")
Back to Journals » Infection and Drug Resistance » Volume 13
Raoultella ornithinolytica: Emergence and Resistance
Authors Hajjar R, Ambaraghassi G , Sebajang H, Schwenter F, Su SH
Received 23 September 2019
Accepted for publication 13 December 2019
Published 15 April 2020 Volume 2020:13 Pages 1091—1104
DOI https://doi.org/10.2147/IDR.S191387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Roy Hajjar,1,* Georges Ambaraghassi,2,* Herawaty Sebajang,1 Frank Schwenter,1 Shih-Hann Su2
1Digestive Surgery Service, Department of Surgery, Centre Hospitalier de l’Université de Montréal (CHUM), Montréal, Québec, Canada; 2Department of Medical Microbiology and Infectious Diseases, Centre Hospitalier de l’Université de Montréal (CHUM), Montréal, Québec, Canada
*These authors contributed equally to this work
Correspondence: Roy Hajjar; Georges Ambaraghassi
Centre Hospitalier de l’Université de Montréal, 1000, Rue Saint-Denis, Montréal, Québec H2X 0C1, Canada
Tel +1 514 890 8000
Email [email protected] [email protected]
Abstract: Raoultella ornithinolytica is an encapsulated Gram-negative, oxidase-negative, catalase-positive, aerobic, non-motile rod that belongs to the Enterobacteriaceae family. This bacterium was initially classified in the genus Klebsiella as Klebsiella ornithinolytica, until the creation of the genus Raoultella in 2001. R. ornithinolytica is usually found in water environments and soil, and due to its ability to convert histidine to histamine, it has been associated with histamine poisoning in humans. R. ornithinolytica is an emerging entity in human infections, with several reports of virulent infections in comorbid at-risk patients. Increasing reports are potentially due to better and more precise identification tools. The objective of this article is to provide a comprehensive review of reported cases of R. ornithinolytica infections, the emergent virulence of described multiresistant strains, and an overview of currently used identification methods.
Keywords: Raoultella ornithinolytica, Raoultella spp., infection, resistance
Background
Raoultella ornithinolytica is an encapsulated Gram-negative, oxidase-negative, catalase-positive, aerobic, non-motile rod that belongs to the Enterobacteriaceae family.1–5 It was initially classified in cluster II of the genus Klebsiella as Klebsiella ornithinolytica along with other environmental organisms comprising Klebsiella terrigena, Klebsiella planticola and Klebsiella trevisanii.2,3 With advanced phylogenetic testing including 16S rRNA and rpoB sequence analysis, the genus Klebsiella was further divided into two genera.3 Thus, in 2001, the genus Raoultella was created and species included in the cluster II of the genus Klebsiella were transferred and renamed to the new genus.3,6 The Raoultella genus is named after Didier Raoult, a French bacteriologist from the Université de la Méditerranée in Marseille, France.3
R. ornithinolytica has been found in water environments, soil, insects, fish, ticks and termites.3,5,7–11 This bacterium converts histidine to histamine causing histamine poisoning with cutaneous flushing, better known as the scombroid syndrome associated with fish poisoning.7,9 In addition to skin flushing, this syndrome may cause vomiting, diarrhea, headache or pruritus depending on the quantity of ingested histamine.11,12 This syndrome is mainly associated with “scombroid” fish belonging to the Scombridae and Scomberesocidae families where exogenous microbial decarboxylation of histidine occurs.12–14
The incidence of human disease associated with R. ornithinolytica is low with few previously reported cases of clinical infections requiring treatment. The low prevalence of R. ornithinolytica related infections in the literature might be explained by the challenges and difficulty to properly identify this species with conventional biochemical and phenotypic tests. Similarly to other members of the Enterobacterales order, such as Aeromonas, Plesiomonas and Leclercia and non-fermenting Gram-negative bacteria, such as Stenotrophomonas maltophilia, Burkholderia cepacia complex and Alcaligenes faecalis, due to the scarcity of reported cases, the associated pathogenicity and antibiotic susceptibility testing remain overlooked.15–18 Nonetheless, there is a rapidly emerging role for R. ornithinolytica in human infections, with some multi-drug resistant strains being increasingly reported.4,11,19
Objective
The objective of this paper is to provide a comprehensive review of available current knowledge on the emerging role of R. ornithinolytica in human infections, its virulence and resistance to antibiotic treatment.
Data Sources
A literature review was performed in Medline, Pubmed and Embase, using the expressions “Raoultella ornithinolytica” and “Raoultella spp.”, to identify reported cases of infections with Raoultella ornithinolytica. The references of identified publications were also reviewed for the identification of relevant cases.
Identification
Adequate identification of Raoultella species remains a challenge with conventional identification methods.1 It is suggested that R. planticola can represent up to 19% of misidentifications of Klebsiella and Raoultella species with conventional testing.20–22
