")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 11
Rationale and design of the VISION study: a randomized, open-label study to evaluate the long-term safety of vonoprazan as maintenance treatment in patients with erosive esophagitis
Authors Uemura N, Kinoshita Y, Haruma K, Yao T, Kushima R, Kanoo T
Received 22 June 2017
Accepted for publication 15 October 2017
Published 24 January 2018 Volume 2018:11 Pages 51—56
DOI https://doi.org/10.2147/CEG.S144149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Andreas M. Kaiser
Naomi Uemura,1 Yoshikazu Kinoshita,2 Ken Haruma,3 Takashi Yao,4 Ryoji Kushima,5 Tatsuhiro Kanoo6
1Department of Gastroenterology and Hepatology, National Center for Global Health and Medicine, Kohnodai Hospital, Chiba, Japan; 2Department of Gastroenterology and Hepatology, Faculty of Medicine, Shimane University, Shimane, Japan; 3Department of General Internal Medicine 2, Kawasaki Medical School General Medical Center, Okayama, Japan; 4Department of Human Pathology, Juntendo University Graduate School of Medicine, Tokyo, Japan; 5Department of Clinical Laboratory Medicine, Shiga University of Medical Science Hospital, Shiga, Japan; 6Takeda Pharmaceutical Co., Ltd, Osaka, Japan
Abstract: Erosive esophagitis (EE) occurs when the epithelial mucosa is damaged due to gastric acid reflux, and the incidence of this disease is increasing in Japan due to changes in diet and lifestyle. The condition can be treated using proton pump inhibitors (PPIs) that act by irreversibly blocking the H+,K+-ATPase responsible for acid secretion. Vonoprazan is a K+ competitive channel inhibitor, which reversibly and potently inhibits gastric acid secretion. However, long-term data on vonoprazan use are limited. The aim of the VISION trial is to investigate the long-term efficacy and safety of vonoprazan in comparison with the PPI lansoprazole. This randomized, multicenter, 5-year, open-label study has a planned recruitment of 195 participants (2:1 allocation vonoprazan:lansoprazole) from 33 sites in Japan. The study comprises an 8-week “healing” phase (vonoprazan 20 mg or lansoprazole 30 mg p.o.) and a 260-week “maintenance” phase (vonoprazan 10 mg or lansoprazole 15 mg). Safety populations in both phases are defined as participants who receive at least one dose of the study or control drug in the healing and maintenance phases, respectively. The full analysis set in both phases is defined as participants who are randomized and receive at least one dose of the study or control drug in the healing and maintenance phases, respectively. The primary endpoint of the study is the histopathological evaluation of gastric mucosa for the presence of neoplastic alteration of gastric mucosal epithelial cells. Secondary efficacy endpoints include endoscopic EE recurrence rate and EE healing rate, and secondary safety endpoints include incidence of adverse events (coded using MedDRA terminology) and endoscopic evaluation of malignant changes in the gastric mucosa. Patient recruitment started in March 2016 and is now complete. The estimated study completion date is February 2022.
