")
Back to Journals » Patient Preference and Adherence » Volume 14
Realizing the Potential of the Patient Perspective
Authors Simon TA , Khouri MS , Kou TD , Gomez-Caminero A
Received 8 April 2020
Accepted for publication 6 October 2020
Published 22 October 2020 Volume 2020:14 Pages 2001—2007
DOI https://doi.org/10.2147/PPA.S257355
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Teresa A Simon,1 Marlene S Khouri,2 Tzuyung D Kou,3 Andres Gomez-Caminero3
1Physicians Research Center, LLC, Toms River, NJ, USA; 2Innovation Law, Bristol Myers Squibb, Princeton, NJ, USA; 3Worldwide Patient Safety, Bristol Myers Squibb, Princeton, NJ, USA
Correspondence: Teresa A Simon
Physicians Research Center, LLC, Toms River, NJ 08755, USA
Tel +1 732 818-7900
Email [email protected]
Abstract: Assessing a patient’s perspective on their treatment is part of an increasingly integrated approach to pharmacovigilance and treatment optimization. New tools and methods developed in partnership with patients can capture and quantify cognitive and behavioral aspects of the treatment experience. These treatment insights have the potential to shape the drug development process, as well as supplement patient-reported outcome data in a way that is meaningful to the patient. We highlight examples of tools developed to assess the impact of treatment on the aspects of disease that are of utmost concern to the patient in their daily life.
Keywords: drug development, patient engagement, patient perspective, patient-reported outcome
Introduction
The value of having the patient’s perspective of their disease and treatment experiences is widely recognized. This is reflected by patient engagement in treatment decision making with healthcare professionals (HCPs) in routine clinical practice, and by researchers during drug development.1–3
In routine care, consideration of the “patient experience” involves HCPs engaging their patients in shared decision making about patient treatment options.3 This process has not changed. The decision to treat and choice of medication remain with the HCP and patient. Together they identify the optimal treatment, taking into consideration its benefit–risk profile (efficacy and safety), as well as other factors that may not be assessed during drug development such as comorbidities, other medications, or economic burden. Although the decision to treat is made within this relationship, the decision to follow through with treatment is entirely up to the patient. Much of a patient’s commitment to taking the medication relies on their respect of the provider4 and their ability to trust the prescriber; factors contributing to decreased patient commitment may include fear about experiencing a side effect, misunderstanding the reason the medicine was prescribed and other medicines (including herbal or over-the-counter therapies) that may impact how committed they are to taking an additional medicine.5 Social and cultural aspects may also play a role in a patients commitment to taking a medication.4,6,7
In drug development, understanding the patient experience and perspective has been perceived as an important factor since the 1980s and is documented by the use of validated patient-reported outcome (PRO) measures including both quantitative and qualitative methods.3,8–11 Such validated PRO measures are widely used to capture a patient’s perspective relative to their own symptoms of the disease under study, as well as effects on their physical function and quality of life. In the US, the 21st Century Cures Act encourages an integrated approach to treatment evaluation in which patient experience data, measured as PROs, are incorporated into the drug development process and are used in health authority drug approval frameworks worldwide to inform the interpretation of efficacy and safety data, thereby placing the patient perspective at the heart of the evaluation process.12–15
However, what is lacking is the patient viewpoint on how side effects, tolerability, and treatment burden impact their daily life and the patient’s willingness to tolerate the medication. This commentary is a call to action to propose systematic methods for collecting data on the patient experience associated with the side effects, tolerability, and burden of a given medication.
Realizing the Potential of the Patient Voice
So, where is the gap? From our perspective, patients should be engaged early in the development of a product to gauge if they would be willing to tolerate such a product. There is increasing interest in understanding the patient perspective relative to side effects and tolerability.16,17
During drug development, adverse events (side effects) are reported by the treating physicians and by patients who participated in the clinical trials. The safety profile of a medication is a tally of these adverse events. The adverse events are then listed on a medication label and package insert upon regulatory approval (eg, by the Food and Drug Administration [FDA] in the US or the European Medicines Agency [EMA] in the EU) to inform and assist the HCP in prescribing the best medication for a patient as well as to communicate possible side effects to the patient.
