")
Back to Journals » Infection and Drug Resistance » Volume 15
Rapid Identification and Drug Sensitivity Test to Urinary Tract Infection Pathogens by DOT-MGA
Authors Liu Z, Tang H, Xu H, Lu G, Yang W, Xia Z, Zhu Y , Ni S, Men W, Shen J
Received 15 January 2022
Accepted for publication 17 March 2022
Published 31 March 2022 Volume 2022:15 Pages 1391—1397
DOI https://doi.org/10.2147/IDR.S356045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Zhen Liu,1 Hao Tang,1 Huaming Xu,1 Guoping Lu,2 Wensu Yang,1 Zhaoxin Xia,1 Yi Zhu,1 Shenwang Ni,1 Wanqi Men,1 Jilu Shen1
1The Fourth Affiliated Hospital of Anhui Medical University Laboratory Department, Hefei, People’s Republic of China; 2Laboratory Department of Fuyang Hospital Affiliated to Anhui Medical University, Fuyang, Anhui, 236000, People’s Republic of China
Correspondence: Jilu Shen, The Fourth Affiliated Hospital of Anhui Medical University Laboratory, No. 100 Huaihai Avenue, Xinzhan District, Hefei, Anhui Province, 230012, People’s Republic of China, Tel +86 151 5515 2963, Email [email protected]
Aim: To reduce the inspection time for urinary tract pathogens and provide a rapid and effective therapeutic plan for clinical anti-infection treatment, this study developed a rapid identification (ID) and antimicrobial sensitivity test (AST) method by DOT-MGA.
Methods: We grouped midstream urine samples with single bacteria according to the number of bacteria (≤ 5/5– 15/≥ 15) under per oil microscope after Gram staining. Then we adopted differential centrifugation to process the grouped samples to collect precipitate. MALDI-TOF MS was performed using precipitate directly or after short-term culture. If succeed, we resuspended the precipitate into droplets with or without antibiotics at a MALDI target. Four hours later, mass spectrometer (MS) was used to identify the culture on the target and to analyse AST.
Results: Samples (count ≥ 15), which precipitate can be directly identified by MS; otherwise, the precipitate need a short-term cultured for 3– 6 h before ID. The consistency of the ID results between conventional culture and the precipitate is 100%. Compared with broth microdilution method, DOT-MGA for predicting AST had a high consistency. EA and CA for IPM, LEV, CAZ, NIT, and FOT were 100%/100%, 98%/90%, 98%/92%, 100%/90%, 98%/94%, respectively. No VME was observed in all tests. Besides, MIC50 for the five antibiotics by DOT-MGA and broth microdilution method were ≤ 1/≤ 0.5,> 2/2,≤ 4/≤ 2,≤ 32/≤ 16,≤ 64/≤ 32 and MIC90 were ≤ 1/≤ 0.5, > 2/> 4, 16/16, 128/128, 128/64.
Conclusion: This study can shorten the ID time (minimum 0.5h) and AST (minimum 4h) of the main pathogens of urinary tract infection to 5– 10 hours, which greatly reduce the inspection time and provide substantial help for the rapid diagnosis and treatment of patients with urinary tract infection.
Keywords: MALDI-TOF, DOT-MGA, rapid drug susceptibility test, urinary tract infection, antibiotics resistance
Introduction
Urinary tract infection is a common infectious disease, which causes about 150 million patients worldwide.1,2 UroPathogenic Escherichia coli is the most common pathogen, which can cause more than 80% of community-acquired urinary tract infections.3 Regular urine pathogen ID and AST requires at least 24–72 h. So that the empirical treatment of clinicians may lead to some bad results. Such as alter the species and abundance of microbiota, cause the dominant growth of drug-resistant bacteria, finally lead to the failure of anti-infection treatment and serious complications.4,5 Therefore, it is particularly important to explore a rapid ID and AST method for infectious pathogens of urinary tract to reduce complications and improve prognosis.
