")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Real-World Cost of Nasal Polyps Surgery and Risk of Major Complications in the United States: A Descriptive Retrospective Database Analysis
Authors Ge W, Wang D, Chuang CC, Li Y, Rout R, Siddiqui S , Kamat S
Received 5 July 2022
Accepted for publication 20 October 2022
Published 7 November 2022 Volume 2022:14 Pages 691—697
DOI https://doi.org/10.2147/CEOR.S380411
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Dean Smith
Wenzhen Ge,1 Degang Wang,1 Chien-Chia Chuang,2 Yongtao Li,3 Raj Rout,4 Shahid Siddiqui,1 Siddhesh Kamat1
1Health Economics and Outcomes Research, Medical Affairs, Regeneron, Tarrytown, NY, USA; 2Global Health Economics and Value Assessment, Sanofi, Cambridge, MA, USA; 3Global Medical Affairs, Sanofi, Bridgewater, NJ, USA; 4Global Medical Affairs, Sanofi, Reading, UK
Correspondence: Siddhesh Kamat, Email [email protected]
Background: Endoscopic nasal polyp (NP) surgery is a treatment option for patients with chronic rhinosinusitis with nasal polyps (CRSwNP). Previous studies report NP surgery costs of $8000– 13,000 and risk of major complications of NP surgery of ~0.1– 1%. Limited contemporary data for costs and complications associated with NP surgery in US clinical practice are available.
Methods: IQVIA PharMetrics Plus claims data were used to identify patients with NP surgery in 2019 with ≥ 3 years continuous baseline health-plan enrollment prior to index date (date of first eligible NP surgery) and ≥ 30 days continuous enrollment after index (follow-up). In this descriptive analysis, total costs of NP surgery were estimated as all medical costs on the index date (or during the entire hospital stay for patients who received surgery in the inpatient setting). Total medical costs (all-cause) were estimated for all medical services occurring from the index date to the index date +9 or +29 days (10-day and 30-day). Major complication was defined as cerebrospinal fluid (CSF) leak, orbital injury, or major hemorrhage within 30 days of index.
Results: Of 6311 patients, median age was 46 years (interquartile range: 34– 56); 59.7% were male; 88.2% had no NP surgery in the prior 3 years; 63.7% had allergic rhinitis, and 37.1% had asthma. Mean (SD) total medical cost of surgery was $14,697 (11,679) and mean (SD) 10-day total medical cost was $15,401 (11,968). Major complications occurred in 102 (1.7%) patients. Total medical costs and 10-day costs were higher in patients with major complications than those without ($23,605 [19,264] vs $15,251 [11,741]).
Conclusion: In this descriptive analysis, NP surgery costs and rates of major surgical complications were updated using recent real-world data in the US. Results indicated that NP surgery complication rates were numerically higher than previously reported.
Keywords: chronic rhinosinusitis with nasal polyps, nasal polyp surgery, real-world, complications, costs
Corrigendum for this paper has been published.
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is predominantly driven by type 2 inflammation, and is characterized by symptoms of nasal congestion and/or obstruction, nasal discharge, facial pain and/or pressure, and decreased sense of smell.1 In addition to intranasal corticosteroids, treatment for severe CRSwNP has historically included systemic corticosteroids (SCS); however, a substantial proportion of patients become refractory to SCS therapy.2,3 Non-pharmacological treatment options such as endoscopic nasal polyp (NP) surgery may be performed to alleviate symptoms in patients with more severe CRSwNP, when medical therapy fails to achieve appropriate symptom control.4,5 However, in some patients polyp recurrence rates may be as high as 40%,6 and surgery may not adequately reverse loss of smell.7,8
Previous cost estimates for NP surgery in the US have ranged from approximately $8000–$13,000.9–13 However, because they were derived using data from no later than 2016, these estimates may not reflect current practice patterns. Previous studies in the UK, Japan and Taiwan have reported that a minority of patients (approximately 0.5%) who received NP surgery experienced major complications including cerebrospinal fluid (CSF) leak, orbital injury, or major hemorrhage;14–16 such complications result in additional treatment costs. Another previous study in the US using claims data from patients who received endoscopic sinus surgery reported a major complication rate of 1% (CSF leak, 0.17%; orbital injury, 0.07%; hemorrhage requiring transfusion, 0.76%); however, the study period was 2003–2007 and therefore may not reflect current clinical practice.17
Currently, cost estimates of NP surgeries in the literature were variable and limited data exist on the complication rates following NP surgery in routine clinical care in the US. Real-world evidence on complications and associated costs are essential inputs for the clinical and economic evaluation of treatment options. To address this data gap, this retrospective, real-world descriptive analysis evaluated the risk of major complications and total medical costs related to NP surgery (with or without complications) using data from a large US commercial insurance database.
