")
Back to Journals » International Journal of General Medicine » Volume 15
Rationale and Design of LAPIS: A Multicenter Prospective Cohort Study to Investigate the Efficacy and Safety of Low-Dose Aspirin in Elderly Chinese Patients
Authors Wang X , Chen X, Liu W, Liang W , Liu M
Received 3 October 2022
Accepted for publication 17 November 2022
Published 24 November 2022 Volume 2022:15 Pages 8333—8341
DOI https://doi.org/10.2147/IJGM.S391259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiting Wang, Xiahuan Chen, Wenwen Liu, Wenyi Liang, Meilin Liu
Department of Geriatrics, Peking University First Hospital, Beijing, People’s Republic of China
Correspondence: Meilin Liu, Department of Geriatrics, Peking University First Hospital, Beijing, People’s Republic of China, Email [email protected]
Purpose: Although aspirin can effectively reduce the occurrence of atherothrombosis, it is significantly associated with increased bleeding, with elderly individuals being at increased risk of cardiovascular diseases(CVDs) and hemorrhage. While the adverse effects of aspirin can be reduced by using the lowest effective dose, its optimal dose remains undetermined in the elderly Chinese population with both higher cardiovascular and bleeding risks. This study aims to assess the current status of aspirin therapy in real-world clinical settings as well as investigate the efficacy and safety of different doses of aspirin intake (≤ 50 mg/d and > 50 mg/d) for CVD prevention and management in elderly Chinese individuals.
Patients and Methods: The Low-dose Aspirin for Primary and Secondary Prevention of Cardiovascular Disease in the Elderly Study (LAPIS) is a multicenter, prospective, observational cohort study. At least 10,000 people aged ≥ 60 years who require long-term aspirin therapy will be recruited. The effectiveness outcome is a composite of major cardiovascular events(MACEs), including nonfatal myocardial infarction, unstable angina, arteriosclerotic disease requiring surgery or intervention, nonfatal stroke, transient ischemic attack, or cardiovascular death (excluding intracranial hemorrhage). The safety outcome is a composite of the first occurrence of fatal bleeding, major bleeding and minor bleeding. Information on the incidence of aspirin-associated gastrointestinal adverse events will also be collected for safety analyses. Outcome measurements will be performed at intervals of 30 days, 3 months, 6 months and then every 6 months for the next 3 years.
Conclusion: The results of the LAPIS study will ascertain the efficacy and safety of different doses of aspirin for the prevention and management of CVD, thereby providing evidence to determine the optimal evidence-based dose of aspirin therapy in Chinese elderly individuals.
Trial Registration: ChiCTR1900021980 (chictr.org.cn). Registered on March 19, 2019.
Keywords: low-dose aspirin, effectiveness outcome, safety outcome, Chinese elderly
Introduction
Cardiovascular disease (CVD) is the leading cause of disability and death in the elderly population. This condition has become a growing public health concern in China, with CVD prevention as a top priority. Although aspirin reduces the occurrence of atherothrombosis,1,2 and is considered an established agent for the chemoprevention of colorectal cancer(CRC),3–5 this medication is associated with a high risk of bleeding.6 Low-dose aspirin has been shown to be effective in the secondary prevention of CVD, with cardiovascular benefits outweighing the risk of hemorrhage.1,7 However, the role of aspirin in primary prevention trials of patients whose CVD risk is lower than that in secondary prevention trials remains debatable. Moreover, the US Preventive Services Task Force (USPSTF)8 recommends against initiating aspirin at 75–100 mg/d for the primary prevention of CVD in adults aged ≥ 60 years. Since the risk of atherothrombosis is higher in the elderly population, the potential benefits of aspirin may be greater in these subjects than in younger adults. Therefore, the limited use of aspirin may indiscriminately reduce its net benefit, particularly in patients with a high 10-year risk of myocardial infarction or stroke. Moreover, an increased risk of bleeding has been observed in elderly individuals,9,10 particularly in elderly Chinese individuals with lower body weights and Helicobacter pylori infection,11 which leads to the discontinuation of aspirin therapy. Therefore, before prescribing aspirin, the balance between cardiovascular benefits and potential risk of hemorrhage should be considered.