In recent years, matrix assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) has become a reference standard for microbial ID.6 Increasing evidence have shown that MALDI-TOF MS can directly detect microorganisms in urine samples.7,8 In addition, previous studies reported that the direct-on-target microdroplet growth assay (DOT-MGA) can rapidly achieve strain ID and AST in one diagnostic workflow.9,10 At present, many studies have shown that the rapid ID and AST of bacteria-positive blood culture are feasible and accurate, Idelevich et al11 and Ilka et al12 used DOT-MGA to quickly detect the drug resistance of Gram-negative bacteria in positive blood culture, and explored the methicillin resistance of Staphylococcus aureus in the cultured samples. Recently, our research group also published a new method for directly detection of bacterial drug resistance in positive blood cultures based on DOT-MGA.13 However, there is no report of rapid ID programme and AST by DOT-MGA directly for urine samples instead of culture. Therefore, this study aims to find a method for rapid ID and AST of the infectious pathogens of urinary tract, in order to minimize turnaround time and provide reference for precise clinical treatment.
Materials and Methods
Bacterial Strains
We selected 52 midstream urine samples with single bacterial under the view of each oil mirror after gram staining. Each sample was counted, grouped, pre-treated and precipitated. Then compared the result of precipitation direct or short-term cultured membrane by MS with conventional culture.
Considering that the pathogens of urinary tract infection are mainly Enterobacteriaceae bacteria, we selected an additional 50 strains of urine infected with single Enterobacteriaceae bacteria, count ≥15/oil lens, and tested by DOT-MGA in order to obtain its sensitivity to five antibiotics. The minimum inhibitory concentrations (MICs) of 50 samples was obtained by micro broth dilution method.
Evaluation of Bacterial Population, Pre-Treatment, and MALDI-TOF MS ID
Number of bacteria were counted using 10μL urine smear with Gram staining. Results were classified it into ≤5/oil lens, 5–15/oil lens, and ≥15/oil lens. From the same sample, 10 mL of urine were centrifuged (2000g, 2min), the supernatant was then transferred to a new centrifuge tube, followed by centrifugation at higher speed (12000g, 5min). The resultant pellet was resuspended with 1mL of 0.45% saline and centrifuge again (12000g, 5min). After rinsing for two times, the pellet was divided into two parts.One was identified by MALDI-TOF MS (Bruker Daltonik GmbH, Bruker, Germany), the other was transferred onto blood agar plate (Shanghai Comajal Microbial Technology Co., Ltd, China). At 3h, 4h, 5h, and 6h after short-term culturing, samples were collected and identified by MS. In addition, 1μL of fresh urine was directly identified by MS without pre-treatment.Compared all identification results by MS with bacterial colony after 18–24h in conventional culture.
Drug Sensitivity Test
MIC for all isolates was determined by microbroth dilution reference method according to the CLSI and ISO guidelines, and we chose five points near the break point. The reference strain E. coli ATCC25922 was used as a quality control (QC). In brief, a bacterial suspension of 0.5 McFarland was added to a cation-adjusted Mueller-Hinton broth (CA-MHB, Qingdao Rishui Biotechnology Co., Ltd.). After the addition of the antibiotics, in which, imipenem (IPM, Solarbio), ceftazidime (CAZ, Solarbio), levofloxacin (LEV, Glpbio), nitrofurantoin (NIT, Glpbio), fosfomycin (FOT, Glpbio) concentration ranged from 0.5μg/mL to 8μg/mL, 2 μg/mL to 32 μg/mL, 0.25 μg/mL to 4 μg/mL, 16 μg/mL to 256 μg/mL, 32 μg/mL to 512 μg/mL, respectively. The final concentration of the bacterial suspension was approximately 5x105cfu/mL.The results were read after 18 ±2 h for incubation at 35 ± 1 °C. The MIC results were interpreted according to the EUCAST breakpoint.
DOT-MGA
Enterobacteriaceae bacteria (50 Cases), count of bacteria ≥15/oil lens of single bacteria and identification scores by MS ≥1.7 after collecting, were used to perform the DOT-MGA for fast AST. The above precipitation was configured into 0.5 McFarland suspension (108 CFU/mL). The solution was further diluted 100 times with Mueller Hinton II broth and 100μL bacterial suspension was mixed with 100μL antibiotic solution in the wells of the microtiter plate (5x105CFU/mL). Additionally, the selection of five antibiotics was agreement with the broth microdilution reference method, and three sensitivity/intermediate/resistance breakpoints (IPM 1/2/4 μg/mL, LEV 0.5/1/2 μg/mL, CAZ 4/8/16 μg/mL, NIT 32/64/128 μg/mL, FOT 64/128/256 μg/mL) were selected according to the CLSI and ISO guidelines. Six-microliter of each mixed solution was loaded onto the microwells of the MALDI target plate (Bruker Daltonik GmbH, Bruker, Germany) with 4-mL deionized water added to the bottom of the box and the box was incubated at 35°C ± 1°C for 4 h, then the broth was removed from the target plate with filter paper, followed by MS identification. Three bacterial suspensions without antibacterial drugs were set as a growth control and identification hole for each sample to determine the validity of this experiment.
