")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Real-World Effectiveness of Insulin Glargine 300 Initiation in Switzerland
Authors Thomann R, Zechmann S , Alexander-David N, Jornayvaz FR
Received 22 May 2020
Accepted for publication 16 June 2020
Published 3 July 2020 Volume 2020:13 Pages 2359—2365
DOI https://doi.org/10.2147/DMSO.S252667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Robert Thomann,1 Stefan Zechmann,2 Nicola Alexander-David3,†, François R Jornayvaz4
1Bürgerspital Solothurn, Solothurn, Switzerland; 2Institute of Primary Care, University of Zurich, Zurich, Switzerland; 3Private Practice, Bellinzona, Switzerland; 4Hôpitaux Universitaires de Genève, Geneva, Switzerland
†Nicola Alexander-David passed away on March 02, 2020
Correspondence: François R Jornayvaz
Hôpitaux Universitaires de Genève, Rue Gabrielle-Perret-Gentil 4, Geneva 1205, Switzerland
Email [email protected]
Introduction: Insulin glargine 300 U/mL (Gla-300; Toujeo®) is a second-generation once-daily basal insulin. Previous randomized controlled trials showed comparable HbA1c reductions with lower rates of hypoglycemia of Gla-300 versus Gla-100.
Patients and Methods: We report the 12 months results of the Swiss cohort of Toujeo-1, a prospective, observational multicenter study exploring the real-world effectiveness of Gla-300 in adult patients with type 2 diabetes (T2D) uncontrolled (HbA1c 7.5– 10%) on oral therapy and compared these to the overall Toujeo-1 cohort (conducted in Switzerland and Germany). Primary endpoint was the percentage of patients achieving individual HbA1c targets. Secondary endpoints included changes in HbA1c, fasting plasma glucose (FPG), body weight, insulin dose, incidence of hypoglycemia and overall safety.
Results: The analysis included 47 patients (14 women) with a mean age of 64.1 years and a diabetes duration of 8.4 years. Swiss physicians determined a higher HbA1c treatment target (7.4 vs. 7.0%) and patients received higher Gla-300 doses at baseline (20.2 vs. 14.7 units/day) and the 12-month follow-up (31.0 vs. 26.2 units/kg) than in the total cohort (n=721). After 12 months, the addition of Gla-300 reduced HbA1c by 1.5% (p< 0.0001) to an HbA1c of 7.2%, and FPG by 3.3 mmol/L (p< 0.0001) to an FPG of 7.1 mmol/L. At 12 months, 70.2% achieved their individual HbA1c target, more than in the overall Toujeo-1 cohort (49.9%). Body weight remained stable throughout. Only episodes of symptomatic, non-severe hypoglycemic events were documented (2.1%) with similar rates as for the overall Toujeo-1 population.
Conclusion: In patients with T2D on oral therapy and newly treated with basal insulin, Gla-300 improves glycemic control with a low risk of hypoglycemia and no increase of body weight. The results for Switzerland are consistent with those reported for the overall Toujeo-1 cohort and reveal that treatment targets and approaches slightly differ between both countries.
Keywords: insulin glargine 300 U/mL, type 2 diabetes, real-world, Switzerland
Introduction
Treatment target achievement remains a concern in patients with type 2 diabetes (T2D). A study assessing adherence to the Swiss national targets for good disease management in diabetes, demonstrated, for Switzerland, that even with an overall high standard of diabetes care, there is still room for improvement.1 Over 60% of the patients with T2D diagnosed at least 5 years ago did not achieve an HbA1c target below 7%.
