")
Back to Journals » Open Access Journal of Sports Medicine » Volume 5
Rate of injury and subjective benefits of gravitational wellness weightlifting
Authors Burke D, Bell R, Al-Adawi S , Alexandroni A, Dorvlo A, Burke D
Received 14 March 2014
Accepted for publication 1 May 2014
Published 12 September 2014 Volume 2014:5 Pages 215—221
DOI https://doi.org/10.2147/OAJSM.S64078
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
David T Burke,1 Regina Bell,1 Samir Al-Adawi,2 Ariel Alexandroni,1 Atsu Dorvlo,3 Daniel P Burke4
1Emory University School of Medicine, Atlanta, Emory University, GA, USA; 2Department of Behavioral Medicine, College of Medicine and Health Sciences, 3Department of Mathematics and Statistics, College of Science, Sultan Qaboos University, Muscat, Oman; 4Georgia College and State University, Milledgeville, GA, USA
Background: A preliminary study using the "gravitational wellness" weightlifting technique demonstrated this to be a unique technique for loading the musculoskeletal system with extremely high loads over short arcs. This leads to rapid weekly strength gains using 30-minute weekly training sessions. This study was designed to further assess the benefit–risk ratio of the gravitational wellness weightlifting technique.
Purpose: This descriptive/retrospective study examined musculoskeletal and well-being outcomes as well as injuries reported by consecutive participants at one gravitational wellness gym.
Materials and methods: All adults presenting for training at the Atlanta, Georgia, gravitational wellness system facility over a 6-month period were invited to participate. Data were obtained by telephone interview concerning the presenting complaint/objective of training, subjective outcome, weights lifted, and injuries incurred during training.
Results: Of the 77 participants contacted via telephone, 92% agreed to participate (male, n=40; female, n=31). The participants ranged in age from 18 years to 69 years, with a mean age of 48.6 years. Of these, 42 (59%) presented to the gym with the objective of improving a defined musculoskeletal issue. The modal of these was chronic low-back pain. The subjects realized improvement on a 5-point Likert scale of 4.2/5 for their presenting complaint, and improved by 4.27/5 in their overall subjective health. There were no injuries.
Conclusion: This study of consecutive participants at a gravitational wellness gym found that by lifting large weights over short arcs 30 minutes per week, participants significantly increased their strength, reduced their musculoskeletal pain, improve their subjective well-being, and reported a low rate of injury.
Keywords: gravitational wellness system, rate of injuries, weight training, descriptive study
Introduction
According to the Centers for Disease Control and Prevention, almost 36% of US citizens over the age of 20 years are obese.1 To address this issue, interventions have been proposed that target physical activity, nutrition, and lifestyle changes.2,3 That exercise has a direct influence on various health parameters is now well recognized. Some have, in fact, advocated that physical activity be considered a vital sign when visiting a physician.4,5 While most exercise studies have focused on aerobic conditioning, a growing number of strength- and power-training studies have demonstrated that these forms of exercise deliver significant health benefits as well.6 Among these benefits, strength training has been found to ease pain and improve quality of life, and may even manage or prevent cognitive and emotional disorders.
With the recent emphasis on the positive effects of strength training, the popularity of weight training has risen. Between 1998 and 2007, the number of people participating in weight training increased by almost 65%.7 Concurrent with this rise has been an increase in the risk of injury. Some have estimated that 2.4%–7.6% are injured with weight training equipment each year, with the majority of injuries occurring in the lower back or shoulder.7,8 Although not insignificant, when compared to injury rates of high-impact activities or other sports, the magnitude of weight training-induced injury appears to be relatively low.8 Weight training thus appears to have a positive benefit–risk ratio.
When methods by which weight training might be undertaken are considered, two issues must be addressed. One is the frequency of the training, and the other is the intensity. Most methods center on the belief that increased weights will result in improved outcomes.