Methods
Study Design and Data Source
This was a retrospective cohort study using claims data from a nationally representative commercial insurance database (IQVIA PharMetrics Plus), with over 190 million US enrollees since 2006, and over 30 million patients with ≥3 years continuous enrollment. Patients with claims for NP surgery (identified by current procedural terminology [CPT] codes: see Table S1 for an overview of included procedures) between January 1, 2019 and December 31, 2019 were included (Figure 1); date of the first eligible NP surgery was the index date. An eligible surgery was defined as one in those patients who had ≥3 years continuous enrollment prior to the index date (baseline), during which they had ≥1 diagnosis of NP as indicated by International Classification of Diseases, Ninth and Tenth Revisions, Clinical Modification (ICD-9-CM and ICD-10-CM) codes (Table S1) and had ≥30 days continuous enrollment after the index date (follow-up), and were insured by commercial plans on index date. Patients who had NP surgery codes in the 12 weeks preceding index were excluded, to ensure that the index CPT indicated a new NP surgery, rather than follow-up care or procedures. IQVIA PharMetrics Plus data are anonymized and are in compliance with Health Insurance Portability and Accountability Act requirements. As such, research using this dataset does not constitute human subject research, and therefore no institutional review board approval was sought.
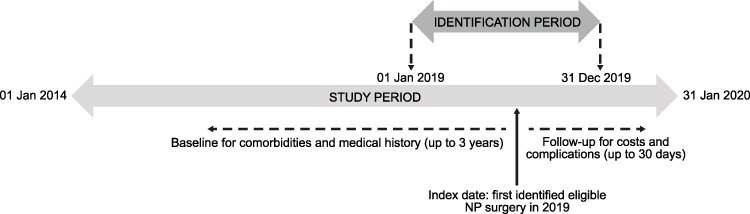 |
Figure 1 Study design. |
Demographic and Clinical Characteristics
Age, sex, and baseline comorbidities were identified at index. Baseline comorbidities including asthma, atopic dermatitis (AD), allergic rhinitis, cardiovascular disease (CVD), diabetes, and chronic kidney disease (CKD) were defined as having ≥1 ICD-10-CM code of the corresponding disease (at any time in the record). Characteristics of the index surgery, including inpatient or outpatient (outpatient defined as day case surgery) and type of surgery (first/repeat surgery) were identified. If the patient had no NP surgery during the 3-year baseline, the index surgery was defined as first surgery; if a patient had ≥1 NP surgery during baseline, the index surgery was defined as repeat surgery. Patients were stratified by the setting of the index surgery, ie, inpatient or outpatient.
Outcome Measures
Total surgery costs were calculated as costs occurring on the index date or throughout the entire stay for patients who received surgery in the inpatient setting. Total medical costs (10-day and 30-day) were calculated as paid amounts of all services occurring within 10 or 30 days of the index date, respectively. Costs were inflation-adjusted to 2021 US dollars ($). Since the focus of this study was medical costs, pharmacy costs were not included in this analysis. Major complication was defined as experiencing at least one of following events within 30 days of the index date, without such an event during the 30 days prior to the index date (see Supplementary Table S1 for specific diagnosis or procedure codes used): CSF leak, orbital injury, and major hemorrhage requiring inpatient/emergency department (ED) visit or transfusion.
Statistical Analysis
All analyses were descriptive, and no formal statistical testing was performed. Baseline characteristics were described for all patients as well as by first/repeat surgery. Risk of major complication was calculated. Total surgery costs and total medical (all-cause) costs (10-day) were reported for all patients as well as by first/repeat surgery. Total surgery costs and total medical (all-cause) costs (10-day and 30-day) were also reported separately for patients with and without major complications. Continuous variables were reported as mean (SD) or median (interquartile range [IQR]), and categorical variables were reported as count (%).