Insulin glargine 300 U/mL (Gla-300, Toujeo®, Sanofi-aventis) is a second-generation basal insulin analog. A meta-analysis of the EDITION clinical development program showed a comparable efficacy in terms of the HbA1c reduction with Gla-100, but with a reduced risk of hypoglycemia.2 In EDITION 3, Gla-300 demonstrated, over a 6-month and a 12-month, a comparable efficacy to Gla-100 in terms of HbA1c reduction, with a lower risk of hypoglycemia, in T2D patients uncontrolled on oral antidiabetics (OADs).3
For the evaluation of the efficacy and safety, randomized controlled trials (RCT) are pivotal for regulatory bodies in the drug approval process. Nonetheless, the intensive monitoring and education provided during the RCTs are not always representative of daily clinical practice.4 Thus, non-interventional, observational studies representative of a “real-world” setting are important to validate the results from clinical trials.5,6
Toujeo-1 is a 12-month prospective real-world study to investigate the effectiveness and safety of Gla-300 in patients with T2D who were uncontrolled on oral antidiabetic drugs (OADs) ± Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 RA). Data for the pooled patients from Germany and Switzerland have been published recently,7 but data specific for Switzerland are lacking. It was therefore the purpose of the present analysis to provide Switzerland specific data and to put these data into perspective with the ones in the overall Toujeo-1 dataset.
Patients and Methods
The Toujeo-1 explored the real-world effectiveness of Gla-300 in adult patients with T2D uncontrolled on their previous OAD therapy with or without a Glucagon-Like Peptide1 Receptor Agonist (GLP-1 RA).7 Investigators were general practitioners and specialists in internal medicine, endocrinology/diabetology. The Swiss cohort started Gla-300 treatment between November 2015 and December 2016 in 21 participating centers. The study was approved by an independent local ethics committee. All procedures carried out were in line with the ethical standards of the responsible committees on human experimentation and with the Declaration of Helsinki. It was registered at the ISRCTN registry (ISRCTN12809144, www.ISRCTN.org).
Study Population
Patients with T2D were included if their HbA1c was ≥7.5% and ≤10.0%, their age was ≥18 years, and after their treating physician had decided to initiate a basal insulin supported oral therapy with Gla-300, independent from study participation. The observation plan did neither give any recommendation on what Gla-300 dose to use nor did it provide any titration algorithm. Physicians were asked to document a patient-individual HbA1c target to be able to determine a target achievement rate. Patients needed to be able to self-measure blood glucose levels. They were not included if they had type 1 diabetes, any pre-existing insulin regimen, if Gla-300 was not indicated, or if the patient was pregnant, had cancer, or a history of alcohol- or drug abuse. All patients provided written informed consent.
Outcome Measures
The primary endpoint of the analysis was the percentage of patients achieving their individually pre-defined HbA1c target value after 6 and 12 months, respectively. Secondary endpoints included changes in HbA1c, fasting plasma glucose (FPG), body weight and insulin dose, as well as hypoglycemia incidence and overall safety.
Statistical Analyses
Data were collected using an electronic case report form (eCRF). The observation plan comprised a documentation at baseline, 6 months, and 12 months after the initiation of Gla-300. Baseline characteristics and demographics were reported as mean ± SD or percentage, as appropriate, and were based on the full analysis set 2 (FAS2), including all patients with written informed consent, with at least one documented dose of Gla-300 at any time, an initiation of Gla-300 not more than 2 weeks before the first documentation, with HbA1c at baseline not above 10%, and all other inclusion/exclusion criteria fulfilled. Descriptive statistics of continuous variables were compared using a two-tailed paired t-test.
Results
Study Population Demographics and Clinical Characteristics
A total of 47 patients (14 women) completed all three major documentations including the 12 months follow-up. Mean age was 64.1 years (Table 1), mean BMI 31.8 kg/m2, and the majority of patients had long-standing T2D (mean 8.4 years). The mean HbA1c at baseline was 8.7% and patients had an assigned mean individual treatment target of 7.4%. Noteworthy differences between the Swiss and the overall cohort were a lower proportion of female patients (29.8% vs. 42.4%) and a more lenient HbA1c target (7.4% vs. 7.0%).
