")
Back to Journals » International Medical Case Reports Journal » Volume 8
Radical cystectomy and pelvic lymphadenectomy with ileal conduit urinary diversion and abdominal wall reconstruction: an interesting case of multidisciplinary management
Authors Sofos S, Walsh C, Parr N, Hancock K
Received 21 January 2014
Accepted for publication 24 March 2014
Published 16 January 2015 Volume 2015:8 Pages 29—31
DOI https://doi.org/10.2147/IMCRJ.S61094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Stratos S Sofos,1 Ciaran Walsh,2 Nigel J Parr,2 Kevin Hancock1
1Whiston Hospital, Prescot, 2Arrowe Park Hospital, Wirral, Merseyside, UK
Abstract: The ileal conduit for urinary diversion after radical cystectomy is a well-described procedure. Furthermore, parastomal hernias, prolapse, stenosis, and retraction of the stoma have been reported as some of the more common complications of this procedure. The subsequent repair of parastomal hernias with a biological mesh and the potential of the conduit to “tunnel” through it has also been described. In this case report, we present a combined repair of a large incisional hernia with a cystectomy and a pelvic lymphadenectomy for invasive bladder cancer, with the use of a biological mesh for posterior component abdominal wall primary repair as well as for support to the ileal conduit used for urinary diversion.
Keywords: incisional hernia, posterior component separation, biological mesh
Introduction
The ileal conduit for urinary diversion after radical cystectomy is a well-described procedure. It makes use of a short segment of ileum to allow urine to pass through the abdominal wall and empty through an everted stoma into a stoma collection device.
Furthermore, parastomal hernias, prolapse, stenosis, and retraction of the stoma have been reported in up to 31% of cases as some of the more common complications of this procedure.1–3 The subsequent repair of parastomal hernias with a mesh and the potential of the conduit to “tunnel” through it has also been described.
However, in our case report, we present a combined primary repair of a large incisional hernia with a cystectomy and pelvic lymphadenectomy, with the use of a biological mesh for the abdominal wall repair as well as support to the ileal conduit.
Case report
A 72-year-old generally fit and well gentleman presented to the urology outpatient clinic with a highly aggressive bladder tumor (G3 pTa) and subepithelial (T1) transitional cell cancer in association with carcinoma in situ. He had originally been treated with a full dose of Bacillus Calmette–Guérin and maintenance, but had relapsed while on this treatment. His case was further complicated by a large incisional hernia (Figure 1A) secondary to a previous laparotomy for a perforated appendix.
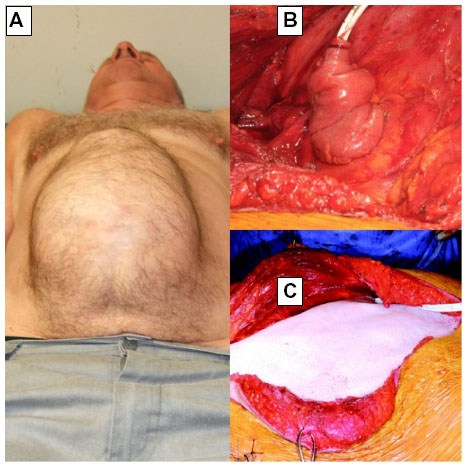 | Figure 1 (A) Preoperative – incisional hernia visible; (B) ileal conduit; (C) biological mesh applied. |
The large incisional hernia extended from just below the xiphisternum to well below his umbilicus, and also from the right and left flanks. The overlying skin was emaciated and there was little underlying healthy, durable tissue.
After discussion with the patient, a joint, multidisciplinary decision was made to undertake the surgical excision of the bladder along with the repair of the incisional hernia between urology, general surgery, and plastic surgery teams. With regards to reconstruction options, a neobladder was offered to the patient; however he declined this option.
At induction, the patient was given intravenous antibiotics (gentamycin and co-amoxiclav), which were continued for 5 days postoperatively.
The procedure commenced with excision of the skin over the hernia sac as part of a long midline incision. On opening the peritoneal cavity there were a number of adhesions involving the distal small bowel, but no other significant abnormality.