Post-approval and in practice, physicians initiate a conversation with their patient, alone or with the patient’s caregiver, as appropriate, to determine what is important to the patient about managing their illness or disease. For many patients, it would depend on the stage and nature of their illness (Is it acute or chronic? Does it have a high mortality risk?) as well as other factors related to their personal circumstances (Do they work? How many children do they care for? Do they have help? What treatments are affordable? Do their cultural beliefs influence their viewpoint on certain medications?). Such factors are important aspects of treatment selection, but these data are rarely formally collected. It is also important to take into consideration what other medications (prescription and over-the-counter) a patient is taking.
In addition, patients are seldom asked about the personal impact or their own experience of a side effect, which would help with understanding their “willingness to tolerate” and inform an assessment of the burden of the effect. We define tolerability here as how the side effect (adverse event) impacts the person’s day-to-day life (whereas in clinical research, tolerability [or lack of] is usually a term associated with the discontinuation of treatment). There are many questions related to this concept. What is the patient’s threshold of tolerance? Does the patient have a preference for the type of side effect they experience? What is their willingness to tolerate dizziness or nausea – is one more tolerable than the other? What treatment beliefs, concerns, or approaches impact their attitude towards the treatment? What experience do they have with certain side effects? Are some side effects perceived as more concerning because of the patient’s beliefs or prior experiences? Clearly, decisions that must be made regarding treatment choice are highly personal, but there are few reports in the literature as to the best ways to capture the patient perspective.18,19 Similarly, there are few reports that evaluate patient willingness to tolerate a side effect associated with a treatment.20,21
Better understanding of the impact of side effects and tolerability may help to identify certain side effects that a patient population will not tolerate. For example, the medicine may have an acceptable benefit–risk profile; however, there may be certain side effects or consequences that patients in general, or a subset of patients with a specific comorbidity, may not be willing to tolerate. The side effect may have too great an impact on their daily living for the treatment to be worthwhile. Alternatively, if a medication causes a side effect and the treatment for the side effect interacts with an over-the-counter medication that the patient population takes often, this could have downstream consequences that were not well understood during development.
Even after agreeing to a particular treatment plan, a patient may choose not to take the medication. Electronic health records and insurance claims data can show the medication was filled and dispensed, but do not document compliance. Patients may or may not contact the prescriber to request an alternative therapy if they decide not to take what was prescribed; both cognitive and behavioral aspects contribute to the decision. So, where do we go from here?
Missing Data and Health Authority Environment
In order to get to market, a product needs to be safe and efficacious. Safety is currently a concept that, as previously noted, is quantified by counting events; an evaluation of the severity of a particular event is determined by data on discontinuations and hospitalizations as a result of the event. However, should not a safety assessment include patients’ willingness to tolerate the medication? Health authorities are committed to routinely reviewing the benefit–risk profile of medications. These are quantitative assessments. What can be done to improve the understanding of a patient’s willingness to tolerate the side effects of a medication and how the side effects impact their daily lives in addition to the symptoms of their disease? Patients may have improved function, but at what cost?
We believe the tendency is for physicians to focus on quantitative assessments of treatment and clinical outcomes. The literature has shown that side effects resulting in poor tolerability, as well as the impact of these effects on daily life, mental well-being, and quality of life, are often of more interest to the patient than the quantitative assessments physicians tend to prioritize. This can lead to a patient–physician disconnect in the treatment decision process and the overall delivery of care. For example, in a systematic review of patients with rheumatoid arthritis (RA), the 43% patient–physician discordance in assessment of disease was partly attributed to differences in the tools employed; Patient Global Assessment includes the psychological impact of RA whereas the Physician Global Assessment is an assessment of disease activity alone.22
Health authorities, including the FDA and the EMA, support the inclusion of the patient perspective during drug development.12,15 This includes collecting patient experience data and a plan for issuance of patient-focused drug development guidance.23 There is also an ongoing collaboration between the FDA and the EMA to share best practices on patient engagement, called the FDA/EMA Patient Engagement Cluster workgroup.24
The pharmaceutical industry is highly influential in determining the role patients play in drug development25 and medical product sponsors are being actively encouraged to conduct patient preference studies to ensure their clinical development programs are guided by patient concerns and interests and/or specific patient populations.26–28 In 2018, the EU Network for Health Technology Assessment (EUnetHTA) began including patients in its early scientific advice service and has since reported the positive influence patient feedback has had on the recommendations made to companies to improve the quality and appropriateness of data supporting any future HTA assessment of their product.29 Patient recommendations have mostly focused on use of more appropriate clinical endpoints in trials and on the adaptation of inclusion/exclusion criteria to account for different patient subgroups.