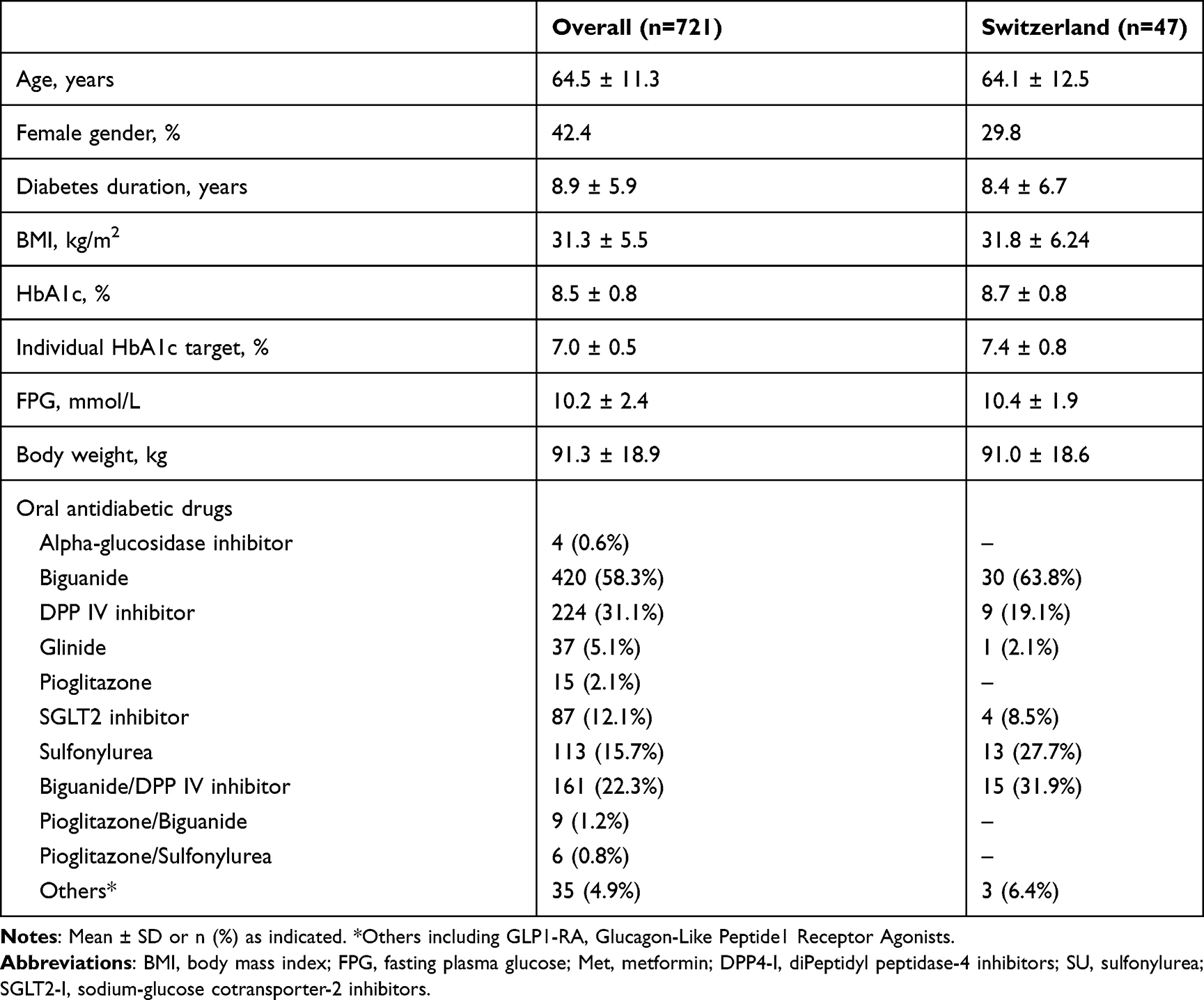 |
Table 1 Study Population (mFAS12) |
Treatment Characteristics
The majority of patients received metformin (45 patients, 95.7%), 24 patients (51.1%) a DPP-4 inhibitor, 13 patients (30%) a sulfonylurea and 4 patients (8.5%) a SGLT-2 inhibitor. Sulfonylurea therapy was discontinued in 4 patients; other non-insulin anti-hyperglycemic treatment remained stable throughout the study. Patients were initiated on a mean dose of 20.2 units per day (Table 2) which increased by the time of the 6 months visit (30.6 units/day; p<0.0001 vs. baseline) and remained stable thereafter (31.0; p<0.0001 vs. baseline). Body weight was not altered after Gla-300 treatment, with a statistically non-significant weight loss of 1.2 kg after 12 months.
