")
Back to Journals » Clinical Epidemiology » Volume 6
Quality of venous thromboembolism diagnoses among prostate cancer patients in the Danish National Registry of Patients
Authors Drljevic A , Borre M, Høyer M, Ehrenstein V, Nguyen-Nielsen M
Received 7 April 2014
Accepted for publication 4 June 2014
Published 4 October 2014 Volume 2014:6 Pages 351—357
DOI https://doi.org/10.2147/CLEP.S65681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Aska Drljevic,1 Michael Borre,2 Morten Høyer,3 Vera Ehrenstein,4 Mary Nguyen-Nielsen4
1Department of Pharmacology, 2Department of Urology, 3Department of Oncology, 4Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark
Background and aim: It is well established that cancer patients have an increased risk of venous thromboembolism (VTE). However, no previous study has examined the quality of VTE diagnoses related to cancer patients in the Danish National Registry of Patients (DNRP). To support future studies on cancer and risk of VTE, this study aimed to estimate the positive predictive value (PPV) of VTE diagnoses among prostate cancer (PC) patients registered in the DNRP.
Materials and methods: We conducted a validation study using data from hospitals within the Central Denmark Region, which covers a population of 1.3 million people. Using the DNRP, we identified a total of 120 PC patients registered with VTE within the period 1995–2012. We also identified a random sample of 120 PC patients with no VTE registration within the same period. Therefore, a total of 240 patients were selected for medical chart review. We compared data from the DNRP to data collected from medical record review (ie, reference standard). We then computed PPV, sensitivity, and specificity with corresponding 95% confidence intervals (CIs) using the Jeffreys method.
Results: The final study sample included 232 PC patients, of which 115 were registered with VTE and 117 had no registration of VTE in the DNRP. We found the overall PPV of VTE diagnoses in the DNRP to be 86.1% (95% CI 78.9%–91.5%). Sensitivity was 98.0% (95% CI 93.8%–99.6%), and specificity was 87.8% (95% CI 81.4%–92.6%). We also found the PPV of incident PC diagnoses in the DNRP to be 98.3% (95% CI 96.1%–99.4%).
Conclusion: For PC patients, the registration of VTE diagnoses in the DNRP is associated with a high PPV. We provide evidence that data from the DNRP are valid for studies on risk of VTE among cancer patients.
Keywords: positive predictive value, prostatic neoplasms, validation study, venous thromboembolism
Introduction
Prostate cancer (PC) is the most common cancer among men in Denmark.1,2 The average annual number of Danish men newly diagnosed with PC in the period 2007–2011 was 4,362.2 In the 10-year period from 2002 to 2011, PC incidence increased by 86%, while PC mortality remained stable.3,4 A large part of the increase in PC incidence is screening-induced, and PC incidence and prevalence rates are projected to increase further with the growing elderly population.5
The risk of venous thromboembolism (VTE) is increased among cancer patients, and is highest among patients with metastatic disease.6 In 2010, Severinsen et al used data from a cancer-free population and estimated that the positive predictive value (PPV) of in-hospital VTE diagnoses in Denmark was 75%.7 Severinsen et al also showed that the PPV varied by type of VTE (deep venous thrombosis [DVT] or pulmonary embolism [PE]), type of diagnosis (primary or secondary), and sex. Since the PPV is directly proportional to the prevalence of disease,8 that study provides a conservative PPV estimate for cancer-specific populations. The PPV of VTE in cancer patients is expected to be higher than in the general population.
The Danish National Registry of Patients (DNRP) is a registry of all admittances to national hospitals since 1977, as well as contacts with emergency rooms and outpatient clinics since 1995.9 The registration of incident PC in the DNRP has previously been shown to be reliable, with a PPV of 87% when compared to the registration of incident PC in the Danish Cancer Registry (DCR) as the reference standard.10 However, no previous study has examined the quality of VTE diagnoses among Danish cancer patients. Therefore, to support future studies on cancer and risk of VTE, this data-validation study aimed to estimate the PPV of VTE diagnoses related to PC patients in the DNRP.