Aspirin dose is reportedly associated with a risk of bleeding.12 Currently, the recommended dose of aspirin for the primary and secondary prevention of CVD is 75–100 mg/d based on clinical guidelines, aspirin 50 mg/d is only recommended for preventing stroke and other cardiovascular events for patients with noncardiogenic transient ischemic attacks(TIA) or ischemic stroke,13 and evidence of lower doses of aspirin for the primary and secondary prevention of CVD is lacking. Nevertheless, owing to the risk of bleeding in elderly individuals, physicians in real-world clinical practice prescribe a lower dose of aspirin than the recommended dose. Some studies conducted by our team focused on the difference in outcomes between the recommended aspirin doses and lower doses(≤ 50 mg/d) in elderly Chinese individuals. An observational, retrospective study showed that aspirin at a dose of 40 mg/d could significantly inhibit platelet aggregation and reduce the risk of bleeding and other adverse reactions in patients with very advanced ages.14 A multicenter, randomized controlled trial showed that aspirin at 50 mg/d and 100 mg/d in elderly individuals had similar antiplatelet aggregation effects and good short-term safety profiles.15 Moreover, a single-center interim analysis of a multicenter, prospective, observational cohort study indicated that 50 mg/d aspirin may be preferred to balance the safety and effectiveness in Chinese individuals over 60 years of age who need long-term aspirin for the prevention and management of CVD.16 However, evidence from the elderly Chinese population is still lacking, and the effective and safe dose of aspirin in the elderly remains unknown.
In these contexts, we will carry out this multicenter, prospective, observational cohort study to assess the current situation of aspirin therapy in real-world clinical settings as well as investigate the efficacy and safety of different doses of aspirin intake (≤ 50 mg/d and > 50 mg/d) for CVD prevention and management in Chinese individuals over 60 years of age.
Materials and Methods
Study Objectives and Hypothesis
The main objective of this study was to assess the current situation of aspirin therapy in real-world clinical settings and to investigate the efficacy and safety of different doses of aspirin intake (≤ 50 mg/d and > 50 mg/d) for CVD prevention and management in elderly Chinese individuals. We hypothesize that a lower dose of aspirin(≤ 50 mg/d) in Chinese individuals over 60 years of age will lead to similar cardiovascular benefits but fewer bleeding events than the recommended dose of aspirin (> 50 mg/d).
Study Design
Low-dose aspirin for primary and secondary prevention of CVD in the elderly study (LAPIS; chictr.org.cn, ChiCTR1900021980) is a multicenter, prospective, observational cohort study. Participants are being recruited from 50 to 100 centers across China. Enrollment began in April 2019, and the study will be completed in 2024. The LAPIS procedures do not interfere with aspirin therapy given to the patients, and the dosage and treatment duration of aspirin are decided by the treating physician. The combined use of antiplatelet drugs (such as clopidogrel, ticagrelor, and cilostazol) or anticoagulant drugs (such as warfarin, dabigatran, rivaroxaban, and edoxaban) will not be altered at the discretion of the clinicians and documented in the case report form (CRF). The observation period was defined as the time between enrollment and the final visit for general examination (at least 3 years for each participant). Participants will be followed up on the 30th day, 3rd and 6th months, and then every 6 months (at least 9 times) until the end of the LAPIS study. Outpatient/inpatient face-to-face or phone/WeChat visits will be used for follow-up visits. At each visit, an independent group of physicians will carefully examine and verify all events. Information about the continuation or temporary interruption of aspirin, laboratory tests, concomitant medications, and detailed information about major cardiovascular events (MACEs), bleeding, and gastrointestinal events will be recorded. If a patient withdraws or is lost to follow-up, observation will be terminated, and the date and reason will be recorded. A flow chart of the study is shown in Figure 1. The study visit schedules and assessments are shown in Table 1.
