")
Back to Journals » Psychology Research and Behavior Management » Volume 13
REAC Cervicobrachial Neuromodulation Treatment of Depression, Anxiety, and Stress During the COVID-19 Pandemic
Authors Pinheiro Barcessat AR , Nolli Bittencourt M , Duarte Ferreira L , de Souza Neri E , Coelho Pereira JA, Bechelli F, Rinaldi A
Received 6 August 2020
Accepted for publication 21 October 2020
Published 9 November 2020 Volume 2020:13 Pages 929—937
DOI https://doi.org/10.2147/PRBM.S275730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Einar Thorsteinsson
Ana Rita Pinheiro Barcessat, 1,* Marina Nolli Bittencourt, 2,* Larissa Duarte Ferreira, 3 Erick de Souza Neri, 3 José Alfredo Coelho Pereira, 4 Fabio Bechelli, 5 Arianna Rinaldi 4, 6
1Postgraduate Program in Health Sciences, Federal University of Amapá, Macapá, Brazil; 2Department of Nursing, Federal University of Mato Grosso, Cuiabá, Brazil; 3Health and Biological Sciences Department, Federal University of Amapá, Macapá, Brazil; 4Research Department, Rinaldi Fontani Foundation, Florence, Italy; 5International Scientific Society of Neuro Psycho Physical Optimization with REAC Technology, São Paulo, Brazil; 6Department of Neuro Psycho Physio Pathology and Neuro Psycho Physical Optimization, Rinaldi Fontani Institute, Florence, Italy
*These authors contributed equally to this work
Correspondence: Arianna Rinaldi
Department of Neuro Psycho Physio Pathology and Neuro Psycho Physical Optimization, Rinaldi Fontani Institute, Florence, Italy
Email [email protected]
Introduction: In addition to the effects of coronavirus infection, the Covid-19 pandemic has induced widespread psychosocial distress, which has triggered the onset of anxious and depressive states, reactive to the socio-relational and economic situation induced by the pandemic. Some of our participants showed depressive and anxious attitudes even in the absence of real pictures of depression and anxiety. This phenomenon, combined with mechanisms of emulation and conditioning, can trigger a vicious cycle within interpersonal relationships and promote the administration of unnecessary treatments. Various approaches have been proposed to help populations suffering from psychosocial problems induced by the Covid-19 pandemic, but there is an objective difficulty in treating a large population.
Methods: To contain and reduce this widespread psychosocial unease, in this study we used two radio electric asymmetric conveyer (REAC) technology neuromodulation treatments, neuro postural optimization (NPO) and neuropsychophysical optimization–cervicobrachial (NPPO-CB), aimed at optimizing an individual’s response to the effects of environmental stressors. These treatments are quick and easy to administer; therefore, they can be administered to a large cohort of participants in a short time. To evaluate the effects of the REAC NPO and NPPO-CB treatments, the DASS-21 psychometric test was used because it has already been used to test depression, anxiety, and stress during the Covid-19 pandemic.
Results: The results of the study confirm the usefulness of REAC NPO and NPPO-CB treatments in helping participants to have better coping strategies for the environmental pressures and reduce the neuropsychological and behavioral effects induced by the Covid-19 pandemic.
Discussion: The results obtained in this study are consistent with previous clinical studies confirming the usefulness of the treatments to face neuropsychological and behavioral effects induced by exposome pressure.
Keywords: coronavirus, behavioral disorders, noninvasive neurostimulation, DASS-21
Corrigendum for this paper has been published
Introduction
While the Covid-19 pandemic has affected many countries, it has impacted different populations differently. Brazil has been particularly affected, particularly among countries in the equatorial area, where it was thought that the pandemic would not spread or at least be mitigated because of Brazil’s consistently warm climatic. This erroneous belief that equatorial and subequatorial populations would be protected from the pandemic probably contributed to aggravating a sense of psychological unease by triggering a sense of depression, anxiety, and stress1–4 in the population, which is difficult to self-manage. However, in all populations involved in the Covid-19 pandemic, its impact on mental health and emotional distress5,6 is increasingly observed in various clinical situations7 and healthy participants.8,9
Various therapeutic strategies have been proposed to deal with the problems of psychoemotional distress and its most common consequences induced by the Covid-19 pandemic, such as depression10,11 and anxiety.12–14 Essentially, these strategies are based on psychological support.6,15 However, psychological support requires prolonged and continuous physical or web-based contact between a psychologist and a patient, which limits the number of patients able to be treated. While other therapeutic neuromodulation techniques have previously demonstrated efficacy in treating these disorders, such as neuromodulation treatments using radio electric asymmetric conveyer (REAC) technology,16–23 although they have the advantage of requiring much shorter administration times, unfortunately, they are not web-based.
Our study aimed to investigate how the effects of two neuromodulation treatments using REAC technology, neuro postural optimization (NPO) and neuro-psycho-physical optimization–cervicobrachial (NPPO-CB), evaluated by a depression, anxiety, and stress scale (DASS-21), can help participants develop better coping strategies for environmental pressures never experienced before, such as those induced by the Covid-19 pandemic. These two neuromodulation treatments have been specifically designed and used to improve exposome response and resilience and counteract epigenetic conditioning. Moreover, these treatments are quick and easy to administer; therefore, they can be administered to a large cohort of participants over a short time.