R. ornithinolytica and R. planticola are two closely related species and differentiating them with phenotypic methods is difficult. Data collected from studies with 16S rDNA sequencing did show high DNA homology between R. ornithinolytica and R. planticola, with these bacteria bound in a tight cluster. Few phenotypic tests are available to differentiate these two species. Ornithine decarboxylase (ODC) was proposed for instance to provide a potential separation tool.23 While R. planticola has been reported as ODC negative, R. ornithinolytica is ODC positive.24,25 However, ODC-negative R. ornithinolytica has nonetheless been described and such isolates can be misidentified as R. planticola and Klebsiella oxytoca.24 Indole production is another biochemical test that can be helpful in distinguishing between R. ornithinolytica and R. planticola. While R. ornithinolytica is indole-positive, R. planticola is indole variable.24,25 Moreover, previous studies have reported cases of incorrect identification of R. ornithinolytica as K. oxytoca. Park et al (2011) conducted a study comparing three identification systems (VITEK®2, MicroScan and API 20E) for the identification of R. ornithinolytica and K. oxytoca.24 Among R. ornithinolytica isolates identified with sequence-specific primer PCR, VITEK®2 provided 100% correct identification of R. ornithinolytica, while Microscan and API 20E identified 92.6% and 88.9% of the isolates as Klebsiella oxytoca.24 Novel techniques, such as lateral-flow test strips, have been developed for rapid detection of R. ornithinolytica and closely related species and have showed favorable results. To our knowledge, this technology has been mainly applied to the food industry.26
While phenotypic-based identification systems yielded conflicting results for distinguishing K. oxytoca from R. ornitholytica, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) has allowed better characterization and detection with improved differentiation between Klebsiella and Raoultella spp.1,27 This technology was used in our previous work to properly identify R. ornithinolytica in a patient with gut-derived sepsis.28 However, because mass spectra from R. ornithinolytica and R. planticola are highly similar, difficulty in differentiating between these two species has been reported with MALDI-TOF technology.29,30 Misidentification as Enterobacter aerogenes (now Klebsiella aerogenes) has also been reported with the use of MALDI-TOF.29 This could be potentially explained by the fact that K. aerogenes is closely related to Raoultella species (formerly environmental Klebsiella species) in the phylogenetic tree derived from 16S rDNA sequencing.3,23,31
Virulence and Resistance
As stated by Haruki et al (2014), R. ornithinolytica was thought to be highly virulent due its occurrence in fragile patients with significant comorbidities and its initial association with the Klebsiella genus, which comprises several virulent strains.33 However, according to previously reported cases, prognosis in highly variable and depends on the patient’s overall health status and the type of infection, and outcomes are not necessarily poor when proper treatment is promptly initiated.33
Most species in the genus Raoultella are usually broadly sensitive to antibiotics based on the isolates from case series in the literature.34 Similarly to some Klebsiella species, Raoultella spp. exhibit intrinsic resistance to ampicillin and ticarcillin which are the result of chromosomally encoded beta-lactamases.34–37 Chun et al (2015) reported a series of 16 patients with isolates showing antibiotic susceptibility to cephalosporins ranging from 69% to 100%, 93% susceptibility to amoxicillin/clavulanic acid, 88% to trimethoprim/sulfamethoxazole (TMP-SMX) and 100% to meropenem, imipenem and piperacillin/tazobactam.4 Seng et al (2016) reported, in the largest series published, that resistance to amoxicillin/clavulanic acid, ceftriaxone, quinolones, TMP-SMX and aminoglycosides were 16%, 4%, 6%, 10 and 1% respectively.1 No resistance to imipenem-cilastatin was reported.1 Multidrug resistant R. ornithinolytica, with acquired antibiotic resistance genes, has nonetheless been isolated in clinical specimens. Production of beta-lactamases remains the most frequently described mechanism of resistance. Strains exhibiting beta-lactamases from Ambler class A, B and D have been reported. Several case reports have described isolates producing extended-spectrum beta-lactamases belonging to the SHV, TEM and CTX-M.34,38,39 AmpC beta-lactamases producing strains were also isolated from clinical specimens in Iraq.40