Materials and methods
Study design and setting
We conducted a validation study set in the Central Denmark Region, restricted to admittances and contacts to Aarhus hospitals. The Central Denmark Region covers approximately 1.3 million residents (23% of the total Danish population).11 The public health care system provides the entire Danish population (5.6 million residents) with free and equal access to hospital services and treatments.12,13
Study population
Using the DNRP, we identified a total of 6,584 incident PC patients who were diagnosed at Aarhus hospitals within the period 1995–2012. Among these, 120 patients with PC were registered with VTE. VTE was strictly defined as either PE or DVT. All inpatient and outpatient admissions and discharges (both primary and secondary diagnoses) registered with VTE were included. However, registrations to emergency rooms were excluded since, these have previously been shown to be unreliable.7 We also queried a random sample of 120 PC patients not registered with VTE. Therefore, a total of 240 patients with PC were identified for detailed medical chart review, and these were spread among 20 different medical and surgical departments (see Figure 1). After review of the medical records, three patients from the VTE group and one patient from the non-VTE group were identified as not having PC and were therefore excluded. Two patients from the non-VTE group had a registered VTE – 2 and 15 years – prior to the PC diagnosis dates, and two patients from the VTE group were registered with VTE – 3 and 10 years – prior to their PC diagnosis dates. These four patients were also excluded (see Figure 1).
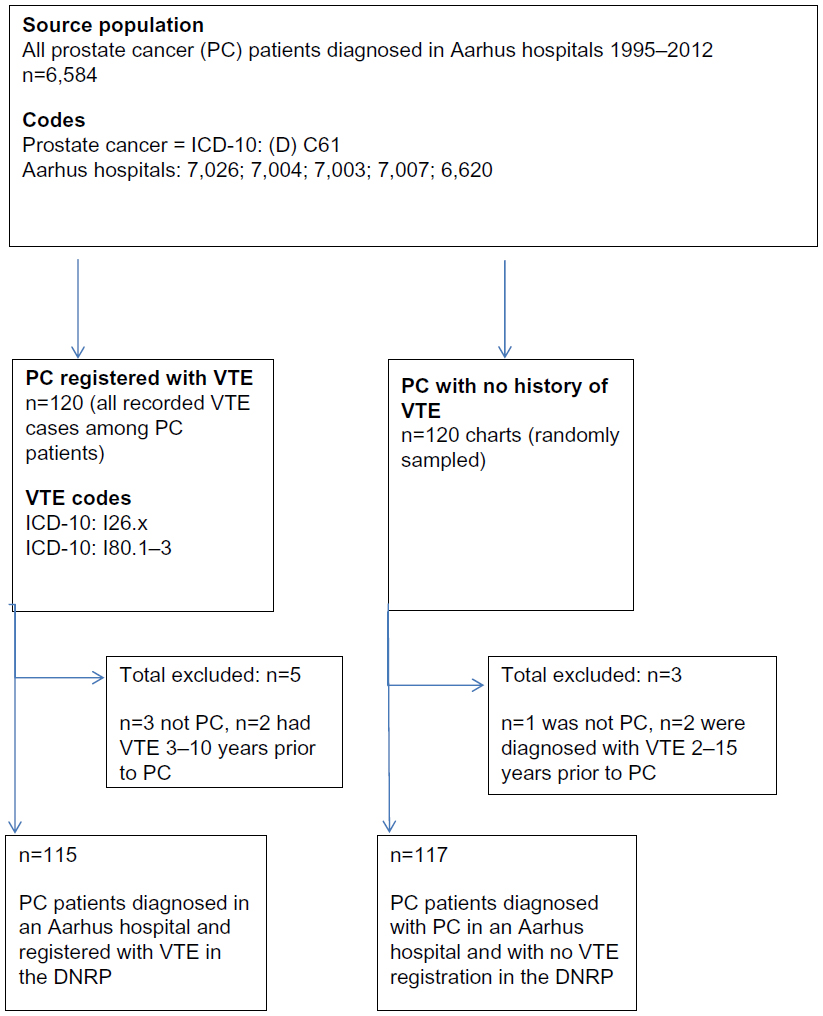 | Figure 1 Flow chart of PC patients selected for study sample. |
The Danish National Registry of Patients
The DNRP is a registry of all admittances to national hospitals since 1977, including contacts with emergency rooms and outpatient clinics since 1995.9 The registry contains data on dates of admission and discharge, diagnoses, procedures, some hospital-administered medications, and a unique ten-digit civil registration (CPR) number that all Danish residents are assigned upon birth or immigration.9 The CPR number allows for unambiguous data linkage across multiple registries.13 Diagnoses are coded by the treating physicians at the time of discharge using the International Classification of Diseases (ICD)-8 (1977–1993) and the ICD-10 (1994–present). Since 1996, surgical procedures have been coded by the Danish version of the Nordic Medico-Statistical Committee Classification of Surgical Procedures.