Keywords: erosive esophagitis, gastric mucosa, lansoprazole, long-term safety, vonoprazan, K+ competitive channel inhibitor, neoplasia
Introduction
Erosive esophagitis (EE) is a condition in which gastroesophageal reflux causes esophageal mucosal breaks (damage), defined as an area of slough or erythema with a discrete lined demarcation between it and adjacent mucosa.1,2 It occurs as a consequence of gastric acid reflux, resulting from relaxation of the lower esophageal sphincter (LES), reduced esophageal clearance function (eg, esophageal motility), and impaired esophageal mucosal defense mechanisms.3 Increased exposure to gastric acid correlates with the severity of EE.4 The prevalence of EE in Japan, which has been increasing since the 1990s, is approximately 10%. This increase is thought to be primarily due to changes in environmental factors that have resulted in increased gastric acid secretion (ie, westernization of diet, a reduction in the rate of Helicobacter pylori infection) together with an aging population.5,6 Additional risk factors include high body mass index/obesity and hiatus hernia.6,7
Treatment of EE is centered around reducing gastric acid secretion, and the current recommended first-line therapy is the use of proton pump inhibitors (PPIs).1 Healing rates of EE with the use of a PPI are 80%–90% after 8 weeks of treatment,8,9 although rates tend to be lower in patients with more severe disease at baseline.10 While current guidelines from Japan recommend the use of more aggressive (double-dose, twice-daily) PPI maintenance therapy in severe EE to prevent recurrence,1 their potent acid-suppressing effects over the long-term give rise to safety concerns. Recent meta-analyses indicate that long-term use of PPIs is associated with an increased risk of gastric mucosal hyperplasia, especially enterochromaffin-like cells,11,12 and that the risk of corpus atrophy is markedly higher in H. pylori-positive patients than in H. pylori-negative patients.12
Vonoprazan is an orally bioavailable potassium (K+)-competitive acid blocker approved for the treatment of EE in Japan.13,14 Similar to PPIs, vonoprazan inhibits the H+,K+-ATPase enzyme, which is responsible for catalyzing the final stage of gastric acid secretion.13 Unlike PPIs, however, the enzyme is inhibited in a K+-competitive and reversible manner.15 Preclinical studies showed that vonoprazan was associated with a greater degree and more sustained suppression of gastric acid secretion as compared with the PPI, lansoprazole15,16; moreover, in a double-blind, randomized, controlled trial, vonoprazan was non-inferior to lansoprazole, and was well-tolerated for up to 52 weeks.17 In a randomized, open-label, crossover study in healthy male subjects, vonoprazan demonstrated a more rapid and sustained acid-inhibitory effect (pH4 holding time ratio [HTR]) than equivalent doses of esomeprazole or rabeprazole.18
Investigating the safety of long-term vonoprazan is important, as vonoprazan is a more potent inhibitor of acid secretion than other acid inhibitors, including PPIs. Therefore, clinical studies comparing the long-term safety of vonoprazan in comparison with PPIs are planned. As data on the efficacy and safety of long-term vonoprazan use in EE are limited, the Vonoprazan study In patients with eroSIve esophagitis to evaluate lONg-term safety (VISION) will assess the long-term safety of vonoprazan when given as maintenance treatment for up to 5 years in patients with EE.
Methods
Study design and treatment
VISION is a randomized, multicenter, 5-year open-label study that is being conducted across 33 sites in Japan. The study comprises two phases: the “healing” phase of 8 weeks, and the “maintenance” phase of 260 weeks (Figure 1). Patients endoscopically diagnosed with EE (Los Angeles [LA] classification grades A–D)19 at the start of treatment (Week 0 of the healing phase) will be randomly assigned to either vonoprazan 20 mg or lansoprazole 30 mg, given orally once daily (OD) for up to 8 weeks. Patients with endoscopically confirmed healed EE at Week 4 or 8 in the healing phase will be eligible to enter the maintenance phase, wherein vonoprazan 10 mg or lansoprazole 15 mg OD will be administered for up to 260 weeks. If the starting dose within the maintenance phase is considered suboptimal, it may be increased to vonoprazan 20 mg or lansoprazole 30 mg OD. Any patient not benefitting from treatment at the end of the healing phase (Week 8) will complete the study without entering the maintenance phase. Full details of patient eligibility criteria are shown in Table 1.