 |
Table 2 Gla-300 Titration (mFAS12) |
Patients in Switzerland received more sulfonylurea (27.7% vs. 15.7%) and biguanides (metformin) either alone (63.8% vs. 58.3%) or in combination with DPP-4 inhibitors (31.9% vs. 22.3%). DPP-4 inhibitor use alone was lower in Switzerland (19.1% vs. 31.1%). They also received more Gla-300 at baseline (20.2 units/day) than patients in the overall Toujeo-1 study (14.7 units/day) and units were still higher at the 12 months follow-up visit (31.0 vs. 26.2 units/day). The loss of body weight was slightly higher in Switzerland (−1.2 kg) compared to the overall Toujeo-1 population (−0.3 kg).
Real-World Effectiveness Outcomes
Six months after initiating basal insulin Gla-300, mean HbA1c significantly decreased from 8.7% at baseline to 7.5% (p<0.0001) at the 6 months follow-up, and further to 7.2% (p<0.0001) after 12 months (Table 3). Regarding the primary end-point, 25 (53.2%) patients at 6 months and 33 (70.2%) patients at 12 months reached their individually pre-defined HbA1c target value (p<0.0001) (Table 4). Patients in Switzerland had substantially higher target achievement rates at 6 months (53.2% vs. 33.4%) and 12 months (70.2% vs. 49.9%) but at more lenient individual targets (7.4% vs. 7.0%).