Results
A total of 6311 eligible patients were included in the data analysis (see Figure 2 for patient attrition).
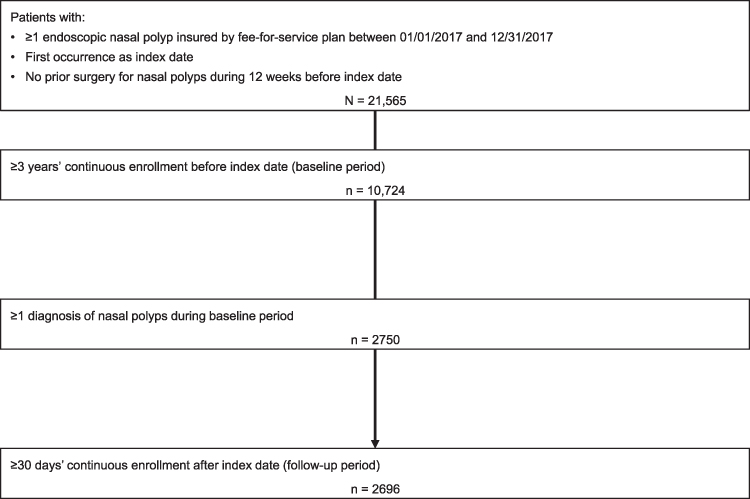 |
Figure 2 Patient selection. |
Demographic and Clinical Characteristics
The median (IQR) age was 46 (34–56) years, and 59.7% of patients were male (Table 1). More than 90% of index surgeries occurred in the outpatient setting. Baseline allergic rhinitis and asthma were common and affected 63.7% and 37.1% of patients, respectively. Diabetes, cardiovascular diseases, and chronic kidney disease were identified in 10.1%, 6.9%, and 2.0% of patients at baseline, respectively. The majority of patients (88.2%) had no record of NP surgery in the 3 years prior to index; patients who had a record of prior NP surgery generally reported allergic rhinitis (78.7% vs 61.7%) and asthma (52.3% vs 35.1%) more frequently than patients with no prior surgery (Table 1).
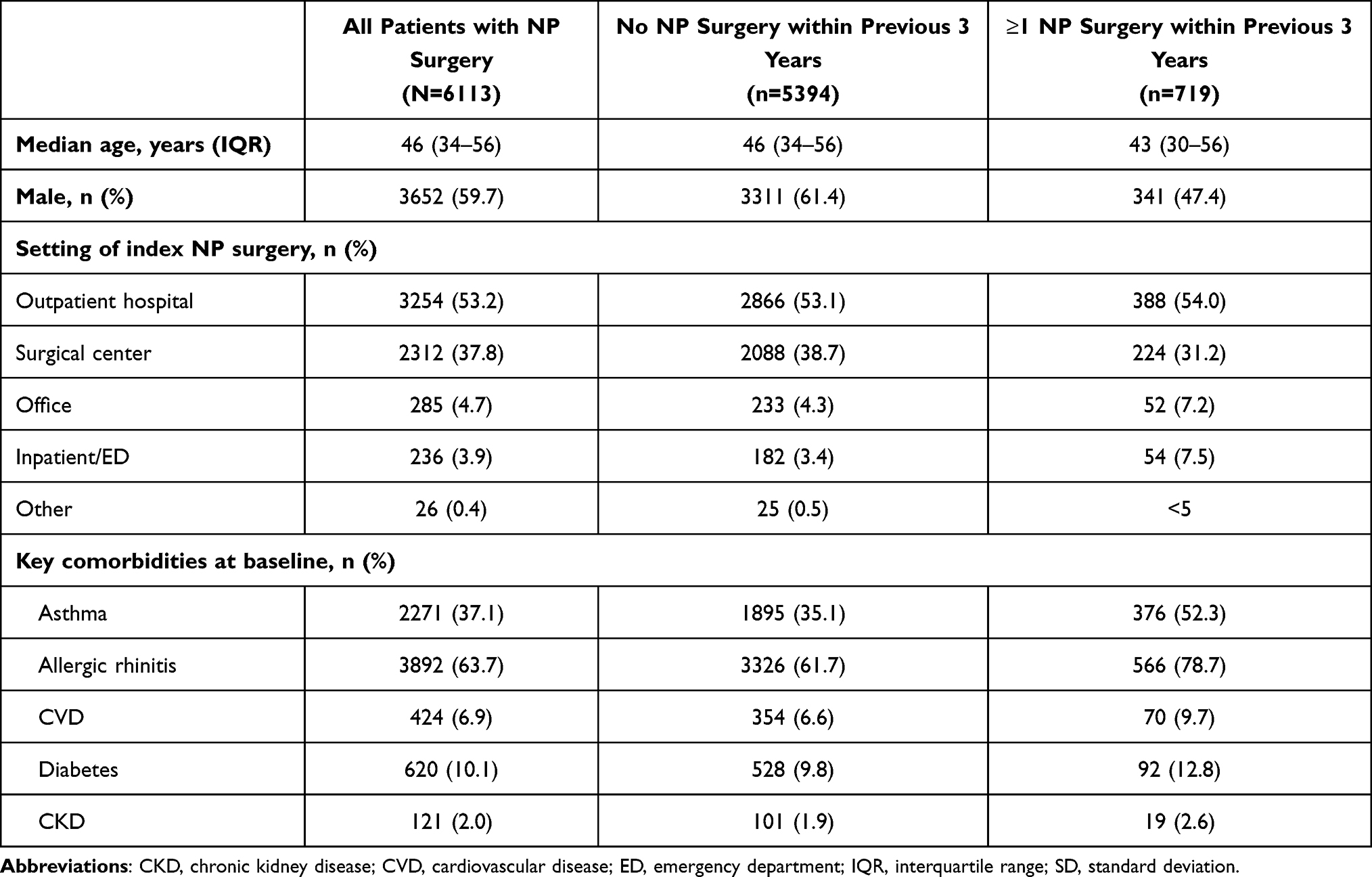 |
Table 1 Demographic and Clinical Characteristics of Patients with NP Surgery |
Costs and Outcomes
The mean (SD) total NP surgery cost was $14,697 (11,679), and was comparable for first and repeat surgeries (Table 2). The mean (SD) respective costs of NP surgery for patients who received surgery in the outpatient and inpatient settings were $14,418 (10,581) and $35,740 (39,370). The mean (SD) total medical 10-day costs were $15,401 (11,968) overall and were $15,174 (10,998) for first surgery and $15,511 (16,767) for repeat surgery. Major complications occurred in 102 (1.7%) patients during the 30 days after index NP surgery: 71 patients had major hemorrhage, 19 had orbital injuries, and 13 had CSF leak (one patient had both orbital injury and CSF leak). Of these, 88/5394 (1.6%) patients experienced major complications with their first surgery and 14/719 (2.0%) with repeat surgery; rates of major hemorrhage, CSF leak, and orbital injuries were similar with first and multiple surgeries. Half of the complications occurred within 4 days of index date (median [Q1–Q3] time to major complication: 3.5 [0–8] days). Total medical costs were higher in patients who experienced major complications compared with those who did not (within 10 days: $23,605 [19,264] vs $15,251 [11,741]; within 30 days: $27,406 [23,064] vs $16,186 [12,325]; Table 3), even after considering differences in surgery costs between the two groups ($19,762 [15,125] in patients who experienced major complications compared with $14,604 [11,587] in those who did not).
