")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Quality of Respiratory Infection Disease Prevention in Outpatient and Emergency Departments in Hospitals in Inner Mongolia, China: An Exit Poll Survey
Authors Xie Y , McNeil E , Fan Y, Chongsuvivatwong V , Zhao X, Sriplung H
Received 7 February 2020
Accepted for publication 21 May 2020
Published 2 June 2020 Volume 2020:13 Pages 501—508
DOI https://doi.org/10.2147/RMHP.S248772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Yijing Xie,1,2 Edward McNeil,2 Yancun Fan,1 Virasakdi Chongsuvivatwong,2 Xingsheng Zhao,3 Hutcha Sriplung2
1Health Management Faculty and Research Institute for Health Policy of Inner Mongolia, Inner Mongolia Medical University, Hohhot, Inner Mongolia, People’s Republic of China; 2Epidemiology Unit, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand; 3Inner Mongolia People’s Hospital, Hohhot, Inner Mongolia, People’s Republic of China
Correspondence: Hutcha Sriplung
Epidemiology Unit, Faculty of Medicine, Prince of Songkla University, 15 Kanchanawanit Road, Hat Yai, Songkhla 90110, Thailand
Tel +66 7 445 1165
Fax +66 7 442 9754
Email [email protected]
Purpose: Measures to prevent respiratory infection diseases (RIDs) in hospitals are important to protect both patients and physicians. In 2003, an outbreak of severe acute respiratory syndrome occurred in Inner Mongolia Autonomous Region (IMAR) of China. We aimed to evaluate competency in RID prevention procedures in terms of hospital performance and physician behavior.
Patients and Methods: We conducted a cross-sectional study in 10 tertiary general public hospitals in 3 cities of IMAR. In each hospital, we chose the respiratory and ear–nose–throat outpatient departments (OPDs) and the emergency department (ED) to invite patients with symptoms of cough to join the study before they consulted a physician. After their consultation, we asked the patients to complete a checklist to score the performance of the departments and the behavior of their physicians in terms of RID prevention practices according to international professional guidelines.
Results: From 711 respondents, in the domain of hospital performance, display of posters on directive to wash hands after coughing/sneezing had an average score of 0.452 (range 0– 1), while other cough etiquette items had scores averaging between 0.33 and 0.39. The average score for air ventilation was 0.66. For physicians’ performance, informing patients the location of handwashing facilities scored the highest (0.62), while low scores were seen for offering a mask to coughing patients (0.14) and encouraging coughing patients to distance themselves from others (0.17). Most RID prevention procedures received low scores in EDs in both hospital performance and physician behavior domains.
Conclusion: Hospitals in IMAR should improve their performance in RID prevention procedures, especially in giving information to RID patients through the display of posters. The practice of physicians in preventing respiratory infection spread was suboptimum. ED staff and hospital administrators should improve their procedures to prevent the spread of respiratory infections, especially given the increasing occurrences of global pandemics such as COVID-19.
Keywords: hospital performance, physician behavior, spread of respiratory infections, real patients survey
Introduction
Respiratory infectious diseases (RIDs), droplet or airborne transmission, can trigger nosocomial or healthcare-associated infections in health care, which, although common, are preventable.1 When patients with RIDs come to the gateway of the hospital system, the infection can easily spread to other patients and healthcare workers without notice. Prevention of RIDs is a vital indicator to improve the quality of hospital safety.2 Hospital safety is one of six domains of health care quality according to the World Health Organization.3 Thus, exploring the prevention of RIDs can guide healthcare workers, hospital managers, and policymakers to improve aspects of the quality of hospital care.
From guidelines of the World Health Organization,4–6 the National Center for Disease Control and Prevention,7,8 and elsewhere,9,10 the prevention and control of respiratory infectious diseases are critical in disease control. Prompt, competent, and economically efficient prevention measures include the provision of handwashing facilities and offering masks or tissues to patients who have a cough and asking them to keep a distance from other patients. From those guidelines, to alert the patients to notify staff and to adopt respiratory hygiene procedures within the hospital vicinity is an essential recommendation.
Following the severe acute respiratory syndrome (SARS) outbreak in 2002, China was the first country where the mutated virus spread across the world. In January 2020, an outbreak of coronavirus in China alarmed the world that RIDs prevention is an important global concern.
There are laws and policies about respiratory infection prevention aiming to improve safety in hospitals in different countries, including China.11–13 In Inner Mongolia Autonomous Region of China (IMAR), where the prevalence of tuberculosis is the third highest in all provinces of China and the prevalence of tuberculosis among healthcare workers is also high,14,15 there is still no evidence or documentation of in-hospital spread of RIDs and the effectiveness of prevention measures. Hospitals need effective means to mitigate outbreaks and control them, especially at outpatient departments (OPDs), and emergency departments (EDs), the main gateways to hospitals.
There are two sets of safety protocols to be implemented at hospital entrances. Hospitals must warn patients, via the display of posters, that they are capable of spreading their infections to the others and advise them how to reduce the spread. Hospital personnel should engage in respiratory triage and promptly apply respiratory prevention and control procedures.7,8,16 When hospital personnel encounter a symptomatic patient, they should take the patient’s history and decide on respiratory prevention measures, including isolation.
