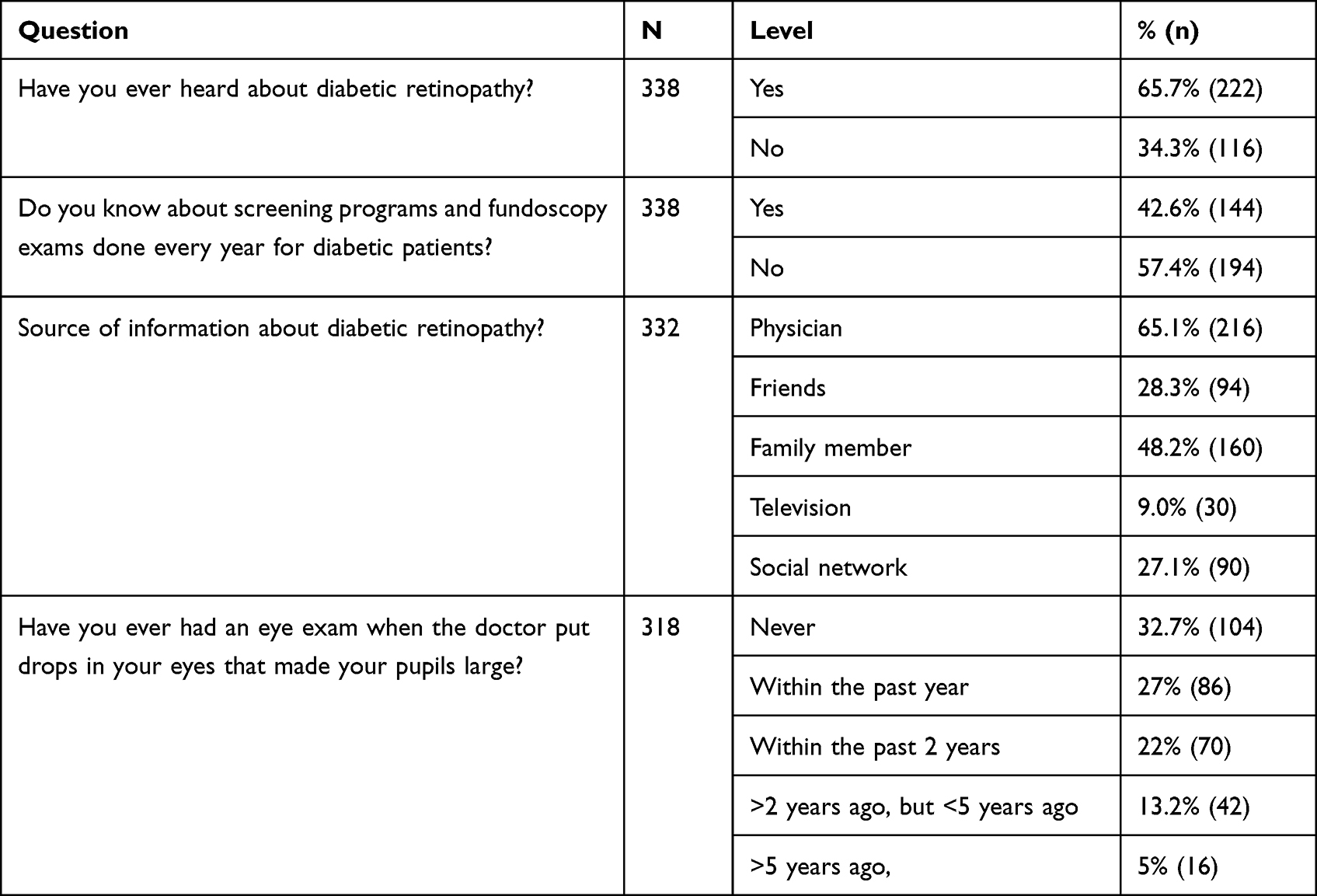 |
Table 4 Participant Knowledge of DR and Screening Programs |
Approximately 21.7% of illiterate patients, 27.6% of patients with primary school education, 30.0% with intermediate school education, 30.8% with secondary school education, and 33.3% with university or higher education underwent routine annual exams. Awareness about the importance of an annual DR screening exam was higher in patients with high levels of education (P = 0.005). Patients who were not undergoing routine DR annual exams were asked what the reasons were that would delay or prevent them from getting their annual screening/test for diabetic eye disease done while their vision was still good; their answers are shown in Figure 1.