The FDA’s increasing receptiveness to the patient perspective was demonstrated by the approval of two products (glycopyrronium for the treatment of primary axillary hyperhidrosis and telotristat etiprate for the treatment of carcinoid syndrome), each of which included the patient experience in the development and approval processes.28,30 The development of these products incorporated qualitative studies to understand the patient perspective and identify themes in the gaps of study data collection. These gaps were then incorporated into the larger study program quantitatively via the recording of specific symptoms related to the disease or refined PROs.28,30–32
The early engagement of patients in drug development is less common for chronic diseases than for rare diseases and, as a consequence, important aspects of the patient perception of the treatment experience may not be captured by study endpoints, potentially limiting the clinical utility of the data generated.33 The types of regulatory decisions that could be supported by patient experience data, and the evidentiary standards for different regulatory contexts, are currently ill defined.34
The Future of Medical Assessment
Improving the Assessment of Side Effects and Tolerability
Although the patient’s perspective on what side effect profile they are willing to tolerate is an individual matter, it is currently discussed after the product is on the market and only between the HCP and the patient. We are advocating for earlier patient engagement in the drug development process so that the patient voice is heard clearly and can help inform the regulatory evaluation of a product (Figure 1A). The collection of cognitive and behavioral information could provide valuable insights into the patient perspective of treatment by highlighting outcomes and side effects that are important to the patient, distinct from PROs which are generally influenced by prior studies of a similar treatment or disease.33 The patient’s perspective or opinion is not currently part of the formal assessment. We propose that during clinical trials, patients should be given the opportunity to rate or weigh any side effect (adverse event) they experience in real time (ie as they are experiencing the event). How does this side effect impact their daily life? What is their willingness to tolerate a certain effect or risk profile associated with the medication? During this engagement, patients should be asked about prior experience with medicines and their beliefs around medications. How can this information be collected and used?
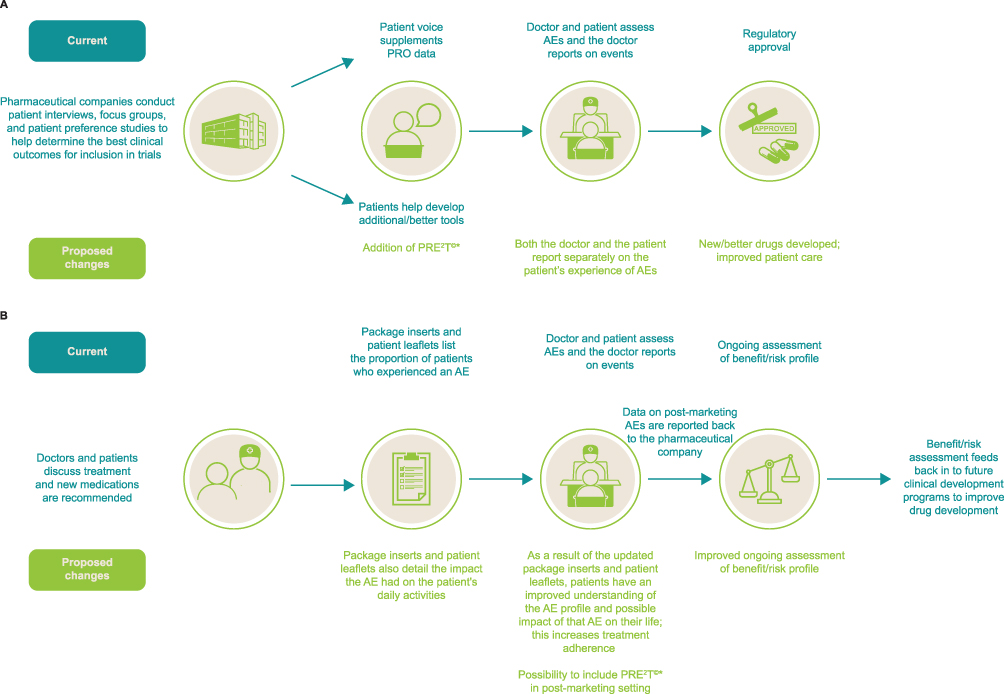 |
Figure 1 The potential of the patient voice in (A) drug development and (B) clinical practice. *PRE2T© currently in development. |
We recognize that an assessment of the true impact of treatment on the patient requires consideration of the patient voice, and we support gaining an understanding of each patient’s detailed account of the nature and personal significance of any side effects of treatment, together with the impact of treatment on aspects of their disease and their psychological and physical well-being.3 Much of this information is not captured electronically; however, qualitative and quantitative methods can be employed to address these gaps in data collection.35–39
Technological advances have facilitated the collection of real-world patient data and the push to use these data has grown exponentially. Given the explosion of real-world data collection, the benefits and risks of a medication can be monitored continually in ongoing assessments. Medication manufacturers and health authorities use a Benefit-Risk Action Team (BRAT) framework.40 Some of the other methods applied to safety and efficacy data to evaluate the benefit–risk profile of a medication are the Quality-adjusted Time Without Symptoms and Toxicity (Q-TWiST) analysis,41 the Risk Assessment and Categorization Tool (RACT), and Multi-Criteria Decision Analysis (MCDA).42,43
Refining Tools
