")
Back to Journals » Patient Preference and Adherence » Volume 16
Quality of Life Status and Influencing Factors Among Patients with Deep Vein Thrombosis
Authors Huang J, Liu X, Wu Z , Ma Y
Received 20 December 2021
Accepted for publication 18 March 2022
Published 8 April 2022 Volume 2022:16 Pages 949—956
DOI https://doi.org/10.2147/PPA.S353128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Jing Huang,1,2 Xiao-yan Liu,1,2 Zhou-peng Wu,3 Yu-kui Ma3
1Department of Vascular Surgery, West China Hospital, Sichuan University, West China School of Nursing, Sichuan University, Chengdu, People’s Republic of China; 2Department of Orthopedics, Orthopedic Reaserch Institute, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 3Department of Vascular Surgery, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Zhou-peng Wu, Department of Vascular Surgery, West China Hospital, Sichuan University, No. 37 Guoxuexiang Wuhou District, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Objective: The objective of the study was to describe the quality of life (QoL) status and investigate the influencing factors of QoL among patients with deep vein thrombosis (DVT).
Methods: A retrospective analysis at a single center was performed, and the clinical data of 161 patients with DVT admitted to West China Hospital of Sichuan University from June 2019 to June 2020 were collected with the Villalta scale, Hospital Anxiety and Depression Scale (HADS), and Chronic Venous Insufficiency Questionnaire (CIVIQ). The relationship between QoL and influencing factors, including characteristics, course of DVT, postthrombotic syndrome (PTS), psychological status, and behaviors, was analyzed by Student’s t-test, analysis of variance and multiple linear regression.
Results: A total of 161 patients who completed all the questionnaires between 2019 and 2020 were included, and 110 patients (68%) were male. The mean QoL score acquired by the CIVIQ scale was 74.18± 8.44, and the results showed significant differences between patients of different ages, genders, behaviors and psychological statuses (P < 0.05). Multiple regression analysis showed that age (P = 0.024), negative mood (P < 0.001), CCI index (P < 0.001), PTS (P < 0.001) and regular exercise (P = 0.002) influenced the CIVIQ scale evaluation model, in which exercise regularly was a protective factor for QoL, and age, negative mood, CCI index and PTS were risk factors for QoL.
Conclusion: The QoL of DVT patients was impaired and associated with age, mood, CCI index and PTS. Regular exercise is beneficial for improving the quality of life of DVT patients.
Keywords: deep vein thrombosis, quality of life, influencing factors
Introduction
DVT is the abnormal condensation of blood in a deep vein, typically in the lower leg,1 which is known as VTE2 combined with pulmonary embolism (PE). VTE is the main cause3 of the global disease burden and is characterized by high morbidity and a high mortality rate. It can also cause bleeding, recurrent venous thrombosis, PTS, persistent breathing difficulties, pulmonary hypertension and other complications.4,5 PTS develops in 40–60% of patients following a proximal DVT of the lower limb and results in chronic manifestations including pain, heaviness, swelling, itching, and ulcers.6 While increasing the burden of medical expenses, the outcomes also have a substantial impact on the psychological and physical health, well-being, and daily functioning of patients, and threatens the life of patients following VTE.
Traditional measures of morbidity and mortality are limited in describe and quantify the impact of illness, particularly chronic illness, and various generic and disease-specific instruments have been constructed to assess the overall and multidimensional outcomes.7 The increasing awareness of those chronic sequelae, together with an increased using of patient reported outcome measures to assess the impact of illness, has highlighted the utility of studying QoL in patients with DVT.8
According to the WHO, QoL is regarded as “… an individual’s perception of his/her position in life in the context of the culture and value systems in which he/she lives, and in relation to his/her goals, expectations, standards and concerns”.9 It is a broad-ranging concept, consists of individuals’ physical health, social relationships, environmental, level of independence, psychological, and spiritual components, and used for the evaluation of patients’ own health status and disease burden to reflect the clinical efficacy, disease prognosis and health economy. QoL is useful in medical decision making for ensuring improvement of the life domains who deems most important,10 can fully and effectively reflect the patient’s health status,11 and also an outcome measure for chronic venous disease to allow for consistent reporting and comparison between studies.
