")
Back to Journals » Pragmatic and Observational Research » Volume 11
Rate of Significant Endometrial Pathology in Women at Low Risk for Endometrial Hyperplasia or Cancer Presenting with Abnormal Uterine Bleeding
Authors Sattanakho P, Kleebkaow P , Sangkomkumhang U, Booranabunyat S, Buppasiri P
Received 4 December 2019
Accepted for publication 17 January 2020
Published 11 February 2020 Volume 2020:11 Pages 13—18
DOI https://doi.org/10.2147/POR.S240930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor David Price
Pattarawadee Sattanakho,1 Pilaiwan Kleebkaow,1 Ussanee Sangkomkumhang,2 Sukjai Booranabunyat,3 Pranom Buppasiri1
1Department of Obstetrics and Gynaecology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Department of Obstetrics and Gynecology, Khon Kaen Regional Hospital, Khon Kaen, Khon Kaen Province, Thailand; 3Department of Obstetrics and Gynecology, Mahasarakham Hospital, Mahasarakham Province, Thailand
Correspondence: Pranom Buppasiri
Department of Obstetrics and Gynaecology, Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand
Tel +66-43-202489
Fax +66-43-348395
Email [email protected]
Background and Objectives: To determine the rate of significant endometrial abnormalities in premenopausal women at low risk for endometrial hyperplasia and cancer presenting with abnormal uterine bleeding (AUB).
Patients and Methods: This descriptive study was conducted from January 1, 2016 to March 31, 2019. The inclusion criteria were premenopausal women, 35– 50 years, presenting with AUB, low risk for endometrial hyperplasia or endometrial cancer, and having undergone endometrial sampling or uterine curettage. Nulliparous, obesity, diabetes mellitus, polycystic ovary syndrome, chronic anovulation, infertility, tamoxifen therapy and/or a family history of uterine, ovarian, breast and colon cancer were excluded. Data regarding baseline characteristics were collected, and histopathology reports were reviewed.
Results: During the study period, 644 subjects were recruited, 557 of whom had adequate endometrial tissue for histopathology study. The pathology demonstrated benign in most cases (96%). The rate of significant abnormal endometrial pathology was 4% (23 cases) including 19 cases of endometrial hyperplasia without atypia (3.3%), and 4 cases of endometrial cancer (0.7%).
Conclusion: The rate of significant abnormal endometrial pathology in premenopausal women at low risk for endometrial hyperplasia or endometrial cancer presenting with AUB was very low. This information should be incorporated into the counseling process regarding the risks and benefits of endometrial sampling.
Keywords: abnormal uterine bleeding, endometrial sampling, endometrial pathology
Introduction
Abnormal uterine bleeding (AUB) is defined as a bleeding pattern that differs in frequency, duration, and amount from that observed during a normal menstrual cycle.1 Abnormal uterine bleeding is one of the most common complaints encountered in gynecological out-patient clinic. According to the International Federation of Gynecology and Obstetrics (FIGO) classification system, the causes of AUB during a woman’s reproductive years including endometrial polyp, adenomyosis, leiomyoma, malignancy and hyperplasia, coagulopathy, ovulatory dysfunction, endometrial pathology, iatrogenic cause, and those causes not yet classified (PALM-COEIN).2 The most serious cause is a malignancy. The known risk factors for endometrial carcinoma are chronic unopposed estrogen, late menopause, obesity, nulliparous, polycystic ovary syndrome, diabetes mellitus, and Lynch syndrome.3,4 Although endometrial cancer occurs primarily in postmenopausal women, up to 14% of those afflicted are premenopausal, 4.5% of whom are under 40 years old.5 There are various methods used to access endometrial tissue such as endometrial sampling, dilatation and curettage, fractional curettage or hysteroscopy and direct biopsy. Endometrial sampling and dilatation and curettage (D&C) have shown nearly equal accuracy in the diagnosis of endometrial pathology and had good consistency with the histopathology diagnoses of hysterectomized specimens.6,7
Endometrial sampling is recommended in women with postmenopausal bleeding but evidence is inconclusive whether or not the procedure should be performed in premenopausal women.1,8 Some studies suggest that endometrial sampling should be performed in women older than 35 years old with AUB.5,9 However, the Society of Obstetricians and Gynecologists of Canada (SOGC) suggests that the procedure should be conducted in women aged over 40 years old or in cases whose bleeding does not respond to medical therapy, and also in younger women with risk factors for endometrial cancer.8 The American College of Obstetricians and Gynecologists (ACOG) recommends performing endometrial sampling in women aged over 45 years old or in younger women with some risk factors such as obesity, polycystic ovary syndrome, failed medical treatment, or persistent bleeding.1
Although endometrial sampling procedure is safe, causes less pain, does not require anesthesia, and can be conducted at the out-patient clinic, the instrument kit is costly (300 Thai baht or 10 USD/piece). In addition, the procedure can induce anxiety and pelvic discomfort and may need to be repeated if the specimens for histopathology study are not adequate. This study aimed to investigate endometrial pathology in premenopausal women who were at low risk for endometrial hyperplasia and endometrial carcinoma presenting with AUB.
