")
Back to Journals » OncoTargets and Therapy » Volume 8
Radium-223 for the treatment of castration-resistant prostate cancer
Authors Joelle El-Amm J, Aragon-Ching J
Received 15 December 2014
Accepted for publication 17 February 2015
Published 18 May 2015 Volume 2015:8 Pages 1103—1109
DOI https://doi.org/10.2147/OTT.S44291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Daniele Santini
Joelle El-Amm, Jeanny B Aragon-Ching
Division of Hematology and Oncology, George Washington University Medical Center, Washington, DC, USA
Abstract: The vast majority of patients with metastatic castration-resistant prostate cancer (mCRPC) develop bone metastases. Bone metastases are a source of significant morbidity and affect quality of life in these patients. Several bone-targeting agents are approved for the treatment of bone metastases in prostate cancer, including bisphosphonates, denosumab, and radiopharmaceuticals. Radium-223 is a novel first-in-class alpha-emitting radiopharmaceutical that has been approved for treatment of patients with mCRPC with bone metastases. Radium-223 delivers cytotoxic radiation to the sites of bone metastases and offers the advantage of minimal myelosuppression. The landmark Phase III ALSYMPCA trial demonstrated that, in addition to providing bone-related palliation, radium-223 can also prolong overall survival in patients with mCRPC with bone metastases in the absence of visceral metastases and in the absence of lymphadenopathy greater than 3 cm. Ongoing trials will further elucidate its use in sequence or combination with other available therapies for mCRPC.
Keywords: prostate cancer, radiopharmaceuticals, bone metastases, radium-223
Introduction
Prostate cancer is a prevalent malignancy worldwide and remains the most common noncutaneous malignancy in the USA.1 Androgen suppression therapy is the cornerstone of therapy in metastatic prostate cancer. However, relapse usually occurs and prostate cancer becomes castration-resistant. The first approved therapeutic agent that showed a survival advantage in metastatic castration-resistant prostate cancer (mCRPC) was docetaxel. Six years later, cabazitaxel was shown to overcome taxane resistance and was approved in the second-line setting. More recently, two oral agents, abiraterone and enzalutamide, gained approved for use in the treatment of mCRPC. Bone metastases from prostate cancer are a major cause of disease-related morbidity and mortality and affect more than 90% of patients with mCRPC.2,3 Morbidity and mortality stem from the increased bone pain, reduced hematopoiesis, increased risk of fractures, malignant hypercalcemia, and increased skeletal-related events.4–6 The term skeletal-related event encompasses complications of bone metastases that include pathologic fractures, spinal cord compression, and need for surgery or radiation therapy, all of which affect quality of life as well. Recently, more insight in the pathophysiology of bone metastases has brought new bone-targeted agents aiming at reducing the rate of skeletal-related events and improving survival.7 This review describes the recently approved radiopharmaceutical agent radium-223, its mechanism of action, the clinical trials involved in securing its approval, and its place in therapy in clinical practice.
