")
Back to Journals » International Journal of Women's Health » Volume 15
Rare Vulvar Angiomyofibroblastoma: Case Series and Literature Review
Authors Chen L, Sun Q, Zhang J, Xu X, Fan X
Received 13 January 2023
Accepted for publication 13 March 2023
Published 22 March 2023 Volume 2023:15 Pages 427—431
DOI https://doi.org/10.2147/IJWH.S403121
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ling Chen,1 Qiuwei Sun,1 Junchao Zhang,1 Xizhong Xu,2 Xiaofang Fan1
1Department of Ultrasound Medicine, Affiliated Hospital of Jiangnan University, Wuxi City, Jiangsu Province, People’s Republic of China; 2Department of Gynecology, Affiliated Hospital of Jiangnan University, Wuxi City, Jiangsu Province, People’s Republic of China
Correspondence: Xiaofang Fan, Department of Ultrasound Medicine, Affiliated Hospital of Jiangnan University, No. 200, Huihe Road, Binhu District, Wuxi City, Jiangsu Province, 214062, People’s Republic of China, Tel + 86-13861843829, Email [email protected]
Background: Angiomyofibroblastoma (AMFB) is an uncommon disease with few literature reports, leading to the poor understanding of its diagnosis, treatment, and postoperative follow-up plans among gynecologists.
Objective: To study the clinical and pathological features of vulvar AMFB and discuss its treatment and prognosis.
Case Summary: The 3 cases were characterized by a gradually increasing painless mass in the vulva. Preoperative diagnosis was difficult and mainly depended on ultrasonic examination. Immunohistochemistry confirmed clear boundaries of AMFB. This condition could be completely cured by surgery, and the prognosis was good.
Conclusion: The vulvar AMFB is a rare tumor that is frequently misdiagnosed before surgery. Ultrasound is preferred in auxiliary diagnosis, and surgery remains the best treatment, and long-term follow-up is necessary to avoid recurrence or other complications.
Keywords: angiomyofibroblastoma, diagnosis, surgery, follow-up
Introduction
Angiomyofibroblastoma (AMFB), a rare benign mesenchymal tumor, often occurs in women of reproductive age, mostly in the vulva, vagina, and perineum.1,2 It has occasionally been reported in the male scrotum and groin.3 Because it is difficult to differentiate AMFB from other vulvar tumors, AMFB cannot be diagnosed preoperatively.4 Its clinical manifestations and pathological characteristics resemble those of several other vulvar tumors, but their biological behavior and prognoses are different.1,5,6 Hence, the differential diagnosis of AMFB is crucial. In this report, we discussed the clinicopathological features and differential diagnosis of 3 cases of AMFB to enhance the understanding of this rare tumor.
Case Presentation
Case 1
A 50-year-old woman presented with a 2.5 cm diameter mass in left labium majus for 12 months which was preoperatively diagnosed as a genital cyst and then surgically excised. The ultrasonographic manifestations included nearly elliptic mass with complete border, non-uniform hypoechoic background, irregularly distributed short-strip high echo, without any echo attenuation or enhancement on the posterior region (Figure 1A). The surgical excision of the lesion was conducted and a mass was taken for pathological examination. The lesion was completely cured by local excision. Grossly, the mass was well defined and its smooth surface was surrounded by an intact membrane. Sectioning showed a solid white mass with no any necrosis or bleeding deterioration. Histologically, a 2.5 × 2 × 2 cm vulvar mass was reported, featured by alternating hypercellular and hypocellular regions of oval or epithelioid stromal cells, aggregated around blood vessels. Immunohistochemically, the expression of estrogen receptor (ER), progesterone receptor (PR), vimentin, CD34, smooth muscle actin (SMA) was positive, and negative for desmin, MSA, AE1/AE3, and S-100. Low level of proliferation (Ki67) was recorded. The diagnosis of AMFB was determined.
