")
Back to Journals » Infection and Drug Resistance » Volume 12
Reactivation of herpesvirus in patients with hepatitis C treated with direct-acting antiviral agents
Received 20 August 2018
Accepted for publication 7 February 2019
Published 2 April 2019 Volume 2019:12 Pages 759—762
DOI https://doi.org/10.2147/IDR.S184598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Ali A Ghweil, Mohamad M Helal
Department of Tropical Medicine and Gastroenterology, Qena Faculty of Medicine, South Valley University, Qena, Egypt
Background: We performed a case-series analysis of reactivation of herpesvirus in patients with hepatitis C virus (HCV) infection treated with direct-acting antiviral (DAA) agents.
Methods: Eight cases were detected among 100 treated patients with DAA regimens in Qena University Hospital from June 2016 to June 2017. Herpesvirus was reactivated in eight patients who received DAA therapy. None of the cases had risk factor for herpes zoster reactivation.
Results: The DAA regimens used were sofosbuvir/daclatasvir in six cases and sofosbuvir/ledipasvir in two cases. Immune changes that follow HCV clearance might lead to reactivation of other viruses, such as herpesvirus.
Conclusion: Patients with HCV infection suspected of having herpesvirus infection should be treated promptly.
Keywords: HCV, HZ, DAA
Introduction
The development in hepatitis C virus (HCV) drug therapy in the last few years has led to the evolution of antiviral treatment for HCV with progression from interferon (IFN) to the direct-acting antivirals (DAAs).1
HCV infection can now be treated in almost all patients with these well-tolerated and effective combinations of oral DAAs. Even those patients who were not eligible for treatment by pegylated IFN–based regimens as in the case of patients with advanced liver disease or patients with comorbidities, or those who failed treatment, now have perfect choice of treatment modalities.2
Perelló et al reported herpesvirus (HV) reactivation in patients with HCV infection treated with DAA therapy.3
Immune system changes that occur after starting DAAs could play a role in HV reactivation. However, the exact mechanisms involved in HV reactivation in the early phases of HCV clearance in patients treated with DAAs are not clear.4
Patients and methods
One hundred chronic hepatitis C patients attending the outpatient clinics of the Tropical Medicine & Gastroenterology and the Internal Medicine Departments, Qena University Hospital were included in the study. All eligible patients were included according to the inclusion criteria approved by the National Committee for Control of Viral Hepatitis: age 18–75 years, HCV RNA positivity, any BMI (weight in kilograms/squared height in meters), and only treatment-naïve patients were included in this study. Exclusion criteria included hepatitis B virus (HBV) coinfection, HIV, decompensated liver cirrhosis, inadequately controlled diabetes mellitus (HbA1c >9%), hepatocellular carcinoma, or extrahepatic malignancy. Diagnosis of liver cirrhosis was on clinical basis involving laboratory tests and ultrasonography findings of liver cirrhosis and/or liver stiffness measurement ≥12.5 kPa.5
Patients were subjected to history taking, clinical examination, and routine laboratory workup. All patients were treated with sofosbuvir-based treatment regimens according to the approved treatment recommendations. The study was approved by the ethical committee of Qena Faculty of Medicine-South Valley University. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients before treatment.
Results
We present the baseline characteristics of the eight herpes zoster (HZ) infected patients in Table 1.