Bone-targeted agents
The first class of agents investigated and approved for the treatment of skeletal-related events in patients with mCRPC were the bisphosphonates. Bisphosphonates act by adhering to hydroxyapatite crystal-binding sites in the bone matrix, therefore preventing osteoclast adherence and inhibiting osteoclast progenitor differentiation and survival by stimulating osteoblasts.8,9 Zoledronic acid is the only bisphosphonate that the US Food and Drug Administration (FDA) has approved to prevent skeletal-related events in patients with mCRPC. In a randomized Phase III clinical trial, zoledronic acid was found to decrease the rate of skeletal-related events. However, it had no effect on overall survival, performance status, disease progression, or quality of life.10,11 Pamidronate, on the other hand, failed to show a reduction in skeletal-related events in two randomized, placebo-controlled trials.12 Denosumab is a humanized monoclonal antibody that binds to the pro-osteoclastogenic factor receptor activator of nuclear factor kappa B ligand (RANK-L), inhibiting RANK-L-mediated bone resorption.13 Denosumab (Xgeva®; Amgen, Thousand Oaks, CA, USA) was approved by the FDA in November 2010 for the prevention of skeletal-related events in patients with bone metastases from solid tumors including prostate cancer. This approval was based on a large randomized, double-blind Phase III clinical trial that compared denosumab with zoledronic acid in patients with bone metastases from prostate cancer.14 The median time to the first skeletal-related event was significantly longer in the denosumab arm compared with the zoledronic acid arm (20.7 versus 17.1 months, respectively; P=0.0002 for noninferiority and P=0.008 for superiority, hazard ratio 0.82). Zoledronic acid and denosumab are currently widely used in clinical practice in combination with systemic therapy in prostate cancer.15
The other class of bone-targeted agents includes the radiopharmaceuticals.16 Radiopharmaceuticals emit either alpha or beta particles, both of which deliver damaging radiation to cancer cells. Historically, the most commonly used radiopharmaceuticals are the b-emitters, ie, strontium-89 chloride (Metastron®; GE Healthcare, Arlington Heights, IL, USA) and samarium-153 (Quadramet®; EUSA Pharma, Oxford, UK).
Strontium-89 was initially approved by the FDA in 1993. Its half-life is 50.5 days; it has a beta energy of 1.5 MeV and is excreted rapidly via the renal route.17,18 The efficacy of strontium-89, demonstrated as complete pain response, ranged between 8% and 77% with a mean value of 32%, while that for partial response was 44%, with a mean duration of response of 15 months.19 The main toxicity of strontium-89 is hematologic, ie, a significant reduction in white blood cells and platelets with a predicted nadir at 6 weeks and a protracted recovery time of up to 6 months.20 Samarium-153 was approved by the FDA in 1997. Its half-life is 1.9 days, and it provides rapid pain relief within 2–7 days.21–23 Multiple clinical trials were conducted with these two agents, but none demonstrated an overall survival benefit.24–29 These agents are not commonly used in clinical practice, mainly due to their severe side effects, including profound and frequent myelosuppression. Another limitation of these β-emitters is that they are renally excreted, which also limits their use. Table 1 summarizes the characteristics of the different bone-targeted agents approved for use in mCRPC.