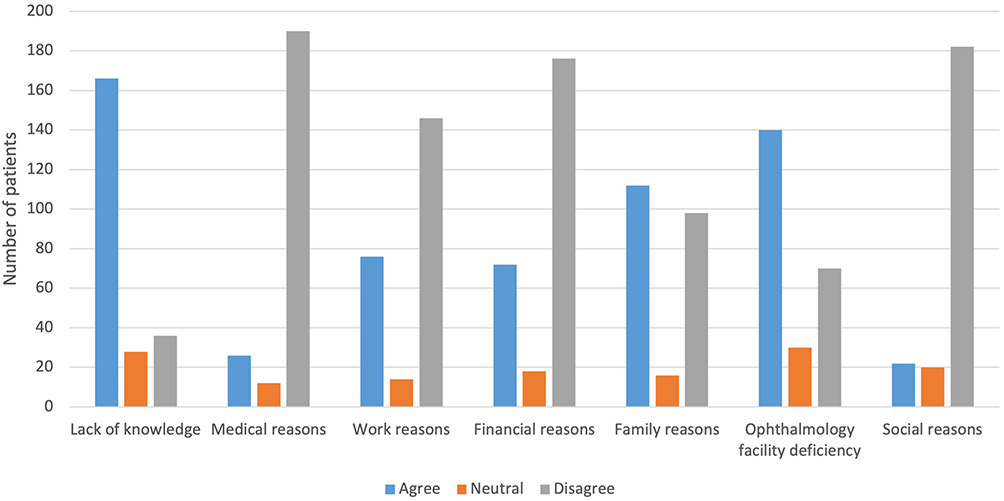 |
Figure 1 Patient perceived barriers to annual diabetic retinopathy screening. |
For those who did not go immediately to the hospital when they noticed that something was wrong with their vision, approximately 67.6% (232) underwent ophthalmology evaluation within one month of noticing eye symptoms. In contrast, 30.5% (102) of the patients waited for over 3 months before visiting the ophthalmology service. These patients were asked what the reasons were that would delay or prevent them from seeking help and getting eye care when they noticed that their vision was affected. Their answers are placed in a descending order by how frequently they were identified by patients; “I do not know the next step to be taken to get medical care and I thought my visual loss was caused by aging”, were the most common reasons (Figure 2).
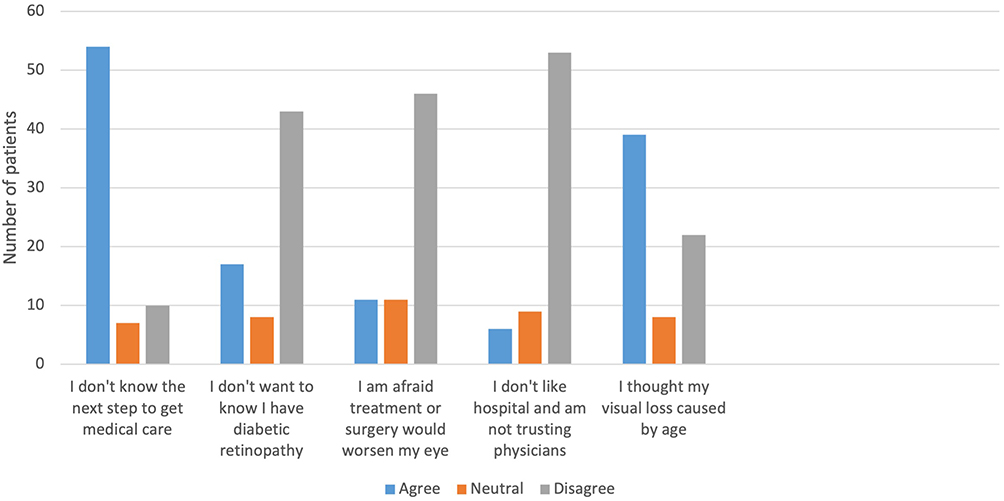 |
Figure 2 Patient attitude toward illness, for those not seeking immediate care for visual impairment. |
On analyzing the sociodemographic characteristics of this subgroup of patients, 102 were found to be mostly old patients (>60 years), 58.8% (60) were not working, 43.1% (44) had no income, 51% (52) underwent follow-up at a primary health care and not a general hospital, and 84.3% (86) did not have health insurance.