Medical record review
We retrieved patients’ medical records for review (n=240). The same physician reviewed all of the medical records. In the data abstraction, we confirmed/invalidated VTE diagnoses and collected supplemental data on metastases, history of recent surgery, related VTE diagnostics (eg, scans, D-dimer, etc,), and administered VTE treatments. Double data entry and proofreading of data were performed by two independent persons in order to minimize and control for eventual data-entry errors and typos. Patients who, according to the medical record, did not have a biopsy-verified PC or who were registered with VTE ≥2 years prior to the PC diagnosis date were then excluded from the analyses (see Figure 1).
Statistical analyses
We estimated the PPV, sensitivity, and specificity with corresponding 95% confidence intervals (CIs) to find the concordance between VTE diagnoses in the DNRP and the medical records.14 We estimated the corresponding 95% CIs using Jeffreys method.15 We computed descriptive statistics to describe and compare PC patients in the VTE group and PC patients in the non-VTE group. We also estimated the PPV of incident PC diagnoses in the DNRP and the sensitivity of VTE diagnostics among PC patients with VTE. Sampling from the DNRP was performed using SAS statistical software, version 9.2 (SAS Institute, Cary, NC, USA). All other data management and analyses were performed using STATA statistical software, version 12 (StataCorp, College Station, TX, USA).
Results
Characteristics
Table 1 summarizes the descriptive statistics for the study sample, including information extracted from medical record review on age, metastases, history of surgery, VTE-related diagnostics, and VTE-related treatments. Patients registered with VTE were slightly older (median age 73.2 years, interquartile range 59.6–86.8 years) than the patients registered without VTE (median age 72.0 years, interquartile range 60.4–83.6 years).
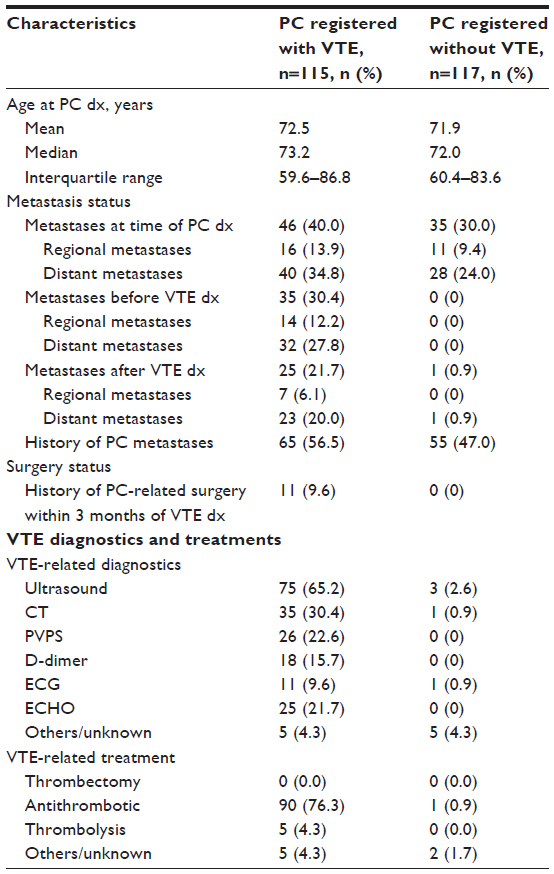 | Table 1 Characteristics of 232 PC patients included in study sample |
Among the PC patients registered with VTE, 40.0% (n=46) had evidence of metastases at the time of PC diagnosis, 30.4% (n=35) had evidence of metastases before VTE diagnosis, and 21.7% (n=25) had evidence of metastases occurring after the VTE diagnosis. In contrast, within the non-VTE group, 30.0% (n=35) had evidence of metastases at the time of PC diagnosis, no patients had evidence of metastases before the VTE diagnosis, and 0.9% (n=1) had evidence of metastases after the VTE diagnosis. Also, 9.6% (n=11) of patients in the VTE group had a history of PC-related surgery within 3 months of the VTE diagnosis, whereas no patients in the non-VTE group had a history of recent PC-related surgery.