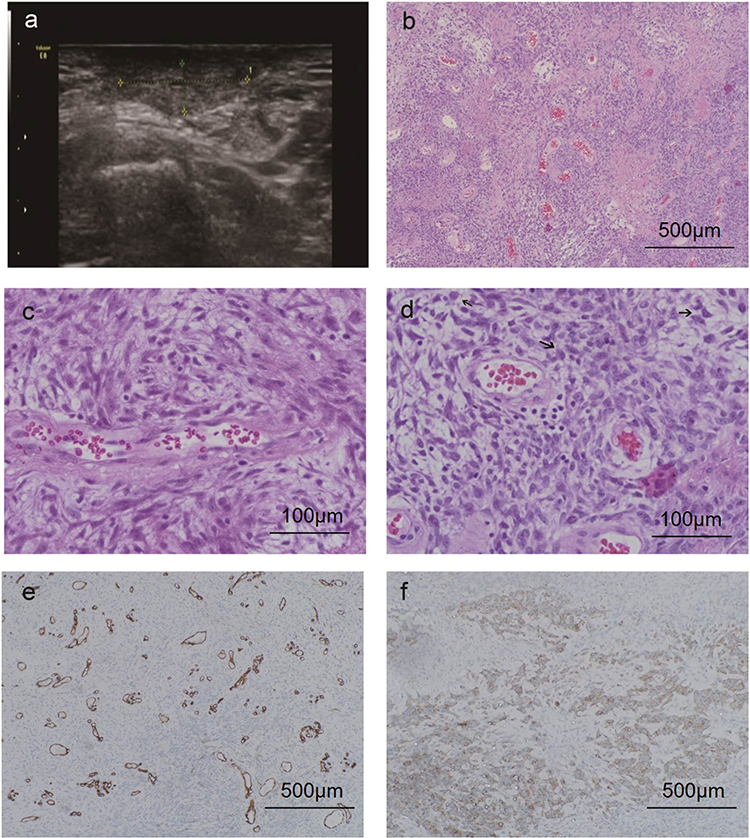 |
Figure 1 Ultrasonography and pathology of AMFB. (A) Ultrasound indicates a moderate echo in the mass. (B) The hypercellular areas of cells are alternately distributed with hypocellular areas of cells, and abundant thin-walled small blood vessels are seen (HE×100). (C) The hypercellular areas of cells, tumor cells are distributed in bundles or patches around blood vessels, cells are spindle-shaped, cytoplasmic eosinophilic, and some cells are round or oval and epithelioid in shape (HE×400). (D) One case has slightly abundant tumor cells, and the mitotic phase is visible (about 1–2/10HPF)(HE×400). (E) Vascular endothelial cells CD34(+)(IHC×100). (F) Tumor cell vimentin(+)(IHC×100). |
Case 2
A 42-year-old woman developed with a genital mass, 2.5 cm diameter, having grown for 4 months. The mass caused no pain, no bleeding, and no discharge. Macroscopically, the patient had oval masses (2.5×1.8×1.5 cm) with a distinct boundary or capsule, a grey or grey-red section surface, partial edema, and soft texture. Ultrasound examination showed the regular vascularity and homogeneous echo in the mass. Histopathologic examination after the excision of the mass showed a well-differentiated tissue with no rupture of its capsule. The hypercellular areas alternated with hypocellular areas and abundant thin-walled small blood vessels were observed (Figure 1B). In the hypercellular areas, tumor cells, spindle-shaped and cytoplasmic eosinophilia, were distributed in bundles or patches around blood vessels, and some round or oval and epithelioid cells were observed (Figure 1C). The nuclei were rod-shaped, ovoid, or round, and the nucleoli were inconspicuous. In the hypocellular areas, the tumor cells were scattered in a loose edematous matrix. The pathological findings also suggested that tumor cells were relatively abundant and mitosis was visible (approximately 1–2/10 HPF) (Figure 1D). On the suspicion of AMFB, the immunohistochemistry indicated the following results: ER (+), PR (+), Vimentin (+), CD34 (+), SMA (+), desmin (-), MSA (-), AE1/AE3 (-), s-100 (-), and Ki67 (+, <5%) (Figure 1E and F). During the following half a year later, the patient was followed up and developed recurrence, which was cured by reoperation and the pathological results after the second surgical resection were the same as those of the previous surgery.