The tools currently used to assess QoL among VTE patients include generic and disease-specific instruments. Studies before involving QoL assessment of DVT patients mostly adopt generic instruments such as the Medical Outcome Survey Short-Form 36 items (SF-36) and the Medical Outcome Survey Short-Form 12 items (SF-12),12 which can be used irrespective of illness but may lack the sensitivity to capture disease specific aspects and to detect clinically-relevant changes over time. Therefore, disease-specific QoL measures is recommended in clinical trials.13,14
Studies have shown that scores of QoL in patients following DVT was significant lower comparing to population norms or matched controls with no history of DVT,15–17 and QoL in patients with DVT for four months was impaired and comparable to patients suffering from chronic diseases of the heart, lung, or joints.18 What’s worse, compared to other patients with chronic vascular diseases (CVD), DVT patients seem to have poorer QoL.19,20 However, a meta-analysis of patients with a history of DVT showed that QoL scores were comparable to population norms one year after an episode of DVT,21 and a longitudinal study showed that QoL in patients following DVT improved over time.22 Many studies have shown that PTS damages the QoL of patients following acute DVT.16,17,22,23 Factors have been found to be associated with impaired QoL such as the course of disease, age, obesity, comorbidity, location and extent of the thrombus, and socioeconomic status, have been assessed to a limited extent and their association with impaired QoL has been inconsistent across studies.17,22,24,25
Due to cultural differences between homelands and abroad and because the assessment results of quality of life with the same tool may be different in different regions,26 foreign research results cannot reflect the status in China.Therefore, the aim of this review is to present the status of QoL and associated factors among DVT patients in China. The results may contribute to design of a better management system for those patients and improve their QoL.
Methods
Participants
This cross-sectional study recruited DVT patients treated at West China Hospital, Sichuan University from June 2019 to June 2020. The inclusion criteria met the DVT diagnostic standards of standards for the diagnosis and efficacy of clinical diseases, and patients could be communicated with. The exclusion criteria were patients with mental disorders, cognitive disorders or incomplete medical records in the hospital information system.
Sample Size
Based on the rule of thumb suggested by Harrell,27 at least 10 subjects per variable in the linear regression model. With the Consideration of a 10% rate of invalid questionnaires, the sample size was estimated as 150.
Data Collection
The data were collected after patient discharge from the hospital for 3 to 6 months. We collected age, gender, marital status, culture, occupation, family income, course of disease, and comorbidity through the hospital information system and investigated smoking history, exercise habits, Villalta scale, psychological status and quality of life through telephone interviews. Before telephone interviews, unified training should be conducted to standardize the language of the investigator, and then the investigator should explain the items of the Villalta scale and other questionnaires. The investigator should check whether the patient has corresponding symptoms and guide the patients to choose the options that accord with their own situation.
The definition of the criterion was as follows: smoking history refers to the existence of continuous smoking of cigarettes for 6 months or more.28 Regular physical exercise was defined as 30 min of moderate exercise 3 times/wk.29
Instruments
Charlson Comorbidity Index (CCI)
The score standard refers to the CCI score of Roffman in 201630, which involves 17 diseases.
Villalta Scale
The Villalta scale was developed for the diagnosis, grading, prediction, and follow-up of postthrombotic syndrome (PTS),31 which consists of five patient-rated venous symptoms (pain, cramps, heaviness, paresthesia, pruritus) and six clinician-rated physical signs (pretibial edema, skin induration, hyperpigmentation, pain during calf compression, venous ectasia, redness). The signs on the Villalta scale are scored from 0 (=absent) to 3 (=severe) and are summed for the total score (range 0–33). A total score <5 indicates no PTS, 5–9 points indicates mild PTS, 10–14 points indicates moderate PTS, and ≥15 points is classified as severe PTS.
Hospital Anxiety and Depression Scale, HADS
The HADS is a 14-question instrument that measures anxiety and depression.32 Each item is scored between 0 (no impairment) and 3 (severe impairment), with a maximum score of 21. A total score of anxiety/depression subscale ≥ 8 means that the patient has anxiety and depression, and total score of HADS ≥ 9 means that the patient is combined with bad emotions.