The exit poll method, initially used for political elections, can be modified to monitor the performance of the health services by obtaining experiences and opinions from symptomatic patients. Trained interviewers can be used to debrief patients who have just received the service using a simple questionnaire asking their experience on the service in terms of hospital and physicians’ performance on the respiratory infection prevention methods. A survey can be self-administered by the patients themselves or receive assistance from trained interviewers.
This study was conducted in IMAR, northern China. The objective is to evaluate hospitals’ performance in respiratory disease control and physicians’ behaviors on RID prevention. A secondary objective is to compare results in three settings where patients with respiratory symptoms, such as coughing, usually seek care: the respiratory and ENT OPD and the emergency department.
Patients and Methods
We conducted a cross-sectional study from January to March 2018 in 10 tertiary general public hospitals in 3 cities of Inner Mongolia, China. In each city, the duration of the survey was approximately 10 days. The ten hospitals included three in Hohhot, five in Baotou, and two in Ordos. In each hospital, we chose outpatient clinics of the respiratory and ENT departments and the ED. We visited the hospital directors and managers to obtain informed consent from the hospitals. In each visit, patients with cough agreed to answers our questionnaires, they were provided informed consent as well as the checklists.
Exit Poll Procedure
At the study settings, we approached patients who had symptoms of cough and, after explaining the study, asked them to join the study. Those who agreed were asked to consult the doctor and, after completion, return to the researcher and complete a checklist. We recruited 23 trained undergraduates as interviewers to assist the patients in completing the checklist. To reduce the Hawthorne effect of healthcare workers being observed by the research team, we conducted the survey at least two months after obtaining informed consent from each hospital.
Study Setting
The 10 tertiary hospitals selected represented institutes offering high-quality healthcare. Two of the hospitals in Hohhot were provincial-level hospitals, one of which was an affiliated hospital of Inner Mongolia Medical University. The third one was a prefecture-level hospital. Of the 5 hospitals in Baotou, two were teaching hospitals of Inner Mongolia Medical University, 2 were affiliated hospitals of Baotou Medical College, and 1 was a teaching hospital of Baotou Medical College. Of the 2 hospitals in Ordos, 1 was a prefecture-level hospital and the other was a county-level hospital.
We chose outpatient clinics of the respiratory and ENT departments and the emergency department because patients with RID symptoms usually present to these places.
Checklist Development
We designed the framework of the checklist based on the guideline of the US Center for Disease Control for outpatient settings. We added into the theme the guidelines on respiratory infection prevention and control from the World Health Organization and the Chinese Ministry of Health and the professional standard.
There were two domains in the checklist: (1) hospital performance: at the entrance to each department, signs or posters displaying respiratory infection prevention; and whether the examination room and waiting area are located in an open-air environment and/or has proper ventilation, and (2) the physicians’ behavior on respiratory infection prevention.
There were 5 items under the hospital performance domain. The first 4 items concern the hospital’s display of posters providing relevant information to patients on (1) awareness of RID symptoms, (2) covering mouths/noses when coughing/sneezing, (3) use and disposal of tissues, and (4) wash hands after coughing/sneezing. The 5th item concerns whether the examination room is located in an open-air environment and/or has proper ventilation.
The physicians’ behavior and responses during the patient consultation consisted of 5 items. These included 2 items about management of respiratory secretions: (1) providing tissues and informing patients the location of receptacles for the disposal of used tissues, and (2) informing patients the location of hand-washing facilities, and 3 items about RID prevention: (3) offering a mask to coughing patients without the patient’s request, (4) giving a mask on request, (5) encouraging coughing patients to distance themselves from others.
All 10 items in the 2 domains were rated as yes, no, or do not know. Patients answered “yes” when they observed or noticed the presence of the posters or signage in the department or the physicians’ behaved as described in the checklist. Patients answered “no” when they did not observe or receive the advice, and “do not know” option allowed patients to be uncertain whether or not the item was present or done. Patients filled in the checklist after they completed consulting the doctors.
Statistical Analysis
The data format was nested and multilevel as physicians in each clinic were observed more than once by different patients. The physician code was one of the items in the questionnaire to link the records of the same physician in the analysis. The patients’ perceptions of physicians and hospital items were grouped into “yes”, indicating that the action was perceived by the patients, “no”, indicating that the action was not observed, and “do not know”, indicating that although the patient did not observe the action, he/she was not confident to state that it did or did not happen. A linear mixed-effects model was fit to determine the department effect on each item of the hospital performance domain after adjusting for city and where the hospital was treated as the random effect. The respiratory OPD was treated as the reference group for comparative purposes. For the 5 items on the checklist, we scored 1 if, according to the patients, the hospital’s performance matched what was described in the checklist, otherwise 0. The average score for each department was calculated. Similar linear mixed-effects models were fitted to the items in the physician behavior domain.
We checked content validity and Cronbach’s alpha coefficient to evaluate the relevance and internal consistency of the checklist. For the hospital performance, Cronbach’s alpha was 0.81, and for physicians’ performance, Cronbach’s alpha was 0.65.
