")
Back to Journals » Cancer Management and Research » Volume 14
Quality of Life of Prostate Cancer Patients Undergoing Prostatectomy and Affective Temperament
Authors Popiołek A , Brzoszczyk B , Jarzemski P , Piskunowicz M , Jarzemski M, Borkowska A , Bieliński M
Received 12 January 2022
Accepted for publication 23 March 2022
Published 20 May 2022 Volume 2022:14 Pages 1743—1755
DOI https://doi.org/10.2147/CMAR.S358054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
Alicja Popiołek,1,2 Bartosz Brzoszczyk,3 Piotr Jarzemski,3 Małgorzata Piskunowicz,1 Marcin Jarzemski,3 Alina Borkowska,1 Maciej Bieliński1
1Department of Clinical Neuropsychology, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Bydgoszcz, Poland; 2Department of Internal Diseases, Jan Biziel University Hospital No.2 in Bydgoszcz, Bydgoszcz, Poland; 3Clinic of Urology, Jan Biziel University Hospital No. 2 in Bydgoszcz, Bydgoszcz, Poland
Correspondence: Alicja Popiołek, Department of Clinical Neuropsychology, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Ul. Skłodowskiej-Curie 9, Bydgoszcz, 85-094, Poland, Tel/fax +48 52 585 37 03, Email [email protected]
Purpose: Prostate cancer (PC) is one of the most common malignancies in men. The population of PC survivors is growing, and understanding the roles of different factors that affect quality of life (QoL) is important. We investigated the effects of affective temperament on the QoL of PC patients.
Patients and Methods: All subjects (n=100) underwent medical evaluation [including demographic data, medical history, physical examination, biochemical tests, and assessment of urinary incontinence (ICIQ-UI SF scale) and erectile dysfunction (ED) (IIEF-5 and subjective ED scale)] and psychological evaluation [including assessment of affective temperament using the TEMPS-A scale, depression and anxiety (using HADS), and QoL (EORTC-QLQ-C30 and EORTC-PR25)]. The relationships between individual variables were examined.
Results: Erection quality after treatment was associated with better QoL in most parameters. Similar strong relationships were observed between the urinary incontinence scale and QoL. Depressive, cyclothymic, irritable, and anxious temperaments were associated with decreased QoL. On the EORTC-PR25 scale, associations were observed between a depressive temperament and worse sexual function and urinary symptoms, between a cyclothymic temperament and worse urinary symptoms, and between an irritable temperament and worse sexual functioning. Multivariate analysis identified the severity of anxiety and depression symptoms measured by HADS as the most important psychological factors affecting QoL.
Conclusion: QoL in PC survivors depends on many factors, including age, interval since diagnosis, tumor stage, treatment, complications, and affective temperament profile. Depressive, cyclothymic, irritable, and anxious temperaments were associated with poorer QoL in selected domains, which was not observed for a hyperthymic temperament. The temperament profile of patients was associated with mood and anxiety level, which were important determinants of a poorer QoL.