In the last decade, several emerging cases of carbapenem resistance were described.41 The first case of the blaKPC carbapenemase-encoding gene in R. ornithinolytica was reported by Castanheira et al (2009) in a postoperative infection after a valve replacement surgery.42 The authors reported the presence of this resistance factor in several Raoultella spp. including R. planticola and R. ornithinolytica, with fatal outcomes in all 3 patients.42 Other carbapenemase-harboring strains were reported in the following years.34,43 The first case of blaNDM-1 in R. ornithinolytica was described in 2013 by Khajuria et al in an adult male patient with postoperative perineal infection, who recovered well with an appropriate antibiotic treatment.44 Other cases of metallo-beta-lactamase-producing R. ornithinolytica harboring NDM or VIM genes were reported since then.41,45–48 An IMI-producing R. ornithinolytica strain acquired by a transposon was also isolated from a clinical sample in China.49 Isolated cases of carbapenemase blaOXA-48-harboring R. ornithinolytica harvested from a surgical site infection in South America and the fecal sample of a patient with Hodgkin lymphoma in Lebanon were also reported.50,51 Other Raoultella species were also described as exhibiting OXA-48 carbapenemase.52–55 Nonetheless, a few strains of R. ornithinolytica generating simultaneously different types of beta-lactamase (TEM, SHV, KPC and OXA) were described.42,56 The first case of co-existence of blaKPC-2 and blaIMP-4 carbapenemase genes in the genus Raoultella was reported by Zheng et al (2015) in a 13-year-old male patient with postoperative infection after an orthopedic surgery.57 The R. ornithinolytica strain was identified in this report by 16S rRNA sequencing and antimicrobial susceptibility was determined with VITEK®2 and Etest strips (Bioméreux, France) on 7 samples collected from the wound fluid and necrotic tissue.57 The isolated strains were reported as resistant to all antimicrobials except ciprofloxacin. All but one strain were also susceptible to TMP-SMX.57
Since the emergence of plasmid-mediated polymyxin resistance by the mcr-1 gene, the latter, along with other mcr resistance genes, have been isolated in many Enterobacteriaceae in different continents.58,59 The mcr gene has rarely been isolated in R. ornithinolytica strains, with the first cases being found in retail vegetables in China.60 Furthermore, emergence of mcr-8 gene and variant was also identified in R. ornithinolytica which raised concern about its co-transferability with other beta-lactamase genes.58,61
Gastrointestinal and Hepatobiliary Infections
Gastrointestinal and hepatobiliary infections are among the most frequently reported infections with R. ornithinolytica in the literature. Fully detailed cases are depicted in Table 1.
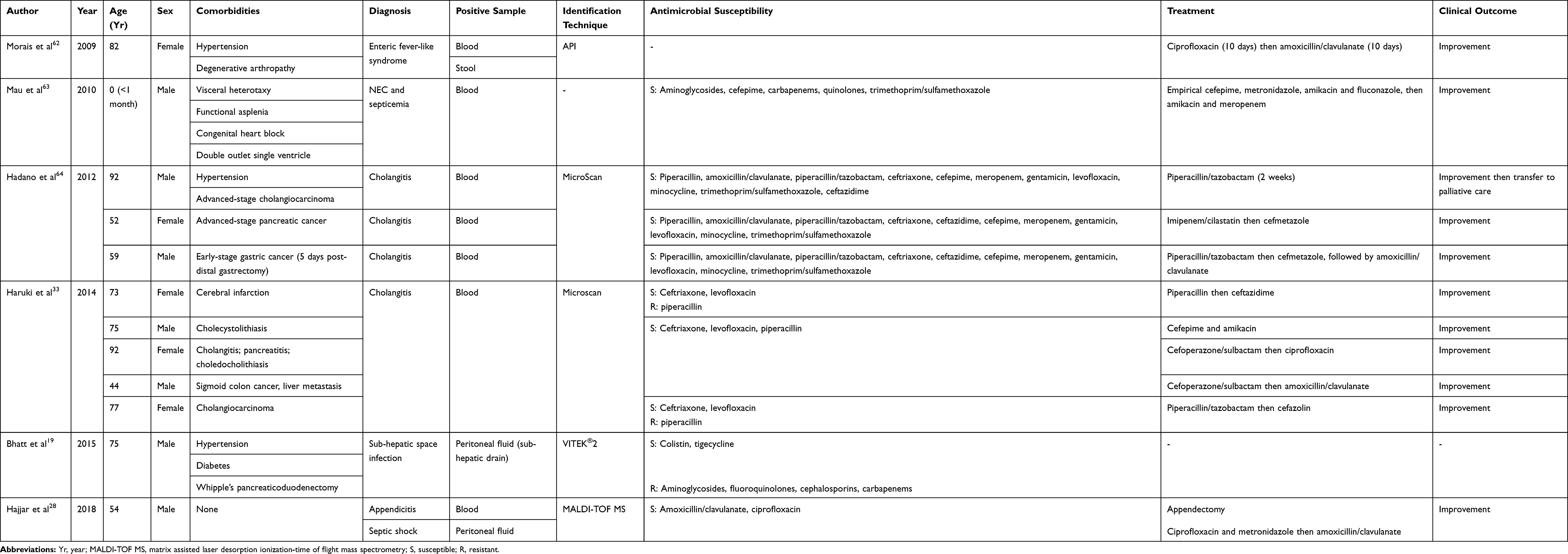 |
Table 1 Reported Cases of Gastrointestinal Infections with Raoultella ornithinolytica |
Bhatt et al reported in 2015 a case of postoperative intra-abdominal infection with R. ornithinolytica after a Whipple’s pancreaticoduodenectomy.19 The author identified a multiresistant strain harboring the New Delhi metallo-b-lactamase gene (blaNDM) in sub-hepatic peritoneal fluid.19 The presence of blaNDM gene was reported only once before, by Khajuria et al (2013) in a patient with a R. ornithinolytica soft tissue infection.44
Seng et al (2016) described, in a series of 112 cases of R. ornithinolytica infections in 4 French university hospitals, 16 cases of gastrointestinal infections with 6 being hospital-acquired.1 The majority of these cases consisted of hepatobiliary and pancreatic infections.1 R. ornithinolytica was also isolated, among other bacteria, in fish fillets potentially involved in an incident of foodborne poisoning in southern Taiwan.12
Chun et al (2015) reported 7 patients with biliary infection in a review of 16 cases of R. ornithinolytica bacteremia.4 All patients had a malignancy except one who suffered from end-stage renal disease on peritoneal dialysis.4 The latter presented with peritoneal dialysis-related peritonitis and R. ornithinolytica was isolated in the dialysate.4
Reported cases of gastrointestinal, and specifically biliary, infections with R. ornithinolytica are often depicted as affecting mainly individuals with an altered immune system either by a malignant condition or a chronic disease. Nonetheless, rare cases involving healthy patients with no identifiable risk factors exist, and usually present as food poisoning and acute gastroenteritis.12,28
Urological Infections
Cases of urinary tract infection (UTI) with R. ornithinolytica are very scarce. Table 2 summarizes the previously detailed cases of UTIs with this pathogen. Among other reported cases, Vos et Laureys (2009) described a case of an infected giant renal cyst causing colonic obstruction and an inflammatory syndrome.65 Chun et al (2015) reported in his case series 2 cases of urosepsis in patients with diffuse large B cell lymphoma and bladder cancer respectively.4 One patient was treated with piperacillin/tazobactam and azithromycin, and the second with imipenem/cilastatin and vancomycin.4 In the latter, a coinfection with Enterococcus faecalis was found.4 The outcome was death in both cases.4 In non-English literature, reported cases include urinary tract infections with R. ornithinolytica in patients with malignancies.66
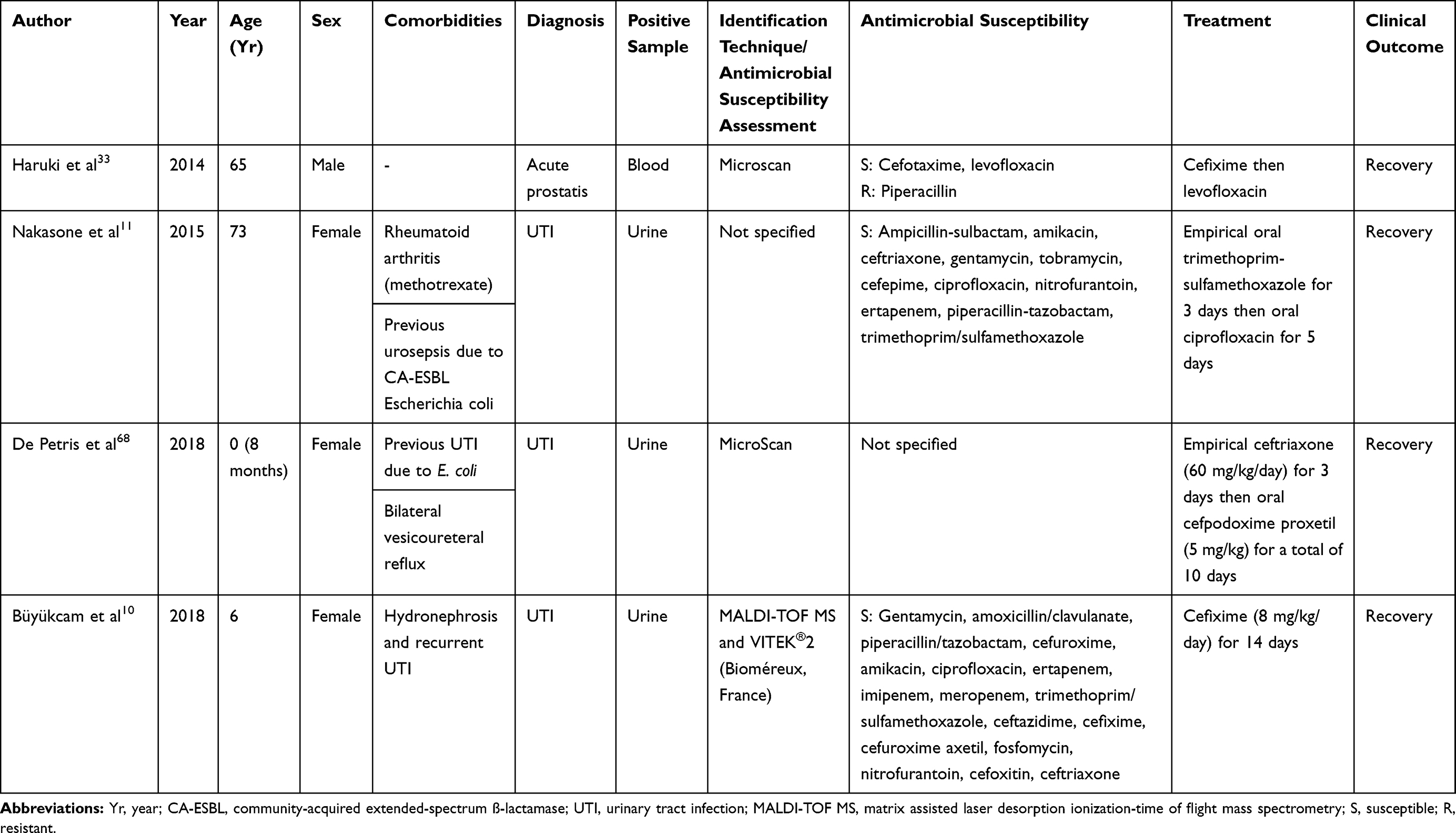 |
Table 2 Reported Cases of Urinary Tract Infections with Raoultella ornithinolytica |
Seng et al (2016) reported in his series of 112 cases 36 urinary infections with R. ornithinolytica, including 20 cases of cystitis, 8 cases of pyelonephritis, 5 cases of prostatitis and 3 cases of renal cyst infection.1 Furthermore, Boattini et al (2016) reported 9 cases of cystitis due to R. ornithinolytica.67
It is worth noting that many of the reported cases were diagnosed in patients with either immunodeficiency, malignant conditions or anatomical abnormalities, thus making them complicated rather than simple community-acquired infections.