Results
A total of 711 (98%) out of 725 patients agreed to participate in this study, including 347 males and 364 females. Participants had an average (standard deviation) age of 45.4 (16.4) years. About half of the patients finished high school/vocational school or junior college and above (Table 1). The majority had a cough lasting less than two weeks and had no fever. From 610 checklists returned with a physician identification code, a total of 96 physicians, 32 males, and 64 females, were identified. Among these, 43 worked in a respiratory OPD, 40 in an ENT OPD, and 13 in ED. Twenty-one physicians worked in Hohhot, 61 in Baotou, and 14 in Ordos.
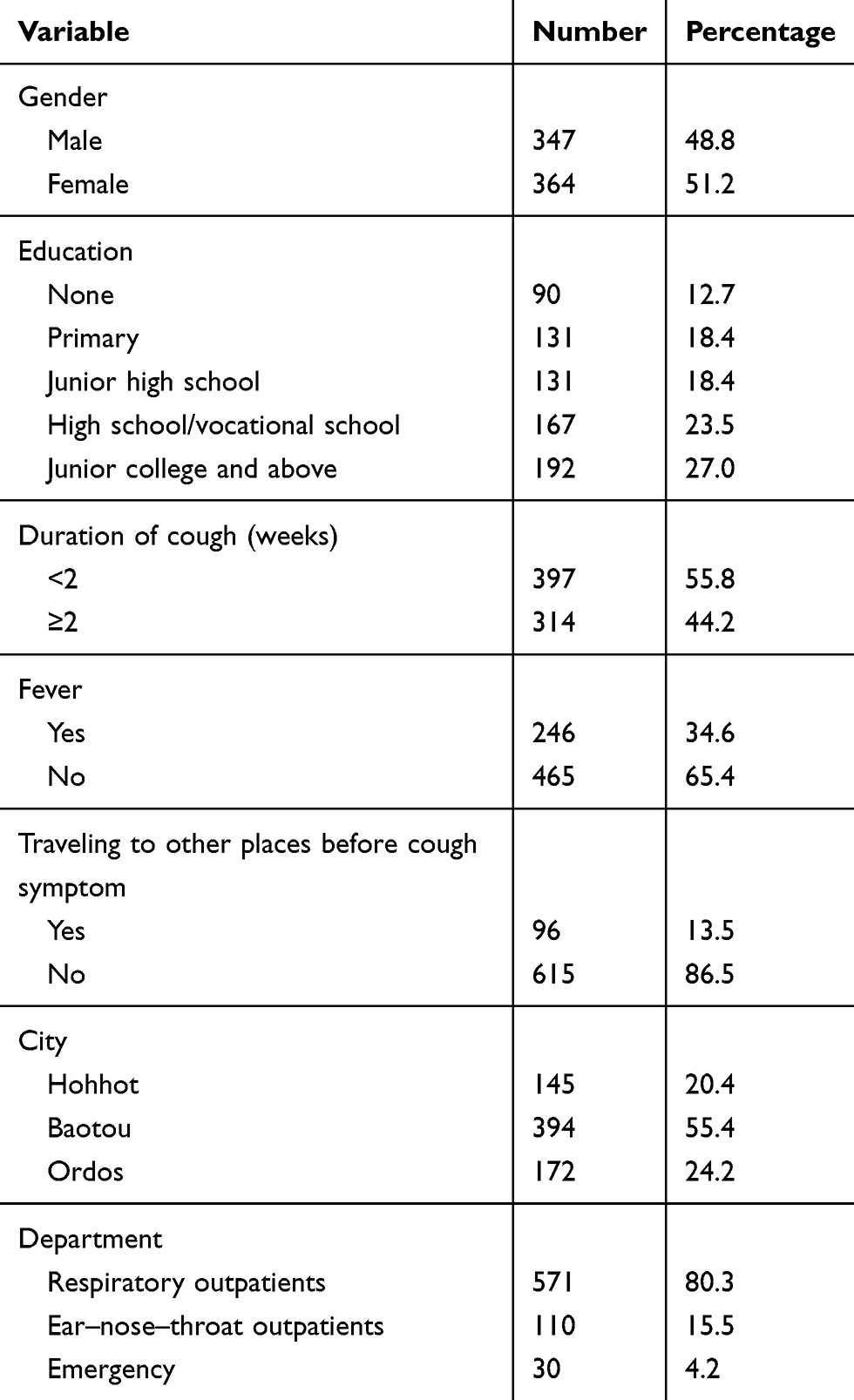 |
Table 1 Frequency and Percentage of Demographic Characteristics of Study Patients |
In the domain of hospital performance, display of signs or posters on directives to wash hands after coughing/sneezing (H4) had the highest average score of 0.45 (Table 2). Display of signs to raise awareness of RID and other cough etiquette (H1-H3) had average scores ranging from 0.33 to 0.39. In terms of air ventilation, the patients gave an average score of 0.66. For physicians, the average score for informing patients the location of receptacles for disposal of used tissues was 0.31 while for informing the location of hand-washing facilities was 0.62. Offering a mask to a coughing patient had an average score of 0.14, while the average score was 0.48 if the patient requested one. Physicians received an average score of 0.17 for encouraging coughing patients to distance themselves from others.