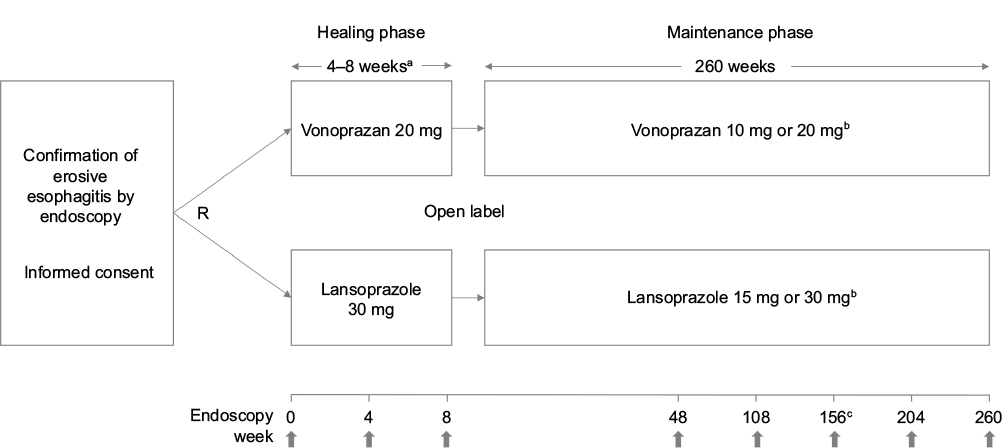 | Figure 1 VISION study design. Notes: aPatients with evidence of healing at Week 4 may progress directly to the maintenance phase without waiting until Week 8. Patients without evidence of healing by Week 8 will complete the study at that point. bDose may be increased at the start of the maintenance phase at the discretion of the physician. cOnce data are collected from all patients, an interim analysis will be conducted. |
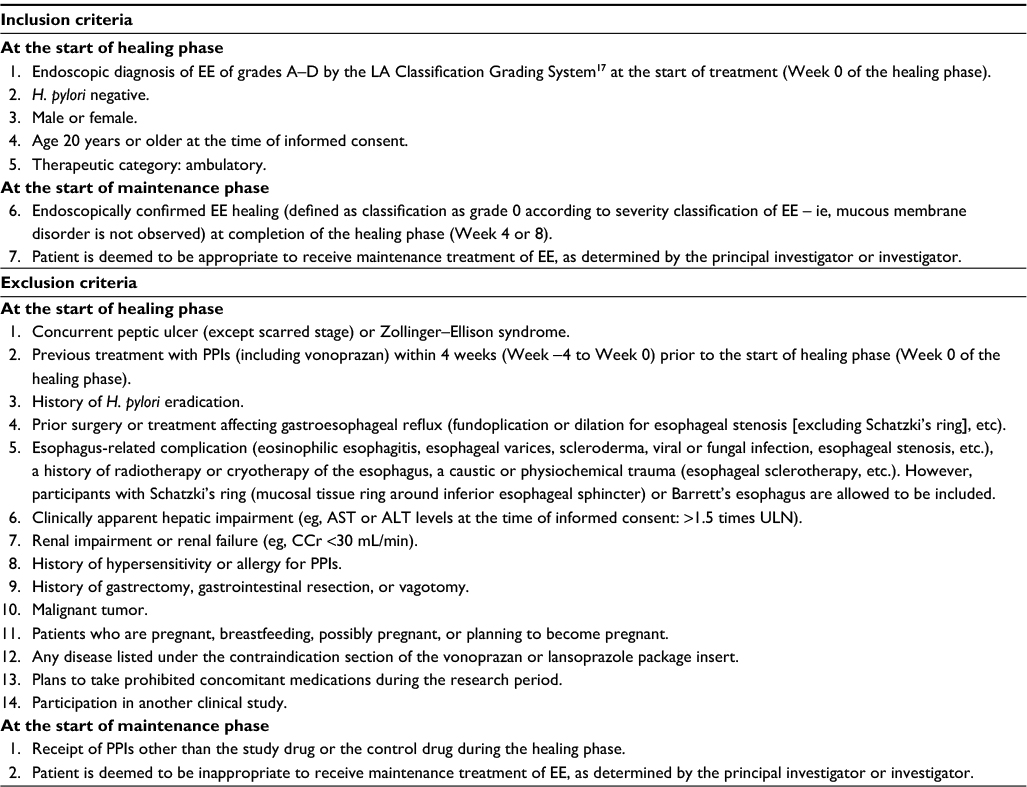 | Table 1 VISION inclusion and exclusion criteria Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; CCr, creatinine clearance; EE, erosive esophagitis; PPI, proton-pump inhibitor; ULN, upper limit of normal. |
Patients will be randomized through allocation of the study drug or control drug via a web registration system. Patients will make a maximum number of 18 visits to the clinic; at Weeks 0 and 4 during the healing phase (Week 8 for subjects with no endoscopic healing of EE at Week 4 in the healing phase) and, then, 12-weekly visits in the maintenance phase up to Week 108, followed by 24-weekly visits up to Week 228, and a final visit at Week 260. Patients may receive treatment until unacceptable toxicity, patient withdrawal/physician decision, or major deviation from the study protocol.