Case 3
A 48-year-old woman complained of a vulvar mass. One year earlier, the patient had found a small nodule in the left labium majus, but no treatment was performed. The gradually growing nodule eventually had spontaneous pain, prompting the patient to come to our department. At the initial visit, a quail egg-sized, elastic subcutaneous mass was found at the left labium majus. On palpation, the mass had a well circumscription and good mobility. The skin covering the mass was observed to be normal. The results of ultrasound examination showed a soft tissue tumor with healthy blood vessels and homogeneous echo. According to the clinical course and the results of ultrasound examination, genital cyst was diagnosed and surgery was conducted under general anesthesia. Macroscopically, the size of the resected tumor was 3.0×2.2×2.0 cm. Histologically, the tumor was composed of sparse collagen fibers and had small or medium-sized blood vessels around which the tumor cells were aggregated, oval, or spindle-shaped with acidophilic and fibrous cytoplasm. In addition, the collections of multinucleated giant cells and epithelioid cells were also observed. The cells were sparse outside the perivascular region. The immunohistochemistry indicated the following results: ER (+), PR (+), Vimentin (+), CD34 (+), SMA (+), desmin (-). Based on these finding, the diagnosis of AMFB with granulomatous inflammation was confirmed. No recurrence was noticed within 6 months after surgery.
The study was performed in accordance with the CARE guidelines. The study was approved by the Ethics Committee of Affiliated Hospital of Jiangnan University (LS2019057), and written informed consent was obtained from the patients for the publication of images or data appearing in this article.
Discussion
AMFB is a rare benign soft tissue tumor. Only about 70 cases of vulvar AMFB have been reported in women outside China. Fletcher et al first reported 10 cases of female vulva AMFB in 1992,2 and then Laskin et al reported 11 cases of AMFB in 1998 in the male reproductive tract.7 A total of 71 cases of vulvar AMFB reported in the literature till 2012 were summarized by Sims et al8 who described the tumor as a painless mass with a duration of 2 months to 10 years in patients with a mean age of 45 (range, 17−86) years. Generally, the tumor is 0.5–5 cm in diameter, occasionally reported up to 10 cm, and is often misdiagnosed as a Bartholin’s gland cyst, abscess, or lipoma.9–11
The clinical data of the 3 patients showed similarity to those reported abroad, but the median duration of the disease was shorter than that reported abroad, which may be attributed to the increased awareness of their health. Due to the short course of this disease, the mean volume of the mass was also lower than those previously reported. No cases were diagnosed with AMFB before the surgery. Intraoperative findings revealed clear boundaries, good activity, good plasticity, and a grey-white or yellow color of the AMBF that could be completely resected. Wolf et al proposed that ultrasound shows clear boundaries of AMFB and presents as a solid mass with hypoechoic echo, with a partially visible blood flow signal in the mass, suggesting that it could assist in the diagnosis of AMFB.12 The ultrasound findings in the present case were similar to those in the literature.