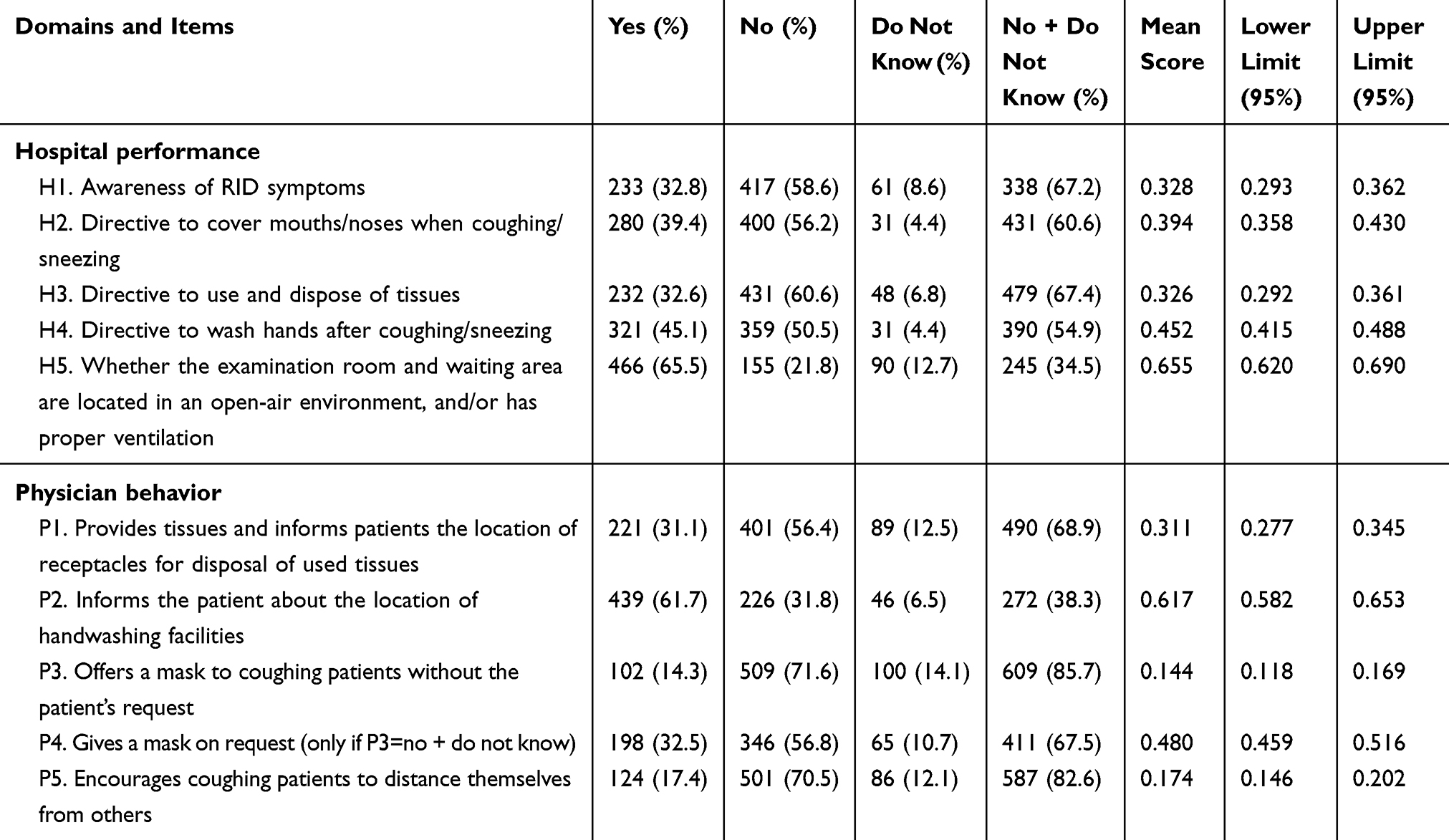 |
Table 2 Mean Scores and 95% Confidence Intervals for Items in the Respiratory Prevention and Control Checklist |
Table 3 shows the results of the multivariate linear mixed-effect model for items in the hospital performance domain. We observed consistently significantly lower average performance scores for the emergency department compared to the respiratory OPD. However, the average performance scores between the respiratory and ENT OPDs were not statistically different in any item.