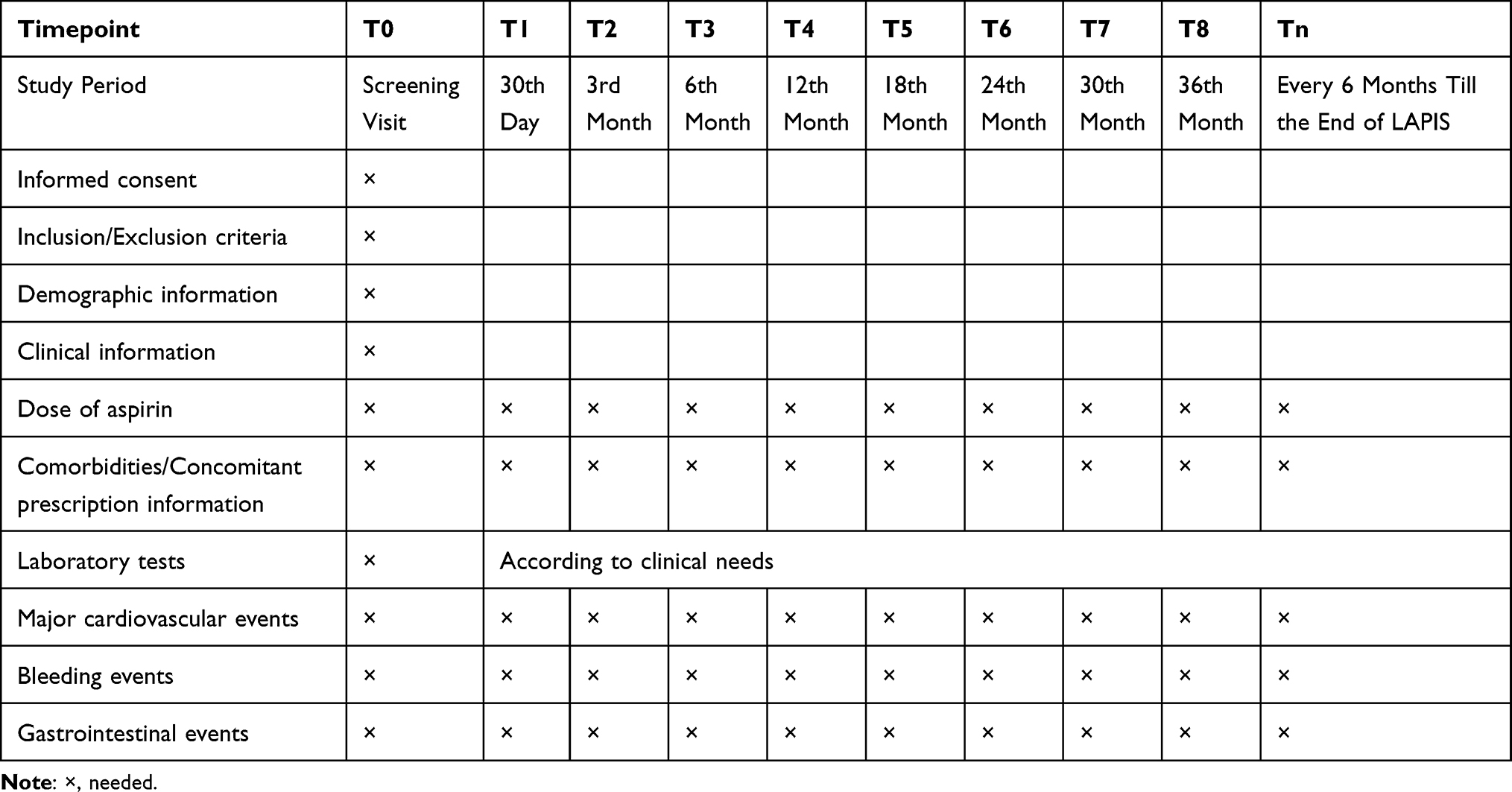 |
Table 1 Schedule of Enrollment, Follow-Up, and Assessments for LAPIS |
 |
Figure 1 Flow chart of the LAPIS study. |
Study Population
Participants aged ≥ 60 years who require long-term aspirin for the primary and secondary prevention of CVD and can provide routine laboratory test results for the past 3 months will be recruited. Participants will be excluded from the study if they meet any of the following conditions: (1) allergy to aspirin, salicylate, or any other ingredients of aspirin; (2) a history of asthma caused by salicylate, salicylate substances, or nonsteroidal anti-inflammatory drugs; (3) life expectancy ≤ 3 years; and (4) refusal to provide written informed consent or difficulty with medication or regular follow-up.
Baseline Data Collection
The baseline data of all participants will be collected after obtaining their informed consent at the initial visit. Demographic information will include age, sex, body weight, smoking history, and alcohol intake. Clinical information will include vital signs, previous history of MACEs (nonfatal myocardial infarction, unstable angina, vascular diseases requiring surgical/interventional revascularization, nonfatal stroke, or transient ischemic attack), hemorrhagic events, gastrointestinal disease, and comorbidities (hypertension, diabetes mellitus, dyslipidemia, or chronic kidney disease). Laboratory tests performed 3 months prior to enrollment included routine blood examination (leukocyte count, hemoglobin, hematocrit, and platelet count), liver function (alanine aminotransferase, aspartate aminotransferase, total bilirubin, direct bilirubin, total bile acid, alkaline phosphatase, gamma-glutamyl transpeptidase), renal function (serum urea nitrogen, uric acid, serum creatinine, and estimated glomerular filtration rate), serum glucose (fasting blood glucose and glycosylated hemoglobin), serum lipids (triglycerides, total cholesterol, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol), and coagulation function evaluation. Prescription information will include the status of aspirin intake and concomitant antithrombotic therapy and other concomitant medications, such as β-blockers, statins, angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), proton pump inhibitors (PPIs), and histamine 2 receptor antagonists (H2RAs). Baseline information will be recorded in detail in the CRF.