Most scholars believe that the disease may originate from stem cells with multidirectional differentiation potential around blood vessels although its histological origin remains unclear.13 Some scholars suggest that AMFB may result from local damage, inflammation, granulation tissue hyperplasia, and estrogen and other factors, which lead to abnormal mother cell proliferation in the muscle fiber, forming a specifically shaped and relatively independent benign tumor. Microscopically, thin-walled blood vessels are abundant and distributed in clusters. The hypercellular areas and hypocellular areas appear alternately. The tumor cells in the hypercellular areas are arranged around the blood vessels; the cell size is consistent, and the cytoplasm is abundant, with oval nuclei. Few tumor cells, which are distributed in the stroma of myxedema, observed in the loose area. The pathological manifestations of the 3 patients conformed to the above characteristics. Immunohistochemistry of AMFB generally shows positive staining for vimentin, estrogen receptor, and progesterone receptor. Recently, it is reported that strong immunohistochemical expression of CYP2E1 is found in AMFB, which may also be used as a new marker in the detection of AMFB in the future.14
Several types of soft tissue tumors occur in the vulva. AMFB is mainly differentiated from the following three types of tumors: (1) Aggressive angiomyxoma (AA) normally occurs in the female pelvic cavity or deep soft tissue, showing infiltrative growth without obvious boundaries; complete resection is difficult, and relapse is common. Microscopically, the mucosal changes of invasive vascular mucosa tumors are relatively extensive, and the tumor cells are distributed evenly, often invading adjacent tissues. (2) Cellular angiofibroma (CA) is usually smaller than AMFB in diameter and shows clear unitary tumor cell formation. Cells are abundant, and fission is clear. There is no change in density. Epithelioid cell clusters are vascular centered, similar to the characteristics of AMFB. The blood vessels in tumors are mostly medium-sized, with thick hyaline wall and a small amount of stroma. (3) Superficial angiomyxoma (SA) shows frequent nodular growth, thick-walled interstitial blood vessels (significantly different from AMFB), rich interstitial mucus, and a few cells; SA is also prone to relapse. In immunohistochemistry, SMA and desmin are negative.
Although AMFB is a rare tumor and can be misdiagnosed preoperatively, the preoperative ultrasonography can assist in the diagnosis of AMFB. Currently, no drugs are available to treat AMFB, and surgery is preferred. The diagnosis is finally confirmed by pathological results. Actually, AMFB should be considered a tumor with a very low risk of sarcomatous overgrowth/dedifferentiation. As a benign tumor, its prognosis is usually good, and the occasional local recurrence is mostly due to residual tumor during surgical resection. This recurrence is not invasive and easily cured by a second operation.15 Only a few malignant cases were reported. A study of 50 cases demonstrated that all patients undergo complete resection of the tumor and are followed up from 3 months to 25 years after surgery, and only one case develops sarcoma 2 years after complete resection.16 Furthermore, Folpe et al reported sarcomatous transformation in AMFB.17 Notably, the pathological findings suggested that tumor cells were relatively abundant and mitosis was visible (approximately 1–2/10 HPF) in one case that recurred half a year later, and the pathological results after the second surgical resection were the same as those of previous surgery. This fully shows that malignant transformation is possible. No cases of distant metastasis have been reported. From the results of these cases and the literature review, gynecologists are suggested to extend the follow-up period, increase the frequency of postoperative follow-up, and use ultrasound examination during re-examination of the case.
Conclusion
The vulvar AMFB is a rare tumor that is frequently misdiagnosed before surgery. Ultrasound is preferred in auxiliary diagnosis, and surgery remains the best treatment, and long-term follow-up is necessary to avoid recurrence or other complications.
Ethics Approval and Informed Consent
The study was performed in accordance with the CARE guidelines. The study was approved by the Ethics Committee of Affiliated Hospital of Jiangnan University (LS2019057), and written informed consent was obtained from the patients for the publication of images or data appearing in this article.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Maternal and child health scientific research project of Wuxi Municipal Health Commission [FYKY 202005].
Disclosure
No potential conflicts of interest were disclosed.
References
1. McCluggage WG. A review and update of morphologically bland vulvovaginal mesenchymal lesions. Int J Gynecol Pathol. 2005;24(1):26–38.