Keywords: quality of life, prostate cancer, complications, prostatectomy, affective temperament
Introduction
Prostate cancer (PC) is one of the most common malignancies in men.1 Advances in screening, early detection, and effective therapies have resulted in an increase in the population of patients with PC. This population includes a) people with a slow and indolent course of disease who are undergoing watchful waiting, and b) people who have been successfully treated (PC survivors).2,3 Both groups require specific care tailored to the problems they face. PC survivors struggle with long-term complications such as urinary dysfunction (narrowing of the urethra, urinary incontinence, urinating problems, hematuria), sexual difficulties, and erectile dysfunction (ED).4–8 A diagnosis of PC and its subsequent treatment are sources of stress and anxiety, which affect not only the patients’ health, but also their daily functioning and social life. In addition, mood and cognitive disorders may develop.9,10 Both physical and psychological symptoms can negatively affect the quality of life (QoL) of PC survivors.11–13 The QoL of cancer survivors depends on the progression of the disease, the course of treatment, and the occurrence of complications after treatment; however, the psychological predisposition of the patient is another important factor affecting QoL.14–16
Temperament refers to core personality traits linked to behavioral and emotional reactivity to environmental stimuli. It is thought to be biologically determined and to remain relatively stable throughout life. Akiskal, drawing inspiration from Kretschmer and Kraepelin, proposed the existence of five types of affective temperament (cyclothymic, dysthymic, irritable, hyperthymic, and anxious) and referred to them as subclinical manifestations of mood disorders. Although over time they became viewed as normal personality domains and studied in non-clinical populations, their extremes are presumed to carry the risk of psychopathology.17,18 Temperament modulates stress reactivity and the coping strategies people use in the face of stressful life events. Temperamental traits can be adaptive or maladaptive according to the circumstances. There is a paucity of literature on affective temperament types in cancer patients, and it remains undetermined whether and to what extent affective temperament is linked to QoL in cancer survivors. Relationships between temperamental traits and the course of the disease and QoL were previously described for various disease entities including metabolic syndrome,19 psoriasis,20 Parkinson’s disease,21 post-traumatic stress disorder,22 and breast cancer.23 However, these studies were based on different definitions and scales of QoL and temperament. Few reports include the assessment of affective temperament using the Temperament Evaluation of Memphis, Pisa, and San Diego Autoquestionnaire (TEMPS-A) in correlation with QoL.24–26 To the best of our knowledge, this is the first study investigating the effects of affective temperament on the QoL of patients with PC.