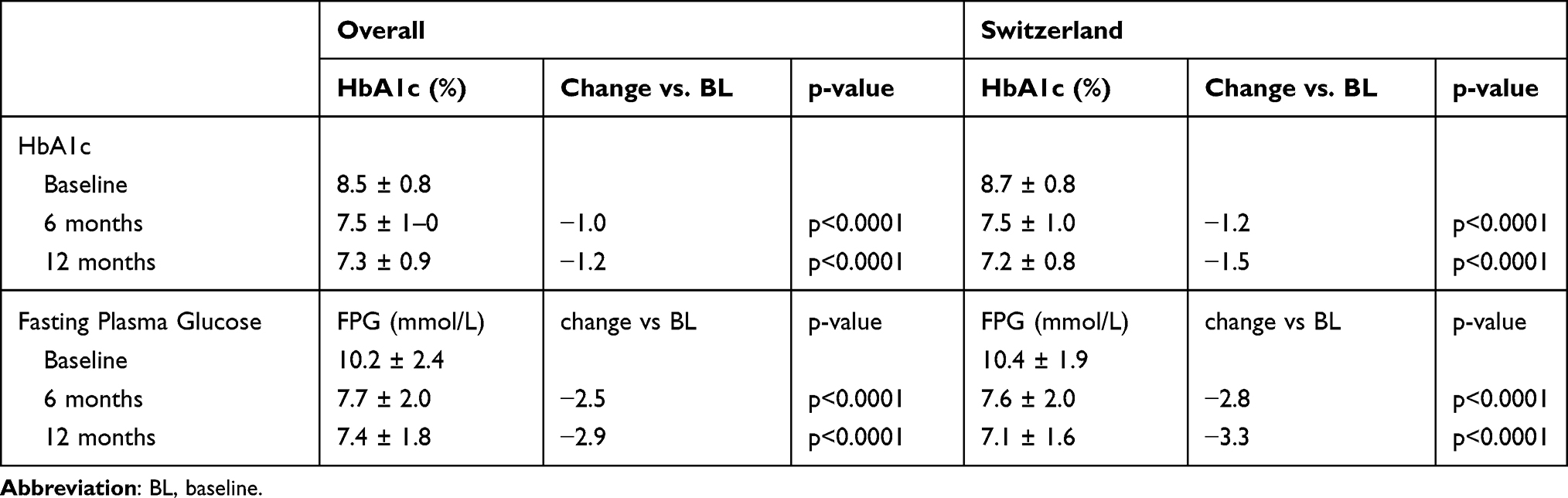 |
Table 3 Change in HbA1c and Fasting Blood Glucose Over Time (mFAS12) |
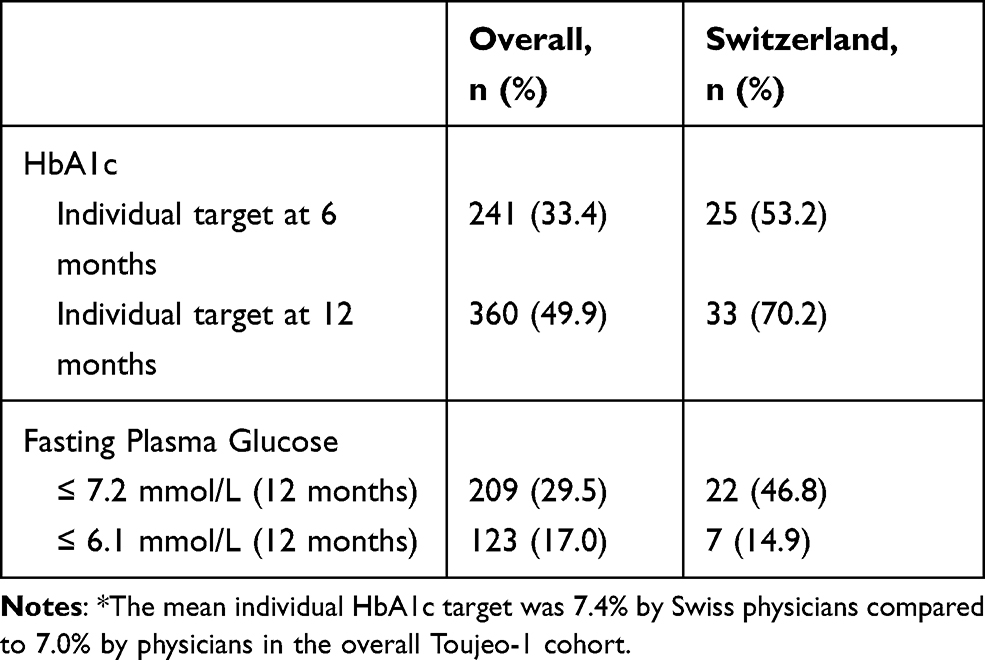 |
Table 4 HbA1c* and Fasting Blood Glucose Achievement (mFAS12) |
Mean FPG levels were reduced from 10.4 mmol/L at baseline to 7.1 mmol/L at 12 months (p<0.0001), corresponding to an FPG change of −3.3 mmol/L (Table 3). After 12 months, 14.9% of the patients reached an FPG ≤ 6.1mmol/L and 46.8% an FPG ≤ 7.2 mmol/L (Table 4). Patients in Switzerland had higher target achievement rates at 12 months compared to the overall cohort (46.8% vs. 29.5%).
Hypoglycemia
During follow-up, the hypoglycemia incidence with Gla-300 was very low (Table 5). After 12 months Gla-300 treatment, one patient (2.1%) had at least one episode of symptomatic hypoglycemia. No patient with severe hypoglycemia was reported. This corresponds to a rate for symptomatic and severe hypoglycemia of 0.02 events per patient-year. Hypoglycemia rates were similar for Switzerland and the overall Toujeo-1 cohort where no severe hypoglycemia was observed and rates of symptomatic or confirmed symptomatic hypoglycemia were in the same order.