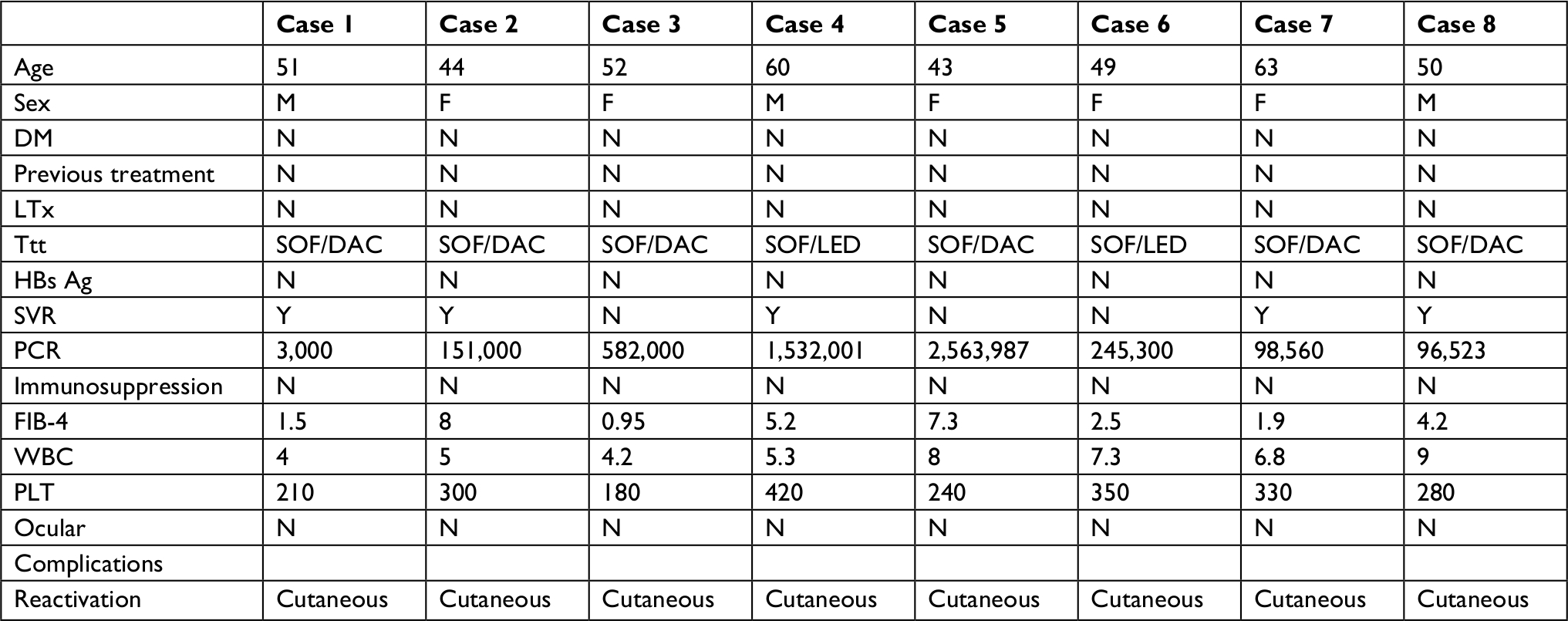 | Table 1 Baseline characteristics of the infected patients Abbreviations: Ag, antigen; DAC, daclatasvir; DM, diabetes mellitus; FIB-4, fibrosis 4; HBS, hepatitis B surface; LTx, liver transplant; PLT, platelet; SOF, sofobuvir; SVR, sustained virologic response; Ttt, treatment; WBC, white blood cell. |
Our study included 100 patients with mean age 45±12 years. Males were predominant, constituting 69% of our cases. Eighty percent of cases were noncirrhotic at the start of treatment and 20% of patients had evidence of liver cirrhosis. Sustained virologic response (SVR) was found in 94% of treated patients while 6% of the treated patients relapsed (Table 2).
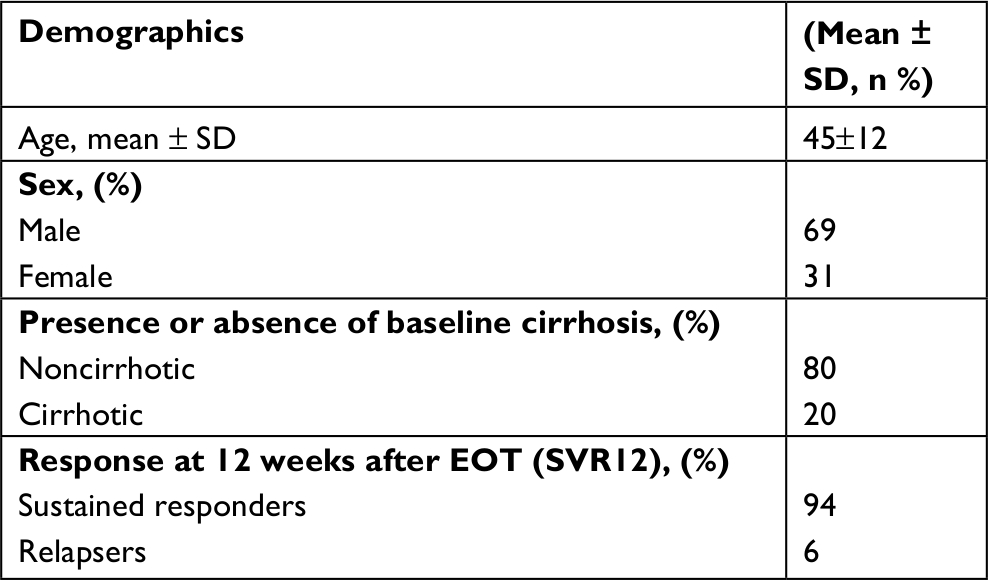 | Table 2 Demographic data in the studied group Abbreviation: SVR, sustained virologic response; EOT, end of treatment. |
Mean FIB-4 score for noninfected patients was 4.5±2.5 and for HZ patients it was 3.35. Mean HCV RNA level was 569,000 IU for HZ patients and 685,230 IU for noninfected patients. All patients were HCV genotype 4. No medications were reported for treatment of any comorbidities in our studied patients.