This study will be conducted in accordance with the ethical principles outlined in the Declaration of Helsinki Ethical Guidelines for Clinical Research, the Ethical Guidelines on Biomedical Research Involving Human Subjects, and the guidelines for Good Clinical Practice (ICH-E6). Approval from the Ethical Review Boards will be sought from each of the different study sites, and informed, written consent will be obtained from all study participants.
Study endpoints
The primary endpoint of the study is histopathological evaluation of the gastric mucosa – specifically, assessing biopsy samples for the presence or absence of neoplastic alteration of epithelial cells and hyperplasia of gastric mucosal epithelial cells, including parietal cells, enterochromaffin-like cells, G cells, and foveolar cells. Other histopathological signs include foveolar hyperplasia, endocrine cell proliferation in the body mucosa, and G-cell hyperplasia in the antral mucosa. Secondary efficacy endpoints are endoscopic EE recurrence rate and EE healing rate, whereas secondary safety endpoints include the incidence of adverse events (AEs) and endoscopic findings showing the presence or absence of fundic gland polyp, hyperplasic polyp, cobblestone mucosa, multiple white and flat elevated lesions, and black spots. Furthermore, safety endpoints include histological evaluation of gastritis using the Sydney classification,20 that is, mononuclear infiltration, neutrophilic infiltration, atrophy, intestinal metaplasia, and H. pylori infection.
Additional assessments to be carried out during the study period include: serum gastrin level; pepsinogen I and II levels and ratios; serum chromogranin A level; laboratory test results; Barrett’s esophagus; and esophageal hiatal hernia.
Assessments
Patient demographics, medical history, and prior drug treatment will be recorded at Week 0. Physical examination, vital signs, and laboratory tests will be conducted at all visits during the healing and maintenance phases, as will recording of concomitant drugs and comorbid disorders. Fasting levels of serum gastrin, pepsinogen I and II, and serum chromogranin A levels will be measured at Weeks 0, 4, and 8 during the healing phase, and at Weeks 12, 24, 48, 108, 156, 204, and 260 in the maintenance phase, except for serum gastrin which will be measured at Weeks 12 and 260 only. Endoscopy will be conducted at Weeks 0, 4, and 8 during the healing phase, and at Weeks 48, 108, 156, 204, and 260 in the maintenance phase. Histopathology of gastric mucosa and histological evaluation of gastritis will be undertaken centrally by two pathologists specializing in gastrointestinal histopathology at Week 0; these investigations will then be re-evaluated at Weeks 48, 108, 156, 204, and 260 in the maintenance phase. An H. pylori urea breath test will also be conducted at Week 0 (after initial endoscopy), as well as CYP2C19 genotype testing.
At each study visit, investigators shall pay attention to the presence of AEs, especially diarrhea, gastrointestinal infections, bone fracture, and pneumonia. AEs will be graded according to severity, with mild defined as an event that is transient and easily tolerated by the subject, moderate as an event that interrupts the subject’s usual activities, and severe as an event that causes considerable interference with the subject’s usual activities.
Medication compliance will be assessed by the investigator at each visit, with drug taking classified as ≥90%, 70–89%, ≥50–69%, and <50% of the prescribed dose. Continued poor compliance (<50%) may result in study withdrawal.