Patients and Methods
Patient Population and Inclusion Criteria
This descriptive study was conducted at 3 hospitals at Khon Kaen Province, Thailand (one university, one regional, and one provincial hospital) from January 1, 2016 to March 31, 2019. Prior approval was obtained from the Khon Kaen University Ethics Committee for Human Research (HE 611055). We included premenopausal women presenting with AUB, aged 35–50 years, and at low risk for endometrial hyperplasia or endometrial cancer. Women with BMI > 30 kg/m2; nulliparous; chronic anovulation or polycystic ovary syndrome; diabetic mellitus; hypertension; tamoxifen use or family history of uterine, ovarian, breast, or colon cancer were excluded. After complete history taking, having physical and pelvic examination; written informed consent was obtained from all participants prior to undergoing endometrial sampling by the gynecologic residents or staff at the Gynecology Out Patient Clinic. A commercial endometrial sampling kit (Endocell®, Wallach, USA) was used without analgesia. In patients whose endometrial cavity could not be accessed by the sampling kit, dilation and curettage or fractional curettage were performed under anesthesia in the operating room. Since the endometrial sampling kit was not available in provincial and regional hospitals, conventional dilatation and curettage or fractional curettage was the procedure of choice. The following data were collected: age, parity, BMI, bleeding characteristics, pelvic ultrasound report, and histopathology study results.
Significant Endometrial Pathology Definitions
Significant endometrial pathology was defined as endometrial hyperplasia with or without atypia and endometrial carcinoma, while benign diseases were proliferative, secretory, atrophic, basal endometrium, endometrial polyp, and inflammatory conditions. Cases of which there was inadequate endometrial tissue for histopathology study were excluded.
Statistical Methods
A study conducted by Getpook et al in 111 premenopausal Thai women demonstrated a rate of abnormal endometrial pathology of 17.1%.10 The study excluded patients with some risk factors such as nulliparous, diabetes, hypertension, but did not eliminate obese women. We thus assumed a prevalence of 15% for this study. Based on this, in order to achieve a power of 80% and a level of significance of 5%, at least 545 participants were needed. Data were displayed as numbers, percentages, and odds ratios. The Pearson Chi-square test and Fisher’s exact test were used to compare qualitative data as appropriate. Logistic regression analyses were conducted to detect odds ratios in different age groups and BMIs in those subjects with significant abnormal endometrial pathology.
This study was conducted in accordance with the Declaration of Helsinki.
Results
During the study period, 644 women undergoing endometrial sampling (501, 77.8%), fractional curettage or dilatation and curettage (134, 20.8%), and manual vacuum aspiration (MVA; 9, 1.4%) due to AUB were recruited. Baseline characteristics of the participants are shown in Table 1. Half of the participants were 45–50 years old (54.2%). Eighty-seven cases (13.5%) had inadequate endometrial tissue for diagnosis, leaving 557 subjects to be included in the final analysis. The vast majority of cases had benign endometrial pathology (96%). Proliferative and secretory endometrium were the two most common endometrial tissue findings. The rate of significant abnormal endometrial pathology was 4% (23 cases) which composed of endometrial hyperplasia without atypia 3.3% (19 cases), and endometrial cancer 0.7% (4 cases). The histopathology study showed endometrioid adenocarcinoma cell type in all 4 cases. Atypical endometrial hyperplasia was not observed in this study. The distribution of endometrial pathology by age group is shown in Table 2.