Resistance training has been shown to improve strength and speed of walking, ultimately resulting in higher scores on such measures as quality-of-life indices.9 Some have argued that virtually all of the benefits of resistance training may be obtained in as few as two 15- to 20-minute training sessions per week.10 One high-intensity weight-training program – the “gravitational wellness” system – has recently been shown to have the capacity to load the musculoskeletal system with uniquely high weights, leading to rapid weekly strength gains using only short, weekly training sessions.11 The gravitational wellness system was developed by a Russian physiologist, Anatoly Samodumov, and brought to the US by Vladimir Chubinsky, a physical therapist. This system evolved to include a weightlifting apparatus that included a wide belt attached to free weights, with a hand-positioning device that allowed the participant to lift high weights over short arcs (Figure 1). The device was considered unique enough that it received patents in both the US and in Russia. In a previous study, a group of middle-aged participants was noted to have progressed to lifting weights averaging over 500 kg.12 The current study was designed to assess the benefit–risk ratio of this very high-intensity weightlifting program.
 | Figure 1 Barbell system positioned according to gravitational wellness system. |
The current investigation was sanctioned by the Emory University Institutional Review Board. This study had three goals. The first was to determine the rate and location of injuries sustained during training with this weightlifting program. The second was to assess the effects of the weightlifting program on the participants’ sense of well-being. The third was to determine the effect of the weightlifting program on the presenting complaint or physical issues that the participants had sought to address.
Materials and methods
Consecutive individuals who presented for training at a gravitational wellness gym in Georgia within the previous 2 years were contacted for participation. Participants were considered for inclusion if they had visited the gym and completed at least one exercise training session. Overall, 77 participants met the criteria for inclusion and were contacted by phone to be offered study participation.
Procedure
Exercise program
All participants were seen at a gravitational wellness center in Georgia. At each exercise session, the participant engaged in four separate exercises. All exercises involved free weights using a barbell system.
Protocol (as outlined in our previous publication12)
The first of the exercises involved the use of a barbell attached to a hoisting belt, attached at each end to a connecting star (see Figure 1). When attached, the participant was asked to bend at the waist and place his/her hands on an upper-body support structure. At this point, the participant was forward flexed at the waist to approximately 90°. The hoisting belt was then placed over the lower back and upper pelvic region of the user. For this maneuver, the feet were approximately shoulder width apart, with the knees bent to 45°. With the belt placed over the lower back, the participant was instructed to inhale, hold their breath, and extend their knees from the starting angle of approximately 45° to near full extension, avoiding a locking of the knees. The lift was to be completed over approximately 3 seconds. Weights were added until the instructor detected that the form of the lift was faltering, thus indicating that the maximal weightlifting capacity was being approached. After this lift, the weight was reduced by 30%, and the participant was asked to complete three additional repetitions, as a cooldown maneuver. The total number of lifts at this station averaged ten.
The second lift was performed using a barbell system positioned within a metal track, such that the starting point of a lift could occur with the patient’s arms fully extended and the knees bent at 45°. The participants’ hands were placed in weightlifting gloves, with the wrist attached to the barbell, so as to assist with the grip of the weights. The subject was asked to keep the back aligned in an upward position, to lean away from the bar at 15°, and to retract the scapula. From this position, the knees were extended, and weights lifted for approximately 3 seconds (see Figure 2). The weights were sequentially increased, until the instructor again noted a faltering of form, indicating that the maximal weightlifting capacity was being approached. With this weight achieved, the weight was reduced by 30%, and the subject was asked to repeat the extension maneuver for three additional repetitions.
 | Figure 2 Hand lift: barbell system positioned according to gravitational wellness system. |
The third lift was performed from a lying position using weightlifting gloves. The weights were again positioned within a track system such that only up-and-down movements were permitted. The participant’s position was such that the barbell was directly above the chin. The grip was slightly wider than shoulder width at the beginning position. A chest-press maneuver was then completed to full extension (see Figure 3). As with the other exercises, weight was added until the subject demonstrated a faltering of form, indicating that the maximal weightlifting capacity was being approached. When this weight was achieved, the weight was reduced by 30%, and the participant was asked to complete three additional repetitions.
 | Figure 3 Chest lift: barbell system positioned according to gravitational wellness system. |
The fourth lift was performed from a lying position using a barbell system contained within upright metal tracks. Wearing tennis shoes, the participant was instructed to lie on the mat, with the soles of the shoes placed at the mid-position of the plantar fascia. The starting position was determined such that the knees were bent at a 45° angle, with the participant instructed to extend the knees, lifting the weights for less than 3 seconds (see Figure 4). Weights were then added as in the previous exercises, until the instructor determined that the form of the subject was faltering, indicating that the maximal weightlifting capacity was being approached. The weight was then reduced by 30%, and the subject completed three additional repetitions. At this reduced weight, the subject’s foot was moved anteriorly and posteriorly on the bar such that the weight was lifted from contact positions just anterior to the calcaneus, and two additional positions until a final lift at the metatarsophalangeal joint. The final maneuver, using the previously described positioning, occurred using the final weight, as previously described. The instructor asked the participant to lift the weights, while the barbell was slowly rotated by the instructor, moving the contact position of the foot from the metatarsophalangeal joint to the anterior calcaneus and back.
