")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 8
Real-world hospital costs for nonchemotherapy drugs and nondrug care associated with platinum-based doublets in the first-line setting for advanced nonsquamous non-small-cell lung cancer in Chinese patients: a retrospective cohort study
Authors Chen J, Wu S, Hu C, Yang Y, Rajan N, Chen Y, Yang C, Li J, Chen W
Received 18 October 2015
Accepted for publication 17 February 2016
Published 26 April 2016 Volume 2016:8 Pages 97—111
DOI https://doi.org/10.2147/CEOR.S98548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Jianhua Chen,1 Shengqi Wu,2 Chenping Hu,3 Yicheng Yang,4 Narayan Rajan,5 Yun Chen,4 Canjuan Yang,6 Jianfeng Li,6 Wendong Chen7
1Department of Medical Oncology, 2Department of Research and Education, Hunan Province Tumor Hospital, 3Department of Respiratory, Xiangya Hospital, Central South University, Changsha, Hunan, 4Lilly Suzhou Pharmaceutical Co., Ltd. Shanghai Branch, Shanghai, People's Republic of China; 5Global Health Outcomes Research, Eli Lilly and Co, Indianapolis, IN, USA; 6Division of Health Outcome Research, Normin Health Changsha Representative Office, Changsha, Hunan, People's Republic of China; 7Normin Health, Toronto, ON, Canada
Objective: The objective of this study was to compare hospital costs per treatment cycle (HCTC) for nonchemotherapy drugs and nondrug care associated with platinum-based doublets in the first-line setting for advanced nonsquamous non-small-cell lung cancer (AdvNS-NSCLC) in Chinese patients.
Methods: Patients receiving platinum-based doublets in the first-line setting for AdvNS-NSCLC from 2010 to 2012 in two Chinese tertiary hospitals were identified to create the retrospective study cohort. Propensity score methods were used to create matched treatment groups for head-to-head comparisons on HCTC between pemetrexed–platinum and other platinum-based doublets. Multiple linear regression analyses were performed to rank studied platinum-based doublets for their associations with the log10 scale of HCTC for nonchemotherapy drugs and nondrug care.
Results: Propensity score methods created matched treatment groups for pemetrexed–platinum versus docetaxel–platinum (61 pairs), paclitaxel–platinum (39 pairs), gemcitabine–platinum (93 pairs), and vinorelbine–platinum (73 pairs), respectively. Even though the log10 scale of HCTC for nonchemotherapy drugs and nondrug care associated with pemetrexed–platinum was ranked lowest in all patients (coefficient –0.174, P=0.015), which included patients experiencing any hematological adverse events (coefficient –0.199, P=0.013), neutropenia (coefficient –0.426, P=0.021), or leukopenia (coefficient –0.406, P=0.001), pemetrexed–platinum had the highest total HCTC (median difference from RMB 1,692 to RMB 7,400, P<0.001) among platinum-based doublets because of its higher drug acquisition costs (median difference from RMB 4,636 to RMB 7,332, P<0.001).
Conclusion: Among Chinese patients receiving platinum-based doublets in the first-line setting for AdvNS-NSCLC, the higher acquisition costs for nonplatinum cytotoxic drugs associated with pemetrexed–platinum could be partially offset by its significantly lower hospital costs for nonchemotherapy drugs and nondrug care.
Keywords: nonsquamous non-small-cell lung cancer, hospital costs, platinum-based doublet, first line, Chinese
Introduction
The incidence of lung cancer in the People’s Republic of China has doubled in the past decade1 likely because of aging population, poorly controlled cigarette smoking, and air pollution associated with rapid economic growth.2,3 Similar to the tumor histology distribution of lung cancer in industrialized countries, >80% of diagnosed lung cancer in Chinese patients is non-small-cell lung cancer (NSCLC).4 Because of the challenges associated with early detection,5 NSCLC is often diagnosed at advanced stage6 in Chinese patients, and chemotherapy is the main therapeutic option7 that may extend survival and improve quality of life in patients with advanced NSCLC over best supportive care alone.8 With substantially increased reimbursement coverage for hospital care in the People’s Republic of China,9 health resource utilization associated with chemotherapy for advanced NSCLC has become an important consideration for both clinical and reimbursement decision-making.
Many advances have been made for treating advanced NSCLC in the past decade. One of those advances is the role of tumor histology in predicting clinical effects of chemotherapy for advanced NSCLC.10 Pemetrexed treatment was found be more effective and associated with less toxicity than gemcitabine treatment in the first-line setting11 when treating advanced nonsquamous non-small-cell lung cancer (AdvNS-NSCLC). Pemetrexed treatment may be associated with lower consumption of health resources if the improved clinical effects and better safety profile translate into fewer treating disease-related symptoms and adverse events (AEs). Thus, we conducted this real-world cohort study to test this hypothesis by comparing the allocation of hospital costs per treatment cycle (HCTC) associated with pemetrexed–platinum and other platinum-based doublets commonly used in the first-line setting for AdvNS-NSCLC in a retrospective cohort of Chinese patients.
Methods
This study was designed as a retrospective cohort study including Chinese patients identified from Hunan Province Tumor Hospital (HNPTH) and Xiangya Hospital (XYH), the two major tertiary hospitals providing cancer care to patients living in Hunan province, People’s Republic of China. The observation time set for patient identification was from January 1, 2010, to December 31, 2012. The study protocol was reviewed and approved by the ethics review boards of HNPTH and XYH.