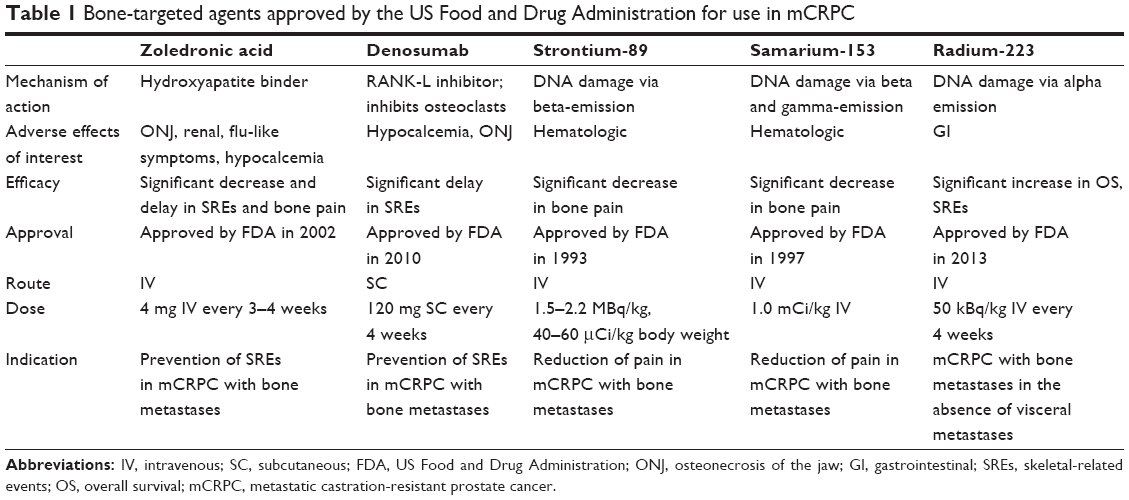 | Table 1 Bone-targeted agents approved by the US Food and Drug Administration for use in mCRPC |
Mechanism of action of radium-223
Radium-223 dichloride (radium-223, Xofigo®, previously known as Alpharadin, Bayer, Whippany, NJ, USA) is a novel radioisotope that emits cytotoxic alpha particles that have a high affinity for the bone matrix. Radium-223 acts as a calcium mimetic by forming complexes with the bone mineral hydroxyapatite in areas of high bone turnover, thereby directly targeting the areas of bone metastases.30
The discovery of radium dates back to 1898 due to the work of Marie and Pierre Curie. Radium-223 can be obtained from actinium-227, the latter having the advantage of a long half-life of 21.7 years.31 Radium-223 is soluble in water as radium-223 chloride, and when administered intravenously, decays over six steps to lead-207, releasing for each atom four alpha particles (each composed of two protons and two neutrons) and two beta particles, with alpha particles emitting 95.3% of the energy and beta particles emitting 3.6%. Only 1.1% of the energy emitted is gamma rays. The released alpha particles are directly cytotoxic to cells by inducing double-stranded DNA breaks.31,32 Radium-223 is excreted mainly through the gastrointestinal tract and has a half-life of 11.4 days. Renal excretion is minimal, unlike with samarium-153 and strontium-89.30
Compared with the beta-emitters, the radiation emitted by radium-223 is more limited, with a much shorter track length of less than 0.1 mm in tissue (compared with 0.6 mm for samarium-153 and 2.4 mm for strontium-89), offering the advantage of less myelosuppression. Alpha particles also have the advantage of a higher mass as compared with beta particles, thus higher linear energy transfer, resulting in more cellular damage at a much shorter range with less damage to normal cells.33 The favorable safety profile of radium-223 led to multiple trials evaluating its efficacy in bone metastases.
Preclinical and Phase I studies
Early preclinical studies of radium-223 in rats demonstrated a bone distribution similar to that of strontium-89, with a bone marrow-sparing advantage, and a selective concentration in bone rather than soft tissues.34 In addition, experimental rats that received chemotherapy and had bisphosphonate-resistant bone metastases showed longer survival when treated with radium-223.35 A dose-escalation Phase I trial that included both breast and prostate cancer patients, of whom 15 had prostate cancer, examined the safety of radium-223 in the treatment of bone metastases.30 The results showed a significant decline in serum alkaline phosphatase of up to 52%, a significant pain response in 60% of patients, with mild and reversible myelosuppression. The pharmacokinetics, pharmacodynamics, and biodistribution of radium-223 were evaluated in a Phase II trial that included ten patients with metastatic prostate cancer to bone.36 Three patients received injections of radium at a dose of 50 kBq/kg, another three received radium at a dose 100 kBq/kg, and four patients received 250 kBq/kg. Radium-223 was rapidly cleared from the circulation, with only 0.5% of radium-223 remaining after 24 hours. The main excretion of the drug was gastrointestinal, with minimal renal excretion. Given the pain relief, tolerability, and rapidity of clearance of the drug, a Phase II trial was initiated in men with mCRPC who had pain requiring external beam radiation therapy.