Among patients registered with VTE, 65.2% (n=75) underwent an ultrasound examination, 30.4% (n=35) underwent a computed tomography examination, and 22.6% (n=26) underwent a pulmonary ventilation and perfusion scan (PVPS). As would be expected for those without a VTE diagnosis, only 2.6% (n=3) underwent an ultrasound, 0.9% (n=1) had a computed tomography scan, and no patients had a PVPS within the non-VTE group. With respect to treatment with antithrombotic drugs, again, consistent with expectations, 76.3% (n=90) were treated within the VTE group and only 0.9% (n=1) in the non-VTE group.
PPV, sensitivity, and specificity of VTE diagnosis among PC patients
The final study sample comprised 232 PC patients, of which 115 were registered with VTE and 117 without VTE in the DNRP. Based on our review of medical records, of the 115 patients registered with VTE, we confirmed 99 patients with VTE (ie, true positives) and found 16 to be erroneously coded with VTE (ie, false positives). Of the 117 patients registered without VTE, we confirmed 115 patients without VTE (ie, true negatives) and found two patients with VTE (ie, false negatives). Using the medical record review as the reference standard, we then computed the overall PPV of VTE diagnoses in the DNRP related to PC patients to be 86.1% (95% CI 78.9%–91.5%). The corresponding sensitivity was 98.0% (95% CI 93.8%–99.6%), and specificity was 87.8% (95% CI 81.4%–92.6%) (see Table 2). Finally, we also computed the PPV of the registration of incident PC in the DNRP to be 98.3% (95% CI 96.1%–99.4%), again using the medical record review as the reference standard (see Table 3).
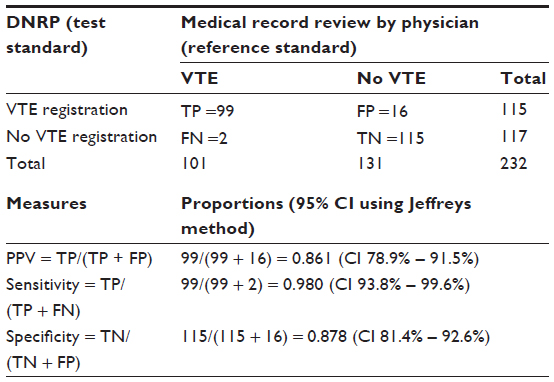 | Table 2 Measures of agreement and validity comparing reporting of VTE diagnoses among prostate cancer patients in the DNRP with patient medical records |
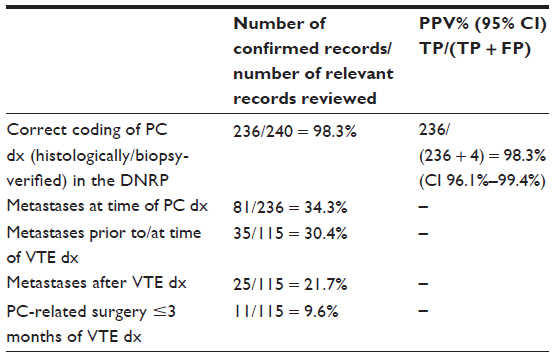 | Table 3 PPV of PC diagnosis in the DNRP and proportions of metastases and PC-related surgery |
Sensitivity of VTE diagnostics among PC patients
Table 4 summarizes our findings on the sensitivity of VTE diagnostic tests. Ultrasound and elevated D-dimer were the most sensitive VTE diagnostics among Danish PC patients, with a sensitivity of 94.1% (95% CI 86.6%–98.0%) and 54.8% (95% CI 39.8%–69.1%), respectively. Electrocardiography and echocardiography had the lowest sensitivity in VTE diagnostics, with sensitivity of 6.7% (95% CI 0.7%–27.2%) and 15.2% (95% CI 6.1%–30.1%), respectively.
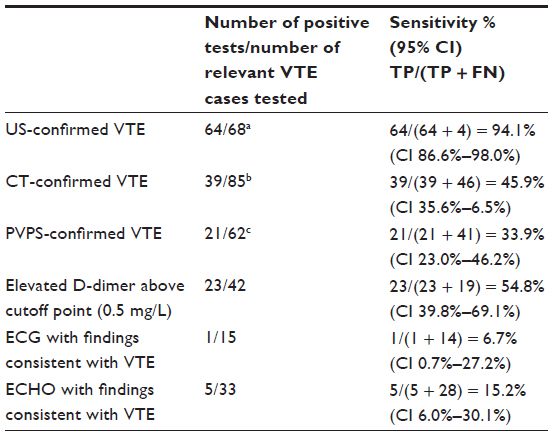 | Table 4 Sensitivity of VTE diagnostics among Danish PC patients |
Discussion
To summarize the key findings of this study, we found a high PPV (86%), sensitivity (98%), and specificity (88%) of the registration of VTE diagnoses in the DNRP related to PC patients. We also found a very high PPV (98%) of incident PC diagnoses in the DNRP. To our knowledge, this is the first study to investigate the quality of VTE diagnosis in the DNPR in a cancer-specific population.