The spectra were classified and annotated using flexControl software (Version 3.4, Bruker Daltonik GmbH, Bruker, Germany), MALDI Biotyper Compass Explorer (Version 4.1, Bruker Daltonik GmbH, Bruker, Germany), and Bruker MBT database matching (Version 9607MSP_3239 Species). Briefly, if the three growth control wells have more than two identification scores ≥1.7, the test is considered valid. For a valid sample, a target score ≥ 1.7 is considered as resistance to the tested drug at the tested concentration, otherwise it is considered sensitive. Whether the final judgment is sensitive, intermediate, or drug-resistant, on the basis of the bacterial growth in the three breakpoint concentrations in the microwells.
Data Analysis
According to bacterial counts, after different pretreatment, analyzed the consistency of Urine pathogen direct identification and colony identification of conventional culture. The results from DOT-MGA were compared with the broth microdilution method to evaluate classification agreement rate (CA), essential agreement rate (EA), very major error (VME), major error (ME), and minor error (mE) etc. Comparison of this study method with traditional bacterial identification and drug sensitivity methods, analyzed the change of TAT time.
Results
Gram Staining Classification and MS Identification of Urine Samples
Direct identification was failed in all the urine samples without pre-treatment. Samples with single bacteria count≥15/oil lens field that its precipitate can be directly identified by MS; otherwise, the precipitate need a short-term cultured for 3–6h before identification. The consistency