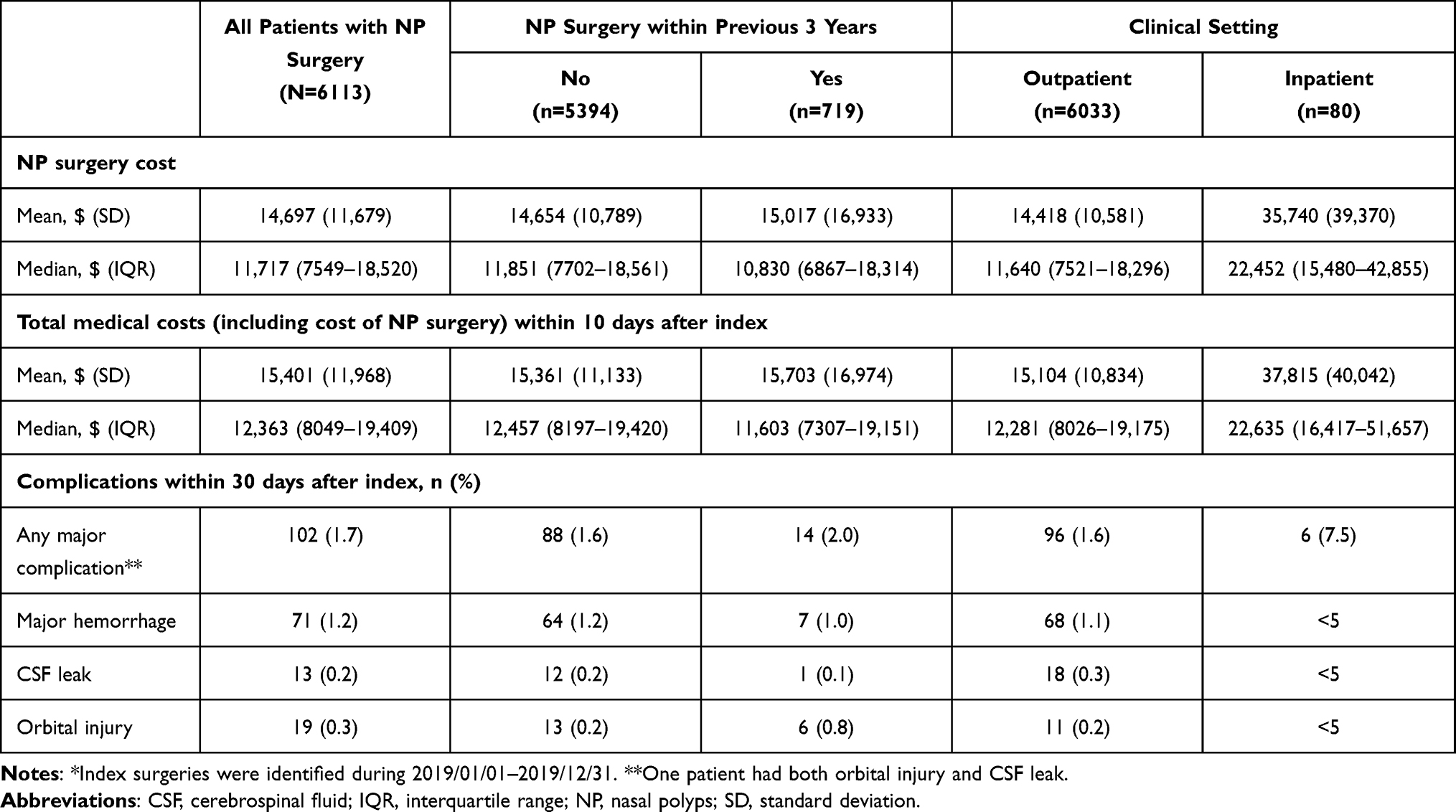 |
Table 2 Costs and Rate of Major Complications After Index NP Surgery* |
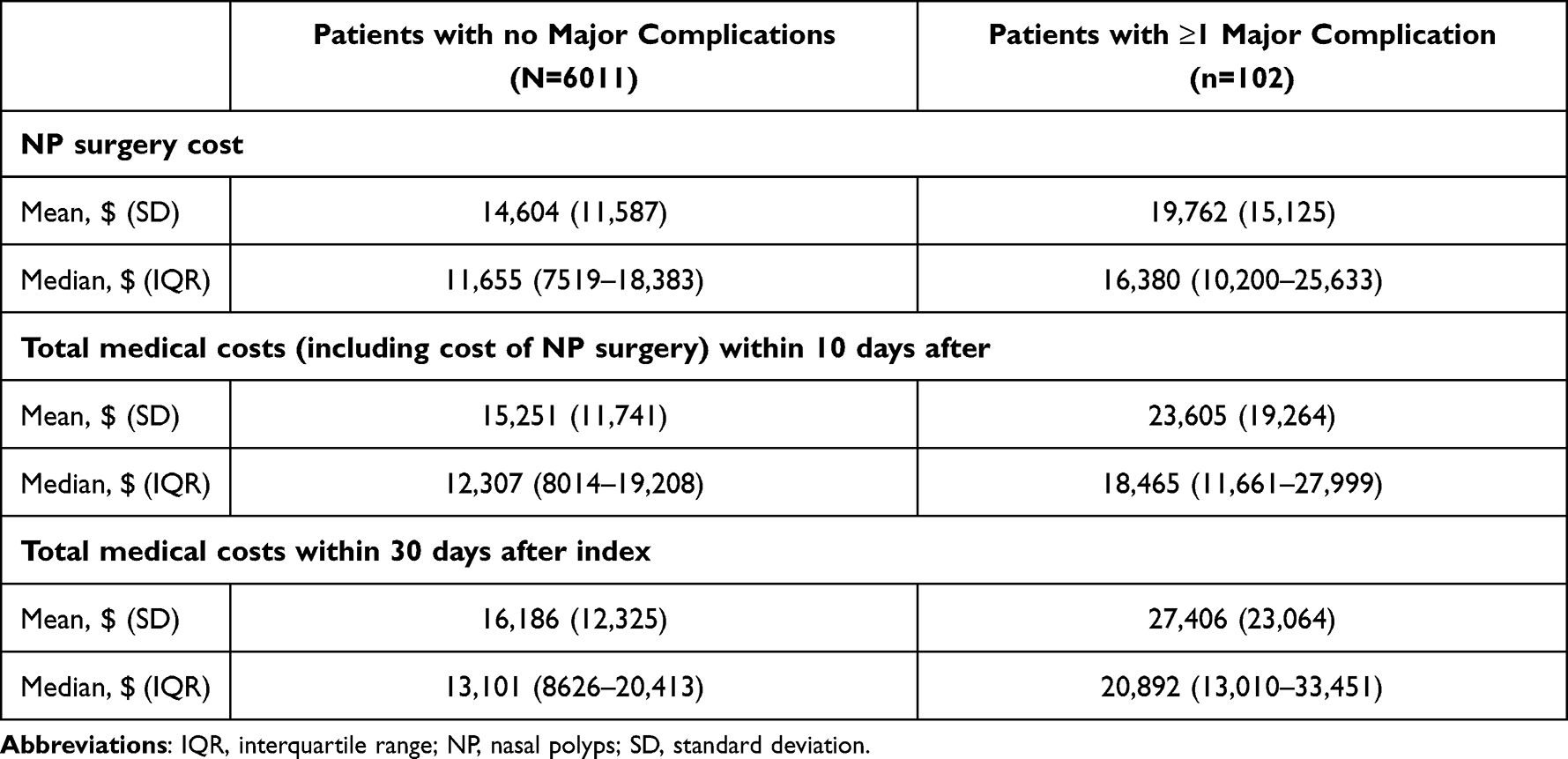 |
Table 3 Costs After Index NP Surgery in Patients with and without Major Complications |
Discussion
This large, real-world claims analysis of patients with CRSwNP who received NP surgery observed higher costs and major post-surgical complication rates than previously reported.9,10,18 One systematic review reported that the mean total cost related to NP surgery ranged from $8200–$10,500,9 and a more recent US claims-based analysis estimated that the total medical cost on the day of the NP surgery procedure was approximately $10,500.10 Another study reported mean disease-related and prescription expenditure within 1 year of NP surgery of $11,166,11 while median (IQR) costs for all NP surgeries were $13,264 (8032–21,897) using the State Ambulatory Surgery Databases for California, Florida, Maryland, and New York (mean costs were not reported).12 In the current study, the cost of NP surgery was defined as all costs that occurred on the index date for outpatient surgery and all costs that occurred during the entire stay for inpatient surgery, with the latter including charges that might not be directly related the NP surgery. However, the NP surgery costs were similar, even when restricting to outpatient surgeries only (mean [SD]: $14,697 [11,679] for all NP surgeries and $14,418 [10,581] for outpatient surgeries), since the majority of NP surgeries occurred in the outpatient setting. Cost estimates were similar between patients experiencing their first NP surgery and those receiving repeat NP surgery.