Patient identification
The electronic hospital admission registry databases in the two hospitals were used to search for patients who were hospitalized for lung cancer between January 1, 2010, and December 31, 2012. The identified patients with NS-NSCLC or histologically unclassified lung cancer were linked with their hospital records to confirm their tumor histology and tumor stage according to the definitions made by the International Staging Committee of the International Association for the Study of Lung Cancer in 2009.12 The medical records of patients with biopsy or cytology-confirmed NS-NSCLC, mainly including adenocarcinoma or large-cell carcinoma, were further reviewed for any records of platinum-based doublet treatment in the first-line setting after the diagnosis of stage IIIb or IV cancer. To have a sufficient sample size for data analysis, our study only included patients receiving cisplatin- or carboplatin-based doublets with pemetrexed (given with supplementation of folic acid and vitamin B12 and approved to treat advanced NSCLC with cisplatin in the first-line setting), docetaxel, paclitaxel, gemcitabine, or vinorelbine. Patients receiving tyrosine kinase inhibitor, epidermal growth factor receptor monoclonal antibody, and/or anti-angiogenic therapy in the first-line setting were excluded in order to control their confounding effects on tumor response and clinical toxicity associated with the studied platinum-based doublets. This study also excluded patients who initialized first-line chemotherapy out of HNPTH or XYH or who had missing information on hospital costs during follow-up.
Data extraction
The follow-up time defined for data extraction was set from the hospitalization with the first administration of platinum-based doublets to the hospitalization with the last administration of platinum-based doublets. We reviewed the hospital records before the first administration of the studied doublets to extract baseline characteristics of patients that included demographic information, type of health insurance plan, smoking status, physical function assessed by the Eastern Cooperative Oncology Group’s performance status, baseline marrow function, and disease information on tumor stage, tumor histology, and metastasis status. We also reviewed hospital prescription records to extract treatment information on administration doses and schedule of the studied platinum-based doublets. Additionally, the prescription records for granulocyte colony-stimulating factor (G-CSF), erythropoietin, thrombopoietin, interleukin 11, and blood products (blood transfusion and/or platelet infusion) were extracted for the patterns of treating hematological AEs13 associated with the studied platinum-based doublets. The extracted information also included tumor response, which was assessed every two treatment cycles using Response Evaluation Criteria in Solid Tumors (Version 1.0)14 and clinical toxicity, which was assessed by the Common Terminology Criteria for Adverse Events (Version 3.0) with modified criteria for anemia15 in the two study hospital settings. The laboratory blood testing results for hemoglobin, white blood cell count, neutrophilic granulocyte count, and platelet count during follow-up were also extracted as supplemental information to confirm hematological AEs. Finally, hospital discharge billing records associated with each hospitalization during follow-up were reviewed to extract hospital costs associated with billable medications and services. Because the billing records only provided the cost sum by category, we tracked the prescriptions of chemotherapy drugs (platinum agent and cytotoxic agent) to estimate the chemotherapy drug costs. The hospital costs were classified into three categories in this study: chemotherapy drug costs, nonchemotherapy drug costs, and nondrug care costs. The perspective of the hospital costs was the People’s Republic of China’s health system, and any hospital costs were taken into account irrespective of their reimbursement status.
Outcome measures
The primary outcome measure in our study was HCTC. The extracted hospital costs from the two study hospitals were categorized by platinum agents, nonplatinum cytotoxic agents, nonchemotherapy drugs, and nondrug care for the allocation of hospital costs. The secondary outcome measures in our study included tumor response, which was classified as complete response, partial response, stable disease, and progressive disease (PD), defined by Response Evaluation Criteria in Solid Tumors (Version 1.0). The secondary outcome measures also included clinical toxicity measured by hematological and nonhematological AEs. Because early treatment discontinuation often occurred within two treatment cycles because of PD, there is often lack of tumor response assessment in these patients. To include the patients with early treatment discontinuation in the data analysis, we further classified tumor response as tumor control (defined as complete response, partial response, or stable disease) and treatment failure (defined as PD or no tumor response assessment associated with early treatment discontinuation) for data analysis. To control the bias associated with missing information on hematological toxicity assessment associated with platinum-based doublets, we used both recorded hematological AE information from hospital medical notes and homological toxicity assessment based on laboratory blood testing results to measure occurrence and severity of hematological AEs associated with studied platinum-based doublets.
Data analysis
One-way analysis of variance and Fisher’s exact test were used to describe the differences in patients’ baseline characteristics and treatments used to prevent and/or treat hematological AEs in patients receiving the five studied doublets. Propensity score methods were used to create matched pairs for pemetrexed–platinum versus the other four studied platinum-based doublets, respectively, after balancing baseline characteristics of patients and treatments for hematological AEs. The matching condition was set as propensity score difference between matched pairs <0.001 when using the greedy approach.16 McNemar’s test was used for head-to-head comparisons of tumor response and occurrences of AEs between propensity score-matched treatment groups. Wilcoxon signed rank test was used to compare the allocation of HCTC and HCTC for nonchemotherapy drugs and nondrug care between matched treatment groups. We further used multiple logistic or linear regression analyses with generalized estimating equation to adjust imbalanced baseline variables (P<0.5 after propensity score matching) in propensity score-matched patients to confirm the observed differences in tumor response, clinical toxicity, and the allocation of HCTC between the matched treatment groups for pemetrexed–platinum versus the other four studied platinum-based doublets.17 Finally, we used vinorelbine–platinum as reference to rank the association between five studied platinum-based doublets and the log10 scale of HCTC for nonchemotherapy drugs and nondrug care in all patients, which included patients stratified by their tumor response and hematological AEs using multiple linear regression analyses with adjustment of baseline characteristics and treatments for hematological AEs. Statistical significance was defined as two-sided P-value <0.05 in this study, and SAS 9.2 was used to perform the data analyses described earlier.