between the identification results and conventional culture was 100%.Among them, there are 40 strains of Enterobacteriaceae bacteria, and 25 strains were directly identified and 15 strains needed short-term culture. That the precipitate, grouping of count 5–15/oil lens and ≤ 5/oil lens needed 3–4h (biofilm growth rate 90.9%) and 5–6h (biofilm growth rate was 100%) before identification, respectively. That is, it can be identified (as shown in Tables 1 and 2).That it significantly reduce detection time, compared with 18–24 hours of conventional detection.
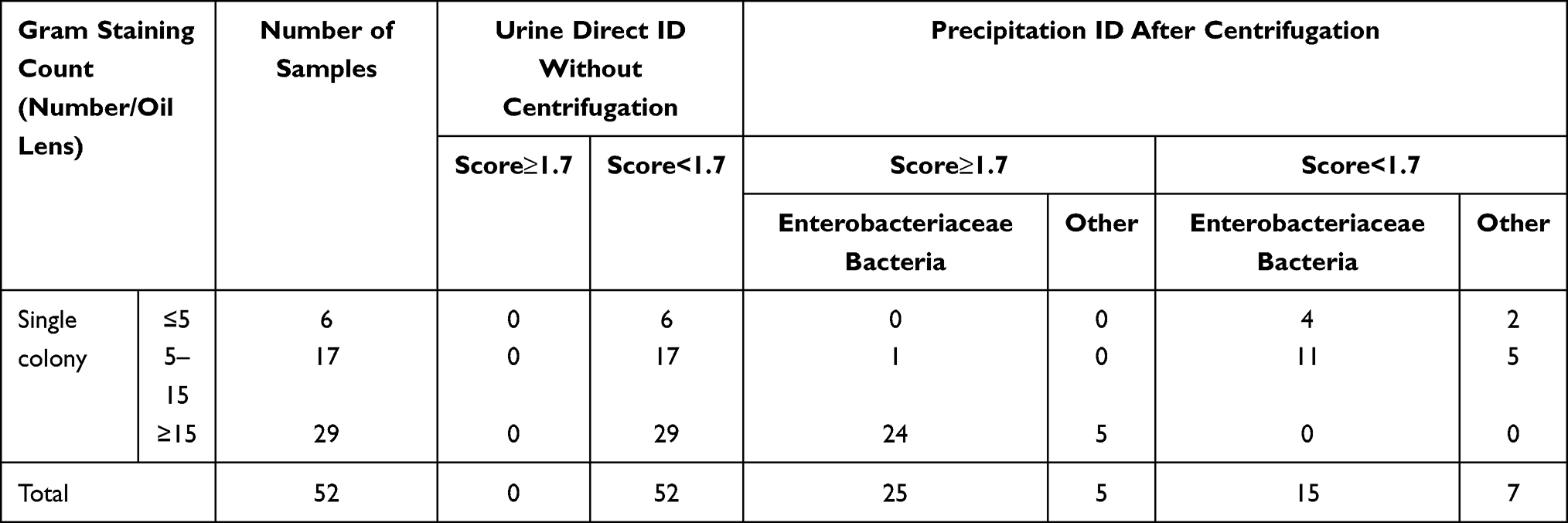 |
Table 1 Gram Staining Classification and MS Identification of Urine Samples |
 |
Table 2 Time of Biofilm in Short-Term Culture of Enterobacteriaceae Bacteria (Score<1.7) |
Comparison of MIC Results Using DOT-MGA and Broth Microdilution Method
The MIC50 for IPM, LEV, CAZ, NIT, and FOT by DOT-MGA and broth microdilution method were ≤1/≤0.5, >2/2, ≤4/≤2, ≤32/≤16, ≤64/≤32 and the MIC90 were ≤1/≤0.5, >2/>4, 16/16, 128/128, 128/64, respectively. The detailed results are shown in Appendix Table 1 and the results of MIC50, MIC90 and MIC range are shown in Table 3.
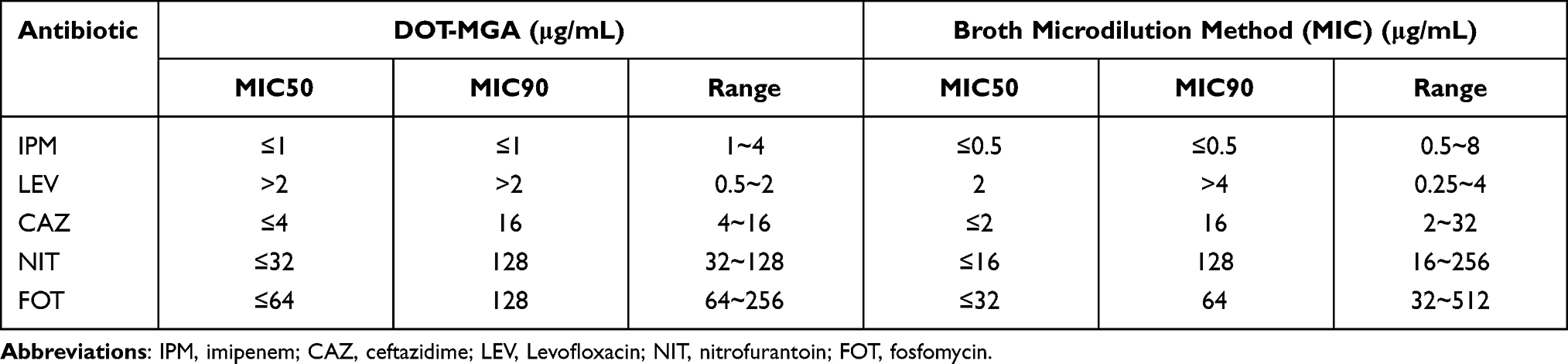 |
Table 3 MIC50, MIC90 and MIC Range for Each Antibacterial Drug of Two Methods |
Concordance Rates of DOT-MGA Method and Broth Microdilution Method
Compared with the broth microdilution method, the EA and CA for IPM, LEV, CAZ, NIT, and FOT of DOT-MGA method are 100%/100%, 98%/90%, 98%/92%, 100%/90%, and 98%/94%, respectively. There was no VME observed in all five types of antibacterial drugs (as shown in Table 4).