In this study, 1.7% of patients experienced a major complication in the 30 days after their index NP surgery. This is numerically higher than rates reported in previous studies in the US (1%),17 the UK (0.4%),14 Japan (0.1–0.5%),15,19 and Taiwan (0.5%). One potential reason for differences in major complication rates reported in this study versus previous studies may be due to improvements in data quality and coding for services. Additionally, previous studies have reported data from single-center analyses, and the present study is therefore more likely to reflect routine clinical practice. Furthermore, there are inter-country differences in clinical practices and healthcare systems that may affect the care received. The most frequent major complication reported in this study was major hemorrhage, which is consistent with findings from other studies reporting major complications in NP surgery patients.15,17
We did not explore potential trends between specific patient characteristics (including comorbidities) at baseline and risk of major complications with NP surgery (although the risk was shown to be higher in patients receiving revision surgery [2.0%] versus first surgery [1.6%]) and this will be an important area of research for future studies. The total medical costs incurred within 30 days by those who did experience complications were numerically higher by approximately 70% compared with patients with no major complications (mean cost: $27,406 vs $16,186, respectively).
In this real-world cohort, more than one-third of patients with CRSwNP also had asthma. Asthma has previously been associated with increased risk of polyp recurrence,20,21 and this was supported by findings from the current study which showed that more patients with asthma had a prior NP surgery.
A potential limitation of this analysis is that it considered only direct medical expenses incurred by third-party payers, and did not consider the wider societal perspective, including the impact on productivity or out-of-pocket expenses. Furthermore, we defined NP surgery costs as all costs that occurred on the date for outpatient surgery or costs occurred during the entire stay for patients who received surgery in the inpatient setting; it is possible that the costs in the inpatient setting may include costs unrelated to NP surgery. Additionally, only claims within 30 days of NP surgery were considered to ensure that complications observed were more likely to be related to the surgical procedure; as such, cost estimates did not include complications that may have occurred beyond the 30-day window. Major complications were identified using medical diagnosis and procedure codes; data on sensitivity and specificity of such codes have not yet been established. However, median (Q1–Q3) time to the onset of complication was as short as 3.5 (0–8) days, suggesting a high likelihood of association with the NP surgery. Furthermore, the study population was all commercially fee-for-service-insured and may not be representative of the entire US population; the 3-year baseline enrolment requirement further limited representativeness. It is possible that patients with an observation of first surgery in our analysis had actually received surgery prior to the 3-year baseline.
Although the overall cost and complication rate associated with NP surgery ultimately depends on a variety of factors, such as the case mix and type of surgery performed, this study provides a valuable real-world insight into the estimated costs of NP surgery and risk of major complications in US clinical practice.
In summary, using recent data in the US, this study indicated that NP surgery-related costs and rate of NP surgery complications were numerically higher than previously reported.
Acknowledgments
Medical writing support was provided by Martin Bell of Curo (part of Envision Pharma Group), and was funded by Sanofi and Regeneron Pharmaceuticals, Inc.
Author Contributions
All authors had full access to all the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Funding
This study was funded by Sanofi and Regeneron Pharmaceuticals, Inc.
Disclosure
Wenzhen Ge, Degang Wang and Siddhesh Kamat are employees and stockholders of Regeneron Pharmaceuticals, Inc. Shahid Siddiqui was an employee and stockholder of Regeneron Pharmaceuticals, Inc at the time of study conduct. Chien-Chia Chuang and Yongtao Li are employees and stockholders of Sanofi. Raj Rout was an employee and stockholder of Sanofi at the time of study conduct. The authors report no other conflicts of interest in this study.