The Chronic Venous Insufficiency Questionnaire, CIVIQ
The CIVIQ33 contains 20 items, including four dimensions: level of pain (pain in ankle or legs, limitation in work or daily activities because of leg problem, sleep bad because of leg problem, the limitation because of leg problem in work or daily activities while standing for a long time), physical (the limitation because of leg problem in work or daily activities while climbing stairs, kneeing, walking briskly, and doing housework), social impairment (the limitation because of leg problem in work or daily activities while travel by car, bus or plane, going to discos, weddings, parties, cocktails, and doing exercises) and psychological (feeling nervous, tired, irritable, being a burden to others, embarrassed to show legs, difficult to get going in the morning, hard for long standing or stretching, limp, unwilling to go out). Each item is scored between 1 (most serious) and 5 (lightest), with a maximum score of 100. Higher scores represent higher QoL due to DVT, and a total score ≥ 80 is divided into groups with satisfactory QoL.
Ethical Issues
All patients provided written informed consent, and the study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This study was approved by the research ethics committee of the hospital [2018-WCE10326].
Data Analysis
SPSS ver. 24.0 (SPSS Inc., Chicago, IL, USA) was used, continuous variables were presented using the mean and standard deviation (SD) or median and interquartile range (IQR), while frequencies and percentages were summarized for categorical variables. Differences between groups were analyzed using Student’s t-test or analysis of variance. Multiple linear regression was used to identify the predictive factors for the quality of life of patients with DVT, and a two-tailed P value of < 0.05 was considered statistically significant for all analyses.