Phase II study
A double-blind, randomized Phase II trial evaluated the effect of radium-223 in patients with mCRPC who had either multiple bone metastases or one painful bone lesion with two consecutive rising prostate-specific antigen (PSA) levels.37 The patients received external beam radiation and intravenous radium-233 at 50 kBq/kg for a total of up to four injections or external beam radiation and placebo. The two treatment arms showed a similar hematotoxicity profile. The radium-223 arm showed better efficacy, with a greater reduction in alkaline phosphatase, a longer time to PSA progression, and an increased time to skeletal-related events. In addition, a trend for improved survival was noted when compared with the placebo arm (65.3 weeks versus 46.4 weeks; P=0.066). These results were confirmed in the 24-month follow-up study, during which there was no increased rate of new malignancies.38 Another double-blind Phase II study analyzed the effect of four different doses of radium-223 (5, 25, 50, 100 kBq/kg) in 100 patients with mCRPC. Pain reduction was noted as early as 2 weeks after the injection, and after 8 weeks, 40%, 63%, 56%, and 71% of patients in the 5, 25, 50 and 100 kBq/kg groups, respectively, had pain reduction, and no major adverse events were noted.39
ALSYMPCA trial
ALSYMPCA (ALpharadin in SYMptomatic Prostate Cancer) is a randomized, double-blind, Phase III clinical trial that led to FDA approval of radium-223 in the USA on May, 15, 2013 for metastatic prostate cancer to bone in the absence of visceral metastases.40 This landmark trial is the first to show an overall survival benefit with the use of a radioisotope. The primary endpoint of the study was overall survival. A total of 921 patients across 19 countries were recruited into the trial. The patients had to have symptomatic bone metastases at two or more sites in the absence of visceral metastases. The patients had either previously received docetaxel, were deemed not candidates for docetaxel, or refused docetaxel. The enrolled patients were randomized in a 2:1 ratio to receive either six cycles of radium-223 at a dose of 50 kBq/kg every 4 weeks in addition to best standard of care or six cycles of placebo every 4 weeks in addition to best standard of care. The patients were enrolled from June 2008 until February 2011. In the middle of 2011, a planned interim analysis showed a survival benefit of radium-223 and the trial was stopped early. The arms of the study were balanced in terms of baseline characteristics. The median age of the patients was 71 years. In both arms, 57% of the patients have previously received docetaxel. An overall survival of 3.6 months was noted in favor of radium-223 (14.9 versus 11.3 months, P=0.00185, hazard ratio 0.695) and the study met its primary endpoint,40 regardless of docetaxel use.41 Secondary endpoints all favored radium-223. Notably, the number of skeletal-related events was reduced and the median time to a skeletal-related event was prolonged in the radium-223 arm by around 6 months (15.6 versus 9.8 months, hazard ratio 0.66, 95% confidence interval 0.52–0.83, P=0.00037).42 Other secondary endpoints (PSA response, time to PSA progression, change in alkaline phosphatase) were also in favor of radium-223. In addition, a higher percentage of patients in the radium-223 arm had a significant improvement in their quality of life as assessed by the FACT-P (Functional Assessment of Cancer Therapy-Prostatic) score (25% versus 16%, P=0.02). Radium-223 yielded no severe grade adverse events. Most notably, the incidence of grade 3 and 4 anemia, neutropenia, and thrombocytopenia was minimal (1.8%, 0.7%, and 3.2%, respectively). Interestingly, more adverse events occurred in patients treated with placebo than with radium-223 (96% versus 93% all grade adverse events, respectively, and 62% versus 56% grade 3 and 4, respectively). In the subgroup analysis looking at patients with prior docetaxel exposure, a higher incidence of grade 3–4 thrombocytopenia was shown in those who received radium-223 at 9% (31 of 347 patients) versus only 3% (five of 171 patients) in the placebo group.41 Reassuringly, no differences in grade 3–4 anemia or neutropenia was seen in either treatment group.