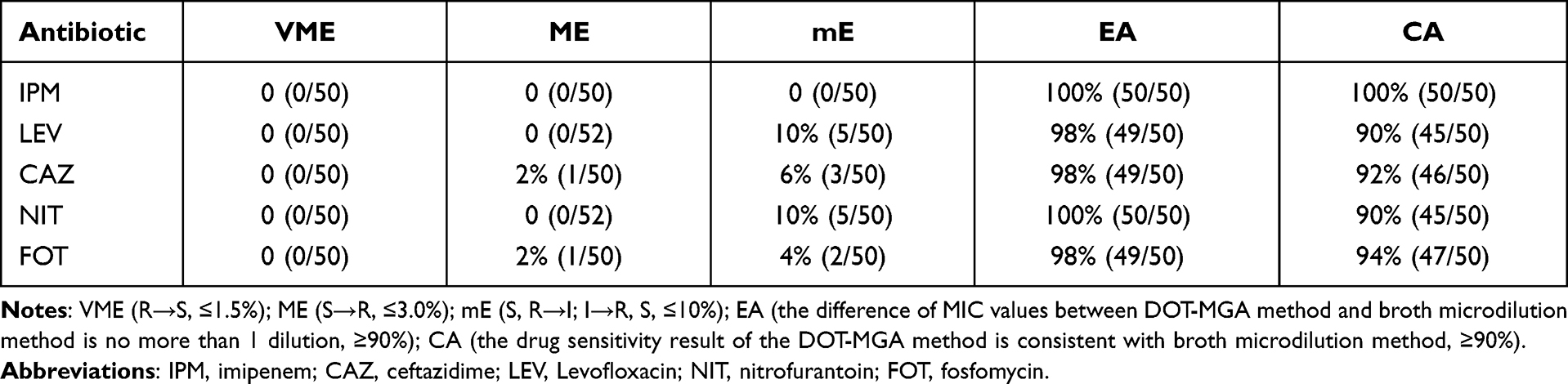 |
Table 4 The Concordance Rates of DOT-MGA Method and Broth Microdilution Method |
Greatly Reduced TAT
The TAT of our research methods, which contains ID (0.5–6h) and AST (4h) was 5–10h. While the traditional method needed 36–48h (as shown in Table 5).
 |
Table 5 TAT of Two Methods |
Discussion
The number of patients with urinary tract infections is increasing every year all over the world. The emergence of drug-resistant bacteria makes the treatment of urinary tract infections even difficult.17 Regular urine pathogen ID and AST requires at least 48–72h.7,8 This delayed treatment will lead to the dominant growth of drug resistant bacteria and inappropriate treatment. Therefore, it is particularly important to find a faster method to identify pathogens and test drug sensitivity in urinary tract infection.
Performing urine smear at the initial steps has obvious advantages. For samples with three types of bacteria, patients can be quickly informed for re-collection; for the samples with no observed bacteria, the culture result usually shows no obvious bacterial growth, which is equivalent to negative result; the time required for the ID and AST of the infected samples is also greatly reduced, which can significantly shorten the patients’ waiting time compared with the samples processed by the regular procedure. Not all urine can be identified directly. We need to evaluate it before proceeding to the next step. For urine with high bacterial count, by grouping and pre-treatment, we can obtain the ID results of pathogens as soon as half an hour. For urine with low bacterial count, we can obtain bacterial membrane through short-term culture for ID. This greatly shortens the ID time from 18–24h to 0.5–5h. After the 4h incubation of DOT-MGA, the pathogen sensitivity to antibacterial drugs can be predicted. Compared with the broth microdilution method, CA is more than 90%; VME, ME, and mE all meet the ISO requirements of ≤1.5%, ≤3.0%, and ≤10%, respectively.14 We also calculated the MIC50 and MIC90 of each antibiotic in the two methods. The indexes are basically the same.
The data suggest that this method can replace the micro broth dilution method. In this experiment, the drug sensitivity test can be shortened from 18–24h to 4–5h. In terms of time, it is also much better than the micro broth dilution method.The all results show that this research method has great advantages.
The method developed by this study can shorten the ID time the AST time, which reduces the starting time of effective antibacterial therapy to 5–10h. It will be possible reduces inpatient days and cost, improves prognosis, avoid chronic disease, and reduces complications. The rapid and accurate drug sensitivity data provide fundamental support for clinicians’ precise treatment, which can significantly avert the overuse of antibacterial drugs in the treatment of urinary tract infections. Next, we will study the application of this research method in many of the above aspects.