In this study, the concept of affective temperament provides a framework to investigate the adaptation of PC survivors. We hypothesize that temperament type may be associated with mood, anxiety, postoperative complications, and subjective health-related QoL in men who underwent treatment for PC.
Materials and Methods
Participants
The study included 100 Caucasian men of Polish nationality who underwent radical prostatectomy for PC. The patients were recruited from the University Hospital/University-Affiliated Urology Clinic. Table 1 lists the demographic and clinical characteristics of the studied population. All participants provided written informed consent to participate in the study. The inclusion criteria were as follows: histopathologically confirmed diagnosis of prostate adenocarcinoma and subsequent treatment with radical prostatectomy, the ability to understand the purpose of the study and perform tests, and no incapacitation. The exclusion criteria were dementia and/or diagnosed serious somatic, psychiatric, or neurological diseases. In the study group, there were no patients with complications on the level of Clavien 3 and higher. There were 23 patients with additional oncological treatment: (21 pts radiotherapy (RTx); 9 pts androgen deprivation therapy (ADT); 7 pts ADT + RTx).27 The study was approved by the Bioethics Committee of the Nicolaus Copernicus University, Collegium Medicum in Bydgoszcz (Approval No 476/2017) and complies with the Declaration of Helsinki.
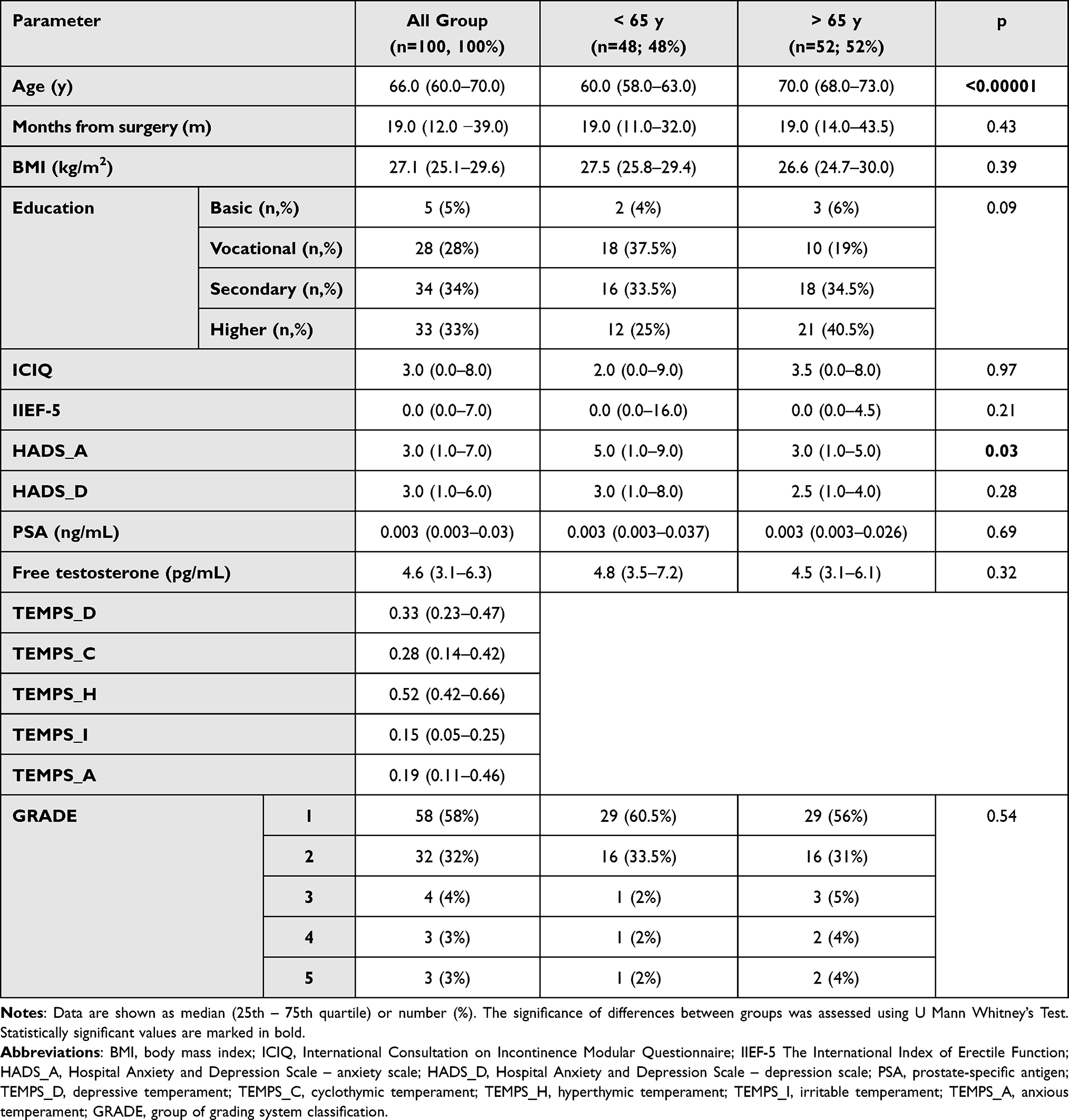 |
Table 1 Demographic and Clinical Data in Subgroups with Age >65y and < 65y |
Methods
All subjects underwent medical and psychological evaluations.
The medical evaluation included demographic data (age, education), medical history, physical examination, and biochemical tests (free testosterone level and prostate-specific antigen determined by immunoenzymatic methods).
Medical history included detailed information on disease symptoms, time of onset, disease progression, grade group according to the International Society of Urological Pathology classification,28 previous therapies, comorbidities, and the occurrence of postoperative complications, taking into account Clavien-Dindo Classification. The following instruments were used to measure various aspects of complications: urinary incontinence, scale ICIQ-UI SF; ED, IIEF-5 and subjective ED scale.
ICIQ-UI SF: The International Consultation on Incontinence Questionnaire-Urinary Incontinence (ICIQ-UI SF) is a short and simple tool to screen for incontinence and its impact on QoL.29 It consists of four questions, of which three address the prevalence, severity, and impact on QoL and the fourth addresses the patient’s perception of the cause and type of leakage. A higher score indicates a greater severity of symptoms.
IIEF-5: The International Index of Erectile Function - 5 (IIEF-5) consists of five questions assessing the prevalence and severity of ED and sexual intercourse satisfaction.30 Fewer points indicate worse erectile function, and zero means no erection.
In the subjective assessment of the quality of erection, the patient’s task was to assess, on a scale of 1 to 5, the quality of erection after surgery. A higher score indicates a better subjective quality of the erection.