The enrolled patients entered a designated 3-year follow-up program after receiving six injections of radium-223 or placebo. A total of 574 patients from 921 patients entered the follow-up program (n=406 received radium-223 and 168 received placebo). A total of 322 patients in the radium-223 group withdrew from the follow-up program (79%) and 144 withdrew from the placebo arm (86%), the most common cause being death. The median duration of follow-up was 10.4 months for the radium-223 group and 7.6 months for the placebo group. Only 20 patients (16 in the radium-223 group and four in the placebo group) completed the 3-year follow-up. In addition, long-term follow-up of the ALSYMPCA trial at 1.5 years showed that radium-223 continues to be very safe, with no increased incidence of second cancers, acute myelogenous leukemia, myelodysplasia, or aplastic anemia.43
Future directions
Timing of the use of radium-223 in the treatment sequence of mCRPC remains a challenging and unanswered question, given the vast availability of a wide range of therapies, ranging from chemotherapy, oral androgen inhibitors, and other bone-targeted therapies. The efficacy of radium-223 seems to be independent of prior use of docetaxel, and its safety profile seemed similar both in the pre-docetaxel and post-docetaxel setting, except for higher hematologic toxicity and nausea and vomiting in the post-docetaxel setting and higher benefit in delaying skeletal-related events in the post-docetaxel setting than in the pre-docetaxel setting. The mechanism of action of radium-223 does not appear to prohibit the use of other available systemic therapies in mCRPC, and while the pivotal ALSYMPCA trial only allowed use of best supportive therapy with older agents, such as ketoconazole, newer androgen-targeting agents like abiraterone or enzalutamide can conceivably be combined with radium. To this end, several ongoing trials will further elucidate its place in combination or sequence with other agents, including abiraterone and enzalutamide (Table 2), further establishing its role in the treatment of mCRPC. The utility of combining radium with docetaxel was also examined in a Phase I/II trial (NCT01106352) that showed the combination was efficacious and safe, although the Phase II trial dose of docetaxel had to be reduced to 60 mg/m2 to avoid additional hematologic toxicity. Future questions regarding the utility and added benefit of administration of radium-223 beyond the six doses given in the registration trials would also be worthy of investigation.
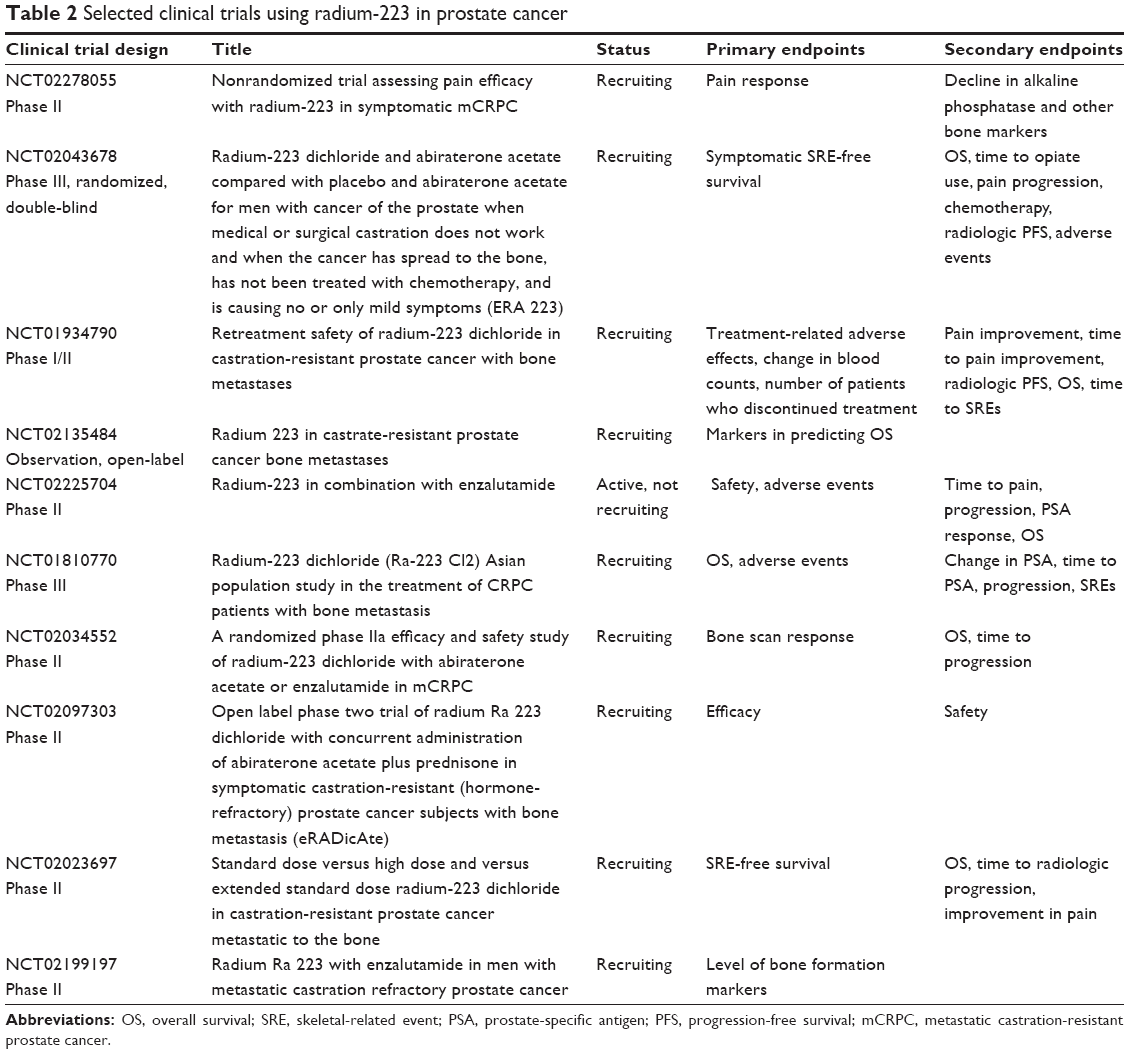 | Table 2 Selected clinical trials using radium-223 in prostate cancer |
Conclusion