Results
The initial search of electronic hospital admission registry databases identified 4,558 patients who were hospitalized for lung cancer. We first excluded 3,054 patients without chemotherapy treatment in hospital and 698 patients with ineligible histology or lack of tumor histology information (333 with squamous histology, 207 with mixed squamous and nonsquamous histology, 91 with small-cell histology, and 67 without biopsy or cytology-confirmed tumor histology). We further excluded 140 patients with tumor stage less than IIIb, 179 patients due to treatment received (166 patients receiving first-line chemotherapy other than the studied five platinum-based doublets and 13 patients receiving tyrosine kinase inhibitor or epidermal growth factor receptor monoclonal antibody in the first-line setting), and 40 patients due to missing hospital billing information. The final data analyses were based on 447 patients who met all eligibility criteria, including 259 patients receiving five studied doublets in HNPTH and 188 patients treated by pemetrexed-, docetaxel-, or gemcitabine-contained doublet in XYH. The patient identification processes in the two hospitals are illustrated in Figure 1.
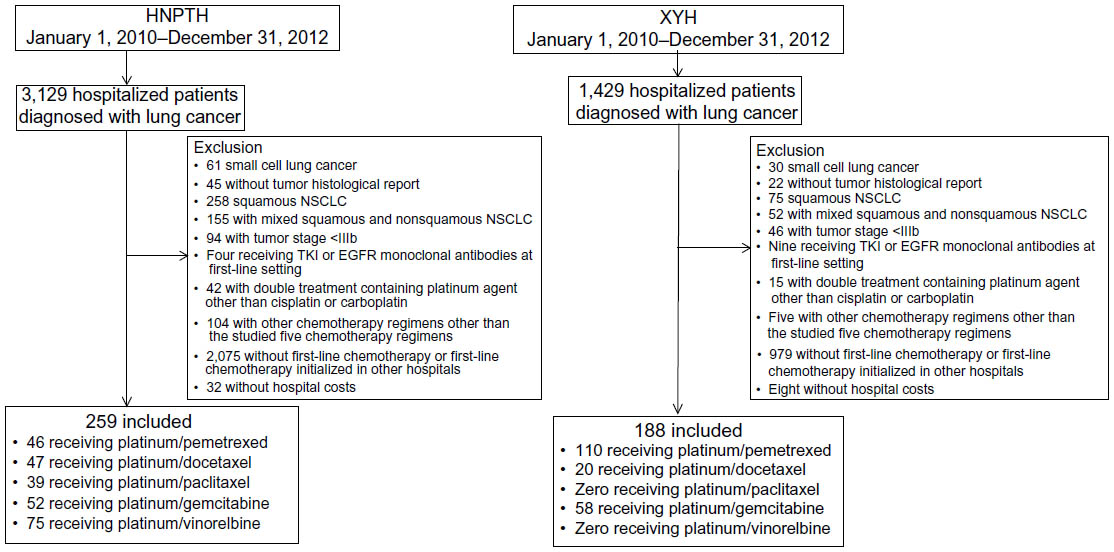 | Figure 1 A flow chart of the patient identification process in the two study hospital settings in Changsha, the provincial capital city of Hunan, People’s Republic of China. |
Patient baseline characteristics and patterns of care
Of the 447 eligible patients, 34.9% received pemetrexed–platinum (n=156), 15% received docetaxel–platinum (n=67), 8.7% received paclitaxel–platinum (n=39), 24.6% received gemcitabine–platinum (n=110), and 16.8% received vinorelbine–platinum (n=75). The comparisons of baseline characteristics of patients across the five treatment groups (Table 1) observed significant differences in the distributions of public health insurance plan for urban residents (35.9%–58.3%, P=0.015), Eastern Cooperative Oncology Group performance status of 0 (4.5%–25.6%, P<0.001) and 1 (69.2%–91.0%, P=0.004), adenocarcinoma histology (95.5%–100%, P=0.014), and pleural metastasis (11.9%–32.1%, P=0.001). Further comparisons of treatment patterns observed highly uneven distribution of the studied platinum-based doublets by hospital setting, hospital admission year, platinum agents, and treatments for treating hematological AEs. For example, pemetrexed was used more frequently in XYH than in HNPTH (58.5% versus 17.8%, P<0.001). The most frequently used doublets in the three hospital admission years were vinorelbine–platinum in 2010 (77.3%, P<0.001), gemcitabine–platinum in 2011 (36.4%, P=0.002), and pemetrexed–platinum in 2012 (43%, P<0.001). Cisplatin was used more frequently in the combination treatment with vinorelbine (93.3%, P<0.001), and carboplatin was used more frequently in the combination treatment with paclitaxel (43.6%, P<0.001). G-CSF was used most frequently in patients receiving paclitaxel treatment (76.9%, P=0.061), and interleukin 11 was used most frequently in patients receiving vinorelbine treatment (16%, P<0.001). The five studied platinum-based doublets were each administered every 3 weeks. Pemetrexed, docetaxel, and paclitaxel were each administered once at day 1 per treatment cycle, while gemcitabine and vinorelbine were administered at both day 1 and day 8 per three-week treatment cycle. The administered doses of the five studied doublets were highly consistent with the recommended doses. The completed treatment cycles associated with the five studied doublets significantly differed even though the average completed treatment cycles had a small range (two to three cycles, P<0.001). The comparisons of treatment patterns across the five treatment groups are summarized in Table 1.