Study Outcomes
Effectiveness Outcomes
The primary effectiveness outcome is a composite of the first occurrence of MACEs, including nonfatal myocardial infarction, unstable angina, arteriosclerotic disease requiring surgery or intervention, nonfatal stroke, transient ischemic attack, and cardiovascular death (excluding intracranial hemorrhage). The most important secondary effectiveness outcomes are as follows: (1) composite of the first nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death (excluding intracranial hemorrhage); (2) first occurrence of nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death (excluding intracranial hemorrhage); (3) first occurrence of unstable angina; (4) first occurrence of arteriosclerotic disease requiring surgery or intervention; (5) first occurrence of transient ischemic attack; and (6) all-cause mortality.
Safety Outcomes
The safety outcome is a composite of the first occurrence of fatal bleeding (Bleeding Academic Research Consortium,17 BARC, type 5), major bleeding (BARC, type 3–4), and minor bleeding (BARC type 1–2). For safety analyses, data on the gastrointestinal adverse events associated with aspirin, including new-onset gastroduodenal ulcer, reflux esophagitis, erosive gastritis, stomach or abdominal discomfort, pain, pressure, heartburn, and nausea, will be collected.
Sample Size Calculation
The recommended dose of aspirin for the primary and secondary prevention of CVD is 75–100 mg/d. Although previous studies have shown that short-term use of aspirin at 40–50 mg/d inhibits platelet aggregation,14,15 there is no evidence of long-term use of aspirin ≤ 50 mg/d in elderly Chinese individuals. According to the single-center interim analysis of the Peking University First Hospital from April 2019 to February 2022,16 165 patients receiving aspirin at 50 mg/d and 261 patients receiving aspirin at 100 mg/d were enrolled in the study. After adjusting for patient characteristics using propensity score matching (PSM), the bleeding event rate was 22.81% in the 50 mg/d aspirin group and 34.21% in the 100 mg/d aspirin group, with a median follow-up period of 691 days. A sample size of 570 patients (190 patients in the 50 mg/d aspirin group and 380 patients in the 100 mg/d group) will be sufficient to provide 80% power at a 0.05 two-sided α level of significance for safety assessment. However, since the MACE rates were similar between the 50 mg/d aspirin group (9.65%) and the 100 mg/d aspirin group (9.65%), it is difficult to calculate the sample size with a particular statistical method for efficacy assessment. Given the exploratory nature of this study, a sample size of > 10,000 is considered efficient to determine the safety and efficacy of each dose of aspirin in elderly individuals. The LAPIS research team will analyze the data annually and adjust the sample size accordingly.
Statistical Analysis
Data will be presented as the mean ± standard deviation (SD) or median (interquartile range) for continuous variables and percentage (%) for categorical variables. Normally distributed continuous variables will be compared using independent sample t-tests. A paired t-test or Wilcoxon rank-sum test will be used to compare continuous variables between the two groups, while ANOVA or the Kruskal–Wallis rank-sum test will be used for multigroup comparisons. All categorical variables will be compared using Pearson’s χ2 test or Fisher’s exact test. Subgroup analysis will be performed based on primary prevention and secondary prevention. Patient characteristics will be compared between patients who received > 50 mg/day aspirin and those who received ≤ 50 mg/day aspirin. PSM with a 1:1 ratio will be performed to adjust for patient characteristics and directly compare outcomes between the two groups. The standardized difference will be calculated to compare patient characteristics between the two groups. Kaplan-Meier analysis with Cox proportional hazards regression will be used for time-to-event analysis to determine hazard ratios (HRs) and 95% confidence intervals (CIs). The Log rank test will be conducted for the overall survival curves. Multivariate Cox proportional hazards models will be developed to identify the independent predictors of MACEs and bleeding events after adjusting for the variables that were known to be strongly associated with the risk of MACEs and bleeding events or differed significantly by univariate analysis. All tests will be two-sided with a significance level of 0.05, unless stated otherwise. Statistical analyses will be performed using SPSS Statistics (version 23.0; IBM, Armonk, NY, USA).
Data Management
The data manager will establish an electronic data capture (EDC) system based on eCRF (www.91trial.com). An investigator will enter data from electronic medical records into the EDC system at each site. Supervisors will review the information in the EDC system weekly and conduct a visit every 6 months. The data manager is responsible for designing and managing the EDC system database. At the end of the LAPIS study, the data manager will locate the database.
Ethical Approval and Study Registration
The LAPIS study was approved by the Institutional Ethics Committee of the Peking University First Hospital (approval number 2018[248)]) and will be conducted in accordance with the Declaration of Helsinki. Before patient enrollment, the protocol and consent forms were approved by the institutional review board of each participating center. All participants will provide written informed consent before enrollment in the study.