Results
Characteristics, Behaviors and Emotions of Participants
Of the 161 initially enrolled patients, 161 VTE patients, including 110 males and 51 females, completed the telephone evaluation, with a mean age of 58.70 ± 8.61 years.
The average CIVIQ score was 74.12 ± 8.43 among the patients (Table 1). Comparing the CIVIQ scores in patients with different degrees of education, marriage, complications, relapse, compliance, and smoking, there were no significant differences (p > 0.05). Female patients had a higher CIVIQ score than male patients (p= 0.002). Patients with severe PTS, alcohol intake, anxiety, depression, negative mood and without regular exercise had a lower CIVIQ score (p< 0.05, Figure 1).
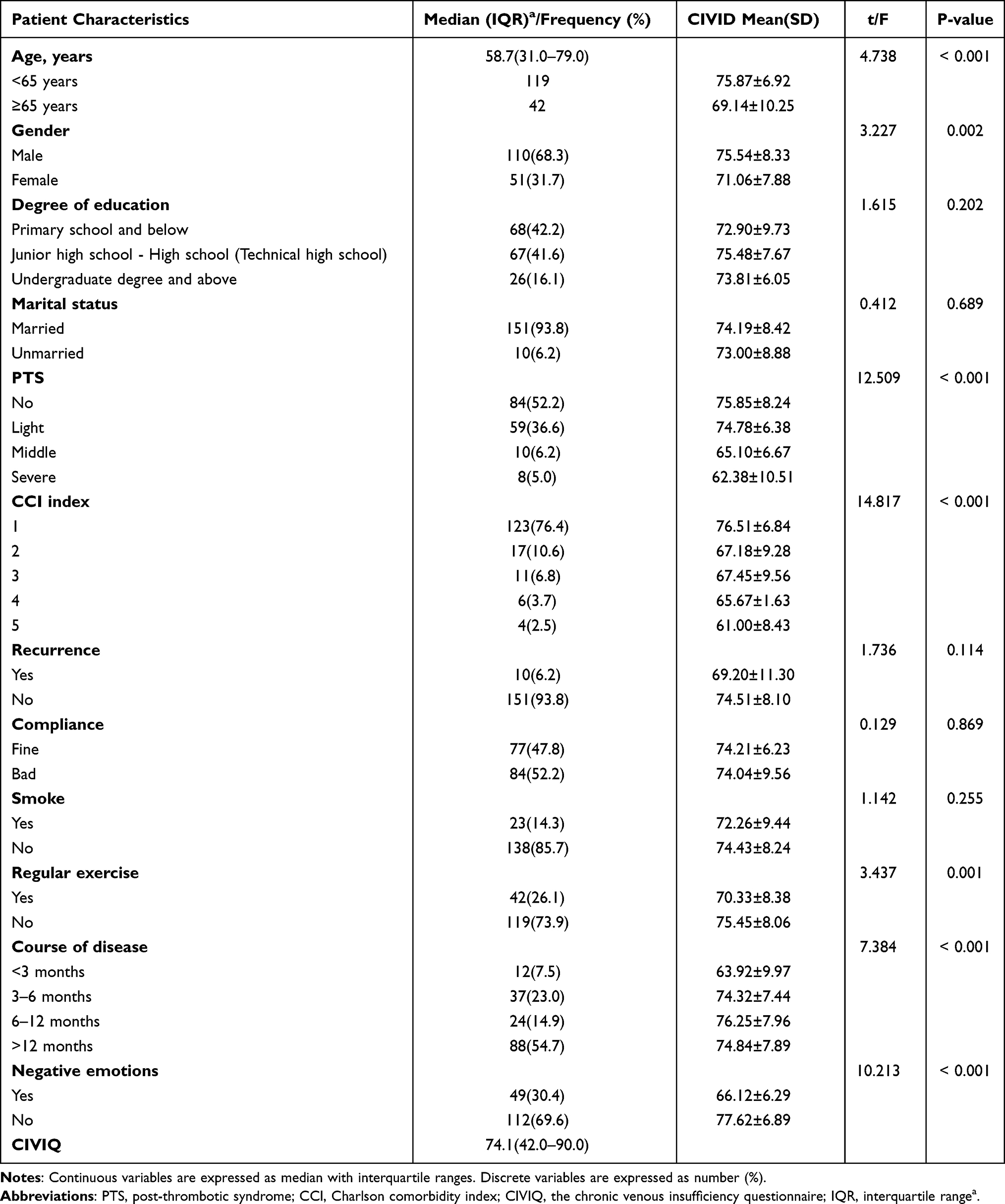 |
Table 1 Characteristics of Study Subjects (n = 161) |
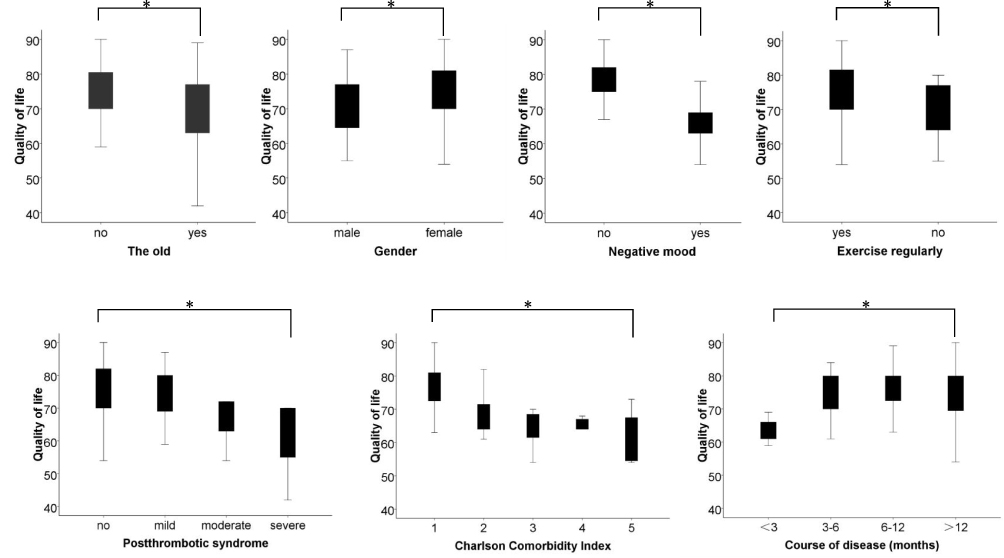 |
Figure 1 Characteristics, behaviors and emotions of participants. Note: *Statistical significance (P<0.01) when comparing quality of life among patients with different characteristics, behaviors and emotion status. |
Influencing Factors of QoL in DVT Patients in Multivariable Analysis
Age, sex, PTS score, smoking history, irregular exercise, CCI index, course of disease and adverse mood conditions were used as independent variables, and the CIVIQ score was used as the dependent variable. The multivariate model indicated that age, negative mood, PTS degree, CCI index and regular exercise had significant associations with the QoL of DVT patients. Age had a negative effect on the CIVIQ score (β = 0.119, P = 0.024). Patients with negative mood (β =−7.776, P < 0.001), higher PTS degree (β =−3.316, P < 0.001), higher score of CCI index (β =−2.199, P < 0.001), longer course of DVT (β = 1.046, P = 0.016) and without regular exercise (β =−3.340, P = 0.002) were more likely to have worse quality of life (Table 2).