To evaluate the effects of REAC NPO and NPPO-CB treatments on depression, anxiety, and stress, we used the DASS-21 psychometric test, which has already been used to test these three traits in previous studies on the Covid-19 pandemic.24–26
Materials and Methods
Ethics
This study is an arm of the REAC Neuromodulation Project of the Health Sciences Department of the Federal University of Amapá, Macapá, Brazil, approved by the ethical committee of the Federal University of Amapá (opinion number 3.640.674). All the study participants were informed about the purpose of the study. Consent was obtained by the study participants prior to study commencement. The study was conducted in full compliance with the Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Participants. This arm was specially created with the aim of social aid in a population that has reported psycho-social unease induced by the Covid-19 pandemic.
Study Design
This was an open-label interventional study conducted in six steps: administration of the first DASS-21 test (T0), preliminary assessment to verify the presence of functional dysmetria (FD) (T1), administration of the NPO treatment (T2), administration of the second assessment to verify the presence/disappearance of FD (T3), administration of the NPPO-CB treatment cycle (T4), administration of the second DASS-21 test (T5), and administration of the third assessment to verify the stability of the disappearance of FD (T6).
DASS-21 Psychometric Test
The DASS-21 test is a 21-item self-report instrument originally developed by Syd Lovibond and Peter Lovibond in 199533 to provide maximum differentiation between depressive and anxious symptoms.34 This test, a measure of mental health, focuses on the three traits of depression, anxiety, and stress. The analysis of these three traits is based on seven questions articulated as items 3, 5, 10, 13, 16, 17, and 21 for depression; items 2, 4, 7, 9, 15, 19, and 20 for anxiety; and items 1, 6, 8, 11, 12, 14, and 18 for stress. The DASS-21 assessment score for each cluster is shown in Table 1. Several studies have demonstrated the reliability and validity of the DASS-21 test as an effective and established tool to measure symptoms of depression, anxiety, and stress in both clinical and non-clinical conditions.35–37
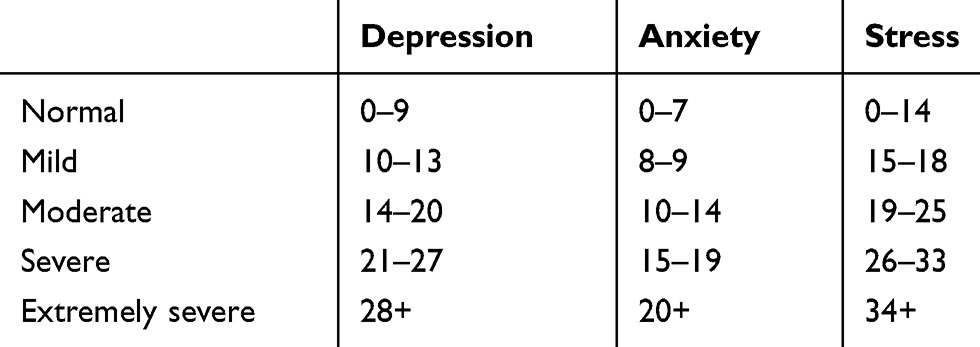 |
Table 1 DASS-21 Test Assessment Score |
REAC Technology
REAC technology was designed to optimize endogenous bioelectric activity. Cellular functions, such as cell migration, proliferation, differentiation, and regeneration and neurotransmission,38 and all other functions underlying life are only possible thanks to an endogenous bioelectric mechanism.39 This mechanism implies that an asymmetrical gradient exists in all the components of our organism that allows the creation of ionic flows, which in turn produce currents and consequently endogenous bioelectric fields (EBFs). Many mechanisms of various natures, including exposome pressure, can invalidate the correct and adequate production of ionic flows and therefore EBFs, causing a wide range of health problems. Because EBFs are also involved in neurotransmission mechanisms,39 their alteration can cause mood and behavior problems. The optimization of endogenous bioelectric activity through REAC technology is made possible because REAC devices emit in the environmental radio electric field, which interacts with the patient’s body through the device’s asymmetric conveyer probe (ACP). This interaction promotes the formation of endogenous gradients that promote the release of charge densities induced by external factors, thus facilitating neuromodulation processes.
REAC Neuromodulation Treatments
REAC neuromodulation treatments are based on a pulsed 5.8 GHz radio electric emission. Each treatment protocol is pre-programmed in a device by the manufacturer and cannot be modified by the operator. The REAC technology device used in this study was a BENE 110 universal model (ASMED, Florence, Italy). For the administration of the NPO and NPPO-CB treatments, the normal prophylaxis measures adopted for any treatment that requires an in-person approach (ie, environmental sanitation, gloves, and mask) were applied. Furthermore, ACPs are individual devices and have antibacterial properties due to the particular characteristics of their material. In the scientific literature and the post-market surveillance of REAC devices, no side effects have been reported.