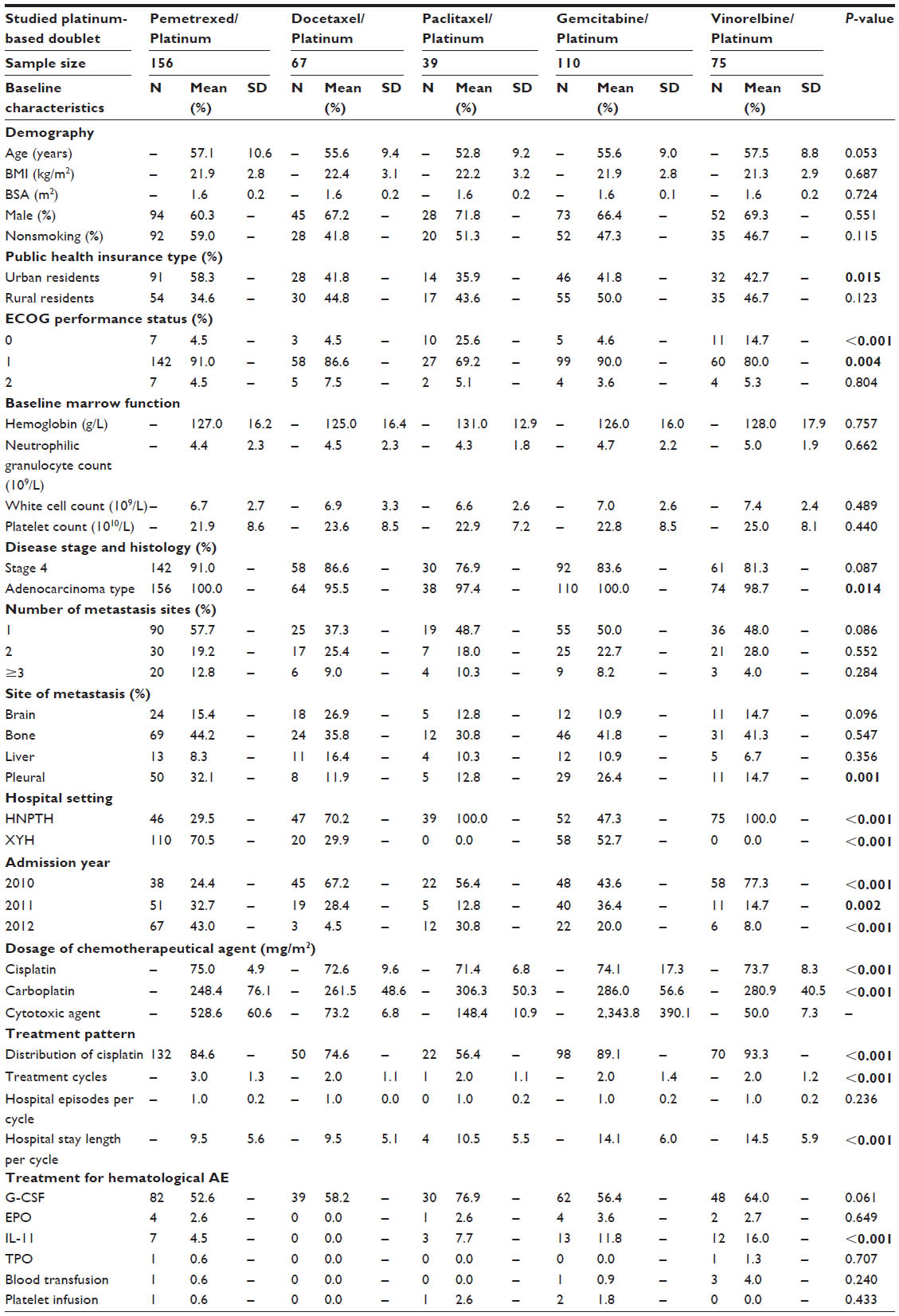 | Table 1 A summary of baseline characteristics of patients and treatment pattern associated with the five studied platinum-based doublets in the first-line setting for AdvNS-NSCLC |
Comparisons of tumor response, clinical toxicity, and allocation of HCTC between propensity score-matched treatment groups
Propensity score methods created 61 matched pairs for pemetrexed–platinum versus docetaxel, 39 matched pairs for pemetrexed–platinum versus paclitaxel–platinum, 93 matched pairs for pemetrexed–platinum versus gemcitabine–platinum, and 73 matched pairs for pemetrexed–platinum versus vinorelbine–platinum for head-to-head comparisons.
Tumor response
The head-to-head comparisons of tumor response indicated that pemetrexed–platinum was associated with significantly higher tumor control rates as compared to the docetaxel (62.3% versus 24.6%, relative risk [RR] 2.533, P<0.001), gemcitabine (61.3% versus 40.9%, RR 1.500, P=0.009), or vinorelbine doublets (63% versus 30.1%, RR 2.091, P<0.001). After adjusting imbalanced baseline variables between matched treatment groups, treatment with pemetrexed–platinum was associated with a significantly lower risk of treatment failure as compared to the other four doublets (odds ratio [OR] ranged from 0.081, P<0.001, for the comparison with vinorelbine–platinum to 0.276, P=0.001, for the comparison with gemcitabine–platinum). The head-to-head comparisons of tumor response are summarized in Table 2.