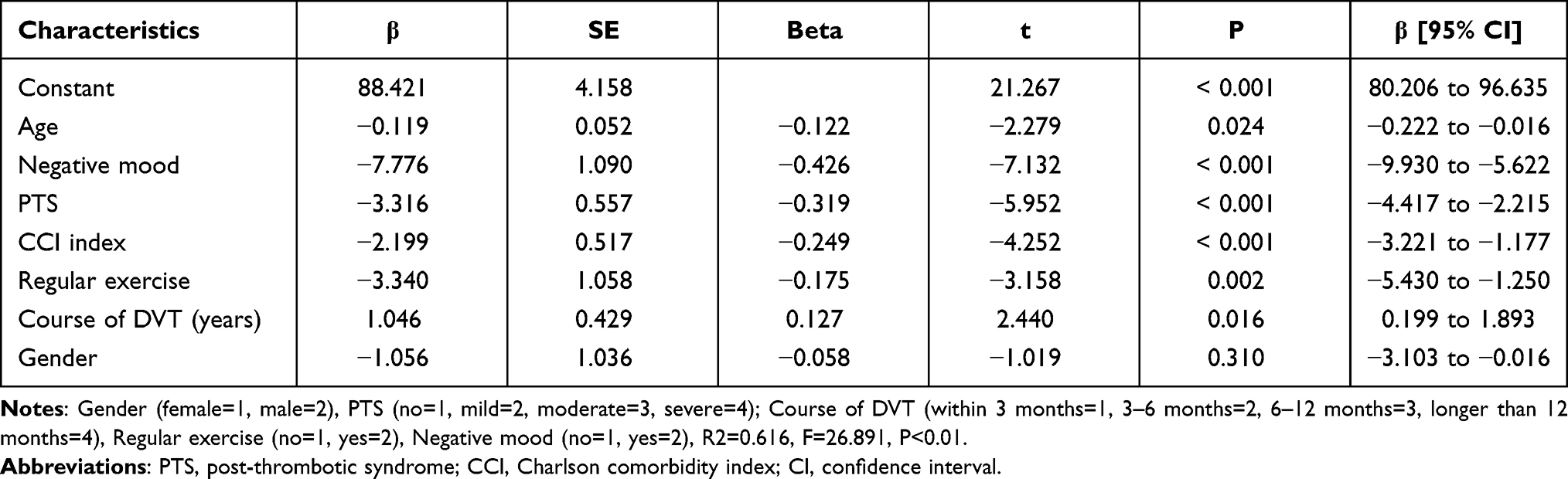 |
Table 2 Multiple Linear Regression for Influencing Factors of Quality of Life |
Discussion
In line with other studies,34,35 our results demonstrate significant impairment in QoL, and the mean CIVIQ score of 161 patients following DVT was 74.12 ± 8.43. A survey34 including 100 DVT patients showed that the mean CIVIQ score of patients was 71.52 to 78.65. The mean CIVIQ score was 71.8–77.0 among 278 patients with acute DVT.35 Female patients had a higher CIVIQ score than male patients, but sex was not a factor affecting quality of life. Giustozzi36 and Utne17 found a connection between QoL and sex in DVT patients with the EQ-5D and the Venous Insufficiency Epidemiological and Economic Studies - the quality of life/symptom (the VEINES-QoL/sym) questionnaire, respectively. We ascribe this disparity to the gender difference of the study populations.
Our results showed no connection between recurrence, marital status, educational level and QoL. Previous study37 also indicated that recurrence is not related to the QoL of DVT patients, but some study26 showed that recurrence is a predictor of QoL among VTE patients, which may be related to the different baseline data of these studies. Only 9 recurrent patients in this study were not able to indicate the relationship between recurrence and QoL. Wik25 investigated 131 female patients with DVT using the VEINES-QoL/sym and found that education level and marital status were independent predictors of decreased QoL. This may be associated with the inclusion of few women in this study, and further studies with larger sample sizes are recommended to analyze the correlation between sex, recurrence, marital status and education level and QoL.