REAC Neuro Postural Optimization Treatment
REAC NPO neuromodulation treatment has been designed to induce a more efficient and functional response27–29 in the whole brain, even in neurodegenerative diseases, such as Parkinson’s and Alzheimer’s.27,31,32 The efficacy of this treatment is evaluated by an assessment of the presence/absence of a neuropsychomotor phenomenon related to a dysfunctional response to the exposome, or FD.27,28 The REAC NPO consists of a single treatment administered with the REAC device probe to a specific area of the auricle scapha. The therapeutic efficacy is long-lasting, remaining after many years; therefore, the NPO treatment is only administered once.
REAC Neuro-Psycho-Physical Optimization Treatments
These treatments are aimed at improving strategies to optimize the allostatic response to environmental stressors and the exposome, allowing the reduction of dysfunctional adaptive behavior patterns that underlie many neuropsychological symptoms and pathologies16–23,30 and improving, as a consequence, the symptoms of depression, anxiety, and stress.16–23,40 Thus, NPPO treatments have been designed to optimize the individual response to environmental stressors, which can induce a wide range of disorders and pathologies. The alarm/stress reaction to stressors can result in increased muscle tension, detectable in the cervicobrachial region,41,42 where the ACP is applied during the NPPO-CB treatment (see Figure 1). The NPPO-CB treatment is administered in cycles of 18 sessions. Each session lasts about four minutes. The minimum time interval between sessions is 1 hour. The maximum number of sessions per day is usually four. In this study, the cycle was administered within approximately three weeks. The number of cycles performed depended on the patient’s condition.
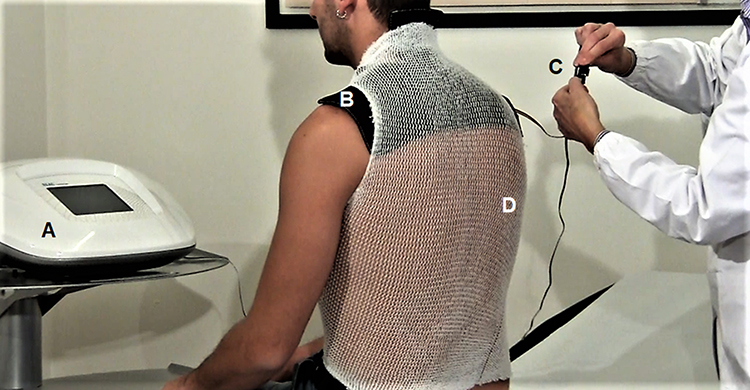 |
Figure 1 The image shows the administration of the NPPO-CB treatment. (A) Device based on REAC technology, model BENE 110 (ASMED, Florence, Italy); (B) Asymmetric conveyer probe (ACP). The ACP is connected to device (A) via a specific connection cable (C). The ACP is held in place using an elastic tubular mesh (D). |
Participants
Undertaken between March 23 and July 11, 2020, this study involved 155 people: 59 men (38.06%), with a mean age of 46.72 ± 12.93 years, and 96 women (61.94%), with a mean age of 53.48 ± 12.37 years. The overall mean age of the group was 51.04 ± 12.87 years. The participants had turned to our project in search of support for a sense of mental and physical discomfort, likely induced by the socio-economic situation created by the Covid-19 pandemic.
Because this study was predominantly aimed at humanitarian aid, the only inclusion criteria were age and a feeling of mental and physical discomfort. The exclusion criteria were pregnancy, diagnosis of psychiatric disease, and ongoing psychopharmacological or psychotherapeutic treatments.
After the administration of the first DASS-21 test (T0), 107 participants tested positive for at least one DASS-21 cluster. The other 48 participants, while reporting depressive, anxious, and stressful states, did not consistently show positivity to the DASS-21 test’s depression, anxiety, and stress clusters. After the DASS-21 test, all 155 participants were administered a test to verify the presence of functional dysmetry27,28 (T1) and afterward underwent a preliminary REAC neuromodulation treatment, NPO (T2).27–32 After the administration of the NPO, the test was repeated to check for the presence/disappearance of FD (T3).
At least one hour after the NPO treatment, the participants started the NPPO-CB treatment cycle (T4). The time interval between the first and last treatment sessions was approximately three weeks. DASS-21 tests were re-administered immediately after the administration of the last NPPO treatment (T5). The time points for the comparison of the DASS-21 test results were T0 and T5.
Statistical Analysis
The IBM Statistical Package for Social Science (SPSS), Version 22, was used for the statistical analysis. Summary statistics of the numbers and percentages of patients in the five categories (ie, normal, mild, moderate, severe, and extremely severe) at the two time points T0 and T5 for the three clusters (ie, depression, anxiety, and stress) were performed (see Figures 2–4).