Upon cystectomy and prostatectomy, the left ureters were brought through the sigmoid mesentery (Figure 1B). A segment of terminal ileum was isolated on its mesentery. Ileo-ileal linear anastomosis was performed. The duplex ureters were spatulated and the posterior margins of the spatulation anastomosed to each other. This was sutured with the proximal end of the conduit. The right ureter was spatulated and a Bricker-type anastomosis performed to the conduit approximately 1 inch from the proximal end, again over a Bard urinary diversion stent.
A posterior component separation of the anterior abdominal wall was performed. The conduit was brought through the window in the small bowel mesentery and the window then closed. The proximal end of the conduit was attached to psoas. The peritoneum and posterior sheath were closed with a polyglatin 910 (Vicryl; Ethicon Inc., Somerville, NJ, USA) absorbable suture. A 20×25 cm porcine mesh was inserted (Figure 1C) and a window was made in the mesh to allow the conduit to pass through. There were no sutures involved to hold the conduit in place through the mesh. The conduit was brought out in the right iliac fossa and everted (Figure 2). The anterior sheath was closed with another absorbable, polydioxanone suture.
 | Figure 2 Postoperative photo of patient with ileal conduit in situ. |
The final pathology revealed residual dysplasia and carcinoma in situ (G3), Stage pT1, pN0 0/24 nodes positive.
Discussion
Ileal conduit for urinary diversion after radical cystectomy for bladder cancer is a well-described procedure. In addition, the repair of parastomal hernias has been described with regards to their frequency and also their repair techniques, some utilizing posterior component separation in the abdominal wall with a mesh repair.4
Robotic radical cystectomy has emerged as a viable technique for bladder cancer patients, due to its enhanced visualization and control of the da Vinci surgical robot. Robotic surgery also offers other advantages, particularly in terms of less intraoperative blood loss as well as improved recovery time. However, in this particular case, a robot was not used because the procedure involved a synchronous major abdominal wall reconstruction.
We present an interesting case where a primary repair of a large incisional hernia was undertaken concurrently with the cystectomy and ileal conduit, and we present the use of the biological mesh as a mesentery channel, offering support and stability, in addition to its use in the abdominal wall reconstruction.
The biological mesh used was a sterile reconstructive tissue matrix that supports tissue regeneration. It is derived from porcine dermis and is used for abdominal wall reconstruction amongst other procedures; ie breast reconstruction, as it has been shown to provide stronger repairs offering biomechanical strength. It is also shown to minimize hernia repair complications and allows for simpler surgeries in the abdominal area in the future.5 This particular mesh was chosen over other biological and synthetic meshes, because of its resistance to infection and the nonadherence to the bowel.
With regards to chemotherapy, we suggest that, if necessary, it should be commenced postoperatively following complete wound healing.
Surgical technique with extra care regarding wound healing is imperative. Such measures would include tensionless closure of the apronectomy and also an attempt to preserve some of the deep inferior epigastric perforators to the preserved part of the abdominal apron. We would also recommend leaving the drains in longer, and also the use of an abdominal binder.
The patient was seen in the follow-up outpatient clinic 3 months postoperatively and he has made an unremarkable recovery.
Disclosure
The authors report no conflicts of interest in this work.
References
Rolstad BS, Erwin-Toth PL. Peristomal skin complications: prevention and management. Ostomy Wound Manage. 2004;50(9):68–77. | |
Herlufsen P, Olsen AG, Carlsen B, et al. Study of peristomal skin disorders in patients with permanent stomas. Br J Nurs. 2006;15(16):854–862. | |
Szymanski KM, St-Cyr D, Alam T, Kassouf W. External stoma and peristomal complications following radical cystectomy and ileal conduit diversion: a systematic review. Ostomy Wound Manage. 2010;56(1):28–35. | |
Seiffert L. Die ‘‘Darm-Siphonblase.” Arch fur Klinische Chirurgie. 1935;183:569. German. | |
Hopkins TB, Trento A. Parastomal ileal loop hernia repair with marlex mesh. J Urol. 1982;128(4):811–812. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.