 |
Table 1 Baseline Characteristics of Participants (N= 557) |
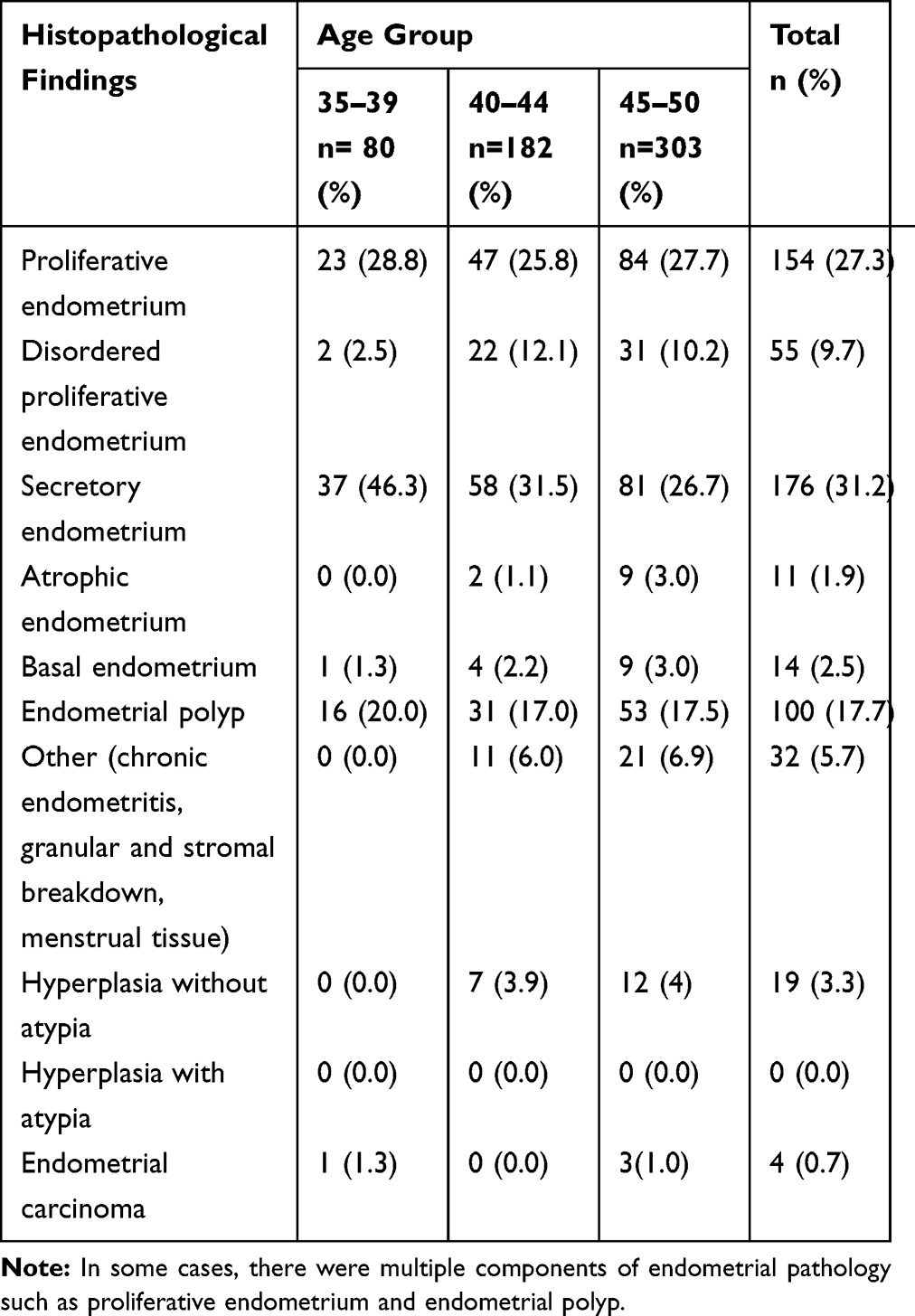 |
Table 2 The Histopathological Findings of Endometrial Study (N= 565) |
The rates of abnormal endometrial pathology were 1.3%, 3.9%, and 5% in patients aged 35–39, 40–44, 45–50 years, respectively. Of the total 23 cases of abnormal endometrial pathology, 65% (15 cases) were in the 45–50 age group. However, the differences between the age groups in this respect were not statistically significant. In low-risk premenopausal women, neither BMI (<30 kg/m2), parity (≥1), bleeding characteristics, nor endometrial thickness was significantly associated with significant endometrial pathology (Table 3).