Osteoarticular Infections
Very few reports of osteoarticular infections with R. ornithinolytica have been published in the literature. Table 3 describes the reported detailed cases of such infections. Seng et al (2016) reported 4 cases of bone and joint infection, including 3 cases of chronic osteitis without orthopedic device and 1 case of tibia pandiaphysitis.1 These cases were community-acquired.1
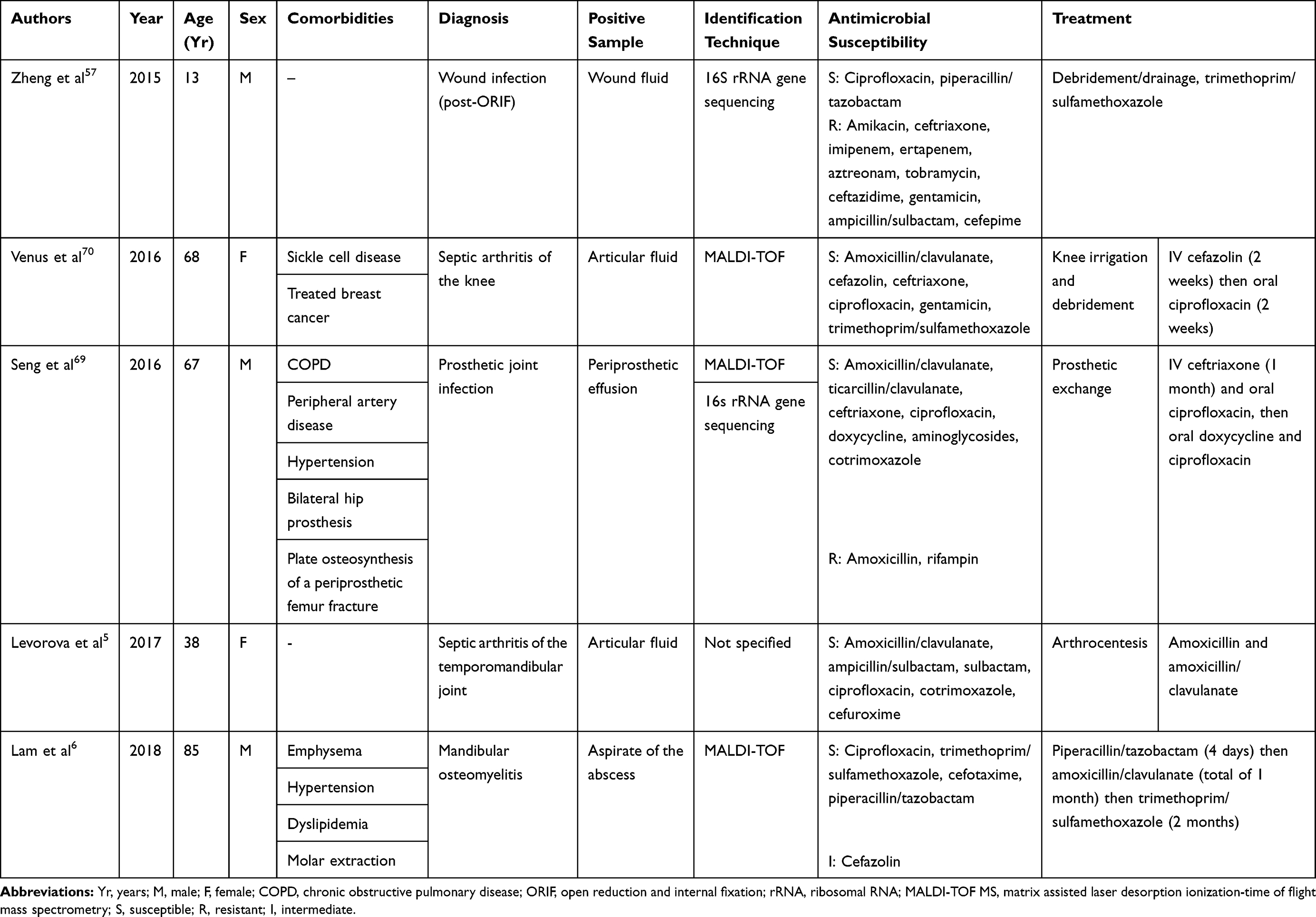 |
Table 3 Reported Cases of Osteoarticular Infections with Raoultella ornithinolytica |
Although several patients in the previously reported cases had multiples comorbidities, none of them appeared to have an active immunosuppressive condition. The clinical presentation and symptoms did not significantly differ from, nor were they more severe than, the cases of osteoarticular infections caused by other pathogens. Furthermore, the majority of cases responded adequately to treatment, the latter consisting usually of debridement and lavage of the affected joint and subsequent prolonged antimicrobial therapy.69 Although response to standard treatment was frequently reported as satisfactory, amputation was previously required to control the infection.69
While some cases may suggest that a prior intervention may have led to infection, other cases were described in immunocompetent patients with no identifiable entry points. Nonetheless, osteoarticular manifestations account for a minority of infectious events with Raoultella ornithinolytica in the literature.
Ear, Nose and Throat Infections
Singh et al (2017) reported a case of ENT infection in a 70-year old female patient with history of tobacco chewing, presenting as pain in the throat and ear, postnasal discharge and voice change.71 The bacterium was identified on throat swab cultures, and antimicrobial susceptibility was determined using the VITEK®2 system.71 The cultured strain was susceptible to piperacillin/tazobactam, ertapenem, amikacin, gentamicin, nalidixic acid, ciprofloxacin, norfloxacin, cefixime, ceftazidime, ceftriaxone and TMP-SMX, and resistant to amoxicillin/clavulanic acid, fosfomycin and cefoxitin.71 The patient received an initial empirical treatment of amoxicillin/clavulanic that was changed to piperacillin/tazobactam and subsequently ciprofloxacin, with clinical improvement.71
In a study aiming at identifying pathogenic bacteria in the saliva of individuals wearing dentures, Derafshi et al (2017) reported 2 cases where R. ornithinolytica was isolated.72 No clinical repercussions or related infections with this pathogen were however described in this cohort.72 In another study aiming at identifying sulphate-reducing bacteria in saliva samples, R. ornithinolytica was isolated in one smoker patient with no local or systemic infection.73
To the best of our knowledge, the only described cases of R ornithinolytica ENT infections include the one reported by Singh et al (2017), and 2 cases of external otitis (one of which hospital-acquired) reported by Seng et al (2016).1,71 The presence R. ornithinolytica in human saliva samples points to its potential role in infection pathogenicity. More cases are however required to better understand the clinical characteristics and risk factors of such infections in the ENT sphere.
Soft Tissue Infections
The first case of cutaneous soft tissue infection with R. ornithinolytica was reported by Solak et al (2011) in a patient with diabetic foot infection that presented with fever, weakness and a maculopapular rash.9 The pathogen was isolated from a wound specimen and identification was done with the VITEK®2 system (Bioméreux, France).9 The patient, who had diabetes, hypertension and chronic kidney disease (CKD), improved after being treated initially with piperacillin/tazobactam then tigecycline after antibiotic susceptibility testing reported that the strain was susceptible only to ertapenem, levofloxacin, and tigecycline.9
Another diabetic foot infection with R. ornithinolytica was reported later by Kabbara et al (2015) in a 68-year old male patient.7 The patient’s past medical history included hypertension, diabetes and CKD.7 The pathogen was identified in cultures from the ankle wound,7 was susceptible to amoxicillin/clavulanate, cefepime, ceftazidime, ceftriaxone, ciprofloxacin, gentamicin, imipenem/cilastatin, piperacillin/tazobactam and TMP-SMX, and resistant to cefazolin.7 The patient was thus successfully treated with amoxicillin/clavulanate.7
Furthermore, Khajuria et al (2013) identified a multi-drug resistant strain of R. ornithinolytica in a perineal surgical site infection that was susceptible only to tigecycline and colistin.44 It is worth noting that the surgical procedure in this patient was performed to repair a perineal injury with urethral rupture.44 Another case of surgical site infection was recently reported in a 64-year-old male patient after an ileocecal resection.50 The identified strain was susceptible to third generation cephalosporins and ciprofloxacin and the patient recovered adequately with appropriate antibiotic treatment.50
Although most soft tissue infections were reported in patients with comorbidities increasing their risk of infectious events, such as diabetes, a first case of surgical wound infection with R. ornithinolytica was reported in a 24-year-old healthy female patient after a bilateral breast reduction surgery.74 In this case, R. ornithinolytica was present in a polymicrobial wound culture including Escherichia coli and Enterococcus faecalis as well, and was treated with bilateral debridement and antibiotic therapy.74 Furthermore, Seng et al (2016) reported in their series 15 cases of skin and wound infection, with 8 cases being hospital-acquired.1
Intrathoracic and Respiratory Infections
Detailed cases of intrathoracic and respiratory infections with R. ornithinolytica are shown in Table 4. Boattini et al (2016) reported in a retrospective analysis 6 cases of pneumonia due to R. ornithinolytica.67 Previous cases of pneumonia or pleural effusions, both community- and hospital-acquired, have also been reported.1 Seng et al (2016) further described 1 and 2 cases of hospital-acquired pericarditis and mediastinitis respectively.1 Sener et al (2011) published a case of fever of unknown origin in a 16-month-old female patient presenting as fever and persistent cough, in whom R. ornithinolytica was identified in bronchoalveolar lavage fluid.13 Previous detailed cases depict patients with postoperative infections or admitted to the intensive care unit (ICU) with severe systemic alterations. The presence of respiratory infections with R. ornithinolytica in the community seems to be extremely uncommon especially in healthy immunocompetent individuals.