The study protocol was registered in the Chinese Clinical Trials Registry on March 19, 2019 with the identification code ChiCTR1900021980.
Discussion
CVD is a serious threat to elderly individuals. Approximately 330 million people suffer from CVD in China, accounting for 43.81% of deaths among urban residents and 46.66% among rural residents.18 Platelet activation and aggregation are the primary causes of arterial thrombosis. Aspirin, a platelet aggregation inhibitor, has been shown to play an important role in the primary and secondary prevention of CVD. In addition, aspirin is considered the most established agent for
chemoprevention of CRC with the delayed impact due to remarkably consistent data from previous cohort studies and randomized clinical trials,19–21 it is reported that the effects of aspirin on cancer are not apparent until at least 3 years after the start of use, and some benefits are sustained for several years after cessation in long-term users.22 A pooled analysis also indicated that regular use of aspirin was associated with a lower risk of CRC for individuals who used aspirin before age 70 years and continued into their 70s or later compared with non regular users.23
However, this medication is associated with an increased risk of hemorrhagic events. Aspirin decreases gastric mucosal prostaglandin levels and causes significant gastrointestinal mucosal damage, acid back diffusion and impaired platelet aggregation, further inducing direct epithelial damage.24 It has been reported that gastrointestinal adverse reactions are significantly more common than clinically overt bleeding in individuals on antiplatelet therapy.25–27 Helicobacter pylori infection is a recognized risk factor for gastrointestinal bleeding during low-dose aspirin treatment, and the infection should be eradicated when identified, especially for Chinese individuals due to the higher prevalence.28 Furthermore, the risk of bleeding increases when aspirin is combined with other antiplatelets and anticoagulants.29,30 The benefit of low-dose aspirin at 75–100 mg/day in the secondary prevention of CVD is well established, while the role of low-dose aspirin in primary prevention is still being debated. The JPPP,31 ARRIVE,32 ASCEND,33 and ASPREE34 clinical trials, as well as a previous meta-analysis,35 have shown inconsistent cardiovascular outcomes with potential benefits offset by increased bleeding risk, and the ASPREE trial found aspirin use to be associated with an increased risk of CRC mortality in older adults at 4.7 years of follow-up.34 Older adults are at a higher risk for both atherosclerotic thrombosis and bleeding, and the bleeding risk associated with aspirin has been shown to increase with age and aspirin dose.22 Some post hoc analyses of randomized controlled trials and observational studies have indicated that the adverse effects of aspirin therapy can be minimized by administering a lower dose,36 which also improves long-term adherence.37
Previous studies have explored the relationship between body weight and the antiplatelet effects of aspirin.38,39 These results suggest an association between body weight and aspirin dosage: low-dose aspirin (75–100 mg/d) is only effective in preventing vascular events in patients weighing less than 70 kg,40 and patients weighing < 60 kg are more likely to experience bleeding events.41,42 In addition, aspirin-mediated reductions in the long-term risk of CRC are also weight dependent, and it has been reported that aspirin 75–100 mg/d reduces the risk of CRC in participants weighing less than 70 kg but not in people weighing 70 kg or more.40 Therefore, a one-dose-for-all approach to aspirin use in elderly individuals is unlikely to be optimal and an individualized therapeutic strategy is warranted. In clinical practice, most physicians are reluctant to prescribe standard-dose aspirin to elderly patients because of the increased risk of bleeding, particularly in patients who are taking other antithrombotic medications. Few studies have focused on the difference in outcomes between the recommended aspirin doses and lower doses(≤ 50 mg/d) in elderly Chinese individuals, and the effective and safe dose of aspirin in elderly individuals remains unknown. Therefore, additional data from large-scale clinical studies should be collected and analyzed in elderly populations with higher comorbidities, polypharmacy, lower body weight, and frailty.
To the best of our knowledge, the LAPIS study will be the first large-scale multicenter prospective observational cohort study to evaluate the efficacy and safety of different doses of aspirin for the primary and secondary prevention of CVD in elderly Chinese individuals. At least 10,000 participants ≥ 60 years of age will be enrolled in the study to provide important information about aspirin treatment in the Chinese elderly population in a real-world clinical setting. We will compare the cardiovascular benefits, bleeding, and gastrointestinal adverse effects of aspirin ≤ 50 mg/d vs aspirin > 50 mg/d in elderly Chinese individuals, particularly in those with a high risk of bleeding or concomitant antithrombotic therapy.