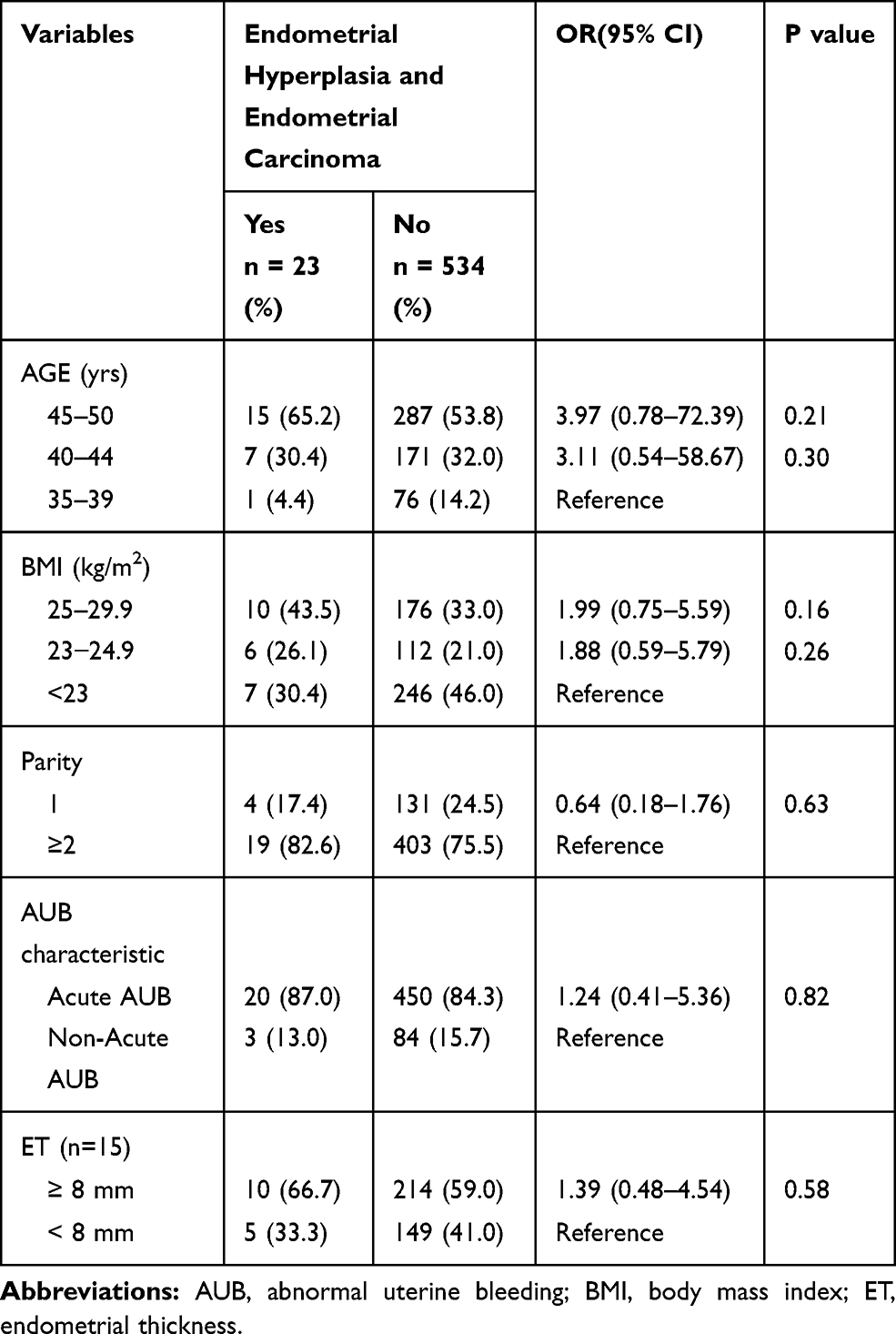 |
Table 3 Factors Associated with Endometrial Hyperplasia and Endometrial Carcinoma (n =23) |
Discussion
Abnormal uterine bleeding commonly occurs in the perimenopausal period, mostly due to decreases in the number of ovarian follicles and increased resistance to gonadotrophic stimulation. Low estrogen production may not be able to maintain normal endometrium. The most common histologic pattern in premenopausal women with AUB in the current study was benign endometrial pathology, the finding was similar to those reported previously.11,12 The rates of endometrial hyperplasia with or without atypia and endometrial cancer in premenopausal women have been reported to vary from 5% to 17% in studies that enlisted approximately 100–3,000 participants regardless of risk factors.3,4,10–13 In the present study, the prevalence of abnormal endometrial pathology was low (4%) because candidates were at low risk for this condition. The most common abnormal endometrial pathology was endometrial hyperplasia without atypia which corresponding to other studies.3,4,11–13
It is known that postmenopausal women are at risk of developing endometrial hyperplasia or cancer, but there are still some conflicting data regarding the age at which premenopausal women should undergo endometrial tissue study.1,8 Some studies have reported no association between age and endometrial hyperplasia or endometrial cancer in premenopausal women.11,14 Esmer et al proposed that each patient should be managed individually depending on the risk factors regardless of age.12 However, Iram et al recommended an age of 45 as the cutoff point at which women should undergo endometrial sampling.4 In this study, although significant abnormal endometrial pathology was most commonly found in the higher age group (45–50 years old), the difference was not statistically significant.