Barriers at the Healthcare Provider (HCP) Level
Approximately 81.4% of the patients had a regular follow-up for their systemic diseases; however, almost one-third were not advised or referred to an ophthalmologist for DR screening by their HCP. Moreover, 25.2% of the patients who were referred to an ophthalmologist had a wait period of 6 months or more between the referral by a primary physician until the first visit to an ophthalmologist. The most frequent HCP mentioned by patients in our study were family physicians (34.8%) and general practitioners (33.5%) (Table 5).
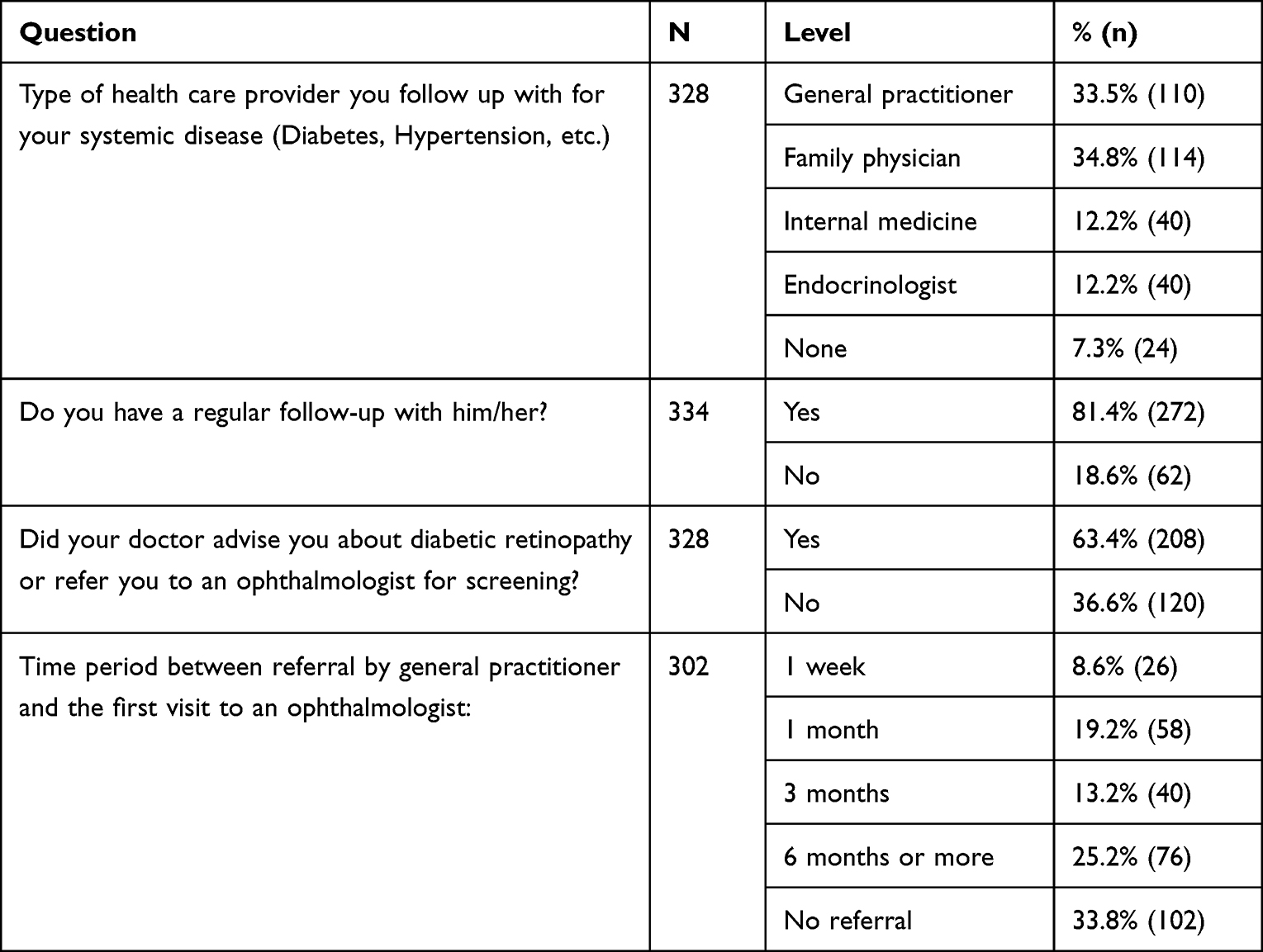 |
Table 5 Characteristics of Healthcare Providers and Their Influence on DR Screening |
Barriers at the Healthcare System Level
Most of the patients in our study had regular follow-ups for their systemic disease at governmental general hospitals or primary health-care centers. However, 42.2% of them faced difficulty in seeking eye care and ophthalmology service in their hospital or nearby hospitals. These difficulties were mostly long appointment time >6 months (57.1%), no retina service (45.1%), and delay or lost referral to tertiary centers if the patient was confirmed with advanced PDR and service was not available (64.5%). Table 6 shows the types of healthcare system and barriers for DR screening and treatment.