 | Figure 4 Leg lift: barbell system positioned according to gravitational wellness system. |
With all of these exercises completed, the participant was instructed to refrain from eating for 2–3 hours. The instructors noted that this instruction was to avoid a shift in the body’s energy system from muscle strengthening to that of digestion. The weekly exercises were completed in the same manner, with the end weight of each session determined by the ability of the participant to maintain form during the performance of each.
Questionnaire
Participants were contacted by telephone, and provided consent for participation by e-mail. The subjects were asked to review the consent, and after verbal agreement, the items of the questionnaire (Supplementary material) were read to the participants concerning their experience with the weightlifting system.
Questions included the age at which they had initiated participation, their sex, whether they had a physical issue that they hoped to improve by participating in the study, and any injury that occurred at the gym. If there was a presenting complaint for which they had sought relief they were further queried as to what degree the issue had improved, using a 5-point Likert scale ranging from “not at all better” to “completely better”. The participants were also asked, in general, whether they felt better after participating in this exercise program, again answering a 5-point Likert scale (see Supplementary material). The participants were then asked if they had experienced any injury during any of the weightlifting sessions. If so, they were asked to describe the injury, and report whether they had missed any training sessions as a result of this injury. They were asked about medical treatment for the injury, and whether this injury remained a problem. The final question was whether they were still participating in this exercise program, and if not, why they had stopped. The Likert-scale data were summarized for mean and median values for both improvement of the presenting physical complaint, as well as improvement in overall well-being.
The weightlifting-participation data were reviewed for weights lifted, with a range of weights lifted by each of the four techniques, as well as the mean and the median weights lifted. The data were also reviewed for number of episodes of participation. The injury risk per episode was calculated by the number of injuries divided by the overall number of injury opportunities/participation.
Results
Of the 77 participants who met the criteria for inclusion, 71 agreed to participate (males, n=40; females, n=31). The participants ranged in age from 18 years to 69 years, with a mean age of 48.6 years and a median age of 50 years. Of these, 42 (59%) had a presenting complaint at their first session. Of the participants, participation ranged from three episodes to 226 episodes, with participants attending a median of 21 sessions.
The mean weights lifted are depicted in Table 1. The mean initial belt lift was 247.79 kg, with a mean final lift of 505.69 kg. The mean initial hand lift was 98.74 kg, with a mean final lift of 181.04 kg. The mean initial chest press was 87.76 kg, with a mean final chest press of 138.81 kg. The mean initial leg press was 223.08 kg, with a mean final leg press of 390.46 kg. No injuries were reported by any of the participants at any weightlifting session, and none reported having discontinued secondary to fear of injury.
 | Table 1 Beginning and end weights lifted (in kilograms) by subjects in belt lift, hand lift, chest press, and leg press |
All of the participants had reported learning of the weightlifting program from a friend or acquaintance. Each noted that they were hopeful of positive health benefits through weightlifting. Of the presenting complaints, 23 reported chronic neck and/or back pain, eight reported joint issues, two reported a desire for strength gains, and nine presented with other issues. These issues improved by an average of 4.2 on a 5-point Likert scale, with back pain improving by an average score of 4.13.
For the question of overall well-being, the group reported a mean gain of 4.27 on the 5-point Likert scale. Of those who did not have a presenting physical complaint, the mean improvement in global well-being was 4.07/5, while for those who did have a presenting complaint overall well-being improved by a mean of 4.25/5 (Tables 2 and 3). The mean improvement in well-being for males was 4.3 and for females was 4.28 (Tables 4 and 5).