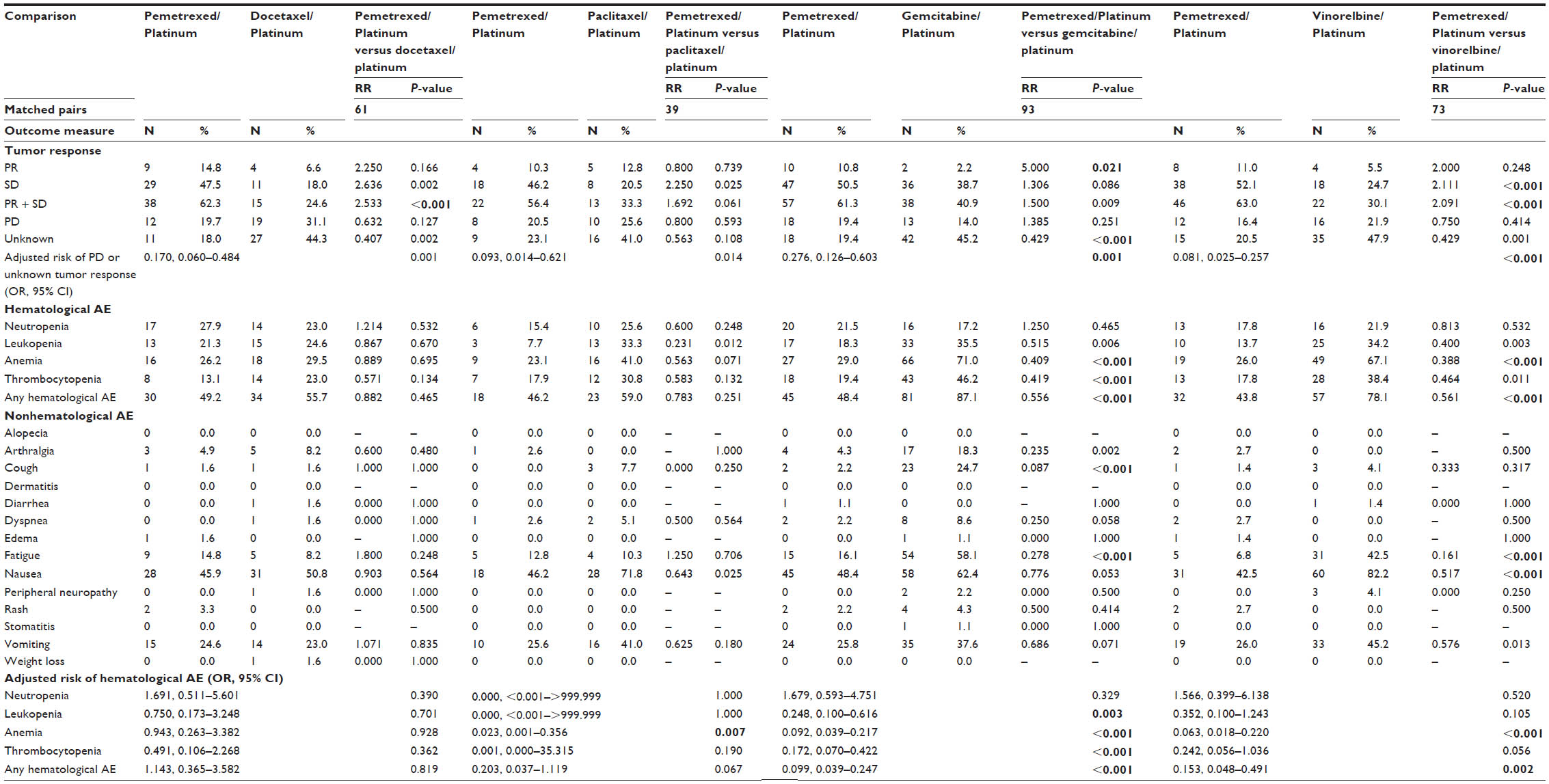 | Table 2 Adjusted comparisons on tumor response and AEs between propensity score-matched treatment groups for pemetrexed/platinum versus the other four studied doublets in the first-line setting for AdvNS-NSCLC |
Clinical toxicity
Head-to-head comparisons of occurrences of AEs indicated that pemetrexed–platinum was highly comparable to docetaxel–platinum regarding clinical toxicity but was associated with fewer hematological AEs than the other three studied doublets. After further adjusting imbalanced baseline variables between the matched treatment groups, pemetrexed–platinum had significantly lower risk of anemia (OR 0.023, P=0.007) than paclitaxel–platinum; significantly lower risks of leukopenia (OR 0.248, P=0.003), anemia (OR 0.092, P<0.001), thrombocytopenia (OR 0.172, P<0.001), and any hematological AE (OR 0.099, P<0.001) than gemcitabine–platinum; and significantly lower risks of anemia (OR 0.063, P<0.001) and any hematological AE (OR 0.153, P=0.002) than vinorelbine–platinum. For nonhematological AEs, pemetrexed–platinum had significantly lower rates of nausea than paclitaxel–platinum (46.2% versus 71.8%, RR 0.643, P=0.025); significantly lower rates of arthralgia (4.3% versus 18.3%, RR 0.235, P=0.002), cough (2.2% versus 24.7%, RR 0.087, P<0.001), and fatigue (16.1% versus 58.1%, RR 0.278, P<0.001) than gemcitabine–platinum; and significantly lower rates of fatigue (6.8% versus 42.5%, RR 0.161, P<0.001), nausea (42.5% versus 82.2%, RR 0.517, P<0.001), and vomiting (26% versus 45.2%, RR 0.576, P=0.013) than vinorelbine–platinum. The head-to-head comparisons of the occurrence rates of hematological and nonhematological AEs between the propensity score-matched treatment groups for pemetrexed–platinum versus the other four studied doublets are summarized in Table 2.