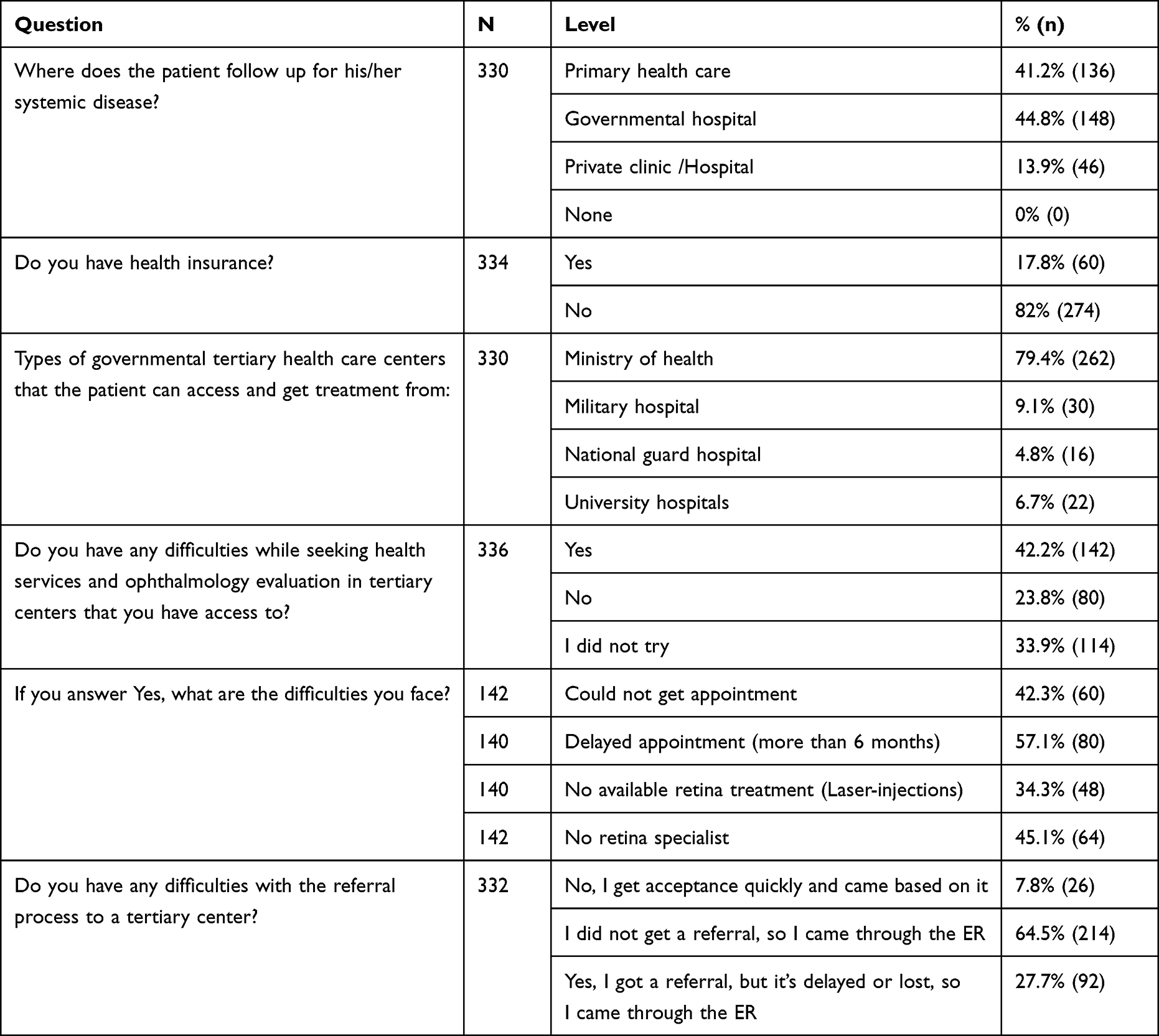 |
Table 6 Health-Care System’s Barrier to DR Screening and Treatment |
Discussion
Diabetic retinopathy is one of the leading causes of visual impairment, and its prevalence is increasing in developing countries.8 Although health education statistics and the literacy rate in Saudi Arabia are comparable to those of developed countries, diabetes-related retinopathy is still widely prevalent.8 Additionally, primary health-care services, which provide free services, are not utilized appropriately, as shown by the results of this study.