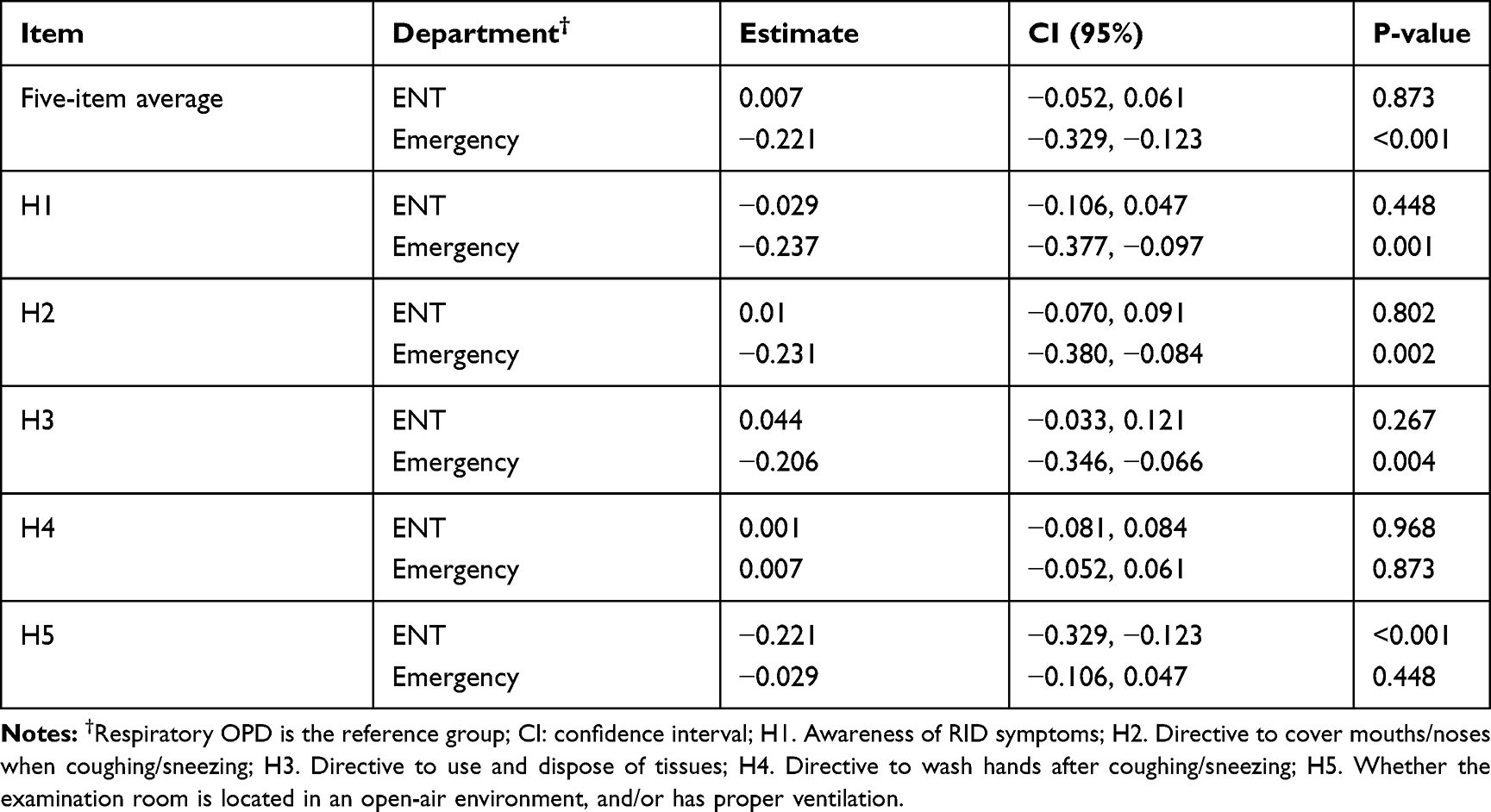 |
Table 3 Differences in Average Scores Between Respiratory OPD and the Other 2 Departments for the 5 Items in the Hospital Performance Domain |
Table 4 shows the results of the multivariate linear mixed-effect model for items in the physician behavior domain. Overall, physicians from ENT OPD had significantly higher behavior scores than those from respiratory OPD. The practice of providing tissues and informing patients about the location of facilities for the disposal of used tissues (P1) and hand-washing (P2) was not significantly different among the three departments. ED physicians offering a mask without the patient’s request (P3) had significantly lower scores compared to those in the respiratory OPD. Scores on providing patients with a mask on request (P4) for physicians in ENT OPD were higher than those in the respiratory OPD. Scores on asking cough patients to distance themselves from other patients (P5) among ENT physicians were significantly higher than respiratory physicians but significantly lower than physicians working in ED.