The psychological examination included the assessment of affective temperament (using a Polish adaptation of the TEMPS-A scale), symptoms of anxiety and depression (HADS), and QoL (EORTC-QLQ-C30 and EORTC-PR25).
TEMPS-A: The Affective Temperament Rating Scale (TEMPS-A) is used to assess the individual dimensions of the affective temperament as described by Akiskal (depressive, TEMPS_D; cyclothymic, TEMPS_C; hyperthymic, TEMPS_H; irritable, TEMPS_I; and anxious temperament scale, TEMPS_A).31 The questionnaire contains 110 items for women and 109 for men, all of which are yes or no questions. The scale is divided into five parts, each dedicated to a different affective temperament (dimension). The number of points scored on each scale reflects the level at which the specific temperament dimension is expressed in the patient.
HADS: The Hospital Anxiety and Depression Scale (HADS) is a questionnaire composed of 14 questions and divided into two sections: anxiety (HADS-A) and depression (HADS-D).32 In each section, the patient answers seven questions regarding his well-being in the last week by selecting the answer that best suits him. The number of points indicates the severity of the disorder, namely, a higher value indicates a higher severity of anxiety and/or depression.
The EORTC-QLQ-C30 questionnaire was created by the European Organization for Research and Treatment of Cancer (EORTC) to assess the QoL of patients diagnosed with cancer.33 It contains five functional scales (addressing physical functioning, social role, emotional functioning, cognitive functioning, and social functioning); three scales assessing disease symptoms (fatigue, nausea/vomiting, and pain); and six individual questions assessing loss of appetite, dyspnea, insomnia, constipation, diarrhea, and financial difficulties. It also includes a general health scale. A low score in a functional scale represents a high/healthy level of functioning, whereas a low score for a symptom scale or item represents a lower level of symptomatology or problems. In the global health status scale, a higher score indicates a better health status.
The EORTC-PR25 is a PC-specific module of the EORTC questionnaire for assessing the health-related QoL of PC patients.34 It has six domains: bowel and urinary symptoms, sexual activity, sexual functioning, and the side-effects of hormonal treatment and incontinence aid. A higher score in the sexual activity domain indicates a better health status, whereas lower scores in the other domains indicate better health status.
Statistical analyses were performed using the STATISTICA 13.1 statistical package.
Because of the distribution of variables that do not meet the criteria of normal distribution, non-parametric tests were used. The Spearman’s rank correlation test was used to assess the relationships between variables. Differences between groups were analyzed using the Mann-Whitney U-test. Multivariate analysis was performed using a regression model. A p value of <0.05 was accepted as the cut-off point for statistical significance.
Results
The analysis of differences in the QoL parameters in the general EORTC scale and the subscales dedicated to patients after prostatectomy (EORTC-PR25) was performed in the age subgroups <65 years and >65 years (Table 2). The subgroups differed significantly only in the reported pain (EORTC-QLQ) and sexual functioning (EORTC-PR25). In both areas, younger patients had worse results.