Obesity is a risk factor for endometrial hyperplasia and endometrial cancer due to excessive exposure to estrogen and chronic endometrial stimulation.1,3,14,15 In general, Asian women tend to have lower BMIs than western women. We thus stratified the BMIs of the women in our study based on new BMI for Asian Pacific population (BMI < 23 kg/m2 = normal, 23–24.9 kg/m2 = overweight and ≥25 kg/m2 = obese).16 There was no power to show statistically significant in patients with a BMI below 30 kg/m2. This was in contrast to other studies, which found that patients whose BMI ≥25 kg/m2 had a greater risk of developing endometrial cancer.17,18
Pregnancy is a protective factor for endometrial hyperplasia and cancer due to longer exposure to progesterone hormone.3 However, Giannell et al found no association of endometrial hyperplasia or endometrial cancer with nulliparous.13 In the present study, having had two or more children did not have a significantly greater protective effect than having had only one child. However, the number in this study might be too small to accurately assess this connection.
There is no specific bleeding pattern associated with endometrial hyperplasia or cancer in this study, as these conditions can occur in patients with either heavy menstrual bleeding or intermenstrual bleeding as previous studies.15 However, Pennant et al found that endometrial cancer was more common in women with intermenstrual bleeding than those with heavy menstrual bleeding.19
Unlike postmenopausal women, endometrial sampling is recommended in cases of endometrial thickness more than 4–5 mm, there was no consensus regarding recommendation for endometrial study in premenopausal women with AUB due to the great variation of endometrial thickness during the cycle.20 Endometrial thickness >16 mm has been suggested as being abnormal.20 However, Giannellla et al proposed that endometrial sampling should be carried out in cases when ET is >11 mm.13 Getpook et al found that ET of <8 mm was associated with less malignant pathology.10 Similarly, we found that most patients with significant abnormal endometrial pathology had an ET of >8 mm, but this difference was not statistically significant.
In the light of this study, common endometrial pathology was normal endometrium and benign pathology. This data can be used to counsel low-risk premenopausal women presenting with AUB. Endometrial sampling should be considered in women in whom medical treatment fails or who experience persistent uterine bleeding.
There were several limitations in this study. Firstly, the retrospective nature of the study led to incomplete data collection. Secondly, transvaginal ultrasonography was not performed in all cases, this might be difficult to give the firm conclusion about the correlation between endometrial thickness and disease. Thirdly, there was no record of the date of menstrual cycle on the day of performing endometrial sampling, which might affect endometrial thickness. Lastly, multiple logistic regression was not performed to identify the effects of independent variables for significant abnormal endometrial pathology due to a small number of cases. Thus, a prospective study with a larger sample size should be conducted to confirm the evidence.
Conclusion
The rate of endometrial hyperplasia or cancer in low-risk premenopausal women was very low. This information should be incorporated into the counseling process regarding the risks and benefits of routinely obtaining endometrial tissue for histopathology study.