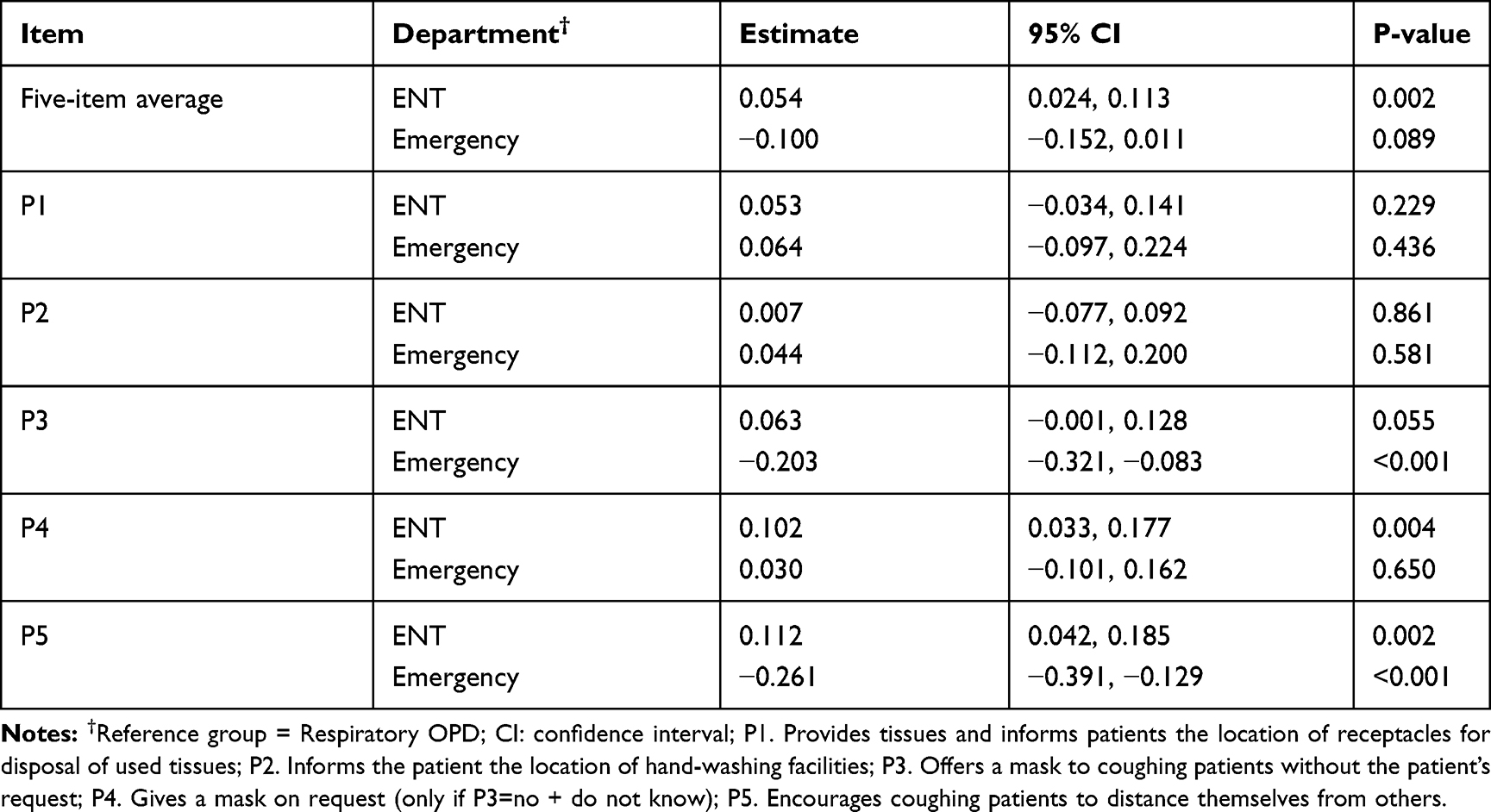 |
Table 4 Differences in Average Scores Between Respiratory OPD and the Other 2 Departments for the 5 Items in the Physician Behavior Domain |
Figure 1 shows the relationship between average hospital performance and physician behavior scores stratified by city separately for the 3 departments. In respiratory OPDs (Figure 1C) there was a positive correlation between the two domains for all cities. That is, as physicians scored higher so did the department’s performance. A similar relationship was seen for ENT OPD and Emergency departments, except for ENT OPD in Hohhot where a negative correlation was seen. In general, ED physicians’ scores were lower than the two OPDs.
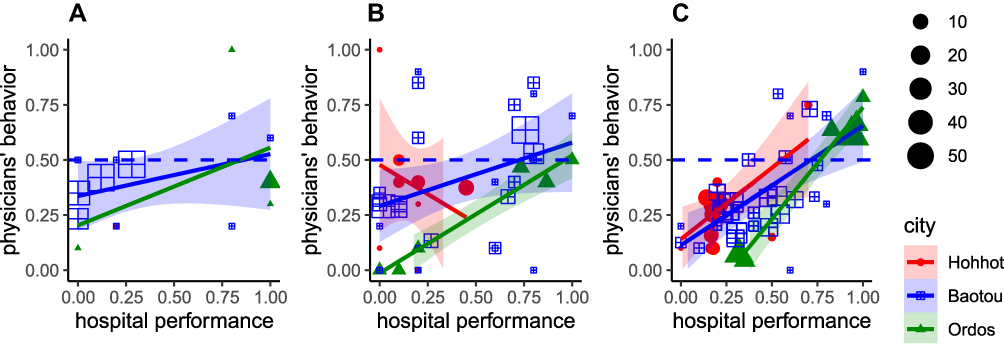 |
Figure 1 Scatterplot of the average hospital performance (x-axis) and physicians’ behavior (y-axis) scores stratified by city for the 3 departments; (A) Emergency, (B) ENT OPD, and (C) respiratory OPD. The red lines and red solid circles represent Hohhot, black lines and grids represent Baotou, and green line and triangles represent Ordos. Each symbol represents one physician and the size of the symbol is proportional to the number of patients who consulted that particular physician. The horizontal dashed line represents a physicians’ behavior score of 0.5. |
Discussion
This survey of 10 hospitals in three cities of Inner Mongolia evaluated health safety domains in hospital performance and physician behavior concerning respiratory disease prevention. We found that most of the departments scored well in the display of posters of directive to wash hands. However, scores for posters explaining how patients should manage their symptoms were low. Signage and posters are simple communication methods for hospitals to inform patients how to behave within a hospital. The World Health Organization recommends the use of visual warnings to protect patients.4–7,17 One study also advised posting visual alerts in appropriate languages at the entrance of healthcare facilities.16 Though the visual media do not assure the proper practice of visiting patients, within a hospital environment, they have a strong influence on the patients as they should follow the hospital rules and regulations.