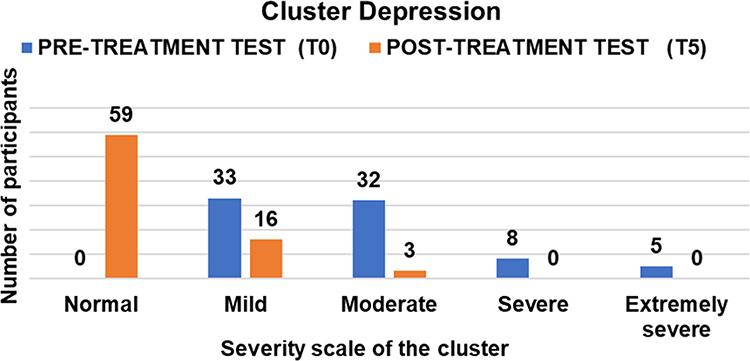 |
Figure 2 Graph of distribution of participants by severity level before and after REAC NPO, and NPPO-CB treatments for the depression cluster. |
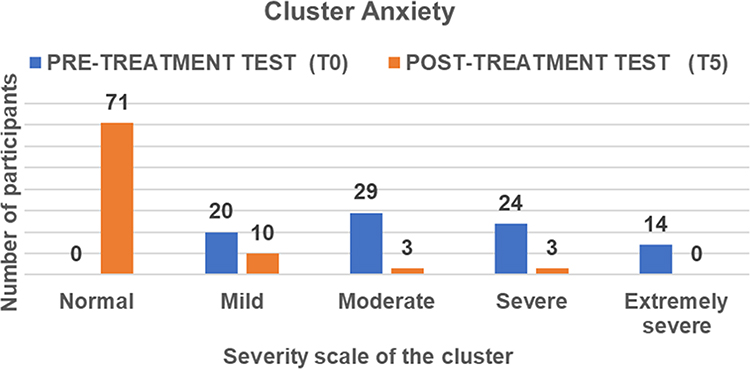 |
Figure 3 Graph of distribution of participants by severity level before and after REAC NPO, and NPPO-CB treatments for the anxiety cluster. |
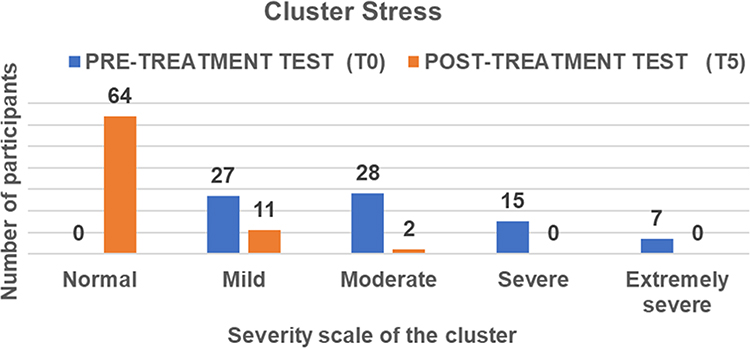 |
Figure 4 Graph of distribution of participants by severity level before and after REAC NPO, and NPPO-CB treatments for the stress cluster. |
The differences in means of the DASS-21 test assessments at T0 and T5, which represent the treatment effect size, are shown in Figure 5 (ie, participants positive to the DASS-21 test) and Figure 6 (ie, participants negative to the DASS-21 test). Wilcoxon and Sign tests were performed to confirm differences in the DASS-21 test assessment scores between T0 and T5 for the three clusters. For both tests, statistical significance was found at p < 0.001 (see Table 2).
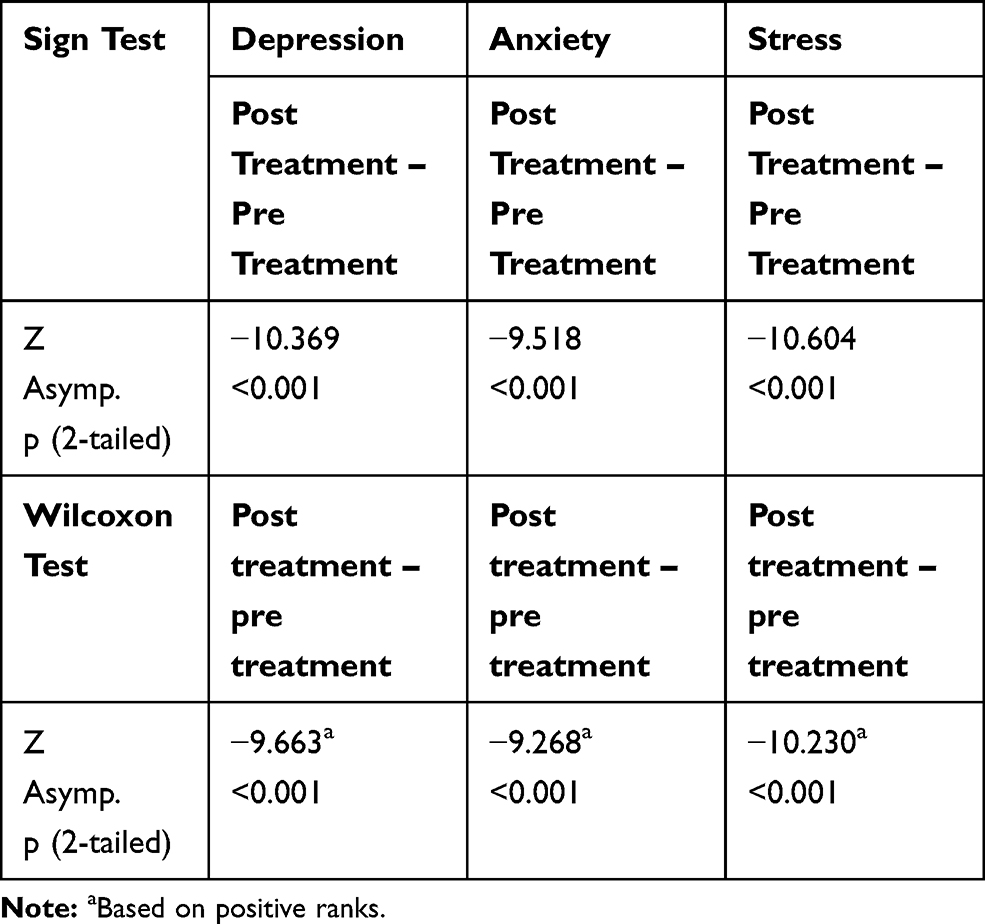 |
Table 2 Statistical Analysis – Sign Test and Wilcoxon Test |
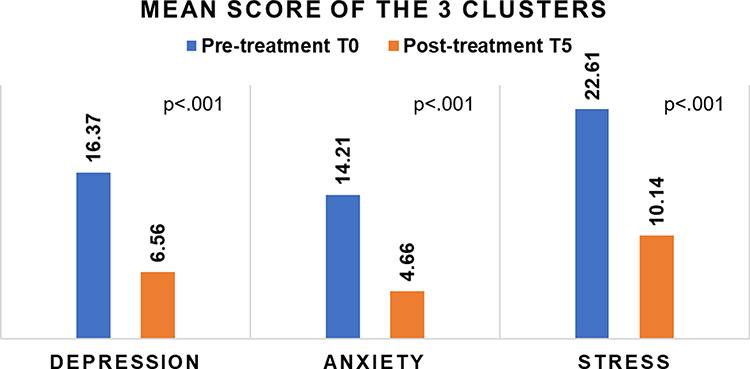 |
Figure 5 Group of the participants positive to DASS-21 test. The graph shows the improved values, moving towards the lower threshold of the normal range in all three clusters, before and after REAC NPO, and NPPO-CB treatments. |
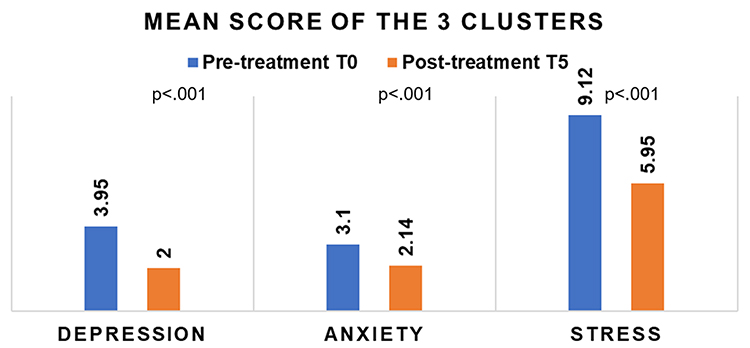 |
Figure 6 Group of the participants negative to all three clusters of DASS-21 test. The graph shows the improved values, moving towards the lower threshold of the normal range in all three clusters, before and after REAC NPO, and NPPO-CB treatments. |
Results
Functional Dysmetria