References
1. Stevens WW, Schleimer RP, Kern RC. Chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol Pract. 2016;4(4):565–572. doi:10.1016/j.jaip.2016.04.012
2. Head K, Chong LY, Hopkins C, Philpott C, Schilder AG, Burton MJ. Short-course oral steroids as an adjunct therapy for chronic rhinosinusitis. Cochrane Database Syst Rev. 2016;4:CD011992. doi:10.1002/14651858.CD011992.pub2
3. Sanan A, Rabinowitz M, Rosen M, Nyquist G. Topical therapies for refractory chronic rhinosinusitis. Otolaryngol Clin North Am. 2017;50(1):129–141. doi:10.1016/j.otc.2016.08.011
4. Patel GB, Kern RC, Bernstein JA, Hae-Sim P, Peters AT. Current and future treatments of rhinitis and sinusitis. J Allergy Clin Immunol Pract. 2020;8(5):1522–1531. doi:10.1016/j.jaip.2020.01.031
5. Chen S, Zhou A, Emmanuel B, Garcia D, Rosta E. Systematic literature review of humanistic and economic burdens of chronic rhinosinusitis with nasal polyposis. Curr Med Res Opin. 2020;36(11):1913–1926. doi:10.1080/03007995.2020.1815683
6. DeConde AS, Mace JC, Levy JM, Rudmik L, Alt JA, Smith TL. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2017;127(3):550–555. doi:10.1002/lary.26391
7. Bachert C, Zhang N, Hellings PW, Bousquet J. Endotype-driven care pathways in patients with chronic rhinosinusitis. J Allergy Clin Immunol. 2018;141(5):1543–1551. doi:10.1016/j.jaci.2018.03.004
8. Haxel BR, Boessert P, Weyer-Elberich V, Fruth K. Course of olfaction after sinus surgery for chronic rhinosinusitis. Laryngoscope Investig Otolaryngol. 2017;2(5):269–275. doi:10.1002/lio2.109
9. Smith KA, Orlandi RR, Rudmik L. Cost of adult chronic rhinosinusitis: a systematic review. Laryngoscope. 2015;125(7):1547–1556. doi:10.1002/lary.25180
10. Velez FF, Sacks H, Messina J, Kozma CM, Malone D, Mahmoud R. Estimating the current cost of endoscopic sinus surgery in the US – a claims-based approach. Value Health. 2018;21:S13. doi:10.1016/j.jval.2018.04.064
11. Hunter TD, DeConde AS, Manes RP. Disease-related expenditures and revision rates in chronic rhinosinusitis patients after endoscopic sinus surgery. J Med Econ. 2018;21(6):610–615. doi:10.1080/13696998.2018.1452748
12. Ference EH, Suh JD, Tan BK, Smith SS. How often is sinus surgery performed for chronic rhinosinusitis with versus without nasal polyps? Am J Rhinol Allergy. 2018;32(1):34–39. doi:10.2500/ajra.2018.32.4495
13. Holy CE, Ellison JM, Schneider C, Levine HL. The impact of balloon catheter dilation on frequency of sinus surgery in the United States. Med Devices. 2014;7:83–89. doi:10.2147/MDER.S60054
14. Hopkins C, Browne JP, Slack R, et al. Complications of surgery for nasal polyposis and chronic rhinosinusitis: the results of a national audit in England and Wales. Laryngoscope. 2006;116(8):1494–1499. doi:10.1097/01.mlg.0000230399.24306.50
15. Suzuki S, Yasunaga H, Matsui H, Fushimi K, Kondo K, Yamasoba T. Complication rates after functional endoscopic sinus surgery: analysis of 50,734 Japanese patients. Laryngoscope. 2015;125(8):1785–1791. doi:10.1002/lary.25334
16. Chou TW, Chen PS, Lin HC, et al. Multiple analyses of factors related to complications in endoscopic sinus surgery. J Chin Med Assoc. 2016;79(2):88–92. doi:10.1016/j.jcma.2015.11.001
17. Ramakrishnan VR, Kingdom TT, Nayak JV, Hwang PH, Orlandi RR. Nationwide incidence of major complications in endoscopic sinus surgery. Int Forum Allergy Rhinol. 2012;2(1):34–39. doi:10.1002/alr.20101
18. Rudmik L, Soler ZM, Mace JC, Schlosser RJ, Smith TL. Economic evaluation of endoscopic sinus surgery versus continued medical therapy for refractory chronic rhinosinusitis. Laryngoscope. 2015;125(1):25–32. doi:10.1002/lary.24916
19. Asaka D, Nakayama T, Hama T, et al. Risk factors for complications of endoscopic sinus surgery for chronic rhinosinusitis. Am J Rhinol Allergy. 2012;26(1):61–64. doi:10.2500/ajra.2012.26.3711
20. Bassiouni A, Wormald PJ. Role of frontal sinus surgery in nasal polyp recurrence. Laryngoscope. 2013;123(1):36–41. doi:10.1002/lary.23610
21. Tan BK, Chandra RK, Pollak J, et al. Incidence and associated premorbid diagnoses of patients with chronic rhinosinusitis. J Allergy Clin Immunol. 2013;131(5):1350–1360. doi:10.1016/j.jaci.2013.02.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.