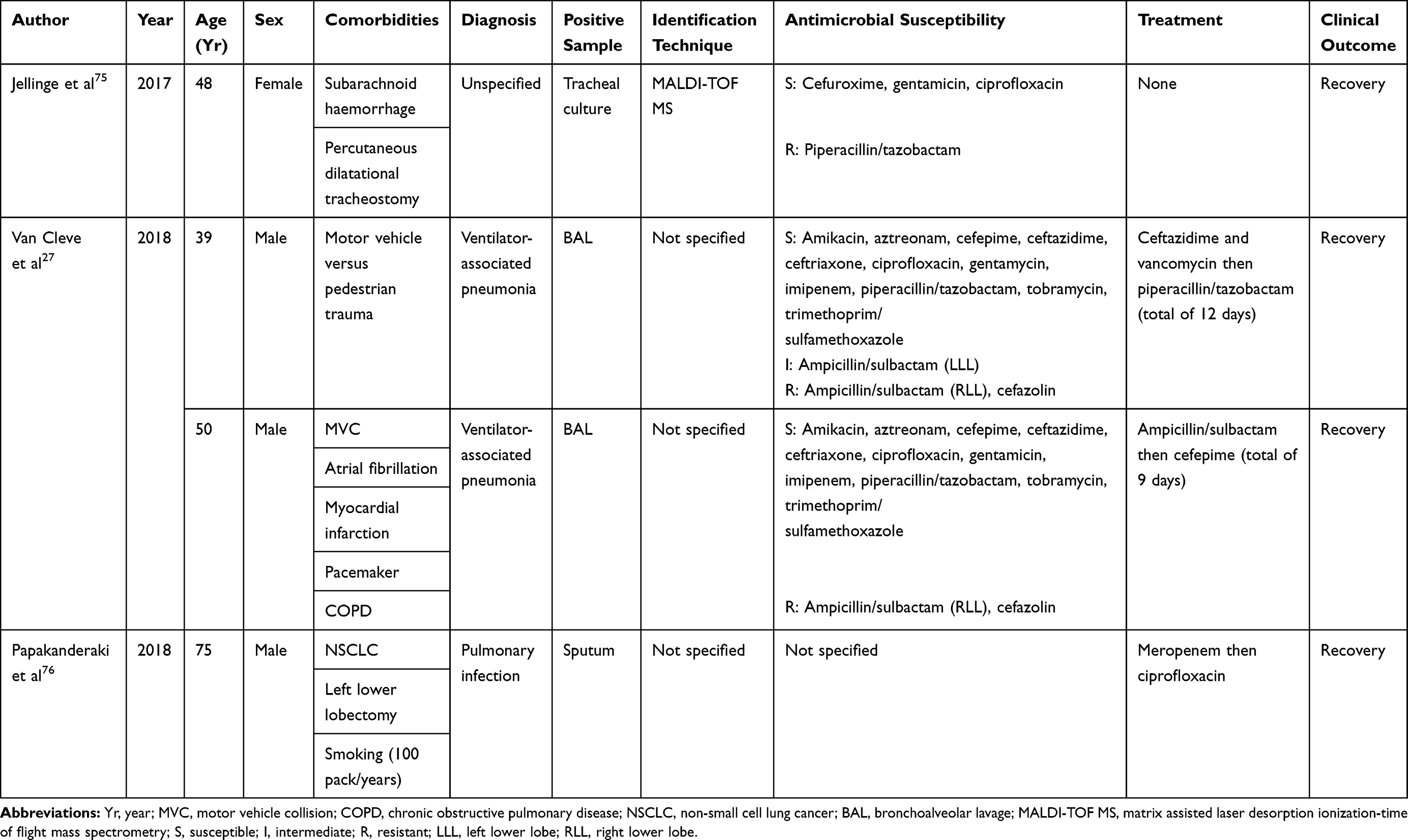 |
Table 4 Reported Cases of Intrathoracic and Respiratory Infections with Raoultella ornithinolytica |
Bloodstream and Other Infections
In addition to previously mentioned reports, several cases of systemic infections with R. ornithinolytica, presenting mainly as bacteremia with a septic status, have been reported without a source being identified. Although recovery was achievable in many of these cases, death occurred in many of them and several reported cases were described in patients with malignant conditions or immunosuppression.
Kaya et al (2015) reported a case of febrile neutropenia with R. ornithinolytica bacteremia in a 37-year-old male patient with acute lymphocytic leukemia.77 The clinical outcome in this case was fatal despite aggressive antibiotic combinations using piperacillin/tazobactam, amphotericin-B, tigecycline, amoxicillin/clavulanate and ciprofloxacin.77 Seng et al (2016) reported 6 cases of bloodstream infection in his series.1 A case of neutropenic fever was moreover depicted by Chun et al (2015) in a patient with a relapsed acute biphenotypic leukemia, that recovered after treatment with cefepime.4 One previous case of postoperative bloodstream infection was reported in an American 51-year-old male patient after valve replacement surgery.42 The isolated strain was susceptible only to amikacin and gentamicin and the outcome was fatal.42 Yamakawa et al (2016) described 2 cases of R. ornithinolytica infection in pediatric patients in whom R. ornithinolytica was detected in blood culture samples.8 Patients were 3 and 7-year-old and had IgA-nephropathy and myeloid leukemia respectively.8 In the first case, antibiotic susceptibility testing reported susceptibility to ceftriaxone, amoxicillin/clavulanic acid and TMP-SMX, and resistance to ciprofloxacin, minocycline and fosfomycin.8 In the second case, the isolated strain was susceptible to meropenem, minocycline and amoxicillin/clavulanic and resistant to levofloxacin, piperacillin and TMP-SMX.8 Treatment consisted of ceftriaxone (2 weeks) and meropenem (17 days) respectively with clinical improvement in both cases.8 Abbas et al (2018) reported a case of neonatal sepsis with a multidrug resistant strain of R. ornithinolytica isolated in blood cultures of a 12 hrs-old infant. The strain was susceptible only to colistin and TMP-SMX.78 Clinical improvement was noted with colistin.78 Moreover, R. ornithinolytica was isolated from blood samples of a preterm infant ventilated for hyaline membrane disease.79 The identified strain harbored the blaNDM-1 gene but remained susceptible to ciprofloxacin, colistin and tigecycline.79 A first case of associated septic shock, multisystem failure and purpura fulminans was also described in a newborn female infant.80 R. ornithinolytica was isolated from blood cultures and showed susceptibility to aminoglycosides, carbapenems, cefepime, quinolones and TMP-SMX.80 Despite aggressive treatment with meropenem, netilmicin, combined hemodynamic and respiratory support, the patient died at an age of 19 days.80 It is worth noting that the patient in this case was preterm and delivery occurred via caesarean section due to oligohydramnios.80 The significance of these factors in the pathogenesis of R. ornithinolytica infections remains unclear as data with infants is scarce.