All 155 participants presented the phenomenon of FD at the first evaluation test (T1). Immediately after the administration of the NPO treatment (T2), they underwent a second evaluation test for FD (T3), which verified the disappearance of FD in 100% of the participants. The stability of this result was confirmed in 100% of the participants by a control test administered at the end of the NPPO-CB treatment cycle (T6).
DASS-21 Depression Cluster
For the depression cluster, 78 (50.32%) participants were found to be positive: 28 men (35.90%) and 50 women (64.10%). The overall mean age of this group was 50.10 ± 13.60 years. At T0, the mean score of depression was 16.37, corresponding to a moderate level of severity. At T5, the mean score of depression was 6.56, corresponding to a normal level of severity. Figure 2 graphically represents the distribution of the participants by level of severity before and after treatment. For 59 (75.64%) participants, REAC treatment reduced the depression symptoms to the normal range, and a general concentration trend toward lower depression scores was observed, with statistical significance between T0 and T5 (Table 2).
DASS-21 Anxiety Cluster
For the anxiety cluster, 87 (56.13%) participants were found to be positive: 29 men (33.33%) and 58 women (66.67%). The overall mean age of this group was 50.48 ± 16.54 years. At T0, the mean score of anxiety was 14.21, corresponding to a moderate level of severity. At T5, the mean score of anxiety was 4.66, corresponding to a normal level of severity. Figure 3 graphically represents the distribution of the participants by level of severity before and after treatment. In 71 (81.61%) participants, REAC treatment reduced the anxiety symptoms to the normal range, and a general distribution trend toward lower anxiety scores was observed, with statistical significance between T0 and T5 (Table 2).