2. Fletcher CD, Tsang WY, Fisher C, et al. Angiomyofibroblastoma of the vulva. A benign neoplasm distinct from aggressive angiomyxoma. Am J Surg Pathol. 1992;16(4):373–382. doi:10.1097/00000478-199204000-00006
3. Ito M, Yamaoka H, Sano K, et al. Angiomyofibroblastoma of the male inguinal region. Arch Pathol Lab Med. 2000;124(11):1679–1681. doi:10.5858/2000-124-1679-aotmir
4. Wang Y, Zhang Y, Lv B, et al. Large-sized pedunculated and polypoidal angiomyofibroblastoma of the vulva: a case report and literature review. J Obstet Gynaecol Res. 2018;44(8):1492–1497. doi:10.1111/jog.13692
5. Dufau JP, Soulard R, Gros P. Angiofibrome cellulaire, angiomyofibroblastome et angiomyxome agressif: variantes d'une meme tumeur stromale de la sphere genitale?. Ann Pathol. 2002;22(3):241–243.
6. Alameda F, Munné A, Baró T, et al. Vulvar angiomyxoma, aggressive angiomyxoma, and angiomyofibroblastoma: an immunohistochemical and ultrastructural study. Ultrastruct Pathol. 2006;30(3):193–205. doi:10.1080/01913120500520911
7. Laskin WB, Fetsch JF, Mostofi FK. Angiomyofibroblastoma like tumor of the male genital tract: analysis of 11 cases with comparison to female angiomyofibroblastoma and spindle cell lipoma. Am J Surg Pathol. 1998;22(1):6–16. doi:10.1097/00000478-199801000-00002
8. Sims SM, Stinson K, McLean FW, et al. Angiomyofibroblastoma of the vulva: a case report of a pedunculated variant and review of the literature. J Low Genit Tract Dis. 2012;16(2):149–154. doi:10.1097/LGT.0b013e318231217b
9. Qiu P, Wang Z, Li Y, et al. Giant pelvic angiomyofibroblastoma: case report and literature review. Diagn Pathol. 2014;9:106. doi:10.1186/1746-1596-9-106
10. Fatusic J, Hudic I, Fatusic Z, et al. Angiomyofibroblastoma of the vaginal portion. Med Arch. 2014;68(6):424–425. doi:10.5455/medarh.2014.68.424-425
11. Nagai K, Aadachi K, Saito H. Huge pedunculated angiomyofibroblastoma of the vulva. Int J Clin Oncol. 2010;15(2):201–205. doi:10.1007/s10147-010-0026-0
12. Wolf B, Horn LC, Handzel R, et al. Ultrasound plays a key role in imaging and management of genital angiomyofibroblastoma: a case report. J Med Case Rep. 2015;9:248. doi:10.1186/s13256-015-0715-4
13. Granter SR, Nucci MR, Fletcher CD. Aggressive angiomyxoma: reappraisal of its relationship to angiomyofibroblastoma in a series of 16 cases. Histopathology. 1997;30(1):3–10. doi:10.1046/j.1365-2559.1997.d01-556.x
14. Tajiri R, Shiba E, Iwamura R, et al. Potential pathogenetic link between angiomyofibroblastoma and superficial myofibroblastoma in the female lower genital tract based on a novel MTG1-CYP2E1 fusion. Mod Pathol. 2021;34(12):2222–2228. doi:10.1038/s41379-021-00886-8
15. Angelico G, Marletta S, Broggi G. Practical Approach to the Diagnosis of the Vulvo-Vaginal Stromal Tumors: an Overview. Diagnostics. 2022;12:2. doi:10.3390/diagnostics12020357
16. Nielsen GP, Young RH, Dickersin GR, et al. Angiomyofibroblastoma of the vulva with sarcomatous transformation (“angiomyofibrosarcoma”). Am J Surg Pathol. 1997;21(9):1104–1108. doi:10.1097/00000478-199709000-00016
17. Folpe AL, Tworek JA, Weiss SW. Sarcomatous transformation in angiomyofibroblastomas: a clinicopathological, histological and immunohistochemical study of eleven cases. Mod Pathol. 2001;14:12A.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.