In the first 2 months after starting DAAs, we encountered four noncirrhotic cases with vesicular eruptions varying in distribution with two patients having vesicles over right side of the chest and two patients having the vesicles extending to the upper back. A diagnosis of HZ was made after consultation with a dermatology consultant who prescribed antiviral and analgesics. All patients achieved SVR.
After 6 months of treatment with DAAs, three cases (two noncirrhotics and one case with compensated cirrhosis) had maculopapular vesicles on an erythematous base over the right hemithorax. HZ diagnosis was established and confirmed by the dermatologist. Of the three cases, only one case had SVR.
After 1 year of treatment, a case with compensated cirrhosis developed vesicular rash on the right costal margin and was diagnosed as HZ after dermatology consultation. The case did not achieve SVR.
Liver enzyme changes together with WBC, neutrophils count, and HB level before, during, and upon reactivation of HZ are summarized in Table 3.
 | Table 3 Laboratory data for herpes zoster–infected patients before and after direct-acting antiviral treatment Notes: Bold values are significant of SVR as a risk factor for HZ reactivation. Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; AT after treatment; BT, before treatment; HB, hemoglobin; HCV, hepatitis C virus; WBC, white blood cell. |
We found that HZ reactivation was significantly associated with achievement of SVR after DAA treatment for HCV (P=0.000) but no significant association between liver condition and HZ reactivation was found (Table 4).
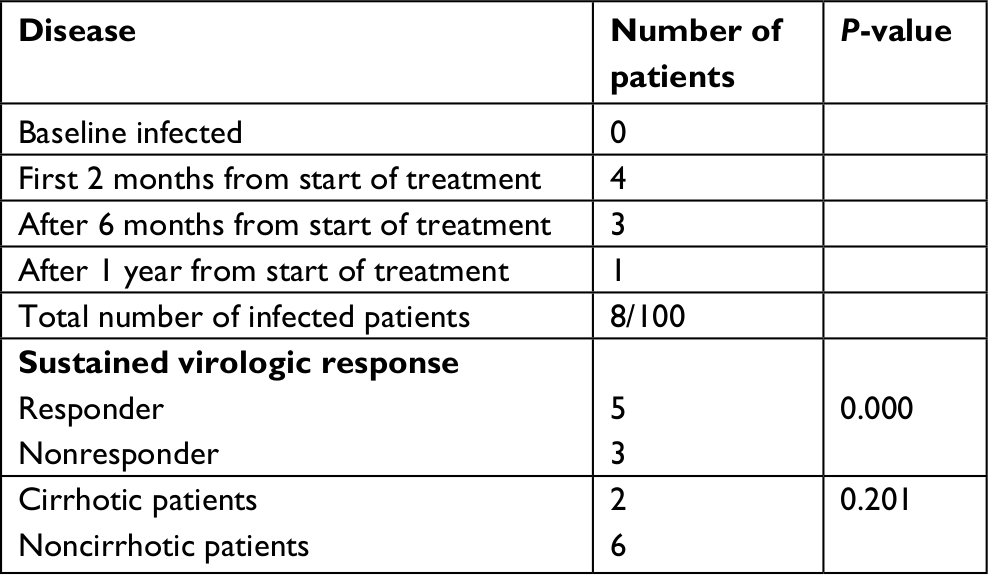 | Table 4 Herpes zoster reactivation after direct-acting antiviral treatment |
Discussion
Bacterial infections were relatively common among HCV patients treated by IFN, especially with advanced liver disease.6,7 With new DAA, infectious complications do not appear to be a problem in this setting. The HV family is known for its ability to establish life-long infection.8
HZ is the result of reactivation of a previous varicella-zoster virus (VZV) infection, remaining latent in cranial nerves and dorsal root ganglia and manifesting when there is immune system suppression.8,9 However, balance between latency and reactivation of VZV seems to be a complex process in which a precise understanding of the activated pathways by clinical factors is lacking.8
Our study was conducted in 100 HCV patients attending the outpatient clinic of Qena University Hospital. During a follow-up period of 1 year of these patients, we encountered eight cases of cutaneous HZ reactivation during DAA treatment with no postherpetic complications. There were no risk factors for HZ reactivation, no posttransplantation states, no physical stress, no immunocompromised status, and none of the patients were known to have diabetes or HIV infection. Of the eight cases, two patients were cirrhotic, and the remaining were noncirrhotic patients. We found that HZ reactivation was significantly associated with achievement of SVR and the liver condition had no role in HZ reactivation.