A few cases of catheter infection and catheter-related bloodstream infections have also been identified.1,81 Among the bloodstream infection cases reported by Chun et al (2015), 5 cases had positive cultures from central lines for R. ornithinolytica.4 All these patients had malignant conditions and one of them died despite treatment.4
Other isolated cases of vascular prosthesis infections, conjunctivitis and meningitis due to R. ornithinolytica were described.1 Because of the rarity of these presentations, potential risk factors and prognosis predictors could not be identified.
Conclusion
In conclusion, R. ornithinolytica is an emerging bacterium in human infections. While formerly known as a relatively harmless pathogen found in aquatic environment and soil, its involvement in some severe clinical human infections we have described sheds light on a potentially increasingly virulent pathogen that affects comorbid at-risk patients. Its proper identification remains challenging and could explain why R. ornithinolytica infections are under-reported, although newer technologies and testing methods are allowing more accurate isolation and recognition of Raoultella species. Nonetheless, although the majority of reported cases are susceptible to standard antibiotic regimens, the emergence of multi-drug resistant strains may pose a serious risk to debilitated patients, and thus requires due consideration to further prevent increased virulence, especially in frail individuals.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Seng P, Boushab BM, Romain F, et al. Emerging role of Raoultella ornithinolytica in human infections: a series of cases and review of the literature. Int J Infect Dis. 2016;45:65–71. doi:10.1016/j.ijid.2016.02.014
2. Sakazaki R, Tamura K, Kosako Y, Yoshizaki E. Klebsiella ornithinolytica sp. nov., formerly known as ornithine-positive klebsiella oxytoca. Curr Microbiol. 1989;18:201–206. doi:10.1007/BF01570291
3. Drancourt M, Bollet C, Carta A, Rousselier P. Phylogenetic analyses of Klebsiella species delineate Klebsiella and Raoultella gen. nov., with description of Raoultella ornithinolytica comb. nov., Raoultella terrigena comb. nov. and Raoultella planticola comb. nov. Int J Syst Evol Microbiol. 2001;51:925–932. doi:10.1099/00207713-51-3-925
4. Chun S, Yun JW, Huh HJ, Lee NY. Clinical characteristics of Raoultella ornithinolytica bacteremia. Infection. 2015;43(1):59–64. doi:10.1007/s15010-014-0696-z
5. Levorova J, Machon V, Guha A, Foltan R. Septic arthritis of the temporomandibular joint caused by rare bacteria Raoultella ornithinolytica. Int J Oral Maxillofac Surg. 2017;46(1):111–115. doi:10.1016/j.ijom.2016.09.008
6. Lam PW, Tadros M, Fong IW. Mandibular osteomyelitis due to Raoultella species. JMM Case Rep. 2018;5(3):e005140. doi:10.1099/jmmcr.0.005140
7. Kabbara WK, Zgheib YR. Diabetic foot infection caused by Raoultella ornithinolytica. Am J Health Syst Pharm. 2015;72(24):2147–2149. doi:10.2146/ajhp150221
8. Yamakawa K, Yamagishi Y, Miyata K, et al. Bacteremia caused by Raoultella ornithinolytica in two children. Pediatr Infect Dis J. 2016;35(4):452–453. doi:10.1097/INF.0000000000001050
9. Solak Y, Gul E, Atalay H, Genc N, Tonbula H. A rare human infection of Raoultella ornithinolytica in a diabetic foot lesion. Ann Saudi Med. 2011;31(1):93–94. doi:10.4103/0256-4947.75794
10. Buyukcam A, Liste U, Bicakcigil A, Kara A, Sancak B. A case of Raoultella ornithinolytica urinary tract infection in a pediatric patient. J Infect Chemother. 2019;25(6):467–469. doi:10.1016/j.jiac.2018.12.011
11. Nakasone E, Kaneshiro R, Min K, Tokeshi J. Emergence of Raoultella ornithinolytica on O‘ahu: a case of community-acquired R. ornithinolytica urinary tract infection. Hawai‘I J Med Public Health. 2015;74:174–175.
12. Lee YC, Lin CM, Huang CY, et al. Determination and frying loss of histamine in striped marlin fillets implicated in a foodborne poisoning. J Food Prot. 2013;76(5):860–866. doi:10.4315/0362-028X.JFP-12-298
13. Sener D, Cokhras H, Camcioglu Y, Akcakaya N, Cakir E. Raoultella infection causing fever of unknown origin. Pediatr Infect Dis J. 2011;30(12):1122–1123. doi:10.1097/INF.0b013e31822bf4f6
14. Kanki M, Yoda T, Tsukamoto T, Shibata T. Klebsiella pneumoniae produces no histamine: Raoultella planticola and Raoultella ornithinolytica strains are histamine producers. Appl Environ Microbiol. 2002;68(7):3462–3466. doi:10.1128/AEM.68.7.3462-3466.2002
15. Gajdacs M. Resistance trends and epidemiology of Aeromonas and Plesiomonas infections (RETEPAPI): a 10-year retrospective survey. Infect Dis (Lond). 2019;51(9):710–713. doi:10.1080/23744235.2019.1640389
16. Keren Y, Keshet D, Eidelman M, Geffen Y, Raz-Pasteur A, Hussein K. Is Leclercia adecarboxylata a new and unfamiliar marine pathogen? J Clin Microbiol. 2014;52(5):1775–1776. doi:10.1128/JCM.03239-13
17. Gajdacs M, Urban E. Prevalence and antibiotic resistance of stenotrophomonas maltophilia in respiratory tract samples: a 10-year epidemiological snapshot. Health Serv Res Manag Epidemiol. 2019;6:2333392819870774.
18. Chawla K, Shashidhar V, Munim FC. Nonfermenting gram-negative bacilli other than Pseudomonas aeruginosa and Acinetobacter Spp. causing respiratory tract infections in a tertiary care center. J Glob Infect Dis. 2013;5(4):144–148. doi:10.4103/0974-777X.121996
19. Bhatt P, Tandel K, Das NK, Rathi KR. New Delhi metallo-beta-lactamase producing extensively drug-resistant Raoultella ornithinolytica isolated from drain fluid following Whipple’s pancreaticoduodenectomy. Med J Armed Forces India. 2015;71(Suppl 2):S609–S611. doi:10.1016/j.mjafi.2015.01.005
20. Podschun R, Ullmann U. Incidence of Klebsiella planticola among clinical Klebsiella isolates. Med Microbiol Lett. 1994;3:90–95.
21. Podschun R, Acktun H, Okpara J, Linderkamp O, Ullmann U, Borneff-Lipp M. Isolation of Klebsiella planticola from newborns in a neonatal ward. J Clin Microbiol. 1998;36(8):2331–2332.