DASS-21 Stress Cluster
For the stress cluster, 77 (49.68%) participants were found to be positive: 28 men (36.36%) and 49 women (63.64%). The overall mean age of this group was 50.93 ± 13.50 years. At T0, the mean score of stress was 22.61, corresponding to a moderate level of severity. At T5, the mean score of stress was 10.14, corresponding to a normal level of severity. Figure 4 graphically represents the distribution of the participants by level of severity before and after treatment. In 64 (83.12%) participants, REAC treatment reduced the stress symptom to the normal range, and a general distribution trend toward lower stress scores was observed, with statistical significance between T0 and T5 (Table 2).
Participants Negative to All Three DASS-21 Clusters
For all three clusters of the DASS-21 test, 48 (30.97%) participants were found to be negative: 20 men (41.67%) and 28 women (58.33%). The overall mean age of this group was 51.66 ± 16.33 years. Although these participants reported values within the normal range in all three DASS-21 clusters at T0; nevertheless, after the REAC treatments, they all improved their values, moving toward the lower threshold of the range of normality for all three clusters (Figure 6).
Discussion
The state of uncertainty for future planning induced in the population by the Covid-19 pandemic had already greatly impacted the emotional and behavioral health status of many of the participants. The prolongation of this situation will broaden the population affected by both mood and behavioral disorders, with undoubted social repercussions. It is therefore important to be able to face the challenges induced by the exposome response,43 resilience,44 and epigenetic conditioning45 that have been shown to play a role in the course of Covid-19 pandemic.
In this study, we observed that feelings of being depressed, anxious, and stressed, although asserted by a percentage of the participants, were not detectable by a specific test for depression, anxiety, and stress, the DASS-21. The psychosocial discomfort induced by the Covid-19 pandemic has probably triggered, and also though emulation, the depressive, anxious, and stressed attitudes that some of the participants elevated in their interpersonal relationships, even without suffering from depression, anxiety, and stress. This aspect must be carefully evaluated because it could lead to the administration of unnecessary treatments. Furthermore, this aspect risks promoting further psychosocial problems when these participants interact with other participants through conditioning. Although various approaches have been proposed to help populations suffering from psychosocial problems induced by the Covid-19 pandemic,15 there is an objective difficulty in treating a large population. Therefore, to try to alleviate psychological and psychiatric disorders induced by the Covid-19 pandemic, it would be appropriate to have effective methods that can be administered to large populations in a simple way with short administration times. The neurostimulation/neuromodulation techniques already used for this purpose are primarily transcranial direct current stimulation techniques.46,47 In this study, we used REAC technology, a neurobiological stimulation/modulation technology, that allows for even faster administration times: the NPO treatment takes a few milliseconds, while the NPPO-CB treatment takes less than five minutes. These two treatments have been studied to improve the allostatic response,48 which is also, and above all, reflected in the psychomotor49 and behavioral attitude.50
The results obtained in this study are consistent with previous clinical studies, confirming the usefulness of the treatments for facing the neuropsychological and behavioral effects induced by exposome pressure. Another interesting aspect we observed in this study is that participants not positive for DASS-21 clusters achieved an improvement compared with their initial test values. This confirms the capacity of REAC neuromodulation treatments to optimize responses to environmental stressors. Therefore, even populations without a formal psychiatric diagnosis should have access to REAC neuromodulation treatments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
A.R. is the daughter of Salvatore Rinaldi and Vania Fontani, authors of the REAC technology patent and reports no other potential conflicts of interest for this work. The other authors declare no conflicts of interest.
References
1. Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. 2020;16(1):57. doi:10.1186/s12992-020-00589-w
2. Picaza Gorrochategi M, Eiguren Munitis A, Dosil Santamaria M, Ozamiz Etxebarria N. Stress, anxiety, and depression in people aged over 60 in the COVID-19 outbreak in a sample collected in Northern Spain. Am J Geriatr Psychiatry. 2020;28(9):993–998. doi:10.1016/j.jagp.2020.05.022
3. Ozamiz-Etxebarria N, Dosil-Santamaria M, Picaza-Gorrochategui M, Idoiaga-Mondragon N. Stress, anxiety, and depression levels in the initial stage of the COVID-19 outbreak in a population sample in the northern Spain. Cad Saude Publica. 2020;36(4):e00054020. doi:10.1590/0102-311x00054020
4. Castelli L, Di Tella M, Benfante A, Romeo A. The spread of COVID-19 in the Italian population: anxiety, depression, and post-traumatic stress symptoms. Can J Psychiatry. 2020;65(10):731–732. doi:10.1177/0706743720938598
5. Bergerot PG, Bergerot CD, Philip EJ. Emotional distress during the COVID-19 pandemic: psycho-oncology perspective. Oncology. 2020;34(7):270–271.
6. Dominguez-Salas S, Gomez-Salgado J, Andres-Villas M, Diaz-Milanes D, Romero-Martin M, Ruiz-Frutos C. Psycho-emotional approach to the psychological distress related to the COVID-19 pandemic in Spain: a cross-sectional observational study. Healthcare (Basel). 2020;8(3).