OPDs and EDs are the first point of contact to a hospital for patients who come with symptoms of a disease, including RIDs and immuno-compromised conditions susceptible to nosocomial infections. The barrier to disease spreading must be strong enough to prevent the spread. Our findings indicate that physicians employed in the 3 study departments of our study hospitals fail to communicate with patients on RID prevention, especially offering masks to coughing patients and encouraging them to distance themselves from others, thus making them the primary source of disease transmission. Tuberculosis control programs and protocols to prevent newly emerging respiratory diseases such as influenza focus on the hospital gateways such as OPDs and EDs.18,19
The level of advice given by physicians to patients to manage their symptoms was insufficient. If an infectious disease outbreak should occur, these hospitals could not prevent the outbreak and could be a source for further disease spread to surrounding areas. It is conceivable that low-cost and straightforward interventions would be useful for reducing the transmission of epidemic respiratory diseases. Offering a mask to coughing patients helps prevent the spread of respiratory infectious diseases. Long-term implementation of some routine measures is challenging without the threat of an epidemic in a hospital.20
In the SARS outbreak in 2003, Inner Mongolia was one of the provinces in China where the World Health Organization declared a disastrous area. Hospital personnel were alerted by a case study which modelled the propagation of SARS infection.21 When the outbreak had a long intermission, and some other diseases intervened, health personnel might have less concern about cough symptoms and the protocols to prevent the spread of RID infection.
We observed a significantly weaker performance of the emergency department than the two OPDs in the models of hospital performance (Table 3) and physician behavior (Table 4). The scores between the respiratory and ENT OPDs were not statistically different in almost all items. The fact that physicians in the Emergency department do not effectively manage cough patients suggests they may be overwhelmed by patients or give more priority to more critically ill patients. This workload may weaken the barrier of respiratory infectious disease prevention of nosocomial infection in hospitals. In our study, the number of patients with cough in EDs was lower than in the other departments. The percentage of patients with cough in EDs differs from country to country according to the hospital system designed to fit the population culture and health system of the country. Emergency departments should conduct the RID prevention into routine patient safety management,22 and the weak point must be managed successfully to avoid leakage of RIDs into the hospital.
Due to the nature of this study that it was a multi-hospital which represented populations and hospitals in the middle area of Inner Mongolia and the numerosity of the exit poll samples, the results could be inferred to the whole areas of IMAR. In general, there was a positive correlation between the performance of hospitals and physicians, except in Hohhot in which the healthcare worker’s scores were negatively associated with the hospital scores. The reasons for this are not clear. It could be a random negative correlation occurring once in many measurements. There was no effect of city on both hospitals’ performance and physicians’ behavior scores (result not shown).
Limitations
Since we purposively selected 10 tertiary public general hospitals in 3 cities, our results may not represent all tertiary public general hospitals in Inner Mongolia. For convenience, we chose only two outpatient departments and the emergency department as our study settings. We did not include pediatric or dental OPDs which have a high risk of respiratory infection.23,24 Although we instructed the patients to record the behaviors of physicians and the performance of the hospitals, it was possible that their observations did not reflect the actual situation. Such the difference between the poll results and the real situation depends on sampling populations and the change in patients’ perception over time. We might have observed a strong difference in the results if we could have conducted another study after the COVID-19 pandemic. The sample size of the emergency department, especially in Hohhot and Ordos, was too small to show the real situation of hospital performance and physicians’ behavior; however, subset analysis of emergency departments was not our main objective. Finally, this study only focused on physicians’ behavior, not of other healthcare workers.
Conclusion
The hospitals providing appropriate ventilation facilities were satisfactory. However, the practice of physicians providing a mask to coughing patients was unsatisfactory. Although the physicians’ behavior improved after the patients’ requested a mask, the quality of preventing the spread of respiratory infection is considered suboptimum. Emergency departments were the worst offenders among the hospital gateways for incoming infectious agents. Physicians’ behavior to prevent RID transmission by coughing or sneezing patients must be a routine practice, especially given the increasing occurrences of global pandemics such as SARS, MERS, and COVID-19.