The LAPIS study will help determine the optimal dose of aspirin for elderly Chinese individuals. The first participant was enrolled in the LAPIS study on April 1st, 2019. As of the date of manuscript submission, 6769 patients have been enrolled from 77 medical centers in 11 Chinese provinces. The study is expected to continue for 5 years, with the final participant visit scheduled for 2024. We look forward to the LAPIS study, which will provide useful information for the overall management of CVD in older adults.
Conclusions
Low-dose aspirin for primary and secondary prevention of CVD in the elderly study (LAPIS) is a multicenter, prospective, observational cohort study that aims to assess the current status of aspirin therapy in real-world clinical settings as well as investigate the efficacy and safety of different doses of aspirin intake (≤ 50 mg/d and > 50 mg/d) for CVD prevention and management in elderly Chinese individuals. It is expected that the results of this study will provide evidence to determine the optimal evidence-based dose of aspirin therapy in Chinese elderly individuals.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We wish to thank the LAPIS Investigators including (1) Beijing: Yingxin Zhao, Beijing Anzhen Hospital Capital Medical University; Mingzhao Qin, Beijing Tongren Hospital Capital Medical University; (2) Tianjin: Hongliang Cong, Tianjin Chest Hospital; Zhuhua Yao, Tianjin People’s Hospital; Yong Liu, Tianjin Fourth Center Hospital; Yingwu Liu, Tianjin Third Central Hospital; (3) Zhejiang: Yunmei Yang, The First Affiliated Hospital, Zhejiang University; Shudong Xia, The Fourth Affiliated Hospital, Zhejiang University; (4) Jiangsu: Yunxia Meng, The First People’s Hospital of Lianyungang; Huaizhong Zhang, Xuzhou Cancer Hospital; (5) Shandong: Xiqiang Liu, Zibo Central Hospital; Xin Zhuge, LinYi Luozhuang Central Hospital; Pida Hao, LinYi Luozhuang People’s Hospital; Yan Hou, Zhangdian People’s Hospital; Huafeng Wei, No.7 & Orthopeadic Hospital; Keshan Liang, The People’s Hospital of Pingyi County; Zhengxiang Zhang, The Fourth People Hospital of Zibo; Peng Dou, Zibo Guangdian Hospital; Lili Wang, Zibo Shengjie Hospital; Hongwei Li, PKUCare Luzhong Hospital; Bo Liu, Shandong Yiyangjiankang Jituan Zibo Hospital; Zhangyong Xia, Liaocheng Brian Hospital; Xiulian Yan, Zibo Gaoqing Hospital; Tao Tian, Linyi People’s Hospital; ZhengHua Zhang, The Sixth People’s Hospital of Zibo; Jianchun Wang, Shandong Provincial Hospital; (6) Neimenggu: Hong Qi, The Affiliated Hospital of Chifeng University; Shichao Liu, Hailar People’s Hospital; Yanchun Li, Hailar People’s Hospital; Yanmei Sun, Chifeng Songshan Hospital; Lili Liu, Xing’anmeng People’s Hospital; Jiuyu Yang, The Second Affiliated Hospital, Inner Mongolia Minzu University; Henabuqi, Xing’anmeng Mongolian Hospital;; (7) Jiangxi: Mengjue Lei, The Jiangxi Provincial People’s Hospital; Jie Hu, The Jiangxi Provincial People’s Hospital; (8) Shanxi: Xiaoping Chen, Taiyuan Central Hospital; (9) Shaanxi: Aiping Jin, The Second Affiliated Hospital of Xi’an Jiaotong University(Xibei Hospital); (10) Hubei: Zhaohui Wang, Union Hospital Tongji Medical College Huazhong University of Science and Technology; Ping He, Union Hospital Tongji Medical College Huazhong University of Science and Technology; and (11) Anhui: Mingcai Huang, The People’s Hospital of Dongzhi County. We would also like to acknowledge the participants and their families who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The low-dose aspirin for primary and secondary prevention of cardiovascular disease in the elderly study (LAPIS) was sponsored by Shandong Xinhua Pharmaceutical Group Co. LTD, China and Project 2019BD019 was supported by the PKUBaidu Fund. The funders of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baigent C, Blackwell L, Blackwell L., et al.; Antithrombotic Trialists’ (ATT) Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849–1860. doi:10.1016/S0140-6736(09)60503-1
2. Casado-Arroyo R, Bayrak F, Sarkozy A, et al. Role of ASA in the primary and secondary prevention of cardiovascular events. Best Pract Res Clin Gastroenterol. 2012;26(2):113–123. doi:10.1016/j.bpg.2012.01.013
3. Drew DA, Cao Y, Chan AT. Aspirin and colorectal cancer: the promise of precision chemoprevention. Nat Rev Cancer. 2016;16(3):173–186. doi:10.1038/nrc.2016.4
4. Chapelle N, Martel M, Toes-Zoutendijk E, et al. Recent advances in clinical practice: colorectal cancer chemoprevention in the average-risk population. Gut. 2020;69(12):2244–2255. doi:10.1136/gutjnl-2020-320990