We identified 16 PC patients who were registered with false-positive VTE. Interestingly, our detailed medical chart review showed that indeed eight of these patients were hospitalized/admitted with suspected VTE, but subsequent in-hospital confirmatory diagnostics ruled out the presence of VTE. Therefore, at least half of the false-positive findings could be attributed to systematic coding error by physicians. A previous study showed that asymptomatic superficial venous thrombosis and asymptomatic DVT occurs more frequently among cancer patients than noncancer patients, further illustrating that timely and valid VTE diagnosis is a particular challenge for cancer-specific populations.16 In 2010, Severinsen et al investigated a cancer-free population and showed that the PPV of in-hospital VTE diagnoses in Denmark was 75%.7 We showed that the PPV of VTE coding related to a cancer-specific population in the DNRP is higher, at 86.1%. We also found that the registration of incident PC in the DNRP is highly reliable, with a PPV of 98.3%. In a previous study, Gammelager et al found that the registration of incident PC in the DNRP had a PPV of 87%; however, that study compared registered DNRP cancer diagnoses to registered DCR diagnoses (where the DCR was the reference standard).10 In contrast, we used data extracted from medical records and case-by-case physician evaluation as the reference standard. Also, our findings showing relatively high sensitivity for D-dimer as a diagnostic measure support previous research.17,18 Finally, our estimates of sensitivity for PVPS, electrocardiography, and echocardiography diagnostic examinations are most likely underestimated, since these analyses were not restricted to PE patients.
Our study has several notable strengths and features. Most importantly, we linked national registry data to collect information on all PC and VTE diagnoses and related therapies provided in the country. We were thus able to identify all PC patients registered with and without VTE in the central region of Denmark. The sample size was sufficient to provide good precision of the PPV, specificity, and sensitivity estimates. Detailed medical chart review was performed by one physician, and all diagnoses were validated/invalidated based on the reviewing physician’s global assessment of the information available in the medical charts. Finally, double data entry was performed by two independent persons in order to minimize and control for eventual data-entry errors and typos.
Nevertheless, this study also has some limitations. Firstly, we included data from only one region in Denmark, which could limit the generalizability of our findings to other regions or countries. However, data were included from five different hospitals in the region, all of which are representative of other hospitals in Denmark. Furthermore, the homogeneous and standardized health care system in Denmark makes it possible to generalize our findings to other regions.13,19 Secondly, the medical record reviewer was not blinded to the VTE-registration status, which potentially could have biased the evaluation process when confirming/invalidating VTE status. Thirdly, the quality and amount of data recorded in the medical records varied, which meant that we had more details and data on some patients than on others. Lastly, we excluded two patients with no VTE registration, which according to the medical records did have VTE years before their PC diagnoses. Similarly, we excluded two patients registered with VTE, but where the VTE date was several years before the PC diagnosis. These patients were excluded on the premise that their VTE diagnoses were not likely to be related to their PC diagnoses, but these patients might nevertheless have had occult PC at the time of the VTE. However, the inclusion of these four excluded patients would have only marginally affected the PPV estimate that is reported here.
Conclusion
In conclusion, we found high PPV of VTE diagnoses (86%) among PC patients, as well as high PPV of incident PC diagnoses (98%) in the DNRP. Data on PC and VTE diagnoses in the DNRP have high validity. This study further substantiates that the DNRP is a valuable and valid data source for epidemiological studies on cancer and risk of VTE.