We noticed delays between the onset of first DR symptoms and timely interventions, which occurred at several steps in the healthcare process—from the reporting of these symptoms to primary HCPs, to the referral to an ophthalmologist, to the time of the ophthalmologist’s evaluation. Our findings represent a first step towards solving these barriers and improving the outcomes of DR patients.
Our study concluded that most of the patients who presented with advanced DR were >50 years old (60.4%), diabetic for >10 years (69.2%), and had a low or no income (49.9%). These results are comparable to those of other studies done in Saudi Arabia that showed the prevalence of DR was greater in older adults (>50 years).9,10
The low income of most patients in our study (>50%) affected compliance with DR screening, despite it being free of cost, because the transportation and time needed for each appointment affected the patients’ work and life. In addition, patients with diabetes have several hospital appointments, most of which are for routine surveillance, and some patients choose to attend only the appointments they see as essential.
The study also found that more than half the patients (69.2%) had been diagnosed with diabetes for over 10 years, which worsens the scenario, as the chances for DR screening awareness rise with this length of time; however, other factors cannot be ignored in screening compliance.
There was no correlation between urban versus rural place of residence and presentation with advanced DR in our study; 61.5% of the patients herein came from the central region of Saudi Arabia, which can be explained by the central location of our center. We also found no correlation between educational level and DR screening rate, as the patients undergoing routine annual exam were at different educational levels (equal percentages).
The mean CDVA was 1.04±0.97 LogMAR (20/200 decimal) in the right eye and 1.15±1.04 LogMAR (20/300) in the left eye. TRD and vitreous hemorrhage in one or both the eyes were the most frequent diagnoses that indicated advanced stage of the disease and a very late presentation.
More than half the respondents (65.7%) were aware that DM could affect their eyes. This result was slightly lower than that in the other studies in Saudi Arabia that reported a DR awareness of 75.62% and 82.6%, respectively.11,12 A patient’s awareness of their own health and treatment are the foundation to diabetes management.13 Therefore, a lack awareness could be considered as a risk factor for the late presentation of advanced-stage DR. Moreover, although most of our patients were aware of DR (65.7%), only 42.6% knew about annual DR screening, and the annual screening rate was 27%, which is inferior to the previously reported rates for the same population.11,12 Patients’ lack of knowledge and challenges in locating an ophthalmology facility or obtaining an appointment were the most frequent barriers for DR screening (Figure 1). These results indicate the need for high-quality patient-doctor communication regarding the importance of DR screening and an understanding of the patient barriers to DR screening during the referral process. Data from our study showed that 81.4% of the patients underwent regular follow-up with their general practitioner. Utilizing or implementing new modalities for DR screening in primary health-care centers, such as digital wide-field fundus camera and artificial intelligence (AI), could aid in the early diagnosis and treatment of DR.
The delay in the healthcare process is complex and multidimensional and is influenced by patients, HCPs, and health system factors including insurance status and the facility capacity, as reflected in our results.14,15 Overall, these findings highlight the importance of involving both health-care centers and their providers to increase DR screening rates and prevent blindness. Three key recommendations based on the findings from our research are:
Reducing Appointments Inconvenience
Difficulties in getting an appointment with the screening clinic, finding the most convenient time, and scheduling follow-up appointment issues were reported to be important factors that may delay presentation. However, improving accessibility, ensuring flexible appointments, and integrating services were reported to facilitate attendance and reduce inconvenience. Utilizing AI and telemedicine may offer more flexible appointments and reduce the transportation burden.
Increasing the Perception of the Importance of DR Screening
A lack of awareness of the importance of DR screening and the frequency of regular fundus examination were reported to be reasons for patients to present late with advanced disease. Primary health-care providers should regularly perform fundus examinations and should always take the opportunity to educate their patients about DR. National campaigns should be established to increase the general population awareness about DR.