Allocation of HCTC
Comparisons of the allocation of HCTC demonstrated that pemetrexed–platinum was associated with significantly higher nonplatinum cytotoxic drug costs (median differences ranged from RMB 4,636 to RMB 7,332 [1 RMB= US$0.16]) but significantly less HCTC for nonchemotherapy drugs and nondrug care (median difference ranged from –RMB 3,251 to –RMB 1,478) than the other four studied doublets. Pemetrexed–platinum was comparable to the other four studied platinum-based doublets regarding the HCTC for platinum agent and nondrug care. Because the saved costs for nonchemotherapy drugs and nondrug care associated with pemetrexed–platinum treatment did not completely offset the high acquisition costs of pemetrexed, the total HCTC associated with pemetrexed–platinum remained significantly higher than the other four studied platinum-based doublets (median increase ranged from RMB 1,692 to RMB 7,400). Further adjusting imbalanced baseline variables after propensity score matching observed that the log10 scale of HCTC for nonchemotherapy drugs and nondrug care associated with pemetrexed–platinum treatment was significantly less than that for docetaxel (coefficient −0.246, P=0.003), paclitaxel (coefficient −0.351, P<0.001), or gemcitabine doublet (coefficient −0.194, P=0.001). The head-to-head comparisons of the allocation of HCTC between propensity score-matched treatment groups for pemetrexed–platinum versus the other four studied doublets are summarized in Table 3.
 | Table 3 Adjusted comparisons on the allocation of HCTC between propensity score-matched treatment groups for pemetrexed/platinum versus the other four studied doublets in the first-line setting for AdvNS-NSCLC |
Ranking the studied doublets by their impact on HCTC for nonchemotherapy drugs and nondrug care in patients stratified by tumor response and hematological toxicity
The multiple linear regression analysis ranked pemetrexed–platinum to have the lowest coefficient (−0.174, P=0.015) for the log10 scale of HCTC for nonchemotherapy drugs and nondrug care among the five studied platinum-based doublets in 409 patients irrespective of their status of tumor control and hematological AEs (Figure 2A). The coefficient associated with pemetrexed–platinum was also ranked the lowest for the log10 scale of HCTC for nonchemotherapy drugs and nondrug care in 272 patients experiencing any hematological AE (coefficient −0.199, P=0.013; Figure 2B), in 73 patients experiencing neutropenia (coefficient −0.426, P=0.021; Figure 2C), and in 119 patients experiencing leukopenia (coefficient −0.406, P=0.001; Figure 2D). However, the coefficient associated with both docetaxel- (coefficient 0.261, P=0.006) and gemcitabine-contained doublets (coefficient 0.252, P=0.021) for the log10 scale of HCTC for nonchemotherapy drugs and nondrug care was significantly higher than vinorelbine–platinum in 272 patients experiencing any hematological AE. No other significant differences were observed regarding the coefficients associated with the five studied platinum-based doublets for the log10 scale of HCTC for nonchemotherapy drugs and nondrug care in patients experiencing tumor control (Figure 2E), treatment failure (Figure 2F), no hematological AE (Figure 2G), anemia (Figure 2H), or thrombocytopenia (Figure 2I).
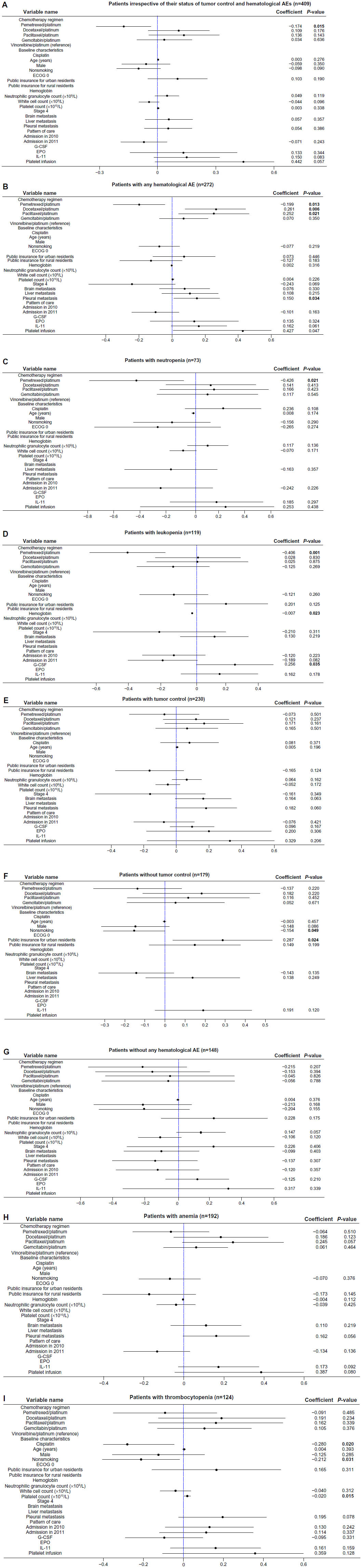 | Figure 2 Impact of the studied five platinum-based doublets on the log10 scale of HCTC for nonchemotherapy drugs and nondrug care in patients stratified by their tumor control status and hematological AEs. |
Discussion
To our knowledge, this study is the first to assess real-world data to demonstrate that superior tumor response and better safety profile associated with chemotherapy could save hospital costs for nonchemotherapy drugs and nondrug care in the first-line setting for AdvNS-NSCLC in Chinese patients. Among the five platinum-based doublets frequently used to treat AdvNS-NSCLC in Chinese patients, pemetrexed was the most expensive nonplatinum cytotoxic agent. However, our study observed that pemetrexed treatment was associated with superior tumor response and less clinical toxicity, which could reduce the utilization of nonchemotherapy drugs and nondrug care and offset the drug acquisition costs of pemetrexed–platinum. Additionally, our study also observed that pemetrexed–platinum was associated with the lowest hospital costs for nonchemotherapy drugs and nondrug care in patients experiencing neutropenia or leukopenia, the two common hematological AEs associated with chemotherapy. This may suggest that pemetrexed treatment could further save hospital costs for nonchemotherapy drugs and nondrug care by causing less severe hematological toxicity. Thus, our study is a great example to demonstrate economic benefits associated with tumor responses and clinical toxicity of chemotherapy when treating cancer patients.