This study also improved the previously reported urine collection method. In the study by Li et al15 the differential centrifugation was carried out at 2000g for 1 minute, and after the last washing step, the samples were centrifuged at 10000g for 2 minute. In the study by Nix et al12 two different differential centrifugation protocols were compared. They found that the starting time of bacterial growth delayed by 2 hours when centrifuged at 2000 rpm 5 minutes compared to the samples centrifuged for 2 minutes. We speculate that centrifugation at 2000 rpm may cause premature precipitation of some bacteria, which would reduce the collection rate. Changing the centrifugation parameters to 2000 g for 2 minutes can better remove white blood cells, cell debris, and mucus, while maintaining a high collection rate. We also adjusted the centrifugation time to 5 minutes for the last two centrifugation steps, our results showed better bacteria collection rate.
The operation method of this research scheme is simple and does not need special instruments and technical personnel, so it is easy to carry out in the basic laboratory. In the existing reports, Li et al15 and Zboromyrska et al6 used flow cytometry to count the number of pathogens in urine samples and performed MALDI-TOF MS identification. They all need flow cytometry and professional operators, and the detection cost is high. The approach reported by this study only requires mass spectrometer, regular microscopy, and Gram staining, which is easy to carry out in most of the clinical laboratories.
The newly developed DOT-MGA method is a rapid AST based on the general phenotype of MALDI-TOF MS, which has been shown by many studies to be useful for predicting the bacterial sensitivity and resistance to specific antimicrobials.16 However, DOT-MGA can be used to predict AST only in the case of a single pathogen infection.And numerous studies have shown that for DOT-MGA, the growth rate of non-fermenting bacteria and Gram-positive cocci is relatively slow, which requires a long incubation time. Therefore, we chose the most common Enterobacteriaceae bacteria in urinary tract infection for the AST experiment. Samples with mixed infections, fungal infections, Gram-positive cocci infections, and non-fermenting bacterial infections were not included in this study. In the future, we will continue to study these aspects to evaluate the application value of this method in the diagnosis of urinary tract infection.
What’s more, most of the existing studies used the intermediate or resistance breakpoint as the drug concentration in distinguishing sensitive strains from resistant strains. By referring to the CLSI M100 document filed in 2019, we determined the sensitivity/intermediate/resistance breakpoints of five antibacterial drugs, which provide precise options for the treatment of patients infected with resistant strains. For example, for multi-resistant strains, intermediary drugs could be used in the treatment by increasing dosage, shortening interval, and/or extending the period of infusion.
In addition, there is no standard procedure for the pre-treatment of sterile samples before ID and the droplet volume and incubation time of the DOT-MGA method. So different researchers may use modified operating protocols, which may cause differences in experimental results. Moreover, how to improve the culture efficiency of gram-positive cocci and fungi in DOT-MGA is also the problem we need to study in the next step. In order to detect faster and carry out more conveniently in the laboratory, the commercialized production of disposable target plates containing antibiotics will be of great value.
Conclusion
This method is superior to the conventional method for the identification of single bacteria in the urinary tract. Compared with the micro broth dilution method, the consistency of the results of drug sensitivity test was more than 90%. The detection time is also much better than the conventional method. The ID and AST methods in this experiment have the advantages of short detection time, low cost, easy operation and accurate results, which can replace the conventional methods and can be popularized and applied in major laboratories.