Target sample size and statistical analysis plan
Based on two prior vonoprazan clinical studies (NCT01456260 and MCT01456247), a sample size of 130 participants in the vonoprazan group and 65 participants in the lansoprazole group has been proposed (2:1 allocation). It is estimated that this will allow data collection from 100, 50, and 30 participants in the first, third, and fifth years, respectively. The safety populations in the healing and maintenance phases are defined as participants who receive at least one dose of the study or control drug in the healing and maintenance phases, respectively. The full analysis set (FAS) are defined as participants who are randomized and receive at least one dose of the study or control drug in the healing and maintenance phases, respectively. The FAS healing and maintenance populations will be used to assess the secondary endpoints of EE healing rate at the end of the healing phase and endoscopic EE recurrence rate, respectively, and will be calculated using point estimate and a two-sided 95% confidence interval. The safety maintenance population will be used to assess primary and secondary endpoints, gastric mucosa histopathology and endoscopic findings, with histological evaluation as per Sydney classification,19 respectively, by calculating the proportion of participants with an event; the incidence of gastric polyp (secondary endpoint) will also be calculated. AEs in the safety maintenance population will by coded using MedDRA terminology.
Trial status
Patient recruitment started in March 2016 and is now completed. Estimated study completion date is February 2022.
Discussion
The VISION study is being undertaken to compare the long-term efficacy and safety of vonoprazan with the PPI lansoprazole in Japanese populations. As the incidence of EE is increasing in Japanese populations,5,6 additional studies are required to understand the long-term safety of the drugs used to treat this condition. Therefore, doses of both vonoprazan and lansoprazole used in the study are equivalent to those routinely prescribed to promote short-term mucosal healing (vonoprazan 20 mg and lansoprazole 30 mg) in the “healing” phase, and longer-term prevention of acid reflux (vonoprazan 10 mg and lansoprazole 15 mg) in the “maintenance” phase of the protocol.
The primary endpoint of gastric mucosal histopathology was chosen because long-term use of PPIs is associated with increased risk of gastric mucosal hyperplasia,11,12 which can be identified using histopathologic methods. As vonoprazan is more potent than other PPIs, safety concerns regarding long-term acid suppression are, therefore, greater.18
The main strength of the study is the recruitment of patients for an extended period (>5 years). This will permit long-term safety and efficacy of vonoprazan to be assessed in a single cohort of patients. The main limitation of the study is that there is likely to be a reduction in the number of patients from whom data can be collected over the long course of the study. In particular, the invasive nature of the endoscopy required to assess morphology of the gastric mucosa may discourage some patients from long-term participation.
Acknowledgments
This study is funded by Takeda Pharmaceutical Co., Ltd. Takeda Pharmaceutical Co., Ltd has been involved in the planning and design of this study, and has contributed to the development and approval of the present manuscript. The final decision to submit the paper, however, lay directly with the authors. The authors acknowledge all patients who are participating in this study and their families, as well as all staff at all investigational sites. The authors thank Kouji Miyata (Takeda Pharmaceutical Co., Ltd Japan) for critical review of the manuscript and suggestions for improvement. The authors also acknowledge Rachel Moir of FireKite (an Ashfield company, part of UDG Healthcare plc), who provided medical writing assistance during the development of this manuscript, which was funded by Takeda Pharmaceutical Co., Ltd and complied with Good Publication Practice 3 ethical guidelines.
Disclosures
NU received honoraria for lectures from Takeda Pharmaceutical Co., Ltd, Eisai Co., Ltd. and AstraZeneca Co., Ltd. YK received research funding and honoraria for lectures from Takeda Pharmaceutical Co., Ltd. KH received research funding and honoraria for lectures. TY received honoraria for lectures from Takeda Pharmaceutical Co., Ltd. TK is employed by Takeda Pharmaceutical Co., Ltd. The authors report no other conflicts of interest in this work.