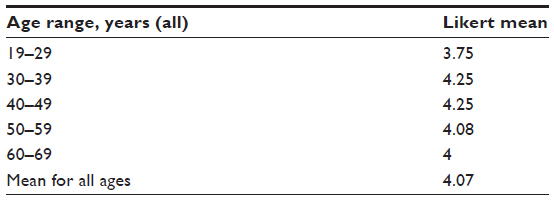 | Table 2 Presenting complaint improvement |
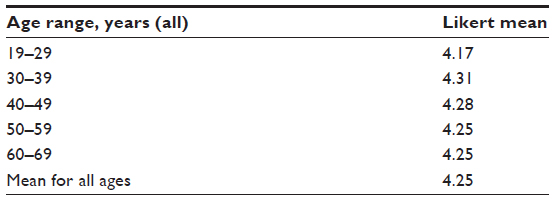 | Table 3 General sense of well-being |
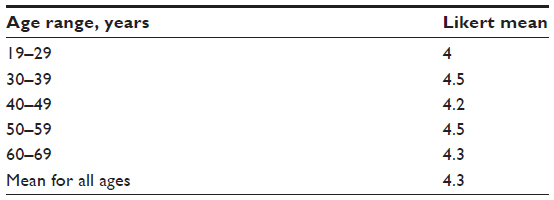 | Table 4 Presenting complaint improvement – males |
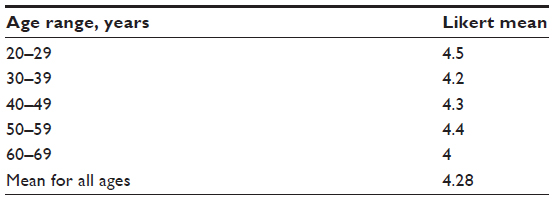 | Table 5 Presenting complaint improvement – females |
Among those not currently engaged in the program, the majority stated that they had completed the program. Others noted that they had scheduling issues that precluded continued participation. Four reported financial reasons for discontinuation.
Discussion
Previous studies concerning the risks of injury from weight training and weight equipment have been estimated to be as low as 2%–8% of participants per year.7 Compared with injuries from competitive team sports and high-impact activity, injuries incurred during weightlifting are relatively low.7
This study involved consecutive participants, averaging 48 years of age, in a weightlifting technique that has been previously reported to result in significantly heavier weights lifted and significant weekly gains compared to other weightlifting programs.13 Despite these high weights, the subjects reported no injuries.
Others have studied injury risk among weightlifters. Despite a relatively low injury rate as a group, there are populations thought to have a relatively greater risk compared to others.7 Jones et al suggested that participants over the age of 45 years are at a higher risk of injury, though this injury risk was thought to be reduced when the activity was supervised.8
The weightlifting technique reviewed in this paper involved a protocol that required the supervision of every lift by the gym director. As the weights noted in this program are significantly higher than reported in other programs, especially with the belt lift technique, this supervision seems a potentially important contributor to the low injury rate. One might note that as the belt system is novel to all participants, one might introduce stress into the lower back that was not intended. Even among participants reporting no experience with weightlifting prior to using this system, supervision with the belt lift seems to have resulted in a high level of safety.
This paper also reviewed the subjective benefits for those who participated in the weightlifting technique. The majority of participants had a presenting physical complaint that they hoped would improve through the weightlifting. The modal of these was chronic musculoskeletal discomfort, particularly of the cervical or thoracic/lumbar spine. All of the participants with back pain complained that the pain was chronic and that it had been resistant to treatment by more conventional therapies. The majority of these reported a significant resolution of this back pain, as reflected by a Likert-scale improvement of 4.13/5.
Even with a low number of participants, given the tenacity of chronic back pain, these findings are encouraging, and suggest the need for further investigation. Studies have shown that when back pain exceeds 6 months in duration, the chance of a single therapeutic intervention resulting in a clinically significant improvement in back pain is quite low.14 Exercise therapy, focusing on strengthening and stabilizing the core muscle groups of the abdomen and back, appears to produce small improvements in pain and functioning in participants with chronic low-back pain.14 In fact, few studies (ie, six of the 43 studies included in a Cochrane review) have been able to demonstrate clinically important and statistically significant differences between intervention and control groups.15 This uncontrolled study found that a very high-weight lifting program resulted in significant improvement or resolution of symptoms in many of the participants, certainly suggesting a need for further inquiry. In addition, a high mean score of 4.2/5 on a Likert scale suggests that this technique may be quite effective for enhanced well-being.
Our study has several limitations. First, the questionnaires were retrospective, asking for participants to judge the effect of the weightlifting on both their chief complaint/medical condition, as well as their overall well-being. Because this was retrospective, the recall may have differed from that expected in a prospective study, in which these effects could be documented during the course of the intervention. Second, participants in this study presented to the gym in a nonrandomized fashion. Expectations of results based on referrals by others may have influenced the overall perception of the intervention. One might expect different results if the study had been prospective, with the subjects randomized to this technique. In addition, the lack of any injuries in the survey is surprisingly troublesome, in that it does not allow for a true calculation of the risk of injury. While the risk of injury during weightlifting has been thought to be historically low, the findings of no injury precludes our ability to compare this to other weightlifting techniques and other exercise interventions.