5. Drew DA, Chan AT. Aspirin in the prevention of colorectal neoplasia. Annu Rev Med. 2020;1:72.
6. Capodanno D, Angiolillo DJ. Aspirin for primary cardiovascular risk prevention and beyond in diabetes mellitus. Circulation. 2016;134(20):1579–1594. doi:10.1161/CIRCULATIONAHA.116.023164
7. Gorelick PB, Weisman SM. Risk of hemorrhagic stroke with aspirin use: an update. Stroke. 2005;36(8):1801–1807. doi:10.1161/01.STR.0000174189.81153.85
8. Davidson KW, Barry MJ, Mangione CM, et al.; US Preventive Services Task Force. Aspirin use to prevent cardiovascular disease: US Preventive Services Task Force recommendation statement. JAMA. 2022;327(16):1577–1584. doi:10.1001/jama.2022.5207
9. Andreotti F, Rocca B, Husted S, et al. Antithrombotic therapy in the elderly: expert position paper of the European Society of Cardiology Working Group on Thrombosis. Eur Heart J. 2015;36(46):3238–3249. doi:10.1093/eurheartj/ehv304
10. Li L, Geraghty OC, Mehta Z, et al. Age-specific risks, severity, time course, and outcome of bleeding on long-term antiplatelet treatment after vascular events: a population-based cohort study. Lancet. 2017;390(10093):490–499. doi:10.1016/S0140-6736(17)30770-5
11. Editorial Board of Chinese Journal of Cardiovascular Disease (Online edition). Expert consensus on prevention and treatment of digestive tract injury associated with oral antithrombotic drugs. Chin J Cardiovasc Dis. 2021;4:e1000081.
12. Serebruany VL, Steinhubl SR, Berger PB, et al. Analysis of risk of bleeding complications after different doses of aspirin in 192,036 patients enrolled in 31 randomized controlled trials. Am J Cardiol. 2005;95(10):1218–1222. doi:10.1016/j.amjcard.2005.01.049
13. Chinese Society of Neurology, Chinese Stroke Society. Chinese guideline for the secondary prevention of ischemic stroke and transient ischemic attack 2022. Chin J Neurol. 2022;55(10):1071–1110.
14. Feng XR, Liu ML, Liu F, et al. Dose-response of aspirin on platelet function in very elderly patients. Beijing Da Xue Xue Bao Yi Xue Ban. 2016;48(5):835–840.
15. Chen XH, Liu ML, Qin MF, et al. Anti-aggregation effect and short-term safety evaluation of low-dose aspirin therapy in the elderly Chinese population: a multicenter randomized controlled clinical trial. Chin Circ J. 2018;33(5):457–462.
16. Wang X, Wang H, Zheng Q, et al. Outcomes Associated with 50 mg/d and 100 mg/d Aspirin for the Prevention and Management of Cardiovascular Disease in Chinese Elderly: single-Center Interim Analysis of a Multicenter, Prospective, Observational Study. Int J Gen Med. 2022;6(15):7089–7100. doi:10.2147/IJGM.S384375
17. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the bleeding academic research consortium. Circulation. 2011;123:2736–2747. doi:10.1161/CIRCULATIONAHA.110.009449
18. The Writing Committee of the report on cardiovascular health and diseases in China. Report on cardiovascular health and diseases burden in China: an updated summary of 2020. Chin Circ J. 2021;36:521–545.