7. de Joode K, Dumoulin DW, Engelen V, et al. Impact of the coronavirus disease 2019 pandemic on cancer treatment: the patients’ perspective. Eur J Cancer. 2020;136:132–139. doi:10.1016/j.ejca.2020.06.019
8. Marelli S, Castelnuovo A, Somma A, et al. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J Neurol. 2020. doi:10.1007/s00415-020-10056-6
9. Husky MM, Kovess-Masfety V, Swendsen JD. Stress and anxiety among university students in France during Covid-19 mandatory confinement. Compr Psychiatry. 2020;102:152191. doi:10.1016/j.comppsych.2020.152191
10. Shader RI. COVID-19 and depression. Clin Ther. 2020;42(6):962–963. doi:10.1016/j.clinthera.2020.04.010
11. Ustun G. Determining depression and related factors in a society affected by COVID-19 pandemic. Int J Soc Psychiatry. 2020;20764020938807.
12. Zhang J, Yang Z, Wang X, et al. The relationship between resilience, anxiety and depression among patients with mild symptoms of COVID-19 in China: a cross-sectional study. J Clin Nurs. 2020;29(21–22):4020–4029. doi:10.1111/jocn.15425
13. Yohannes AM. COPD patients in a COVID-19 society: depression and anxiety. Expert Rev Respir Med. 2020;1–3. doi:10.1080/17476348.2020.1787835
14. Paz C, Mascialino G, Adana‐Díaz L, et al. Anxiety and depression in patients with confirmed and suspected COVID-19 in Ecuador. Psychiatry Clin Neurosci. 2020;74(10):554–555. doi:10.1111/pcn.13106
15. Kaslow NJ, Friis-Healy EA, Cattie JE, et al. Flattening the emotional distress curve: a behavioral health pandemic response strategy for COVID-19. Am Psychol. 2020;75(7):875–886. doi:10.1037/amp0000694
16. Rinaldi S, Fontani V, Aravagli L, Mannu P. Psychometric evaluation of a radio electric auricular treatment for stress related disorders: a double-blinded, placebo-controlled controlled pilot study. Health Qual Life Outcomes. 2010;8:31. doi:10.1186/1477-7525-8-31
17. Rinaldi S, Fontani V, Aravagli L, Margotti ML. Psychological and symptomatic stress-related disorders with radio-electric treatment: psychometric evaluation. Stress Health. 2010;26(5):350–358. doi:10.1002/smi.1298
18. Rinaldi S, Fontani V, Moretti E, et al. A new approach on stress-related depression and anxiety: neuro-psycho- physical-optimization with radio electric asymmetric-conveyer. Indian J Med Res. 2010;132:189–194.
19. Fontani V, Mannu P, Castagna A, Rinaldi S. Social anxiety disorder: radio electric asymmetric conveyor brain stimulation versus sertraline. Patient Prefer Adherence. 2011;5:581–586.
20. Fontani V, Rinaldi S, Aravagli L, Mannu P, Castagna A, Margotti ML. Noninvasive radioelectric asymmetric brain stimulation in the treatment of stress-related pain and physical problems: psychometric evaluation in a randomized, single-blind placebo-controlled, naturalistic study. Int J Gen Med. 2011;4:681–686.
21. Olivieri EB, Vecchiato C, Ignaccolo N, et al. Radioelectric brain stimulation in the treatment of generalized anxiety disorder with comorbid major depression in a psychiatric hospital: a pilot study. Neuropsychiatr Dis Treat. 2011;7:449–455.
22. Rinaldi S, Fontani V, Aravagli L, et al. Stress-related psycho-physiological disorders: randomized single blind placebo controlled naturalistic study of psychometric evaluation using a radio electric asymmetric treatment. Health Qual Life Outcomes. 2011;9:54. doi:10.1186/1477-7525-9-54
23. Fontani V, Aravagli L, Margotti ML, Castagna A, Mannu P, Rinaldi S. Neuropsychophysical optimization by REAC technology in the treatment of: sense of stress and confusion. Psychometric evaluation in a randomized, single blind, sham-controlled naturalistic study. Patient Prefer Adherence. 2012;6:195–199.
24. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729.
25. Tan BYQ, Chew NWS, Lee GKH, et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann Intern Med. 2020;173(4):317–320. doi:10.7326/M20-1083
26. Rizwana S, Muhammad Raheel R, Muhammad U, et al. Assessment of depression, anxiety and stress among COVID-19 patients by using DASS-21 scales. J Med Case Rep Rev. 2020;3(6).
27. Mura M, Castagna A, Fontani V, Rinaldi S. Preliminary pilot fMRI study of neuropostural optimization with a noninvasive asymmetric radioelectric brain stimulation protocol in functional dysmetria. Neuropsychiatr Dis Treat. 2012;8:149–154.