Acknowledgments
All coauthors are salaried employees of Aarhus University and/or Aarhus University Hospital. Dr Nguyen-Nielsen was funded by a PhD Fellowship from Aarhus University, the Department of Clinical Epidemiology, and private grants from Grosserer AV Lykfeldt og Hustrus Legat, Thora og Viggo Groves mindelegat, and Einar Willumsens legat. This study was also supported by a grant from the Danish Cancer Society (R73-A4284-13-S17) and from the Aarhus University Research Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
Ugeskrift for Læger. Prostatakræft, kirurgisk behandling af lokaliseret sygdom – nutidens og fremtidens udfordring. [Prostate cancer, surgical treatment of localized disease - present and future challenges]. 2008. Available from: http://www.laeger.dk/portal/page/portal/LAEGERDK/UGESKRIFT_FOR_LAEGER/TIDLIGERE_NUMRE/2008/UFL_EKCMA_2008_34/UFL_EKCMA_2008_34_53525. Accessed May 13, 2014. Danish. | |
Danish Cancer Society. Statistik om prostatakræft. [Statistics about prostate cancer]. 2014. Available from: http://www.cancer.dk/Hjaelp+viden/kraeftformer/kraeftsygdomme/prostata/statistik+prostatakraeft. Accessed August 5, 2014. Danish. | |
State Serum Institute. Cancerregisteret: Tal og Analyser. [Cancer registry: data and analysis]. Copenhagen: SSI; 2011. Available from: http://www.ssi.dk/~/media/Indhold/DK%20-%20dansk/Sundhedsdata%20og%20it/NSF/Registre/Cancerregisteret/Cancerregisteret%202011.ashx. Accessed October 22, 2013. Danish. | |
State Serum Institute. Dødsårsagsregisteret 2010: Tal og Analyser. [Death register 2010: statistical analysis]. Copenhagen: SSI; 2011. Available from: http://www.ssi.dk/~/media/Indhold/DK%20-%20dansk/Sundhedsdata%20og%20it/NSF/Registre/Dodsaarsagsregisteret/D%C3%B8ds%C3%A5rsagsregisteret%202012.ashx. Accessed October 22, 2013. Danish. | |
Outzen M, Brasso K, Martinussen N, et al. Prostate cancer in Denmark 1978–2009 – trends in incidence and mortality. Acta Oncol. 2013;52(4):831–836. | |
Wun T, White RH. Epidemiology of cancer-related venous thromboembolism. Best Pract Res Clin Haematol. 2009;22(1):9–23. | |
Severinsen MT, Kristensen SR, Overvad K, Dethlefsen C, Tjønneland A, Johnsen SP. Venous thromboembolism discharge diagnoses in the danish national patient registry should be used with caution. J Clin Epidemiol. 2010;63(2):223–228. | |
Juul S. Epidemiologi og Evidens. [Epidemiology and evidence]. 6th ed. Copenhagen: Munksgaard; 2008. Danish. | |
Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(Suppl 7):30–33. | |
Gammelager H, Christiansen CF, Johansen MB, Borre M, Schoonen M, Sørensen HT. Quality of urological cancer diagnoses in the Danish National Registry of Patients. Eur J Cancer Prev. 2012;21(6):545–551. | |
Danske Regioner. Statistik. [Statistics]. Available from: http://www.regioner.dk/om+regionerne/statistik+ny. Accessed November 10, 2013. Danish. | |
Statistics Denmark. Population and population projections. Available from: http://www.dst.dk/en/Statistik/emner/befolkning-og-befolkningsfremskrivning.aspx. Accessed November 12, 2013. | |
Thygesen LC, Ersbøll AK. Danish population-based registers for public health and health-related welfare research – a description of Danish registers and results from their application in research. Scand J Public Health. 2011; 39(7 Suppl):7–209. | |
Weiss N. Clinical epidemiology. In: Rothman K, Greenland S, Lash T, editors. Modern Epidemiology. 3rd ed. Alphen aan den Rijn, the Netherlands: Wolters Kluwer; 2008:642–646. | |
Lawrence D, Brown T, Cai T, DasGupta A. Interval estimation for a binomial proportion. Stat Sci. 2001;16(2):101–133. | |
Gary T, Belaj K, Steidl K, et al. Asymptomatic deep vein thrombosis and superficial vein thrombosis in ambulatory cancer patients: impact on short-term survival. Br J Cancer. 2012;107(8):1244–1248. | |
Ay C, Dunkler D, Pirker R, et al. High D-dimer levels are associated with poor prognosis in cancer patients. Haematologica. 2012;97(8):1158–1164. | |
Ay C, Vormittag R, Dunkler D, et al. D-dimer and prothrombin fragment 1 + 2 predict venous thromboembolism in patients with cancer: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2009;27(25):4124–4129. | |
Danske Regioner. Den Danske Kvalitetsmodel. [The Danish quality model]. Available from: http://www.regioner.dk/sundhed/kvalitet+og+forskning/den+danske+kvalitetsmodel. Accessed May 13, 2014. Danish. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.