Age is a factor that affects quality of life, which is consistent with previous studies. Monreal37 also confirmed that age was associated with the QoL of DVT patients. In addition to the effects of aging of body functions, older people are more likely to suffer from comorbidities. The second factor affecting the QoL of DVT patients is depression, anxiety or negative mood. This is consistent with previous studies.38 For patients, DVT is not only a life-threatening disease that may lead to pulmonary embolism (PE) but also may affect future work and life and increase the psychological burden of patients. Therefore, dynamic assessment of psychological status, early identification and intervention are needed, and comprehensive guidance and full health education are recommended to improve the psychological status of patients.39
Our data suggest that patients with severe PTS at have worse QoL scores, which is consistent with previous studies. There was a significant reduction in QoL with increased severity of PTS.26 Utne17 found that DVT patients with PTS have significantly lower QoL than those with no PTS and that PTS was a predictor of decreased quality of life with acute DVT. More often pain-, skin-, and psychiatric problems, and were more often on sick-leave were reported in cases who developed PTS, resulting in reduced physical tolerance for a day’s work. PTS negatively affects patients’ QoL and causes a significant burden on the healthcare system. These findings highlight the importance of early intervention and prevention of disease progression. In the other hand, DVT patient management should be graded in clinical practice, especially in the continuous management of patients. We should focus on patients with PTS and provide individualized health guidance to improve QoL.
Regular exercise was a predictor of QoL in DVT patients in our study, and the QoL was better among DVT patients with regular exercise. Regular exercise can improve patients’ sports endurance and optimize brain-derived neurotrophic factor (BDNF), which has been implicated in individual emotions.40 Participating in physical activities regularly can release stress, improve sleep conditions and eliminate negative moods, thus improving QoL.41 Physical activity and exercise are inversely associated with depression levels, and increasing physical activity can improve QoL, so physical activity should be promoted more actively within clinical practice. We recommend aerobic exercise, such as walking and jogging, and encourage patients to exercise leg muscle strength, especially calf muscle strength.42
There are several limitations to this study. First, 68.3% of the patients were male and 6.2% of patients were unmarried, denoting a rather homogenous study population, which limited our ability to determine the potential effects of gender/spouse/recurrence characteristics in our analyses. In addition, patients were only sampled from Southwest China, which limits its external validity. Due to a lack of data in other areas, the sample may not be representative of general DVT patients in China. Despite this, our research has provided valuable new data on the relationships among the Villalta scale, emotion status, comorbidities, regular exercise and QOL measures, and the results may still be generalizable to patients from the areas mentioned above.
Conclusion
The QoL of DVT patients is impaired. Age, negative emotions, PTS, CCI index and regular exercise were related to physical status. Early management, including health education, self-management in the whole course, psychological assessment at follow-up and personalized intervention aiming to improve the cognitive level of patients, could be enhanced to improve the QoL of DVT patients.
Disclosure
All authors declare no competing interests in this work.
References
1. Olaf M, Cooney R. Deep venous thrombosis. Emerg Med Clin North Am. 2017;35(4):743–770. doi:10.1016/j.emc.2017.06.003
2. Cushman M. Epidemiology and risk factors for venous thrombosis. Semin Hematol. 2007;44(2):62–69. doi:10.1053/j.seminhematol.2007.02.004
3. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
4. Prandoni P, Kahn SR. Postthrombotic syndrome: prevalence, prognostication and need for progress. Br J Hematol. 2009;145(3):286–295. doi:10.1111/j.1365-2141.2009.07601.x
5. Klok FA, van der Hulle T, den Exter PL, Lankeit M, Huisman MV, Konstantinides S. The post PE syndrome: a new concept for chronic complications of pulmonary embolism. Blood Rev. 2014;28(6):221–226. doi:10.1016/j.blre.2014.07.003
6. Ashrani AA, Heit JA. Incidence and cost burden of post-thrombotic syndrome. J Thromb Thrombolysis. 2009;28(4):465–476. doi:10.1007/s11239-009-0309-3
7. Padberg F
8. Kahn SR, Julian JA, Kearon C, et al. Quality of life after pharmacomechanical catheter-directed thrombolysis for proximal deep venous thrombosis. J Vasc Surg Venous Lymphat Disord. 2020;8(1):8–23. doi:10.1016/j.jvsv.2019.03.023
9. World Health Organization: WHOQOL. Measuring quality of life. Available from: http://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/.