22. Mori M, Ohta M, Agata N, et al. Identification of species and capsular types of klebsiella clinical isolates, with special reference to Klebsiella planticola. Microbiol Immunol. 1989;33(11):887–895. doi:10.1111/mim.1989.33.issue-11
23. Boye K, Hansen DS. Sequencing of 16S rDNA of Klebsiella: taxonomic relations within the genus and to other Enterobacteriaceae. Int J Med Microbiol. 2003;292(7–8):495–503. doi:10.1078/1438-4221-00228
24. Park JS, Hong KH, Lee HJ, et al. Evaluation of three phenotypic identification systems for clinical isolates of Raoultella ornithinolytica. J Med Microbiol. 2011;60(Pt 4):492–499. doi:10.1099/jmm.0.020768-0
25. Walckenaer E, Leflon-Guibout V, Nicolas-Chanoine MH. How to identify Raoultella spp. including R. ornithinolytica isolates negative for ornithine decarboxylase? The reliability of the chromosomal bla gene. J Microbiol Methods. 2008;75(3):405–410. doi:10.1016/j.mimet.2008.07.011
26. Tominaga T. Rapid detection of Klebsiella pneumoniae, Klebsiella oxytoca, Raoultella ornithinolytica and other related bacteria in food by lateral-flow test strip immunoassays. J Microbiol Methods. 2018;147:43–49. doi:10.1016/j.mimet.2018.02.015
27. Van Cleve JR, Boucher BA, Smith DV, Croce MA. Ventilator associated pneumonia caused by Raoultella ornithinolytica in two immunocompetent trauma patients. Respir Med Case Rep. 2018;24:135–137. doi:10.1016/j.rmcr.2018.05.006
28. Hajjar R, Schwenter F, Su SH, Gasse MC, Sebajang H. Community-acquired infection to Raoultella ornithinolytica presenting as appendicitis and shock in a healthy individual. J Surg Case Rep. 2018;2018(5):rjy097. doi:10.1093/jscr/rjy097
29. Richter SS, Sercia L, Branda JA, et al. Identification of Enterobacteriaceae by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry using the VITEK MS system. Eur J Clin Microbiol Infect Dis. 2013;32(12):1571–1578. doi:10.1007/s10096-013-1912-y
30. de Jong E, de Jong AS, Smidts-van den Berg N, Rentenaar RJ. Differentiation of Raoultella ornithinolytica/planticola and Klebsiella oxytoca clinical isolates by matrix-assisted laser desorption/ionization-time of flight mass spectrometry. Diagn Microbiol Infect Dis. 2013;75(4):431–433. doi:10.1016/j.diagmicrobio.2012.12.009
31. Gajdacs M, Urban E. Resistance trends and epidemiology of citrobacter-enterobacter-serratia in urinary tract infections of inpatients and outpatients (RECESUTI): a 10-year survey. Medicina (Kaunas). 2019;55(6):285.
32. Procop GW, Church DL, Hall GS, et al. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Philadelphia: Wolters Kluwer Health; 2017:682–683.
33. Haruki Y, Hagiya H, Sakuma A, Murase T, Sugiyama T, Kondo S. Clinical characteristics of Raoultella ornithinolytica bacteremia: a case series and literature review. J Infect Chemother. 2014;20(9):589–591. doi:10.1016/j.jiac.2014.05.005
34. Sekowska A. Raoultella spp.-clinical significance, infections and susceptibility to antibiotics. Folia Microbiol (Praha). 2017;62(3):221–227. doi:10.1007/s12223-016-0490-7
35. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
36. Gajdacs M, Abrok M, Lazar A, Burian K. Comparative epidemiology and resistance trends of common urinary pathogens in a tertiary-care hospital: a 10-year surveillance study. Medicina (Kaunas). 2019;55(7):356.
37. Pacilli M, Nataraja RM. Raoultella planticola associated with Meckel’s diverticulum perforation and peritonitis in a child: case report and systematic review of the paediatric literature. J Infect Public Health. 2019;12(5):605–607. doi:10.1016/j.jiph.2019.05.003
38. Piccirilli A, Pompilio A, Rossi L, et al. Identification of CTX-M-15 and CTX-M-27 in antibiotic-resistant gram-negative bacteria isolated from three rivers running in central Italy. Microb Drug Resist. 2019;25(7):1041–1049. doi:10.1089/mdr.2019.0016
39. Zurfluh K, Hachler H, Nuesch-Inderbinen M, Stephan R. Characteristics of extended-spectrum beta-lactamase- and carbapenemase-producing Enterobacteriaceae isolates from rivers and lakes in Switzerland. Appl Environ Microbiol. 2013;79(9):3021–3026. doi:10.1128/AEM.00054-13
40. Abid IN. Emergence of Raoultella ornithinolytica producing AmpC-beta-lactamases in the different clinical specimens. J Nat Res Sci. 2016;6(8):124–129.
41. Sun F, Yin Z, Feng J, et al. Production of plasmid-encoding NDM-1 in clinical Raoultella ornithinolytica and Leclercia adecarboxylata from China. Front Microbiol. 2015;6:458. doi:10.3389/fmicb.2015.00458
42. Castanheira M, Deshpande LM, DiPersio JR, Kang J, Weinstein MP, Jones RN. First descriptions of blaKPC in Raoultella spp. (R. planticola and R. ornithinolytica): report from the SENTRY Antimicrobial Surveillance Program. J Clin Microbiol. 2009;47(12):4129–4130. doi:10.1128/JCM.01502-09
43. Tijet N, Sheth PM, Lastovetska O, Chung C, Patel SN, Melano RG. Molecular characterization of Klebsiella pneumoniae carbapenemase (KPC)-producing Enterobacteriaceae in Ontario, Canada, 2008-2011. PLoS One. 2014;9(12):e116421. doi:10.1371/journal.pone.0116421
44. Khajuria A, Praharaj AK, Grover N, Kumar M. First report of blaNDM-1 in Raoultella ornithinolytica. Antimicrob Agents Chemother. 2013;57(2):1092–1093. doi:10.1128/AAC.02147-12
45. Piedra-Carrasco N, Fabrega A, Calero-Caceres W, et al. Carbapenemase-producing enterobacteriaceae recovered from a Spanish river ecosystem. PLoS One. 2017;12(4):e0175246. doi:10.1371/journal.pone.0175246
46. Paskova V, Medvecky M, Skalova A, et al. Characterization of NDM-encoding plasmids from enterobacteriaceae recovered from czech hospitals. Front Microbiol. 2018;9:1549. doi:10.3389/fmicb.2018.01549
47. Li J, Lan R, Xiong Y, et al. Sequential isolation in a patient of Raoultella planticola and Escherichia coli bearing a novel ISCR1 element carrying blaNDM-1. PLoS One. 2014;9(3):e89893. doi:10.1371/journal.pone.0089893
48. Zhou G, Guo S, Luo Y, et al. NDM-1-producing strains, family Enterobacteriaceae, in hospital, Beijing, China. Emerg Infect Dis. 2014;20(2):341–342. doi:10.3201/eid2002.121263
49. Zhang F, Wang X, Xie L, et al. A novel transposon, Tn6306, mediates the spread of blaIMI in Enterobacteriaceae in hospitals. Int J Infect Dis. 2017;65:22–26. doi:10.1016/j.ijid.2017.09.014
50. Reyes JA, Villavicencio F, Villacis JE, et al. First report of a clinical isolate of blaOXA-48- carbapenemase producing Raoultella ornithinolytica in South America. Rev Argent Microbiol. 2019. doi:10.1016/j.ram.2019.02.002