The same findings of HZ reactivation were reported in a recently published series of 10 cases out of 576 (2%) HCV patients treated with DAAs. The mean age of these patients was 67 years and three of them were receiving immunosuppressive therapy following liver transplantation.3
No evidence of HBV infection reactivation was encountered after DAA treatment of our HCV patients.
Suppressive effect of HCV infection on HZ that is removed after treatment by DAAs could be assumed as the main reason for HZ reactivation or may be a possible direct role of DAAs as a part of immune system restoration.10 Another explanation may be immune reconstitution inflammatory syndrome (IRIS), which can be seen in some HIV-infected patients after highly active antiretroviral therapy. This syndrome implies a pathologic inflammatory response to previously acquired conditions in the setting of an improved immune response, with mucocutaneous HZ being one of them. IRIS can happen even several months after initiation of highly active antiretroviral therapy.11
Conclusion
Even when a causal relationship is not confirmed, based on the temporal association and recent experience, we conclude that IFN-free regimens may be associated with increased incidence of HV reactivation, but more cases are required to confirm these findings. Also, we advise a high grade of clinical suspicion for early recognition and management of these cases. SVR achievement after DAA treatment and risk of HZ reactivation is not confirmed based on our small number of cases but it may give a clue to possible occurrence of HZ reactivation after DAAs due to immunity alteration, so high index of clinical suspicion may be needed to guarantee early and prompt management of such cases but more cases are required to prove that association.
Acknowledgments
This abstract of this paper was presented at the APASL Conference 2018, March 14–18, as a poster presentation with interim findings.
Disclosure
The authors report no conflicts of interest in this work.
References
Lutchman G, Kim WR. A glass half full: implications of screening for hepatitis C virus in the era of highly effective antiviral therapy. Hepatology. 2015;61(5):1455–1458. | ||
European Association for Study of Liver. EASL clinical practice guidelines: management of hepatitis C virus infection. J Hepatol. 2014;60(2):392–420. | ||
Perelló MC, Fernández-Carrillo C, Londoño MC, et al. Reactivation of herpesvirus in patients with hepatitis C treated with direct-acting antiviral agents. Clin Gastroenterol Hepatol. 2016;3565(16):30203–30208. | ||
European Medicines Agency (EMA). EMA Reviews Direct-Acting Antivirals for Hepatitis C Review to Investigate Possible Hepatitis B Re-activation. London: European Medicines Agency (EMA); 2016; EMA/199242/2016. | ||
Castera L, Forns X, Alberti A. Non-invasive evaluation of liver fibrosis using transient elastography. J Hepatol. 2008;48(5):835–847. | ||
Carrión JA, Martínez-Bauer E, Crespo G, et al. Antiviral therapy increases the risk of bacterial infections in HCV-infected cirrhotic patients awaiting liver transplantation: a retrospective study. J Hepatol. 2009;50(4):719–728. | ||
Londoño M-C, Perelló C, Cabezas J, et al. The addition of a protease inhibitor increases the risk of infections in patients with hepatitis C-related cirrhosis. J Hepatol. 2015;62(2):311–316. | ||
Grinde B. Herpesviruses: latency and reactivation – viral strategies and host response. J Oral Microbiol. 2013;5(1):22766. | ||
Pavlopoulou ID, Poulopoulou S, Melexopoulou C, et al. Incidence and risk factors of herpes zoster among adult renal transplant recipients receiving universal antiviral prophylaxis. BMC Infect Dis. 2015;15(1):285. | ||
El Kassas M, Wifi MN, Mahdy R, et al. Herpes zoster reactivation in patients with chronic hepatitis C under treatment with directly acting antiviral agents: a case series. Arab J Gastroenterol. 2017;18(1):39–41. | ||
Tsang CSP, Samaranayake LP. Immune reconstitution inflammatory syndrome after highly active antiretroviral therapy: a review. Oral Dis. 2010;16(3):248–256. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.