10. Berghout M, van Exel J, Leensvaart L, Cramm JM. Healthcare professionals’ views on patient-centered care in hospitals. BMC Health Serv Res. 2015;15:385. doi:10.1186/s12913-015-1049-z
11. Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med. 1993;118(8):622–629. doi:10.7326/0003-4819-118-8-199304150-00009
12. Chen YF, Liu BY, Shi XJ, Zhang HQ, Xu YY, Liang LJ. Effects of wechat combined with home visit continuous care on compliance and quality of life after thrombolytic therapy in lower extremity deep vein thrombosis. J Clin Nurs Pract. 2020;5(27):32, 49.
13. Fisher L, Tang T, Polonsky W. Assessing quality of life in diabetes I. A practical guide to selecting the best instruments and using them wisely. Diabetes Res Clin Pract. 2017;126:278–285. doi:10.1016/j.diabres.2016.10.018
14. Fayers P, Machin D. Quality of Life: The Assessment, Analysis and Reporting of Patient-Reported Outcomes.
15. Delis KT, Bountouroglou D, Mansfield AO. Venous claudication in iliofemoral thrombosis: long-term effects on venous hemodynamics, clinical status, and quality of life. Ann Surg. 2004;239(1):118–126. doi:10.1097/01.sla.0000103067.10695.74
16. van Korlaar IM, Vossen CY, Rosendaal FR, et al. The impact of venous thrombosis on quality of life. Thromb Res. 2004;114(1):11–18. doi:10.1016/j.thromres.2004.04.007
17. Utne KK, Tavoly M, Wik HS, et al. Health-related quality of life after deep vein thrombosis. Springerplus. 2016;5(1):1278. doi:10.1186/s40064-016-2949-z
18. Kahn SR, Ducruet T, Lamping DL, et al. Prospective evaluation of health-related quality of life in patients with deep venous thrombosis. Arch Intern Med. 2005;165(10):1173–1178. doi:10.1001/archinte.165.10.1173
19. Kahn SR, M’Lan CE, Lamping DL, et al. The influence of venous thromboembolism on quality of life and severity of chronic venous disease. J Thromb Haemost. 2004;2(12):2146–2151. doi:10.1111/j.1538-7836.2004.00957.x
20. Lozano Sanchez FS, Gonzalez-Porras JR, Diaz Sanchez S, et al. Investigators: negative impact of deep venous thrombosis on chronic venous disease. Thromb Res. 2013;131(4):e123–126. doi:10.1016/j.thromres.2013.01.011
21. Lubberts B, Paulino Pereira NR, Kabrhel C, Kuter DJ, DiGiovanni CW. What is the effect of venous thromboembolism and related complications on patient reported health-related quality of life? A meta-analysis. Thromb Haemost. 2016;116(3):417–431. doi:10.1160/TH16-02-0152
22. Kahn SR, Shbaklo H, Lamping DL, et al. Determinants of health-related quality of life during the 2 years following deep vein thrombosis. J Thromb Haemost. 2008;6(7):1105–1112. doi:10.1111/j.1538-7836.2008.03002.x
23. Haig Y, Enden T, Slagsvold CE, et al. Determinants of early and long-term efficacy of catheter-directed thrombolysis in proximal deep vein thrombosis. J Vasc Interv Radiol. 2013;24(1):17–26. doi:10.1111/j.1538-7836.2008.03002.x
24. Marvig CL, Verhoef TI, de Boer A, et al. Quality of life in patients with venous thromboembolism and atrial fibrillation treated with coumarin anticoagulants. Thromb Res. 2015;136(1):69–75. doi:10.1016/j.thromres.2015.04.026
25. Wik HS, Enden TR, Jacobsen AF, Sandset PM. Long-term quality of life after pregnancy-related deep vein thrombosis and the influence of socioeconomic factors and comorbidity. J Thromb Haemost. 2011;9(10):1931–1936. doi:10.1111/j.1538-7836.2011.04468.x
26. Lloyd AJ, Dewilde S, Noble S, Reimer E, Lee AYY. What impact does venous thromboembolism and bleeding have on cancer patients’ quality of Life? Value Health. 2018;21(4):449–455. doi:10.1016/j.jval.2017.09.015
27. Harrell FE
28. Zhao JW, Zhao G, Hua CF, et al. Self-reported smoking behaviors and toxicant exposure assessment in adult Chinese smokers. Tob Sci Tech. 2020;54(4):57–65.