Improving the Screening Service and Health System Referral Process
Using different screening processes, whether virtual or physical, using digital wide-field fundus cameras, and using AI should be encouraged to improve early detection of DR. Offering these services at the primary health-care level can avoid delays associated with referrals.
The large patient-based sample targeting patients with advanced disease in most tertiary ophthalmology centers in Saudi Arabia is the main strength of this study. However, the study had limitations as it is considered a retrospective self-report and participants may have faced difficulties recalling symptoms, onset, and diagnostic consultation with accuracy.
Conclusion
This study represents one of the first efforts to understand, from the patient perspective, the causes of delayed diagnosis and treatment of DR. Patients’ older age, poor income, asymptomatic natural history of DR in the early stages, lack of knowledge, difficulties in approaching the ophthalmology facilities, family responsibilities, and long referral process were the most observed barriers for DR screening and treatment. Utilizing the new technologies of telemedicine and AI and increasing the general population awareness about DR screening recommendations can be the foundations for overcoming these challenges.
Data Sharing Statement
All data relevant to the study are included in the article.
Author Contributions
All authors made a significant contribution to the work reported, in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Al Rasheed R, Al Adel F. Diabetic retinopathy: knowledge, awareness and practices of physicians in primary-care centers in Riyadh, Saudi Arabia. Saudi J Ophthalmol. 2017;31(1):2–6. doi:10.1016/j.sjopt.2017.01.001
3. Liew G, Michaelides M, Bunce C. A comparison of the causes of blindness certifications in England and Wales in working age adults (16-64 years), 1999–2000 with 2009–2010. BMJ Open. 2014;4:e004015. doi:10.1136/bmjopen-2013-004015
4. Sivaprasad S, Gupta B, Crosby-Nwaobi R, Evans J. Prevalence of diabetic retinopathy in various ethnic groups: a worldwide perspective. Surv Ophthalmol. 2012;57:347–370. doi:10.1016/j.survophthal.2012.01.004
5. Schoenfeld ER, Greene JM, Wu SY, et al. Patterns of adherence to diabetes vision care guidelines: baseline findings from the diabetic retinopathy awareness program. Ophthalmology. 2001;108:563–571. doi:10.1016/S0161-6420(00)00600-X
6. Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35:556–564. doi:10.2337/dc11-1909
7. Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82:844–851.
8. Alharbi AMD, Alhazmi AMS. Prevalence, risk factors, and patient awareness of diabetic retinopathy in Saudi Arabia: a review of the literature. Cureus. 2020;12:e11991.
9. Yasir ZH, Hassan AD, Rajiv K. Diabetic retinopathy (DR) among 40 years and older Saudi population with diabetes in Riyadh governorate, Saudi Arabia–A population-based survey. Saudi J Ophthal. 2019;33:363–368. doi:10.1016/j.sjopt.2019.03.001
10. Al‐Rubeaan K, Abu El‐Asrar AM, Youssef AM, et al. Diabetic retinopathy and its risk factors in a society with a type 2 diabetes epidemic: a Saudi National Diabetes Registry‐based study. Acta Ophthal. 2015;93:e140–e147. doi:10.1111/aos.12532
11. Alzahrani SH, Bakarman MA, Alqahtani SM, et al. Awareness of diabetic retinopathy among people with diabetes in Jeddah, Saudi Arabia. Ther Adv Endocrinol Metab. 2018;9:103–112. doi:10.1177/2042018818758621
12. Al Zarea BK. Knowledge, attitude and practice of diabetic retinopathy amongst the diabetic patients of AlJouf and Hail Province of Saudi Arabia. J Clin Diagn Res. 2016;10:NC05. doi:10.7860/JCDR/2016/19568.7862
13. Tan MY. The relationship of health beliefs and complication prevention behaviors of Chinese individuals with Type 2 diabetes mellitus. Diabetes Res Clin Pract. 2004;66:71–77. doi:10.1016/j.diabres.2004.02.021
14. Syed ST, Gerber BS, Sharp LK. Traveling towards disease: transportation barriers to health care access. J Community Health. 2013;38:976–993. doi:10.1007/s10900-013-9681-1
15. Lee BW, Sathyan P, John RK, et al. Predictors of and barriers associated with poor follow-up in patients with glaucoma in South India. Arch Ophthalmol. 2008;126:1448–1454. doi:10.1001/archopht.126.10.1448
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.