Acknowledgments
This study is a part of the first author’s thesis in partial fulfillment of the requirements for a Ph.D. at Prince of Songkla University, Thailand, and the China Medical Board under the project of ”A second collaborative program to improve the health research capacity of western medical universities in China and Prince of Songkla University”. The authors are grateful to the Inner Mongolia People’s Hospital and Research Institute for Health Policy of Inner Mongolia, Inner Mongolia Medical University, and would also like to thank all participants enrolled in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Haque M, Sartelli M, McKimm J, Abu Bakar M. Health care-associated infections-an overview. Infect Drug Resist. 2018;11:2321–2333. doi:10.2147/IDR.S177247
2. Mehta Y, Gupta A, Todi S, et al. Guidelines for prevention of hospital acquired infections. Indian J Crit Care Med. 2014;18(3):149–163. doi:10.4103/0972-5229.128705
3. World Health Organization. Quality of Care: A Process for Making Strategic Choices in Health Systems. Geneva, Switzerland: World Health Organization; 2006.
4. World Health Organization. Prevention of Hospital-Acquired Infections: A Practical Guide. Geneva, Switzerland: World Health Organization; 2002.
5. World Health Organization. WHO Policy on TB Infection Control in Health-Care Facilities, Congregate Settings and Households. Geneva: World Health Organization; 2009.
6. World Health Organization. Infection Prevention and Control of Epidemic-And Pandemic-Prone Acute Respiratory Diseases in Health Care: WHO Interim Guidelines. Geneva: World Health Organization; 2007.
7. National Center for Emerging and Zoonotic Infectious Diseases, Division of Healthcare Quality Promotion. Guide to infection prevention for outpatient settings: minimum expectations for safe care; 2016. Available from: https://www.cdc.gov/infectioncontrol/pdf/outpatient/guide.pdf.
8. U.S. Department of Health and Human Services Centers for Disease Control and Prevention. Update: recommendations for Middle East respiratory syndrome coronavirus (MERS-CoV). MMWR Morb Mortal Wkly Rep. 2013;62(27):545–560.
9. Steinkuller F, Harris K, Vigil KJ, Ostrosky-Zeichner L. Outpatient infection prevention: a practical primer. Open Forum Infect Dis. 2018;5(5):ofy053. doi:10.1093/ofid/ofy053
10. MacIntyre CR, Chughtai AA. Facemasks for the prevention of infection in healthcare and community settings. BMJ. 2015;350(apr09 1):h694. doi:10.1136/bmj.h694
11. China National Health and Family Planning Commission. Guideline of Control of Healthcare Associated Infection Outbreak; 2016.
12. Standing Committee of the National People’s Congress Law of the People’s Republic of China on Prevention and Treatment of Infection Diseases (2013 Amendment); 2013. Available from: http://www.lawinfochina.com/display.aspx?id=14881&lib=law.
13. Office of The Legislative Counsel, U.S. House of Representatives. Public health service act; 2019. Available from: https://legcounsel.house.gov/Comps/PHSA-merged.pdf.
14. Ma E, Ren L, Wang W, et al. Demographic and socioeconomic disparity in knowledge about tuberculosis in Inner Mongolia, China. J Epidemiol. 2015;25(4):312–320. doi:10.2188/jea.JE20140033
15. He GX, Wang LX, Chai SJ, et al. Risk factors associated with tuberculosis infection among health care workers in Inner Mongolia, China. Int J Tuberc Lung Dis. 2012;16(11):1485–1491. doi:10.5588/ijtld.12.0193
16. Al Harbi IS, Gupta SK. Use of visual triage in the early identification and isolation of acute respiratory infection cases for the control of hospital outbreak/infection in reference to middle east respiratory syndrome-corona virus (MERS CoV). Int J Med Pub Health. 2019;9(1):8–12. doi:10.5530/ijmedph.2019.1.3
17. Jensen PA, Lambert LA, Iademarco MF, et al. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Recomm Rep. 2005;54(RR–17):1–141. doi:10.1037/e548702006-001
18. Lee JY. Tuberculosis infection control in health-care facilities: environmental control and personal protection. Tuberc Respir Dis (Seoul). 2016;79(4):234–240. doi:10.4046/trd.2016.79.4.234
19. Liang SY, Theodoro DL, Schuur JD, Marschall J. Infection prevention in the emergency department. Ann Emerg Med. 2014;64(3):299–313. doi:10.1016/j.annemergmed.2014.02.024
20. Jefferson T, Del Mar CB, Dooley L, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. 2011;7:Cd006207. doi:10.1002/14651858.CD006207.pub4
21. Ng TW, Turinici G, Danchin A. A double epidemic model for the SARS propagation. BMC Infect Dis. 2003;3(1):19. doi:10.1186/1471-2334-3-19
22. Tham KY. An emergency department response to severe acute respiratory syndrome: a prototype response to bioterrorism. Ann Emerg Med. 2004;43(1):6–14. doi:10.1016/j.annemergmed.2003.08.005
23. Daniel OJ, Adejumo OA, Abdur-Razzaq HA, Ebunoluwa JO. Trend of childhood TB case notification in Lagos, Nigeria, 2011–2014. Int J Mycobacteriol. 2015;4(3):239–244. doi:10.1016/j.ijmyco.2015.05.010
24. Seddon JA, Shingadia D. Epidemiology and disease burden of tuberculosis in children: a global perspective. Infect Drug Resist. 2014;7:153–165. doi:10.2147/idr.S45090
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.