The superior tumor response and better safety profile associated with pemetrexed treatments in the real-world first-line setting for AdvNS-NSCLC were consistent with what were observed in Chinese patients receiving pemetrexed treatment in the second-line setting.18 Our study observed superior tumor response but highly comparable clinical toxicity associated with pemetrexed treatment when compared with docetaxel–platinum doublet. Because the highly comparable clinical toxicity between the two doublets should consume similar hospital resources for AE management, the observed superior tumor response associated with pemetrexed treatment was the only known factor contributing to the saved hospital costs for nonchemotherapy drugs and nondrug care associated with pemetrexed treatment. A recent Phase III trial reported that the increased utilization of health resources associated with maintenance therapy in tumor-controlled patients was mainly related to hematological AE management, including blood transfusion, G-CSF, and anti-infection medications.19 Thus, we believe that the better safety profile associated with pemetrexed treatment could further save hospital costs for nonchemotherapy drugs and nondrug care when compared with the paclitaxel-, gemcitabine-, or vinorelbine-based doublet, the three cytotoxic agents usually associated with significant hematological toxicity. Additionally, the better safety profile of pemetrexed treatment was mainly related to hematological toxicity. The saved hospital costs for nonchemotherapy drugs and nondrug care associated with pemetrexed treatment could be the result of less use of health resources for hematological AEs. With the rare use of blood transfusions and platelet infusions in our study cohort, the reduced hospital costs for nonchemotherapy drugs associated with pemetrexed treatment may suggest reduced utilization of nonchemotherapy drugs managing hematological toxicity. Future studies are needed to further confirm our hypothesis on the saved drug costs for hematological toxicity in patients receiving pemetrexed treatment.
Our study ranked the five studied doublets for their impact on hospital costs for nonchemotherapy drugs and nondrug care in patients stratified by tumor response and hematological AE to further explore any other factors that could affect hospital costs for nonchemotherapy drugs and nondrug care. Pemetrexed–platinum doublet was associated with significantly lower hospital costs for nonchemotherapy drugs and nondrug care in patients who experienced neutropenia or leukopenia, the two conditions usually treated with G-CSF and antibiotics.20 This finding suggests that the hematological toxicity associated with pemetrexed treatment could be less severe. Because the small sample size does not allow us to adjust possible confounding effects associated with tumor response and nonhematological AEs in these patients, future studies are needed to confirm our hypothesis regarding the impact of AE severity on hospital costs for nonchemotherapy drugs and nondrug care. Another important factor contributing to lower hospital costs for nonchemotherapy drugs and nondrug care associated with pemetrexed treatment is the treatment administration schedule. Both gemcitabine and vinorelbine were administered twice at days 1 and 8 per treatment cycle, and the length of hospital stay per treatment cycle was increased by 4–5 days when compared to pemetrexed treatment, which was administered only once at day 1 per treatment cycle. Thus, the shorter hospital stay associated with pemetrexed treatment undoubtedly reduced hospital costs for nonchemotherapy drugs and nondrug care.
This study has several significant implications on clinical practice, research, and health policy-making. First, the generated clinical and economic evidences in this study could further reduce uncertainty associated with tumor response, clinical toxicity, and medical costs of platinum-based doublets for AdvNS-NSCLC in the first-line setting. Second, our study design and study methods can be used in other settings to explore the economic impact of clinical effectiveness and toxicity associated with chemotherapy. Third, the real-world tumor response, clinical toxicity, and hospital costs associated with the five studied doublets in our study can be applied to future cost-effectiveness analyses and budget impact analysis, which have been increasingly used to support reimbursement decision-making in the People’s Republic of China. Finally, the tumor response associated with pemetrexed treatment in our study is much stronger than previous studies that mainly included Caucasian patients. We had a hypothesis that Chinese ethnicity could be more sensitive to pemetrexed than other cytotoxic agents. Thus, future studies are needed to confirm our hypothesis regarding the impact of ethnicity on clinical and economic benefits of pemetrexed treatment for AdvNS-NSCLC in the first-line setting.
There are several limitations associated with the retrospective nature of this study. First, about half of the eligible patients had no tumor response assessment because of early treatment discontinuation. Because our study was unable to identify the cause of treatment discontinuation, missing information on tumor response in patients with early treatment discontinuation could bias our comparisons on tumor response. Second, our study was unable to capture clinical toxicity associated with the studied platinum-based doublets outside of the two participating hospitals. The longer hospital stay associated with gemcitabine and vinorelbine doublets increased observation time for treatment toxicity and might overestimate the clinical toxicity associated with the two treatments. Third, the hospital settings were not adjusted in our analysis because paclitaxel- and vinorelbine-contained doublets were not used in XYH. Fourth, this study was unable to make full adjustment of potential confounding effects associated with social economic status on hospital costs for nonchemotherapy drugs and nondrug care due to the lack of information. Because the price of vinorelbine was much lower than other nonplatinum cytotoxic agents, it may be used more often in patients with lower socioeconomic status. Therefore, the confounding effects associated with possible lower socioeconomic status in patients receiving vinorelbine treatment could have overestimated the cost saving associated with pemetrexed treatment for nonchemotherapy drugs and nondrug care. Fifth, selection bias could also be introduced by the propensity score methods that only selected matched patients for comparisons of measured outcomes. The P-values of multiple comparisons between propensity score-matched treatment groups were not further adjusted to reduce the risk of type I error. Finally, the significant economic gaps and demographic differences across Chinese cities11 might affect the generalizability of our study results based on two hospitals in a provincial capital.