In summary, this study of 71 consecutive participants involved in the gravitational wellness weightlifting system found none of the participants reporting any injuries during the weightlifting tasks, and that the technique resulted in significant improvement of specific physical ailments, as well as overall sense of well-being.
Acknowledgment
The subjects who appear in the photographs/figures gave their consent for their images to be used in this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
Centers for Disease Control and Prevention. Obesity and overweight. Available from: http://www.cdc.gov/nchs/fastats/obesity-overweight.htm. Accessed June 9, 2014. | |
Sharma M. Behavioural interventions for preventing and treating obesity in adults. Obes Rev. 2007;8(5):441–449. | |
Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006;174(6):801–809. | |
Hellénius ML, Sundberg CJ. Physical activity as medicine: time to translate evidence into clinical practice. Br J Sports Med. 2011;45(3):158. | |
Sallis RE. Exercise is medicine and physicians need to prescribe it! Br J Sports Med. 2009;43(1):3–4. | |
Pollock ML, Franklin BA, Balady GJ, et al. AHA Science Advisory. Resistance exercise in individuals with and without cardiovascular disease: benefits, rationale, safety, and prescription: an advisory from the Committee on Exercise, Rehabilitation, and Prevention, Council on Clinical Cardiology, American Heart Association; position paper endorsed by the American College of Sports Medicine. Circulation. 2000;101(7):828–833. | |
Kerr ZY, Collins CL, Comstock RD. Epidemiology of weight training-related injuries presenting to United States emergency departments, 1990 to 2007. Am J Sports Med. 2010;38(4):765–771. | |
Jones CS, Christensen C, Young M. Weight training injury trends: a 20-year survey. Phys Sportsmed. 2000;28(7):61–72. | |
Kraemer WJ. General adaptations to resistance and endurance training programs. In: Baechle T, editor. Essentials of Strength Training and Conditioning. Champaign (IL): Human Kinetics; 1994:127–150. | |
Winett RA, Carpinelli RN. Potential health-related benefits of resistance training. Prev Med. 2001;33(5):503–513. | |
Burke DT. Case study of weight training using a novel weight training method. J Rehabil Med Suppl. 2013;45(53):489–490. | |
Burke DT, Tran D, Cui D, Burke DP, Al-Adawi S, Dorvlo AS. Significant progression of load on the musculoskeletal system with extremely high loads, with rapid weekly weight gains, using the Anatoly Gravitational System, in a 10-week training period. Open Access J Sports Med. 2013;4:211–219. | |
Rippetone M, Kilgore L. Practical Programming for Strength Training. 2nd ed. Wichita Falls (TX): Aasgaard; 2009. | |
van Tulder M, Malmivaara A, Hayden J, Koes B. Statistical significance versus clinical importance trials on exercise therapy for chronic low back pain as example. Spine (Phila Pa 1976). 2007;32(16):1785–1790. | |
Hayden JA, van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non-specific low back pain. Cochrane Database Syst Rev. 2005;(3):CD000335. |
Supplementary materials
Injuries incurred in gravitational wellness system weight training
This survey is designed to determine whether and what type of injuries you experienced while engaged in the gravitational wellness system.
At the time of your involvement: Age: ______
Sex: Male/Female
Did you have a physical issue/illness that you hoped to address when you arrived at the gym? (presenting complaint)
On a 5-point scale, to what degree did it improve? 1 (not at all), 2 (a little), 3 (a moderate amount), 4 (quite a bit), 5 (completely resolved)
In general do you feel better after participating in this exercise program (general sense of physical well-being)? 1 (not at all), 2 (a little), 3 (a moderate amount), 4 (quite a bit), 5 (tremendously)
Have you experienced any injury during a session or as a result of the exercise? Yes/No
If yes, what was your injury? __________________________________
Did you miss any training sessions as a result of this injury? Yes/No
How many sessions did you miss? _____
Did you seek medical attention for this injury? Yes/No
What treatment did you receive?
Do you still have problems with this injury? Yes/No
Are you still participating in this exercise technique? Yes/No
If not, did you stop as a result of the injury or fear of sustaining an injury? Yes/No
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.