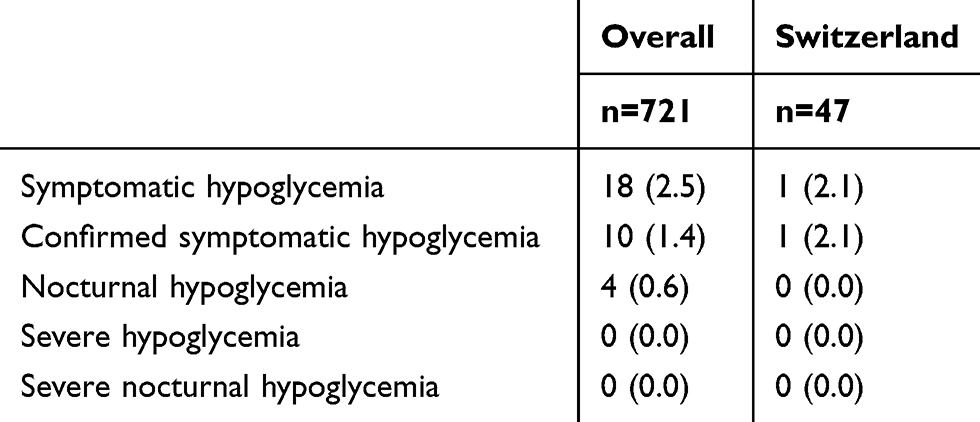 |
Table 5 Hypoglycemia (mFAS12) |
Discussion
Toujeo-1 is the first prospective non-interventional real-world study using Gla-300 in insulin naïve T2D patients in Switzerland. The study demonstrated improved glycemic control with the use of Gla-300 during a 12 months follow-up, with a very low incidence of hypoglycemia and without a significant effect on body weight. Compared with the overall Toujeo-1 study population of which the vast majority was included in Germany, the more lenient mean individual treatment target in Switzerland (7.4% vs. 7.0%), the higher Gla-300 doses applied at baseline (20.2 vs. 14.7 units/day) and throughout the follow-up (31.0 vs. 26.2 units/day), the higher rates of HbA1c (12 months: 70.2% vs. 49.9%) and FPG ≤ 6.1 mmol/L (12 months: 46.8% vs. 29.5%) treatment target achievement were the most noteworthy.
Previous studies reported results of newly initiating Gla-300 in insulin naïve patients with T2D, either in RCTs like EDITION 3,3 BRIGHT,8 or in a retrospective setting like DELIVER-Naïve D that used propensity score matching.9 Toujeo-1 confirms the effectiveness of Gla-300 in a real-world setting with an HbA1c decrease of −1.2% and −1.5% at 6 and 12 months, respectively, similar to the reductions already published. Contrary to what is usually defined as HbA1c target in the RCTs (<7%) and recommended by the American Diabetes Association (ADA, <7%) or American Association of Clinical Endocrinologists (AACE, ≤6.5%), as well as the treatment target defined in the overall Toujeo-1 study7 with <7.0%, the mean individual HbA1c target pursued by the Swiss physicians for their patients was 7.4%. While this HbA1c value is substantially higher than in the aforementioned recommendations and the overall Toujeo-1 study, it is more in line with the recommendation of individualization of the target and with the aim set by the American College of Physicians (ACP, 7% < HbA1c < 8%).
A majority of patients (70.2%) reached their individual HbA1c target after 12 months of Gla-300. The results of the TOP-II study, a similar real-world prospective non-interventional study in Swiss uncontrolled patients with T2D switched from their previous basal insulin to Gla-300, showed that 57% of these patients reached their individual HbA1c target.10 Even if a direct comparison cannot be made, our results are coherent with those of the recently published analysis of a Swiss cohort of patients with T2D (Swiss Diab) that revealed that only 44% of the patients reached the HbA1c target <7% but 77% of the patients reached the HbA1c target <8%.1 This may also point at a reason for the discrepant treatment target achievement between the Swiss and the overall cohort in Toujeo-1. Individual treatment targets were higher (7.4%) than in the overall cohort (7.0%), while at the same time, higher doses of insulin glargine were used.