Acknowledgment
The authors would like to thank Dr. Dylan Southard for his assistance in editing this manuscript.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Committee on Practice Bulletins—Gynecology. Practice bulletin no. 128: diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol. 2012;120:197–206. doi:10.1097/AOG.0b013e318262e320
2. Munro MG, Critchley HOD, Broder MS, et al. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113:3–13. doi:10.1016/j.ijgo.2010.11.011
3. Farquhar CM, Lethaby A, Sowter M, et al. An evaluation of risk factors for endometrial hyperplasia in premenopausal women with abnormal menstrual bleeding. Am J Obstet Gynecol. 1999;181:525–529. doi:10.1016/S0002-9378(99)70487-4
4. Iram S, Musonda P, Ewies AAA. Premenopausal bleeding: when should the endometrium be investigated? A retrospective non-comparative study of 3006 women. Eur J Obstet Gynecol Reprod Biol. 2010;148:86–89. doi:10.1016/j.ejogrb.2009.09.023
5. Duska LR, Garrett A, Rueda BR, et al. Endometrial cancer in women 40 years old or younger. Gynecol Oncol. 2001;83:388–393. doi:10.1006/gyno.2001.6434
6. Demirkiran F, Yavuz E, Erenel H, et al. Which is the best technique for endometrial sampling? Aspiration (pipelle) versus dilatation and curettage (D&C). Arch Gynecol Obstet. 2012;286:1277–1282. doi:10.1007/s00404-012-2438-8
7. Huang GS, Gebb JS, Einstein MH, et al. Accuracy of preoperative endometrial sampling for the detection of high-grade endometrial tumors. Am J Obstet Gynecol. 2007;196:
8. Singh S, Best C, Dunn S, et al. Abnormal uterine bleeding in pre-menopausal women. J Obstet Gynaecol Can. 2013;35:473–475. doi:10.1016/S1701-2163(15)30939-7
9. Singh P. Abnormal uterine bleeding- evaluation by endometrial aspiration. J -Life Health. 2018;9:32–35. doi:10.4103/jmh.JMH_109_17
10. Getpook C, Wattanakumtornkul S. Endometrial thickness screening in premenopausal women with abnormal uterine bleeding. J Obstet Gynaecol Res. 2006;32:588–592. doi:10.1111/jog.2006.32.issue-6
11. Mishra D, Sultan S. FIGO’s PALM-COEIN classification of abnormal uterine bleeding: a clinic-pathological correlation in Indian setting. J Obstet Gynaecol India. 2017;67:119–125. doi:10.1007/s13224-016-0925-8
12. Corbacioglu Esmer A, Akbayir O, Goksedef BPC, et al. Is there an appropriate cutoff age for sampling the endometrium in premenopausal bleeding? Gynecol Obstet Invest. 2014;77:40–44. doi:10.1159/000356959
13. Giannella L, Cerami LB, Setti T, et al. Prediction of endometrial hyperplasia and cancer among premenopausal women with abnormal uterine bleeding. Biomed Res Int. 2019;2019:8598152.
14. Wise MR, Gill P, Lensen S, et al. Body mass index trumps age in decision for endometrial biopsy: cohort study of symptomatic premenopausal women. Am J Obstet Gynecol. 2016;215(598):e1–598.e8. doi:10.1016/j.ajog.2016.06.006
15. Guraslan H, Dogan K, Kaya C, et al. Could body mass index be an indicator for endometrial biopsy in premenopausal women with heavy menstrual bleeding? Arch Gynecol Obstet. 2016;294:395–402. doi:10.1007/s00404-016-4043-8
16. Anuurad E, Shiwaku K, Nogi A, et al. The new BMI criteria for Asians by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workers. J Occup Health. 2003;45:335–343. doi:10.1539/joh.45.335
17. Ghanbari Andarieh M, Agajani Delevar M, Moslemi D, et al. Risk factors for endometrial cancer; results from a hospital-based case-control study. Asian Pac J Cancer Prev. 2016;17:4791–4796. doi:10.22034/apjcp.2016.17.10.4791
18. Wise MR, Jordan V, Legas A, et al. Obesity and endometrial hyperplasia and cancer in premenopausal women. Am J Obstet Gynecol. 2016;214(689):e1–e17. doi:10.1016/j.ajog.2016.01.175
19. Pennant ME, Mehta R, Moody P, et al. Premenopausal abnormal uterine bleeding and risk of endometrial cancer. Int J Obstet Gynaecol. 2017;124:404–411. doi:10.1111/1471-0528.14385
20. Bennett GL, Andreotti RF, Lee SI, et al. ACR appropriateness criteria (®) on abnormal vaginal bleeding. J Am Coll Radio l. 2011;8:460–468. doi:10.1016/j.jacr.2011.03.011
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.