Patients are at the heart of the drug development process, but there are few to no measures that evaluate a patient’s experience and impact a side effect from a medication will have on their daily life. How do we continue to improve the patient experience and patient involvement? It is clear that dialogue among patients, patient advocates, researchers, HCPs, drug developers, and regulatory authorities is key to determine the most appropriate method to assess a patient’s experience with a given treatment in clinical trials. The challenge lies in how to develop tools that accurately capture and quantify the patient experience and tolerability of treatment (ie factors that are regarded by patients as meaningful to treat their illness/disease and improve their quality of life). Current measures that attempt to collect treatment burden are long and cumbersome.44 To realize the true potential of the patient voice, it is critical that new tools are developed to elicit information important to patients in a well-defined and descriptive way to be truly representative of the patient experience.45 There is hope. Knowledge of the issues that influence patient acceptability of treatment is increasing; as a result, new assessments are now being developed in collaboration with both patients and caregivers in various disease areas.46,47
If another dimension of data were to be collected systematically, what clinical utility would it provide? In 2006, Smart proposed that practitioners’ decisions about clinical utility should be based upon four components (appropriateness, accessibility, practicability, and acceptability) to ensure proposed changes to practice are evaluated thoroughly and accurately.48 The recently developed Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events maintained by the US National Cancer Institute is believed to have the potential to provide detailed, descriptive, and patient-centered data to capture the functional burden of possible treatment-related symptoms in oncology trials and to complement data from existing safety assessments. The tool consists of 78 symptoms with one to three items characterizing the frequency, severity, and/or activity interference of each symptom; symptoms are listed in plain language terms and are available in a range of languages. Patients are encouraged to self-report their symptoms, generally on a weekly basis. This new tool was used recently for the first time in an oncology trial, the randomized AURA3 trial of osimertinib or chemotherapy for advanced non-small cell lung cancer, and the patient self-report rate was high, rising from 80% at baseline to around 90% at 24 and 48 weeks.49
Given the evolution of technology, what is lacking is a benefit–risk assessment for the individual patient that takes into consideration other aspects of treatment that are not currently measured (eg cultural differences, economic factors, tolerance). New tools and data visualization can assist patients in understanding the benefit–risk profile of a medication. The use of tools and patient interviews early in drug development has the potential to better inform a patient’s overall experience with a new medication. This includes recording the adverse events they may experience, effectiveness, tolerability, cognitive measures, and cultural aspects, in addition to standard safety data collection. We believe that future programs should include patients not only reporting on outcomes, but rating their experience with adverse events. As such, the lead author (TS) is currently in the process of developing and validating an effect elicitation tool (Patient Reported Effect Elicitation Tool©) that could be implemented in clinical trials, and potentially in a post-marketing setting (Figure 1A and B). The aims of the tool under development will be to gauge how the patient is feeling and assess the impact of any side effects on their daily life. This tool would complement the current conventional measures that evaluate the safety of a medication.
Conclusion
The patient perspective has been included during the drug development process to supplement and enhance the quantitative data collected for regulatory purposes, with the US 21st Century Cures Act allowing for and supporting the collection and use of the patient voice and perspective. As such, at the time of a new drug application, specific questions are asked regarding the use of patient perspective data during the development process. We agree that this is important and we are advocating a similar process and component in understanding the patient perspective as it relates to willingness to tolerate the side effects (adverse events) associated with a medication.