Furthermore, it is well known that initiating and titrating basal insulin is challenging in patients with T2D, explaining a certain level of clinical inertia. After the initiation of insulin therapy, adequately increasing the insulin dose is key to obtain a good glycemic control. In Toujeo-1, patients started Gla-300 with a mean dose of 20.2 units/day, corresponding to a slightly lower dose than the recommended dose. At 6 months, the mean dose increased from 20.2 U/d to 30.6 U/d and remained stable over the next 6 months (31.0 U/d). At 12 months, the mean daily dose in our real-world setting study was lower than that observed in the RCTs EDITION 3 or BRIGHT, in which patient`s insulin dose increased throughout 6 months. It was higher, though, than in the total Toujeo-1 population, indicating that doses used in Germany are obviously lower. These observations need to be considered on the background that, as Toujeo-1 was a non-interventional study, no mandatory FPG target, nor titration scheme or frequency of titration were given. However, Toujeo-1 could demonstrate a real benefit in terms of glycemic control in uncontrolled patients with T2D newly treated with low doses of Gla-300 in a real-world clinical setting.
Among the different barriers to insulin therapy and its titration, fear of hypoglycemia is one of the major concerns, mentioned by both physicians and patients. Among the 47 patients, only 1 patient had an episode of symptomatic hypoglycemia. This is a very low hypoglycemia incidence compared to the 10% reported in the retrospective analysis DELIVER-Naïve D.9 In addition, this incidence in the real-world setting is much lower than the 46% or 66% of patients reporting ≥1 confirmed (≤3.9 mmol/L) or severe hypoglycemia at any time of day in the RCTs EDITION 3 and BRIGHT, respectively. The low incidence rate of hypoglycemia in this study may be explained by the relatively low insulin dose, the less tight HbA1c and FPG targets, and/or the under-reporting of events. Over the 12 months follow-up, 4 patients stopped sulfonylurea treatment, which could lead to a lower hypoglycemia risk as well. Nevertheless, the significant improvement in glycemic control obtained with Gla-300 at a very low risk of hypoglycemia confirms the equilibrium between effectiveness and safety for Gla-300 in a real-world setting.
Contrary to the RCTs, where small weight gains were observed, the mean body weight decreased by 1.2 kg in Toujeo-1 Swiss cohort (no statistically significant) over the 12 months of Gla-300 therapy. Even though data are blunted in the overall Toujeo-1 cohort (−0.3 kg), this result obtained in real-world setting gives a positive signal, as fear of weight gain can be a barrier for initiating basal insulin in patients with T2D.
The strengths of Toujeo-1 are the prospective multicenter design with observational monitoring and follow-up that can be considered representative of primary care in Switzerland. A limitation of the sub-analysis of the Swiss cohort of Toujeo-1 is the relatively small number of patients observed over 12 months (n=47). Starting the study just after the market authorization in Switzerland allowed to collect data on the first Gla-300 users in a real-world setting, but could also represent a challenge as the recruited patients would likely have been the most difficult to achieve good glycemic control. Furthermore, the patient’s care may have been influenced (i.e. be more stringent) because of study participation and the fact that Gla-300 was newly on the market. In EDITION 3 and in BRIGHT, the greatest effect on efficacy, measured either as HbA1c reduction or as FPG reduction, was observed in the first 12 weeks. In our trial, at 6 months, the efficacy was comparable to that reported in the RCTs. However, due to the non-interventional nature of the study, we have no information regarding the speed of insulin up-titration. The mean dose achieved at 6 months remained stable over the next 6 months until the end of the follow-up.
Conclusion
In patients with T2D newly treated with basal insulin, Gla-300 improves glycemic control with a low risk of hypoglycemia and no increase of body weight. The results for Switzerland are consistent with those reported for the overall Toujeo-1 cohort which also included patients from Germany and reveal that treatment targets and approaches slightly differ between both countries.