51. Al-Bayssari C, Olaitan AO, Leangapichart T, et al. Whole-genome sequence of a blaOXA-48-Harboring Raoultella ornithinolytica clinical isolate from lebanon. Antimicrob Agents Chemother. 2016;60(4):2548–2550. doi:10.1128/AAC.02773-15
52. Tafoukt R, Touati A, Leangapichart T, Bakour S, Rolain JM. Characterization of OXA-48-like-producing Enterobacteriaceae isolated from river water in Algeria. Water Res. 2017;120:185–189. doi:10.1016/j.watres.2017.04.073
53. Osterblad M, Kirveskari J, Hakanen AJ, Tissari P, Vaara M, Jalava J. Carbapenemase-producing Enterobacteriaceae in Finland: the first years (2008-11). J Antimicrob Chemother. 2012;67(12):2860–2864. doi:10.1093/jac/dks299
54. Demiray T, Koroglu M, Ozbek A, Altindis M. A rare cause of infection, Raoultella planticola: emerging threat and new reservoir for carbapenem resistance. Infection. 2016;44(6):713–717. doi:10.1007/s15010-016-0900-4
55. Hernandez-Garcia M, Leon-Sampedro R, Perez-Viso B, et al. First report of an OXA-48- and CTX-M-213-producing kluyvera species clone recovered from patients admitted in a university hospital in Madrid, Spain. Antimicrob Agents Chemother. 2018;62(11). doi:10.1128/AAC.01238-18
56. Pfeifer Y, Schlatterer K, Engelmann E, et al. Emergence of OXA-48-type carbapenemase-producing Enterobacteriaceae in German hospitals. Antimicrob Agents Chemother. 2012;56(4):2125–2128. doi:10.1128/AAC.05315-11
57. Zheng B, Zhang J, Ji J, et al. Emergence of Raoultella ornithinolytica coproducing IMP-4 and KPC-2 carbapenemases in China. Antimicrob Agents Chemother. 2015;59(11):7086–7089. doi:10.1128/AAC.01363-15
58. Wang X, Wang Y, Zhou Y, et al. Emergence of colistin resistance gene mcr-8 and its variant in Raoultella ornithinolytica. Front Microbiol. 2019;10:228. doi:10.3389/fmicb.2019.00228
59. Nang SC, Velkov T. The rise and spread of mcr plasmid-mediated polymyxin resistance. Crit Rev Microbiol. 2019;45(2):131–161. doi:10.1080/1040841X.2018.1492902
60. Luo J, Yao X, Lv L, et al. Emergence of mcr-1 in Raoultella ornithinolytica and Escherichia coli isolates from retail vegetables in China. Antimicrob Agents Chemother. 2017;61(10). doi:10.1128/AAC.01139-17
61. Sun P, Bi Z, Nilsson M, et al. Occurrence of blaKPC-2, blaCTX-M, and mcr-1 in enterobacteriaceae from well water in rural China. Antimicrob Agents Chemother. 2017;61(4). doi:10.1128/AAC.02569-16
62. Morais VP, Daporta MT, Bao AF, Campello MG, Andres GQ. Enteric fever-like syndrome caused by Raoultella ornithinolytica (Klebsiella ornithinolytica). J Clin Microbiol. 2009;47(3):868–869. doi:10.1128/JCM.01709-08
63. Mau N, Ross LA. Roultella ornithinolytica bacetremia in an infant with visceral heterotaxy. Pediatr Infect Dis J. 2010;29(5):477–478. doi:10.1097/INF.0b013e3181ce9227
64. Hadano Y, Tsukahara M, Ito K, Suzuki J, Kawamura I, Kurai H. Raoultella ornithinolytica bacteremia in cancer patients: report of three cases. Intern Med. 2012;51(22):3193–3195. doi:10.2169/internalmedicine.51.8349
65. Vos B, Laureys M. Giant renal cyst as cause of colic obstruction. Rev Med Brux. 2009;30:107–109.
66. Garcia-Lozano T, Pascual Pla FJ, Aznar Oroval E. Raoultella ornithinolytica in urinary tract infections. Med Clin (Barc). 2013;141:138–139. doi:10.1016/j.medcli.2012.11.021
67. Boattini M, Almeida A, Cardoso C, et al. Infections on the rise: raoultella spp., clinical and microbiological findings from a retrospective study, 2010-2014. Infect Dis (Lond). 2016;48(1):87–91. doi:10.3109/23744235.2015.1082619
68. De Petris L, Ruffini E. Roultella ornithinolytica infection in infancy: a case of febrile urinary tract infection. CEN Case Rep. 2018;7(2):234–236. doi:10.1007/s13730-018-0333-2
69. Seng P, Theron F, Honnorat E, Prost D, Fournier PE, Stein A. Raoultella ornithinolytica: an unusual pathogen for prosthetic joint infection. IDCases. 2016;5:46–48. doi:10.1016/j.idcr.2016.07.003
70. Venus K, Vaithilingam S, Bogoch II. Septic arthritis of the knee due to Raoultella ornithinolytica. Infection. 2016;44(5):691–692. doi:10.1007/s15010-016-0930-y
71. Singh M, Kaur I, Mundi DK, Kaur A. ENT infection caused by Raoultella ornithinolytica. Niger J Clin Pract. 2017;20(7):914–917. doi:10.4103/njcp.njcp_337_16
72. Derafshi R, Bazargani A, Ghapanchi J, Izadi Y, Khorshidi H. Isolation and identification of nonoral pathogenic bacteria in the oral cavity of patients with removable dentures. J Int Soc Prev Community Dent. 2017;7(4):197–201. doi:10.4103/jispcd.JISPCD_90_17
73. Heggendorn FL, Goncalves LS, Dias EP, Silva Junior A, Galvao MM, Lutterbach MT. Detection of sulphate-reducing bacteria in human saliva. Acta Odontol Scand. 2013;71(6):1458–1463. doi:10.3109/00016357.2013.770163
74. Ayoade F, Mada PK, Alam M. Fat necrosis and polymicrobial wound infection caused partly by Raoultella ornithinolytica after reduction mammoplasty. BMJ Case Rep. 2018;
75. Jellinge ME. Raoultella ornithinolytica diagnosed in a neurointensive patient. a rare case with recovery without antibiotics. J Crit Care Med (Targu Mures). 2017;3(3):120–122. doi:10.1515/jccm-2017-0017
76. Papakanderaki E, Kanakakis K, Goule S, Chounti M, Hountis P. Clinical significance of positive Raoultella Ornithinolytica and Staphylococcus hominis cultures in a post lobectomy patient. A case report. Monaldi Arch Chest Dis. 2018;88(1):885. doi:10.4081/monaldi.2018.885
77. Kaya S, Bayramoglu G, Sonmez M, Koksal I. Raoultella ornithinolytica causing fatal sepsis. Braz J Infect Dis. 2015;19(2):230–231. doi:10.1016/j.bjid.2014.12.010
78. Abbas A, Ahmad I. First report of neonatal early-onset sepsis caused by multi-drug-resistant Raoultella ornithinolytica. Infection. 2018;46(2):275–277. doi:10.1007/s15010-017-1098-9
79. Mahabeer Y, Singh-Moodley A, Mackanjee H, Perovic O, Mlisana KP. First report of neonatal bacteraemia caused by blaNDM-1 Raoultella ornithinolytica. South Afr J Infect Dis. 2016;32(2):40–42. doi:10.1080/23120053.2016.1210939
80. Sandal G, Ozen M. Fatal Raoultella ornithinolytica sepsis and purpura fulminans in a preterm newborn. Indian J Paediatr Dermatol. 2014;15(1):24. doi:10.4103/2319-7250.131833
81. Sekowska A, Dylewska K, Gospodarek E, Bogiel T. Catheter-related blood stream infection caused by Raoultella ornithinolytica. Folia Microbiol (Praha). 2015;60(6):493–495. doi:10.1007/s12223-015-0390-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.