19. Flossmann E, Rothwell PM, British Doctors Aspirin Trial and the UK-TIA Aspirin Trial. Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet. 2007;369(9573):1603–1613. doi:10.1016/S0140-6736(07)60747-8
20. Rothwell PM, Wilson M, Elwin CE, et al. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet. 2010;376(9754):1741–1750. doi:10.1016/S0140-6736(10)61543-7
21. Burn J, Sheth H, Elliott F, et al.; CAPP2 Investigators. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: a double-blind, randomised, placebo-controlled trial. Lancet. 2020;395(10240). doi:10.1016/S0140-6736(20)30366-4
22. Cuzick J, Thorat MA, Bosetti C, et al. Estimates of benefits and harms of prophylactic use of aspirin in the general population. Ann Oncol. 2015;26(1):47–57. doi:10.1093/annonc/mdu225
23. Guo CG, Ma W, Drew DA, et al. Aspirin use and risk of colorectal cancer among older adults. JAMA Oncol. 2021;7(3):428–435. doi:10.1001/jamaoncol.2020.7338
24. Iwamoto J, Saito Y, Honda A, et al. Clinical features of gastroduodenal injury associated with long-term low-dose aspirin therapy. World J Gastroenterol. 2013;19:1673–1682. doi:10.3748/wjg.v19.i11.1673
25. Goldstein JL, Scheiman JM, Fort JG, et al. Aspirin use in secondary cardiovascular protection and the development of aspirin-associated erosions and ulcers. J Cardiovasc Pharmacol. 2016;68(2):121–126. doi:10.1097/FJC.0000000000000387
26. Tang C, Zhu Y, Yang X, et al. Upper gastrointestinal mucosal injury associated with ticagrelor plus aspirin, ticagrelor alone, or aspirin alone at 1-year after coronary artery bypass grafting. J Gastroenterol Hepatol. 2020;35(10):1720–1730. doi:10.1111/jgh.15030
27. Han Y, Liao Z, Li Y, et al. Magnetically controlled capsule endoscopy for assessment of antiplatelet therapy-induced gastrointestinal injury. J Am Coll Cardiol. 2022;79:116–128. doi:10.1016/j.jacc.2021.10.028
28. Chey WD, Leontiadis GI, Howden CW, et al. ACG Clinical Guideline: treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017;112(2):212–239. doi:10.1038/ajg.2016.563
29. Helton TJ, Bavry AA, Kumbhani DJ, et al. Incremental effect of clopidogrel on important outcomes in patients with cardiovascular disease: a meta-analysis of randomized trials. Am J Cardiovasc Drugs. 2007;7:289–297. doi:10.2165/00129784-200707040-00006
30. Eikelboom JW, Connolly SJ, Bosch J, et al.; COMPASS Investigators. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N Engl J Med. 2017;377:1319–1330. doi:10.1056/NEJMoa1709118
31. Ikeda Y, Shimada K, Teramoto T, et al. Low-dose aspirin for primary prevention of cardiovascular events in Japanese patients 60 years or older with atherosclerotic risk factors: a randomized clinical trial. JAMA. 2014;312(23):2510–2520. doi:10.1001/jama.2014.15690
32. Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. 2018;392(10152):1036–1046. doi:10.1016/S0140-6736(18)31924-X
33. Bowman L, Mafham M; ASCEND Study Collaborative Group. Effects of aspirin for primary prevention in persons with diabetes mellitus. N Engl J Med. 2018;379(16):1529–1539.
34. McNeil JJ, Wolfe R, Woods RL, et al. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly. N Engl J Med. 2018;379(16):1509–1518. doi:10.1056/NEJMoa1805819
35. Zheng SL, Roddick AJ. Association of aspirin use for primary prevention with cardiovascular events and bleeding events: a systematic review and meta-analysis. JAMA. 2019;321(3):277–287. doi:10.1001/jama.2018.20578
36. Huang ES, Strate LL, Ho WW, et al. Long-term use of aspirin and the risk of gastrointestinal bleeding. Am J Med. 2011;124(5):426–433. doi:10.1016/j.amjmed.2010.12.022
37. Jones WS, Mulder H, Wruck LM, et al. Comparative effectiveness of aspirin dosing in cardiovascular disease. N Engl J Med. 2021;384(21):1981–1990. doi:10.1056/NEJMoa2102137
38. Furtado RHM, Giugliano RP, Dalcoquio TF, et al. Increased bodyweight and inadequate response to aspirin in individuals with coronary artery disease. J Thromb Thrombolysis. 2019;48(2):217–224. doi:10.1007/s11239-019-01830-z
39. Mourikis P, Zako S, Dannenberg L, et al. Aspirin antiplatelet effects are associated with body weight. Vasc Pharmacol. 2020;125-126:106635. doi:10.1016/j.vph.2019.106635
40. Rothwell PM, Cook NR, Gaziano JM, et al. Effects of aspirin on risks of vascular events and cancer according to bodyweight and dose: analysis of individual patient data from randomised trials. Lancet. 2018;392(10145):387–399. doi:10.1016/S0140-6736(18)31133-4
41. McCall M, Peace A, Tedesco AF, et al. Weight as an assay-independent predictor of poor response to enteric aspirin in cardiovascular patients. Platelets. 2020;31(4):530–535. doi:10.1080/09537104.2019.1667495
42. Wang X, Zhu Q, Wu Y, et al. Effect of body weight on bleeding events of aspirin in ischemic stroke or transient ischemic attack patients. J Clin Pharm Ther. 2022;47(10):1684–1689. doi:10.1111/jcpt.13722
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.