28. Rinaldi S, Mura M, Castagna A, Fontani V. Long-lasting changes in brain activation induced by a single REAC technology pulse in wi-fi bands. Randomized double-blind fMRI qualitative study. Sci Rep. 2014;4:5668. doi:10.1038/srep05668
29. Rinaldi S, Fontani V, Castagna A. Brain activity modification produced by a single radioelectric asymmetric brain stimulation pulse: a new tool for neuropsychiatric treatments. Preliminary fMRI study. Neuropsychiatr Dis Treat. 2011;7:649–654. doi:10.2147/NDT.S26123
30. Fontani V, Rinaldi S, Castagna A, Margotti ML. Noninvasive radioelectric asymmetric conveyor brain stimulation treatment improves balance in individuals over 65 suffering from neurological diseases: pilot study. Ther Clin Risk Manag. 2012;8:73–78.
31. Olazaran J, Gonzalez B, Lopez-Alvarez J, et al. Motor effects of REAC in advanced alzheimer’s disease: results from a pilot trial. J Alzheimers Dis. 2013;36(2):297–302. doi:10.3233/JAD-130077
32. Olazaran J, Gonzalez B, Osa-Ruiz E, et al. Motor effects of radio electric asymmetric conveyer in alzheimer’s disease: results from a cross-over trial. J Alzheimers Dis. 2014;42(1):325–332. doi:10.3233/JAD-140417
33. Lovibond S, Lovibond PF. Manual for the Depression Anxiety Stress Scales. Psychology Foundation of Australia; 1996.
34. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–343. doi:10.1016/0005-7967(94)00075-U
35. Sinclair SJ, Siefert CJ, Slavin-Mulford JM, Stein MB, Renna M, Blais MA. Psychometric evaluation and normative data for the depression, anxiety, and stress scales-21 (DASS-21) in a nonclinical sample of U.S. adults. Eval Health Prof. 2012;35(3):259–279.
36. Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(Pt2):227–239. doi:10.1348/014466505X29657
37. Vasconcelos-Raposo J, Fernandes HM, Teixeira CM. Factor structure and reliability of the depression, anxiety and stress scales in a large Portuguese community sample. Span J Psychol. 2013;16:E10. doi:10.1017/sjp.2013.15
38. McCaig CD, Rajnicek AM, Song B, Zhao M. Controlling cell behavior electrically: current views and future potential. Physiol Rev. 2005;85(3):943–978. doi:10.1152/physrev.00020.2004
39. Levin M. Molecular bioelectricity: how endogenous voltage potentials control cell behavior and instruct pattern regulation in vivo. Mol Biol Cell. 2014;25(24):3835–3850.
40. Rinaldi A, Rinaldi C, Coelho Pereira JA, et al. Radio electric asymmetric conveyer neuromodulation in depression, anxiety, and stress. Neuropsychiatr Dis Treat. 2019;15:469–480. doi:10.2147/NDT.S195466
41. Elbinoune I, Amine B, Shyen S, Gueddari S, Abouqal R, Hajjaj-Hassouni N. Chronic neck pain and anxiety-depression: prevalence and associated risk factors. Pan Afr Med J. 2016;24:89. doi:10.11604/pamj.2016.24.89.8831
42. Roman-Liu D, Grabarek I, Bartuzi P, Choromanski W. The influence of mental load on muscle tension. Ergonomics. 2013;56(7):1125–1133. doi:10.1080/00140139.2013.798429
43. Maguire G. Better preventing and mitigating the effects of Covid-19. Future Sci OA. 2020;6(6):FSO586. doi:10.2144/fsoa-2020-0051
44. Vinkers CH, van Amelsvoort T, Bisson JI, et al. Stress resilience during the coronavirus pandemic. Eur Neuropsychopharmacol. 2020;35:12–16. doi:10.1016/j.euroneuro.2020.05.003
45. Chlamydas S, Papavassiliou AG, Piperi C. Epigenetic mechanisms regulating COVID-19 infection. Epigenetics. 2020;1–8. doi:10.1080/15592294.2020.1796896
46. Shinjo SK, Brunoni AR, Okano AH, Tanaka C, Baptista AF. Transcranial direct current stimulation relieves the severe anxiety of a patient with COVID-19. Brain Stimul. 2020;13(5):1352–1353. doi:10.1016/j.brs.2020.07.004
47. Azabou E, Bao G, Heming N, et al. Randomized controlled study evaluating efficiency of low intensity Transcranial Direct Current Stimulation (tDCS) for dyspnea relief in mechanically ventilated COVID-19 patients in ICU: the tDCS-DYSP-COVID protocol. Front Med. 2020;7:372. doi:10.3389/fmed.2020.00372
48. Ullmann E, Perry SW, Licinio J, et al. From allostatic load to allostatic state-an endogenous sympathetic strategy to deal with chronic anxiety and stress? Front Behav Neurosci. 2019;13:47. doi:10.3389/fnbeh.2019.00047
49. Parsons PA. Fluctuating asymmetry: an epigenetic measure of stress. Biol Rev Camb Philos Soc. 1990;65(2):131–145. doi:10.1111/j.1469-185X.1990.tb01186.x
50. McEwen BS. Allostasis and allostatic load implications for neuropsychopharmacology. Neuropsychopharmacology. 2000;22(2):108–124. doi:10.1016/S0893-133X(99)00129-3
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.