New tools with the ability to detect and quantify tolerability parameters of the treatment are needed to capture the patient voice in a way that can drive decisions in the approval process. Patients working collaboratively with regulatory professionals and HCPs can contribute to the development of standardized processes and methods that can translate into improved experiences both during drug development and in clinical practice.
Acknowledgments
All opinions expressed are those of the authors. Editorial and writing assistance was provided by Linda Brown and Lola Parfitt of Caudex, Oxford, UK, and was funded by Bristol Myers Squibb. John H. Simon developed the Patient Reported Effects Elicitation Tool (PRE2T).
Funding
Funding for this commentary was provided by Bristol Myers Squibb.
Disclosure
Teresa A Simon is a former employee and shareholder of Bristol Myers Squibb; Marlene S. Khouri, Tzuyung Kou, and Andres Gomez-Caminero are all current employees of Bristol Myers Squibb. The authors report no other conflicts of interest in this work.
References
1. Peek ME, Gorawara-Bhat R, Quinn MT, Odoms-Young A, Wilson SC, Chin MH. Patient trust in physicians and shared decision-making among African-Americans with diabetes. Health Commun. 2013;28(6):616–623. doi:10.1080/10410236.2012.710873
2. Beach MC, Keruly J, Moore RD. Is the quality of the patient-provider relationship associated with better adherence and health outcomes for patients with HIV? J Gen Intern Med. 2006;21(6):661–665. doi:10.1111/j.1525-1497.2006.00399.x
3. Harmark L, Raine J, Leufkens H, et al. Patient-reported safety information: a renaissance of pharmacovigilance? Drug Saf. 2016;39(10):883–890. doi:10.1007/s40264-016-0441-x
4. Beach MC, Branyon E, Saha S. Diverse patient perspectives on respect in healthcare: a qualitative study. Patient Educ Couns. 2017;100(11):2076–2080. doi:10.1016/j.pec.2017.05.010
5. American Medical Association. 8 reasons patients don’t take their medications; 2015. Available from: https://www.ama-assn.org/delivering-care/patient-support-advocacy/8-reasons-patients-dont-take-their-medications.
6. Loyola-Sanchez A, Hazlewood G, Crowshoe L, et al. Qualitative study of treatment preferences for rheumatoid arthritis and pharmacotherapy acceptance: indigenous patient perspectives. Arthritis Care Res. 2020;72(4):544–552. doi:10.1002/acr.23869
7. Kretchy IA, Owusu-Daaku FT, Danquah SA, Asampong E. A psychosocial perspective of medication side effects, experiences, coping approaches and implications for adherence in hypertension management. Clin Hypertens. 2015;21(1):19. doi:10.1186/s40885-015-0028-3
8. Rotenstein LS, Huckman RS, Wagle NW. Making patients and doctors happier – the potential of patient-reported outcomes. N Engl J Med. 2017;377(14):1309–1312. doi:10.1056/NEJMp1707537
9. Lievano F, Scarazzini L, Shen F, Duhig J, Jokinen J. The future of safety science is happening now: the modernization of the benefit-risk paradigm. Pharmacoepidemiol Drug Saf. 2017;26(8):869–874.
10. Doyle C, Lennox L, Bell D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open. 2013;3(1):e001570. doi:10.1136/bmjopen-2012-001570
11. Gliklich R, Dreyer N, Leavy M (eds). Registries for Evaluating Patient Outcomes: A User’s Guide.
12. PUBLIC LAW 114–255—DEC. 13. 21st Century Cures Act; 2016.
13. PROTECT. Pharmacoepidemiological research on outcomes of therapeutics by a European Consortium; 2019. Available from: http://protectbenefitrisk.eu/index.html.
14. Centre for Innovation in Regulatory Science. The CIRS-BRAT Framework; 2019. Available from: http://www.cirsci.org/brat/.
15. Administration USFD. 21st Century Cures Act; 2020. Available from: https://www.fda.gov/regulatory-information/selected-amendments-fdc-act/21st-century-cures-act.