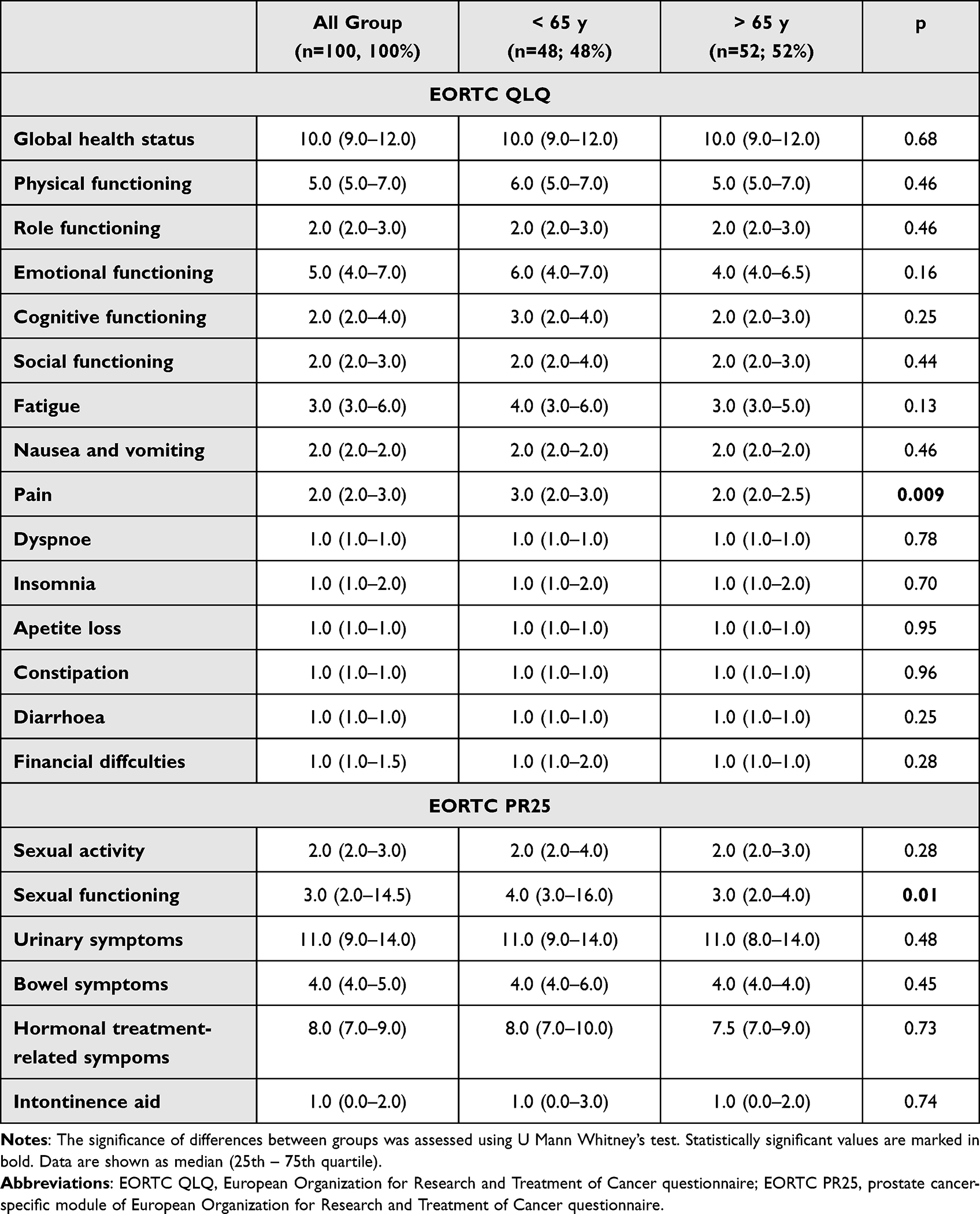 |
Table 2 Quality of Life Dimensions in Subgroups with Age >65y and < 65y |
Analysis of the relationship between EORTC-QLQ and EORTC-PR25 parameters and demographic and clinical factors (Table 3) revealed that the quality of erection after treatment was associated with better QoL in most parameters assessed. Similarly strong relationships were observed between the urinary incontinence scale and QoL.