Ethical Approval
This study involved anonymous use of redundant, abandoned patient urine after laboratory testing, with no contact with the patient, and there was no patient identification performed during data collection. This research does not affect patients’ health and privacy. Therefore, the ethics committee determined that informed consent was not required. The Ethics approval was obtained from the medical ethics committee of Anhui Medical University with the following reference number: LLSC20210802.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was funded through a grant from Anhui Provincial Department of Education for University cooperative research and public health collaborative innovation project in Anhui Province in 2020 (Grant No. GXXT-2020-016) and a grant from Anhui Provincial Health Commission for key scientific research projects in 2021 (Grant No. AHWJ2021a011) and major natural science research projects of colleges and universities in Anhui Province in 2021 (Grant No. KJ2021ZD0032).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flores-Mireles AL, Walker JN, Caparon M, et al. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269–284. doi:10.1038/nrmicro3432
2. McLellan LK, Hunstad DA. Urinary tract infection: pathogenesis and outlook. Trends Mol Med. 2016;22(11):946–957. doi:10.1016/j.molmed.2016.09.003
3. Terlizzi ME, Gribaudo G, Maffei ME. UroPathogenic Escherichia coli (UPEC) infections: virulence factors, bladder responses, antibiotic, and non-antibiotic antimicrobial strategies. Front Microbiol. 2017;8(15):1566. doi:10.3389/fmicb.2017.01566
4. Yan Y, Meng S, Bian D, et al. Comparative evaluation of Bruker Biotyper and BD Phoenix systems for identification of bacterial pathogens associated with urinary tract infections. J Clin Microbiol. 2011;49:3936–3939. doi:10.1128/JCM.05363-11
5. Zugravu R, Licker M, Berceanu-Va ˘duva D, et al. The establishment of resistance phenotypes for bacteria isolated from outpatients in urine cultures. Roum Arch Microbiol Immunol. 2006;65:93–99.
6. Zboromyrska Y, Rubio E, Alejo I, et al. Development of a new protocol for rapid bacterial identification and susceptibility testing directly from urine samples. J Clin Microbiol Infect. 2016;22:
7. DeMarco ML, Burnham C-AD. Diafiltration MALDI-TOF mass spectrometry method for culture-independent detection and identification of pathogens directly from urine specimens, American Society for Clinical Pathology. Am J Clin Pathol. 2014;141:204–212. doi:10.1309/AJCPQYW3B6JLKILC
8. Wang X-H, Zhang G, Fan -Y-Y, et al. Direct identification of bacteria causing urinary tract infections by combining matrix-assisted laser desorption ionization-time of flight mass spectrometry with UF-1000i urine flow cytometry. J Microbiol Methods. 2013;92:231–235. doi:10.1016/j.mimet.2012.12.016
9. Neonakis IK, Spandidos DA. MALDI-TOF MS-based direct-on- target microdroplet growth assay: latest developments. Exp Ther Med. 2020;20(3):2555–2556. doi:10.3892/etm.2020.8976
10. Neonakis IK, Spandidos DA. MALDI-TOF mass spectrometry-based direct-on-target microdroplet growth assay: a novel assay for suscept-ibility testing and beyond. Future Microbiol. 2019;14(9):729–731. doi:10.2217/fmb-2019-0106
11. Idelevich EA, Storck LM, Sparbier K, Drews O, Kostrzewa M, Becker K. Rapid direct susceptibility testing from positive blood cultures by the MALDI-TOF MS-based direct-on-target microdroplet growth assay. J Clin Microbiol. 2018;56:e913–e918.
12. Nix ID, Idelevich EA, Storck LM. Detection of methicillin resistance in Staphylococcus aureus from agar cultures and directly from positive blood cultures using MALDI-TOF mass spectrometry-based direct-on-target microdroplet growth assay. Front Microbiol. 2020;11:232. doi:10.3389/fmicb.2020.00232
13. Tang H, Li R, Xu H, et al. Direct-on-target microdroplet growth assay for detection of bacterial resistance in positive blood cultures. Infect Drug Resist. 2021;14:4611–4617. doi:10.2147/IDR.S336987
14. International Standards Organisation. Clinical laboratory testing and in vitro diagnostic test systems d Susceptibility testing of infectious agents and evaluation of performance of antimicrobial susceptibility test devices. Part 2: evaluation of antimicrobial susceptibility test devices. 2007:ISO20776e2.
15. Li W, Sun E, Wang Y, et al. Rapid identification and antimicrobial susceptibility testing for urinary tract pathogens by direct analysis of urine samples using a MALDI-TOF MS-based combined protocol. Front Microbiol. 2019;10:1182. doi:10.3389/fmicb.2019.01182
16. Idelevich EA, Sparbier K, Kostrzewa M, Becker K. Rapid detection of antibiotic resistance by MALDI-TOF mass spectrometry using a novel direct-on-target microdroplet growth assay. Clin Microbiol Infect. 2018b;24:738–743. doi:10.1016/j.cmi.2017.10.016
17. Öztürk R, Murt A. Epidemiology of urological infections: a global burden. World J Urol. 2020;38(11):2669–2679. doi:10.1007/s00345-019-03071-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.