References
Iwakiri K, Kinoshita Y, Habu Y, et al. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2015. J Gastroenterol. 2016;51(8):751–767. | ||
Hoshihara Y, Hashimoto M. [Endoscopic classification of reflux esophagitis]. Nihon Rinsho. 2000;58(9):1808–1812. Japanese. | ||
Diamant NE. Pathophysiology of gastroesophageal reflux disease. GI Motility online [serial on the Internet]. May 2006. Available from: http://www.nature.com/gimo/contents/pt1/full/gimo21.html. Accessed January 9, 2017. | ||
Iwakiri K, Kawami N, Sano H, et al. Mechanisms of excessive esophageal acid exposure in patients with reflux esophagitis. Dig Dis Sci. 2009;54(8):1686–1692. | ||
Fujiwara Y, Arakawa T. Epidemiology and clinical characteristics of GERD in the Japanese population. J Gastroenterol. 2009;44(6):518–534. | ||
Sugimoto M, Uotani T, Ichikawa H, Andoh A, Furuta T. Gastroesophageal reflux disease in time covering eradication for all patients infected with Helicobacter pylori in Japan. Digestion. 2016;93(1):24–31. | ||
Mishima I, Adachi K, Arima N, et al. Prevalence of endoscopically negative and positive gastroesophageal reflux disease in the Japanese. Scand J Gastroenterol. 2005;40(9):1005–1009. | ||
Japanese Society of Gastroenterology. Evidence-based Clinical Practice Guidelines for Gastroesophageal Reflux Disease (GERD). Tokyo: Nankodo Co., LTD; 2009. | ||
Dekel R, Morse C, Fass R. The role of proton pump inhibitors in gastro-oesophageal reflux disease. Drugs. 2004;64(3):277–295. | ||
Mee AS, Rowley JL. Rapid symptom relief in reflux oesophagitis: a comparison of lansoprazole and omeprazole. Aliment Pharmacol Ther. 1996;10(5):757–763. | ||
Song H, Zhu J, Lu D. Long-term proton pump inhibitor (PPI) use and the development of gastric pre-malignant lesions. Cochrane Database Syst Rev. 2014;(12):CD010623. | ||
Lundell L, Vieth M, Gibson F, Nagy P, Kahrilas PJ. Systematic review: the effects of long-term proton pump inhibitor use on serum gastrin levels and gastric histology. Aliment Pharmcol Ther. 2015;42(6):649–663. | ||
Shin JM, Inatomi N, Munson K, et al. Characterization of a novel potassium competitive acid blocker of the gastric H,K-ATPase, 1-[5-(2-fluorophenyl)-1-(pyridin-3-ylsulfonyl)-1H-pyrrol-3-yl]-N-methylmethanamine monofumarate (TAK-438). J Pharmacol Exp Ther. 2011;339(2):412–420. | ||
Garnock-Jones KP. Vonoprazan: first global approval. Drugs. 2015;75(4):439–443. | ||
Hori Y, Imanishi A, Matsukawa J, et al. 1-[5-(2-fluorophenyl)-1-(pyridin-3-ylsulfonyl)-1H-pyrrol-3-yl]-N-methylmethanamine monofumarate (TAK-438), a novel and potent potassium-competitive acid blocker for the treatment of acid-related diseases. J Pharmacol Exp Ther. 2010;335(1):231–238. | ||
Matsukawa J, Hori Y, Nishida H, Kajino M, Inatomi N. A comparative study on the modes of action of TAK-438, a novel potassium-competitive acid blocker, and lansoprazole in primary cultured rabbit gastric glands. Biochem Pharmacol. 2011;81(9):1145–1151. | ||
Ashida K, Sakurai Y, Hori T, et al. Randomised clinical trial: vonoprazan, a novel potassium-competitive acid blocker, vs. lansoprazole for the healing of erosive oesophagitis. Aliment Pharmacol Ther. 2016;43(2):240–251. | ||
Sakurai Y, Mori Y, Okamoto H, et al. Acid-inhibitory effect of vonoprazan 20 mg compared with esomeprazole 20 mg or rabeprazole 10 mg in healthy adult male subjects – a randomised open-label cross-over study. Aliment Pharmacol Ther. 2015:42(6):719–730. | ||
Armstrong D, Bennett JR, Blum AL, et al. The endoscopic assessment of esophagitis: a progress report on observer agreement. Gastroenterology. 1996;111(1):85–92. | ||
Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis: The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol. 1996;20(10):1161–1181. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.