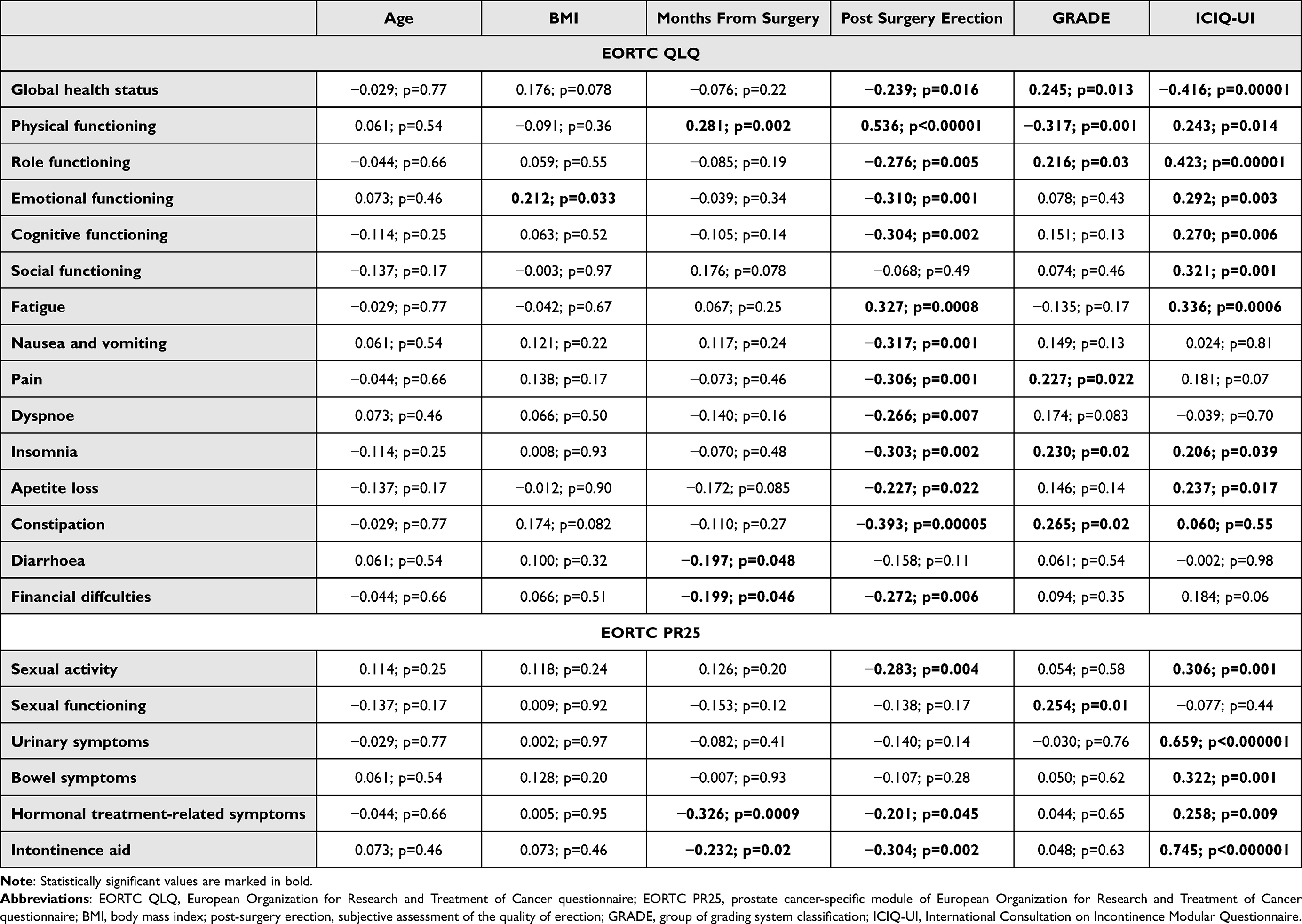 |
Table 3 R-Spearman Correlations of Clinical Factor and Parameters of EORTC QLQ and EORTC P25 |
Depressive, cyclothymic, irritable, and anxious temperaments were correlated with decreased QoL on the general EORTC scales (Table 4). A hyperthymic temperament was not significantly correlated with QoL in this analysis. On the EORTC-PR-25 scale, a depressive temperament was associated with worse sexual functioning and urinary symptoms, a cyclothymic temperament was associated with worse urinary symptoms, and an irritable temperament was associated with worse sexual functioning. On the other hand, a hyperthymic temperament was significantly correlated with better incontinence aid results.