16. Kluetz PG, Kanapuru B, Lemery S, et al. Informing the tolerability of cancer treatments using patient-reported outcome measures: summary of an FDA and critical path institute workshop. Value Health. 2018;21(6):742–747. doi:10.1016/j.jval.2017.09.009
17. Corominas H, Espadaler L, Gómez A, et al. Assessing treatment tolerability for rheumatoid arthritis. Validation and practical applications of the ‘TOL-AR-18 questionnaire’. Reumatol Clin. 2020;16(2 Pt 2):149–155. doi:10.1016/j.reuma.2018.06.005
18. François C, Guiraud-Diawara A, Lançon C, et al. A tolerability burden index in schizophrenia: incorporating patient perspective in clinical trial adverse event reporting. J Mark Access Health Policy. 2017;5(1):1372026. doi:10.1080/20016689.2017.1372026
19. Kim J, Singh H, Ayalew K, et al. Use of PRO measures to inform tolerability in oncology trials: implications for clinical review, IND safety reporting, and clinical site inspections. Clin Cancer Res. 2018;24(8):1780–1784. doi:10.1158/1078-0432.CCR-17-2555
20. Henon C, Lissa D, Paoletti X, et al. Patient-reported tolerability of adverse events in Phase 1 trials. ESMO Open. 2017;2(2):e000148. doi:10.1136/esmoopen-2016-000148
21. Thanarajasingam G, Minasian LM, Baron F, et al. Beyond maximum grade: modernising the assessment and reporting of adverse events in haematological malignancies. Lancet Haematol. 2018;5(11):e563–e598. doi:10.1016/S2352-3026(18)30051-6
22. Desthieux C, Hermet A, Granger B, Fautrel B, Gossec L. Patient-physician discordance in global assessment in rheumatoid arthritis: a systematic literature review with meta-analysis. Arthritis Care Res (Hoboken). 2016;68(12):1767–1773. doi:10.1002/acr.22902
23. U.S. Food & Drug Administration. FDA patient-focused drug development guidance series for enhancing the incorporation of the patient’s voice in medical product development and regulatory decision making; 2019. Available from: https://www.fda.gov/drugs/developmentapprovalprocess/ucm610279.htm.
24. Administration USFD. FDA and European medicines agency patient engagement cluster; 2018. Available from: https://www.fda.gov/forpatients/patientengagement/ucm507907.htm.
25. Hansen MB, Nørgaard LS, Hallgreen CE. How and why to involve patients in drug development: perspectives from the pharmaceutical industry, regulatory authorities, and patient organizations. Ther Innov Regul Sci. 2019;2168479019864294.
26. National Institute of Health and Care Excellence. NICE provides first scientific advice on patient preference study design; 2019. Available from: https://www.benefit-risk-assessment.com/nice-provides-first-scientific-advice-on-patient-preference-study-design-14feb19/.
27. Pink Sheet Pharma Intelligence. There’s more to patient experience data submissions than just guidances, advocates tell US FDA; 2018. Available from: https://pink.pharmaintelligence.informa.com/PS122745/Theres-More-To-Patient-Experience-Data-Submissions-Than-Just-Guidances-Advocates-Tell-US-FDA.
28. Pink Sheet Pharma Intelligence. Patient-reported outcome data helps Dermira’s hyperhidrosis drug Qbrexza Win US FDA Nod; 2018. Available from: https://pink.pharmaintelligence.informa.com/PS123423/PatientReported-Outcome-Data-Helps-Dermiras-Hyperhidrosis-Drug-Qbrexza-Win-US-FDA-Nod.
29. Pink Sheet Pharma Intelligence. Patient voice makes impact in scientific advice from EU HTA network; 2019. Available from: https://pink.pharmaintelligence.informa.com/PS141319/Patient-Voice-Makes-Impact-In-Scientific-Advice-From-EU-HTA-Network.
30. Pariser DM, Hebert AA, Drew J, Quiring J, Gopalan R, Glaser DA. Topical glycopyrronium tosylate for the treatment of primary axillary hyperhidrosis: patient-reported outcomes from the ATMOS-1 and ATMOS-2 Phase III randomized controlled trials. Am J Clin Dermatol. 2019;20(1):135–145. doi:10.1007/s40257-018-0395-0
31. Anthony L, Ervin C, Lapuerta P, et al. Understanding the patient experience with carcinoid syndrome: exit interviews from a randomized, placebo-controlled study of telotristat ethyl. Clin Ther. 2017;39(11):2158–2168. doi:10.1016/j.clinthera.2017.09.013
32. Kulke MH, Horsch D, Caplin ME, et al. Telotristat ethyl, a tryptophan hydroxylase inhibitor for the treatment of carcinoid syndrome. J Clin Oncol. 2017;35(1):14–23. doi:10.1200/JCO.2016.69.2780
33. Evans SR, Follmann D. Using outcomes to analyze patients rather than patients to analyze outcomes: a step toward pragmatism in benefit:risk evaluation. Stat Biopharm Res. 2016;8(4):386–393. doi:10.1080/19466315.2016.1207561
34. Pink Sheet Pharma Intelligence. Patient experience data: US FDA’s evidentiary standards should reflect intended use; 2018. Available from: https://pink.pharmaintelligence.informa.com/PS123898/Patient-Experience-Data-US-FDAs-Evidentiary-Standards-Should-Reflect-Intended-Use.