Conclusion
In summary, this retrospective cohort study demonstrated that the superior tumor response and better toxicity profile associated with pemetrexed–platinum doublet was also related to lower hospital costs for nonchemotherapy drugs and nondrug care, mainly for nonchemotherapy drugs, when compared with other platinum-based doublets frequently used in the first-line setting for AdvNS-NSCLC in Chinese patients. However, the saved hospital costs for nonchemotherapy drugs and nondrug care associated with pemetrexed treatment were not higher enough to completely offset the increased drug acquisition cost of pemetrexed relative to other cytotoxic agents.
Acknowledgments
The authors thank Lisa M Hess, the principal research scientist of Eli Lilly and Co, for her valuable comments and editorial support. They also thank the staff of Normin Health Changsha Representative Office for their logistics and administration support to this study. This research project was supported and monitored by an unrestricted health outcome research grant from Eli Lilly and Co, People’s Republic of China.
Disclosure
Yicheng Yang, Narayan Rajan, Yun Chen are employees of Eli Lilly and Co. Canjuan Yang and Jianfeng Li are employees of Normin Health Changsha Representative Office. Dr Wendong Chen is the founder of Normin Health and receives consulting fee and research funds from Eli Lilly and Co. The other authors report no conflicts of interest in this work.
References
Chen W, Zheng R, Zhang S, et al. The incidences and mortalities of major cancers in China, 2009. Chin J Cancer. 2013;32(3):106–112. | |
Zhao Y, Wang S, Aunan K, Seip HM, Hao J. Air pollution and lung cancer risks in China – a meta-analysis. Sci Total Environ. 2006;366(2–3):500–513. | |
Chen Y, Han S, Zheng MJ, Xue Y, Liu WC. Clinical characteristics of 274 non-small cell lung cancer patients in China. Onkologie. 2013;36(5):248–254. | |
Cha Q, Chen Y, Du Y. The trends in histological types of lung cancer during 1980–1988, Guangzhou, China. Lung Cancer. 1997;17(2–3):219–230. | |
Chen B, Wang Y, Cao H, et al. Early lung cancer detection using the self-evaluation scoring questionnaire and chest digital radiography: a 3-year follow-up study in China. J Digit Imaging. 2013;26(1):72–81. | |
Cai C, Zhou Z, Yu L, Wan Y. Predictors of the health-related quality of life of patients who are newly diagnosed with lung cancer in China. Nurs Health Sci. 2011;13(3):262–268. | |
Xue C, Hu Z, Jiang W, et al. National survey of the medical treatment status for non-small cell lung cancer (NSCLC) in China. Lung Cancer. 2012;77(2):371–375. | |
Elderly Lung Cancer Vinorelbine Italian Study (ELVIS) Group. Effects of vinorelbine on quality of life and survival of elderly patients with advanced non-small-cell lung cancer. J Natl Cancer Inst. 1999;91:66–72. | |
Liu X, Hsiao WC. The cost escalation of social health insurance plans in China: its implication for public policy. Soc Sci Med. 1995;41(8):1095–1101. | |
Scagliotti G, Brodowicz T, Shepherd FA, et al. Treatment-by-histology interaction analyses in three phase III trials show superiority of pemetrexed in nonsquamous non-small cell lung cancer. J Thorac Oncol. 2011;6(1):64–70. | |
Scagliotti GV, Parikh P, von Pawel J, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol. 2008;26(21):3543–3551. | |
Detterbeck FC, Boffa DJ, Tanoue LT. The new lung cancer staging system. Chest. 2009;136(1):260–271. | |
Zhi X, Wu Y, Ma S, et al. Chinese guidelines on the diagnosis and treatment of primary lung cancer (2011 version). Zhongguo Fei Ai Za Zhi. 2012;15(12):677–688. | |
Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–216. | |
Cheng K, Zhao F, Gao F, et al. Factors potentially associated with chemotherapy-induced anemia in patients with solid cancers. Asian Pac J Cancer Prev. 2012;13(10):5057–5061. | |
Austin PC. A comparison of 12 algorithms for matching on the propensity score. Stat Med. 2014;33(6):1057–1069. | |
D’Agostino RB. Estimating treatment effects using observational data. JAMA. 2007;297(3):314–316. | |
Hu CP, Wang Y, Chen JH, et al. Tumor response and clinical toxicity associated with second-line chemotherapy regimens for advanced non-squamous non-small cell lung cancer: a retrospective cohort study. Thorac Cancer. 2014;5(5):365–376. | |
Gridelli C, de Marinis F, Pujol JL, et al. Safety, resource use, and quality of life in paramount: a phase III study of maintenance pemetrexed versus placebo after induction pemetrexed plus cisplatin for advanced nonsquamous non-small-cell lung cancer. J Thorac Oncol. 2012;7(11):1713–1721. | |
Paessens BJ, von Schilling C, Berger K, et al. Health resource consumption and costs attributable to chemotherapy-induced toxicity in German routine hospital care in lymphoproliferative disorder and NSCLC patients. Ann Oncol. 2011;22(10):2310–2319. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.