Data available on radium-223 suggests that this agent, in addition to improving pain, delaying the time to opiate use and external beam radiation, and improving quality of life, does prolong survival. Radium is an attractive option in patients either post docetaxel because of failure or patients who are otherwise not candidates for cytotoxic chemotherapy because of frailty or refusal. The National Comprehensive Cancer Network therefore includes radium-223 as a recommended option for treatment of mCRPC in the first-line setting as well as post docetaxel. The current recommended dose of radium-223 is 50 kBq/kg, administered by a slow intravenous infusion over one minute every 4 weeks for a total of six doses. The question of its optimal use and sequence among the other agents approved in mCRPC remains to be answered, but it certainly is a welcome addition to the arsenal of treatment for mCRPC.
Disclosure
JE reports no conflict of interest. JA reports receiving honoraria for serving on the advisory board of Algeta/Bayer and speaker fees from Janssen and Astellas and Medivation.
References
Fanti S, Krause B, Weber W, et al. Re: Nicolas Mottet, Joaquim Bellmunt, Michel Bolla, et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol. 2011;59:572–583. | ||
Costa L, Badia X, Chow E, Lipton A, Wardley A. Impact of skeletal complications on patients’ quality of life, mobility, and functional independence. Support Care Cancer. 2008;16:879–889. | ||
Mottet N, Bellmunt J, Bolla M, et al. [EAU guidelines on prostate cancer. Part II: treatment of advanced, relapsing, and castration-resistant prostate cancer]. Actas Urol Esp. 2011;35:565–579. Spanish. | ||
Mottet N, Bellmunt J, Bolla M, et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol. 2011;59:572–583. | ||
Friedrich MG, Hellstern A, Hautmann SH, et al. Clinical use of urinary markers for the detection and prognosis of bladder carcinoma: a comparison of immunocytology with monoclonal antibodies against Lewis X and 486p3/12 with the BTA STAT and NMP22 tests. J Urol. 2002;168:470–474. | ||
Oefelein MG, Ricchiuti V, Conrad W, Resnick MI. Skeletal fractures negatively correlate with overall survival in men with prostate cancer. J Urol. 2002;168:1005–1007. | ||
Aad G, Abajyan T, Abbott B, et al. Measurement of the azimuthal angle dependence of inclusive jet yields in Pb+Pb collisions at radical(sNN)=2.76 TeV with the ATLAS detector. Phys Rev Lett. 2013;111:152301. | ||
Oades GM, Coxon J, Colston KW. The potential role of bisphosphonates in prostate cancer. Prostate Cancer Prostatic Dis. 2002;5:264–272. | ||
Rogers MJ, Watts DJ, Russell RG. Overview of bisphosphonates. Cancer. 1997;80(8 Suppl):1652–1660. | ||
Saad F, Gleason DM, Murray R, et al. A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94:1458–1468. | ||
Saad F, Gleason DM, Murray R, et al. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J Natl Cancer Inst. 2004;96:879–882. | ||
Small EJ, Smith MR, Seaman JJ, Petrone S, Kowalski MO. Combined analysis of two multicenter, randomized, placebo-controlled studies of pamidronate disodium for the palliation of bone pain in men with metastatic prostate cancer. J Clin Oncol. 2003;21:4277–4284. | ||
Smith MR, Egerdie B, Hernandez Toriz N, et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med. 2009;361:745–755. | ||
Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet. 2011;377:813–822. | ||