Compliance with Ethics Guidelines
This study was approved by the Commission cantonale d`éthique de la recherché sur l`être (CER-VD; protocol number 464/15). This study conformed with the Helsinki Declaration of 1964, as revised in 2013, concerning human rights. All study participants provided informed consent.
Editorial Assistance
Editorial assistance in the preparation of this article was provided by Sanofi-aventis (suisse) sa.
Acknowledgments
The authors wish to thank the study participants for their involvement in the study.
In memory of Dr. Nicola Alexander-David, who was an investigator in this study and died during the preparation of the manuscript.
Author Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
François R Jornayvaz has received honoraria for consultancy from Sanofi, Eli Lilly, Boehringer Ingelheim and Novo Nordisk. The authors report no other conflicts of interest in this work.
References
1. Schimke KE, Renstrom F, Meier S, Stettler C, Brandle M, SwissDiab Study G. Compliance with guidelines for disease management in diabetes: results from the SwissDiab registry. BMJ Open Diabetes Res Care. 2018;6:e000454. doi:10.1136/bmjdrc-2017-000454
2. Ritzel R, Roussel R, Giaccari A, Vora J, Brulle-Wohlhueter C, Yki-Jarvinen H. Better glycaemic control and less hypoglycaemia with insulin glargine 300 U/mL vs glargine 100 U/mL: 1-year patient-level meta-analysis of the EDITION clinical studies in people with type 2 diabetes. Diabetes Obes Metab. 2018;20(3):541–548. doi:10.1111/dom.13105
3. Bolli GB, Riddle MC, Bergenstal RM, et al. New insulin glargine 300 U/mL compared with glargine 100 U/mL in insulin-naive people with type 2 diabetes on oral glucose-lowering drugs: a randomized controlled trial (EDITION 3). Diabetes Obes Metab. 2015;17:386–394. doi:10.1111/dom.12438
4. Edelman SV, Polonsky WH. Type 2 diabetes in the real world: the elusive nature of glycemic control. Diabetes Care. 2017;40(11):1425–1432. doi:10.2337/dc16-1974
5. Sherman RE, Anderson SA, Dal Pan GJ, et al. Real-world evidence — what is it and what can it tell us? N Engl J Med. 2016;375(23):2293–2297. doi:10.1056/NEJMsb1609216
6. Zhou FL, Ye F, Berhanu P, et al. Real-world evidence concerning clinical and economic outcomes of switching to insulin glargine 300 units/mL vs other basal insulins in patients with type 2 diabetes using basal insulin. Diabetes Obes Metab. 2018;20(5):1293–1297. doi:10.1111/dom.13199
7. Pfohl M, Jornayvaz FR, Fritsche A, et al. Effectiveness and safety of insulin glargine 300 U/mL in insulin-naive patients with type 2 diabetes after failure of oral therapy in a real-world setting. Diabetes Obes Metab. 2020;22(5):759–766. doi:10.1111/dom.13952
8. Rosenstock J, Cheng A, Ritzel R, et al. More similarities than differences testing insulin glargine 300 units/mL versus insulin degludec 100 units/mL in Insulin-naive type 2 diabetes: the randomized head-to-head BRIGHT trial. Diabetes Care. 2018;41(10):2147–2154. doi:10.2337/dc18-0559
9. Sullivan SD, Nicholls CJ, Gupta RA, et al. Comparable glycaemic control and hypoglycaemia in adults with type 2 diabetes after initiating insulin glargine 300 units/mL or insulin degludec: the DELIVER Naïve D real-world study. Diabetes Obes Metab. 2019;21(9):2123–2132. doi:10.1111/dom.13793
10. Wiesli P, Schories M. Improved glycemic control with insulin glargine 300 U/mL (Toujeo®) in patients with type 2 diabetes: real-world effectiveness in Switzerland. Diabetes Ther. 2018;9(6):2325–2334. doi:10.1007/s13300-018-0518-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.