35. Simon TA, Pan X, Kawabata H, Huang HY, Azoulay L. The association between bleeding and the incidence of warfarin discontinuation in patients with atrial fibrillation. Cardiovasc Ther. 2016;34(2):94–99. doi:10.1111/1755-5922.12174
36. Shaw Y, Bradley M, Dominique A, Michaud K, McDonald D, Simon TA. Responding resiliently to chronic disease: rheumatoid arthritis patients’ discourse on coping strategies and challenges. Ann Rheum Dis. 2018;77(Suppl 2):abstract FRI0740–HPR.
37. Simon TA, Bradley M, Lovell D, et al. Using ethnography to understand transition in young adults with JIA. Pediatr Rheumatol. 2018;16(suppl 2):52.
38. Havranek EP, Lapuerta P, Simon TA, L’Italien G, Block AJ, Rouleau JL. A health perception score predicts cardiac events in patients with heart failure: results from the IMPRESS trial. J Card Fail. 2001;7(2):153–157. doi:10.1054/jcaf.2001.24121
39. Leidy NK, Vernon M. Perspectives on patient-reported outcomes: content validity and qualitative research in a changing clinical trial environment. Pharmacoeconomics. 2008;26(5):363–370. doi:10.2165/00019053-200826050-00002
40. Pharmacoepidemiology Research on Outcomes of Therapeutics by a European Consortium. PhRMA BRAT (The pharmaceutical research and manufacturers of America benefit-risk action team). Available from: http://protectbenefitrisk.eu/BRAT.html.
41. Gelber RD, Goldhirsch A. A new endpoint for the assessment of adjuvant therapy in postmenopausal women with operable breast cancer. J Clin Oncol. 1986;4(12):1772–1779. doi:10.1200/JCO.1986.4.12.1772
42. Siebel. Risk assessments for clinical trials; 2017. Available from: https://docs.oracle.com/cd/E88140_01/books/CTMS/ctmsclinicalprog014.htm#:~:text=A%20Risk%20Assessment%20and%20Categorization%20Tool%20%28RACT%29%20template,Templates%20view%20of%20the%20Administration%20-%20Clinical%20screen.
43. Belton V, Stewart T. Multiple Criteria Decision Analysis: An Integrated Approach. Norwell, MA: Kluwer Academic Publishers; 2002.
44. Zidan A, Awaisu A, Hasan S, Kheir N. The Living with Medicines Questionnaire: translation and cultural adaptation into the Arabic context. Value Health Reg Issues. 2016;10:36–40. doi:10.1016/j.vhri.2016.07.001
45. Patrick DL, Burke LB, Gwaltney CJ, et al. Content validity–establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO good research practices task force report: part 1–eliciting concepts for a new PRO instrument. Value Health. 2011;14(8):967–977. doi:10.1016/j.jval.2011.06.014
46. Collier A, Sorensen R, Iedema R. Patients’ and families’ perspectives of patient safety at the end of life: a video-reflexive ethnography study. Int J Qual Health Care. 2016;28(1):66–73. doi:10.1093/intqhc/mzv095
47. Shaw Y, Metes ID, Michaud K, et al. Rheumatoid arthritis patients’ motivations for accepting or resisting disease-modifying antirheumatic drug treatment regimens. Arthritis Care Res (Hoboken). 2018;70(4):533–541. doi:10.1002/acr.23301
48. Smart A. A multi-dimensional model of clinical utility. Int J Qual Health Care. 2006;18(5):377–382. doi:10.1093/intqhc/mzl034
49. Sebastian M, Ryden A, Walding A, Papadimitrakopoulou V. Patient-reported symptoms possibly related to treatment with osimertinib or chemotherapy for advanced non-small cell lung cancer. Lung Cancer. 2018;122:100–106. doi:10.1016/j.lungcan.2018.05.003
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.