Heidenreich A, Bastian PJ, Bellmunt J, et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol. 2014;65:467–479. | ||
Ryan CJ, Saylor PJ, Everly JJ, Sartor O. Bone-targeting radiopharmaceuticals for the treatment of bone-metastatic castration-resistant prostate cancer: exploring the implications of new data. Oncologist. 2014;19:1012–1018. | ||
Laing AH, Ackery DM, Bayly RJ, et al. Strontium-89 chloride for pain palliation in prostatic skeletal malignancy. Br J Radiol. 1991;64:816–822. | ||
Silberstein EB, Williams C. Strontium-89 therapy for the pain of osseous metastases. J Nucl Med. 1985;26:345–348. | ||
Finlay IG, Mason MD, Shelley M. Radioisotopes for the palliation of metastatic bone cancer: a systematic review. Lancet Oncol. 2005;6:392–400. | ||
Pons F, Herranz R, Garcia A, et al. Strontium-89 for palliation of pain from bone metastases in patients with prostate and breast cancer. Eur J Nucl Med. 1997;24:1210–1214. | ||
Turner JH, Claringbold PG, Hetherington EL, Sorby P, Martindale AA. A phase I study of samarium-153 ethylenediaminetetramethylene phosphonate therapy for disseminated skeletal metastases. J Clin Oncol. 1989;7:1926–1931. | ||
Sartor O, Reid RH, Hoskin PJ, et al. Samarium-153-Lexidronam complex for treatment of painful bone metastases in hormone-refractory prostate cancer. Urology. 2004;63:940–945. | ||
Sartor O, Reid RH, Bushnell DL, Quick DP, Ell PJ. Safety and efficacy of repeat administration of samarium Sm-153 lexidronam to patients with metastatic bone pain. Cancer. 2007;109:637–643. | ||
Lewington VJ, McEwan AJ, Ackery DM, et al. A prospective, randomised double-blind crossover study to examine the efficacy of strontium-89 in pain palliation in patients with advanced prostate cancer metastatic to bone. Eur J Cancer. 1991;27:954–958. | ||
Serafini AN, Houston SJ, Resche I, et al. Palliation of pain associated with metastatic bone cancer using samarium-153 lexidronam: a double-blind placebo-controlled clinical trial. J Clin Oncol. 1998;16:1574–1581. | ||
Buchali K, Correns HJ, Schuerer M, et al. Results of a double blind study of 89-strontium therapy of skeletal metastases of prostatic carcinoma. Eur J Nucl Med. 1988;14:349–351. | ||
Porter AT, McEwan AJ, Powe JE, et al. Results of a randomized phase-III trial to evaluate the efficacy of strontium-89 adjuvant to local field external beam irradiation in the management of endocrine resistant metastatic prostate cancer. Int J Radiat Oncol Biol Phys. 1993;25:805–813. | ||
Quilty PM, Kirk D, Bolger JJ, et al. A comparison of the palliative effects of strontium-89 and external beam radiotherapy in metastatic prostate cancer. Radiother Oncol. 1994;31:33–40. | ||
Oosterhof GO, Roberts JT, de Reijke TM, et al. Strontium(89) chloride versus palliative local field radiotherapy in patients with hormonal escaped prostate cancer: a phase III study of the European Organisation for Research and Treatment of Cancer, Genitourinary Group. Eur Urol. 2003;44:519–526. | ||