29. Park S, Kim K, Lee BK, Ahn J. A healthy diet rich in calcium and vitamin c is inversely associated with metabolic syndrome risk in Korean adults from the KNHANES 2013–2017. Nutrients. 2021;13(4):1312. doi:10.3390/nu13041312
30. Roffman CE, Buchanan J, Allison GT. Charlson comorbidities index. J Physiother. 2016;62(3):171. doi:10.1016/j.jphys.2016.05.008
31. Kahn SR, Partsch H, Vedantham S, et al. Definition of postthrombotic syndrome of the leg for use in clinical investigations: a recommendation for standardization. J Thromb Haemost. 2009;7(5):879–883. doi:10.1111/j.1538-7836.2009.03294.x
32. Zheng LL, Wang YL, Li HC. Application of hospital anxiety and depression scale in general hospital: an analysis in reliability and validity. Shanghai Arch Psychiatry. 2003;15(5):264–266. doi:10.3969/j.issn.1002-0829.2003.05.003
33. Zhang FX, Zhang H. The efficacy evaluation way and clinical application for chronic venous insufficiency of the lower limbs. Chin J Pract Surg. 2015;35(12):1267–1271. doi:10.7504/CJPS.ISSN1005-2208.2015.12.03
34. Wang J, Zhang J, Sun JH. Effect of combined therapy on quality of life, venous valve function and recurrence rate in patients with acute deep venous thrombosis of lower limbs. Mod Pract Med. 2018;30(3):384–385. doi:10.3969/j.issn.1671-0800.2018.03.052
35. Li Q, Lin SM, Li YY, et al. Mid-and long-term outcome of catheter-directed thrombolysis combined with endovascular therapy in acute deep venous thrombosis. Chin J Vascular Surg. 2017;9(2):102–105.
36. Giustozzi M, Valerio L, Agnelli G, et al. Sex-specific differences in the presentation, clinical course, and quality of life of patients with acute venous thromboembolism according to baseline risk factors. Insights PREFER VTE Eur J Intern Med. 2021;88:43–51. doi:10.1016/j.ejim.2021.03.014
37. Monreal M, Agnelli G, Chuang LH, et al. Deep vein thrombosis in Europe-health-related quality of life and mortality. Clin Appl Thromb Hemost. 2019;25:1–12. doi:10.1177/1076029619883946
38. Souza Nogueira G, Rodrigues Zanin C, Miyazaki MC, Pereira DG. Venous leg ulcers and emotional consequences. Int J Low Extrem Wounds. 2009;8(4):194–196. doi:10.1177/1534734609350548
39. Liu CP, Chen HW, Wu SH, et al. A survey of anxiety and depression in patients taking warfarin due to venous thromboembolism. Chin J Ger Heart Brain Vessel Dis. 2011;13(11):1008–1010. doi:10.3969/j.issn.1009-0126.2011.11.015
40. Zuhany K, Otto M. Assessing BDNF as a mediator of the effects of exercise on depression. J Psychiatr Res. 2020;123:114–118. doi:10.1016/j.jpsychires.2020.02.003
41. Gerber M, Jonsdottir IH, Lindwall M, Ahlborg G. Physical activity in employees with differing occupational stress and mental health profiles: a latent profile analysis. Psychol Sport Exerc. 2014;15(6):649–658. doi:10.1016/j.psychsport.2014.07.012
42. Zhang Q, Yu Y, Yang T. Clinical effect of cognitive behavioral Intervention on the cognitive level and quality of life in patients with venous thromboembolism. Chin J Pract Nurs. 2017;33(26):2001–2006. doi:10.3760/cma.j.issn.1672-7088.2017.26.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.