Nilsson S, Larsen RH, Fossa SD, et al. First clinical experience with alpha-emitting radium-223 in the treatment of skeletal metastases. Clin Cancer Res. 2005;11:4451–4459. | ||
McDevitt MR, Sgouros G, Finn RD, et al. Radioimmunotherapy with alpha-emitting nuclides. Eur J Nucl Med. 1998;25:1341–1351. | ||
Baidoo KE, Yong K, Brechbiel MW. Molecular pathways: targeted alpha-particle radiation therapy. Clin Cancer Res. 2013;19:530–537. | ||
Cheetham PJ, Petrylak DP. Alpha particles as radiopharmaceuticals in the treatment of bone metastases: mechanism of action of radium-223 chloride (Alpharadin) and radiation protection. Oncology (Williston Park). 2012;26:330–337, 341. | ||
Henriksen G, Fisher DR, Roeske JC, Bruland OS, Larsen RH. Targeting of osseous sites with alpha-emitting 223Ra: comparison with the beta-emitter 89Sr in mice. J Nucl Med. 2003;44:252–259. | ||
Henriksen G, Breistol K, Bruland OS, Fodstad O, Larsen RH. Significant antitumor effect from bone-seeking, alpha-particle-emitting (223)Ra demonstrated in an experimental skeletal metastases model. Cancer Res. 2002;62:3120–3125. | ||
Carrasquillo JA, O’Donoghue JA, Pandit-Taskar N, et al. Phase I pharmacokinetic and biodistribution study with escalating doses of (2)(2)(3)Ra-dichloride in men with castration-resistant metastatic prostate cancer. Eur J Nucl Med Mol Imaging. 2013;40:1384–1393. | ||
Nilsson S, Franzen L, Parker C, et al. Bone-targeted radium-223 in symptomatic, hormone-refractory prostate cancer: a randomised, multicentre, placebo-controlled phase II study. Lancet Oncol. 2007;8:587–594. | ||
Nilsson S, Franzen L, Parker C, et al. Two-year survival follow-up of the randomized, double-blind, placebo-controlled phase II study of radium-223 chloride in patients with castration-resistant prostate cancer and bone metastases. Clin Genitourin Cancer. 2013;11:20–26. | ||
Nilsson S, Strang P, Aksnes AK, et al. A randomized, dose-response, multicenter phase II study of radium-223 chloride for the palliation of painful bone metastases in patients with castration-resistant prostate cancer. Eur J Cancer. 2012;48:678–686. | ||
Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. 2013;369:213–223. | ||
Hoskin P, Sartor O, O’Sullivan JM, et al. Efficacy and safety of radium-223 dichloride in patients with castration-resistant prostate cancer and symptomatic bone metastases, with or without previous docetaxel use: a prespecified subgroup analysis from the randomised, double-blind, phase 3 ALSYMPCA trial. Lancet Oncol. 2014;15:1397–1406. | ||
Sartor O, Coleman R, Nilsson S, et al. Effect of radium-223 dichloride on symptomatic skeletal events in patients with castration-resistant prostate cancer and bone metastases: results from a phase 3, double-blind, randomised trial. Lancet Oncol. 2014;15:738–746. | ||
[No authors listed]. 1.5-year post-treatment follow-up of radium-223 dichloride (Ra-223) in patients with castration-resistant prostate cancer (CRPC) and bone metastases from the phase 3 ALSYMPCA Study 9. Clin Adv Hematol Oncol. 2014;12(4 Suppl 11):9–10. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.