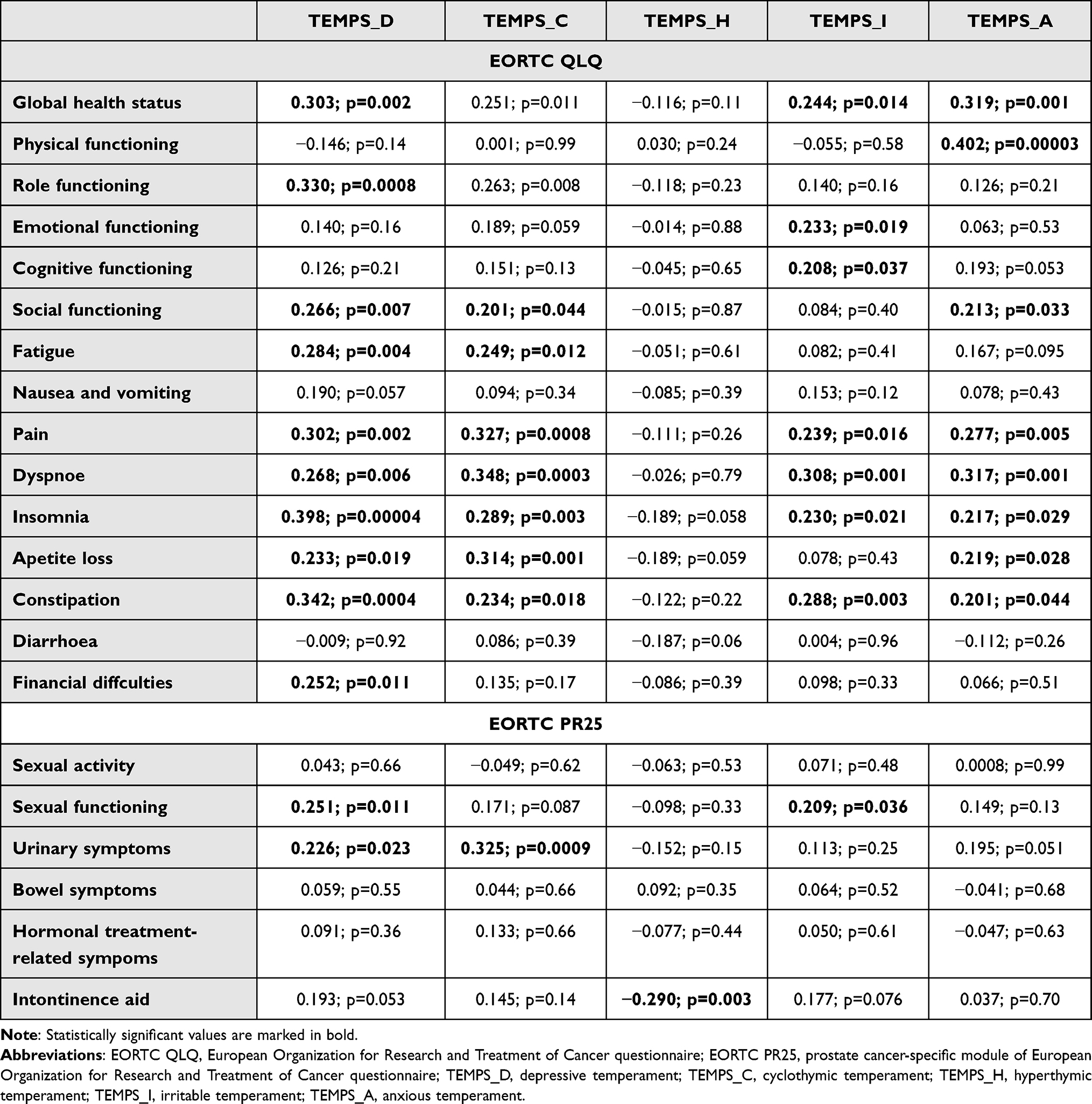 |
Table 4 R-Spearman Correlations of TEMPS Dimensions and Parameters of EORTC QLQ and EORTC P25 |
Another analysis examined the correlation of affective temperaments and selected clinical parameters with the HADS scales, IIEF-5 scale, erection quality, and ICIQ (Table 5). These analyses showed strong relationships between individual dimensions of affective temperament and anxiety and depression, and the occurrence of the most common postoperative complications such as urinary incontinence or ED. The conducted analyzes did not reveal a significant influence of adjuvant therapy on the study of the relationship between affective temperaments and quality of life in the study group.
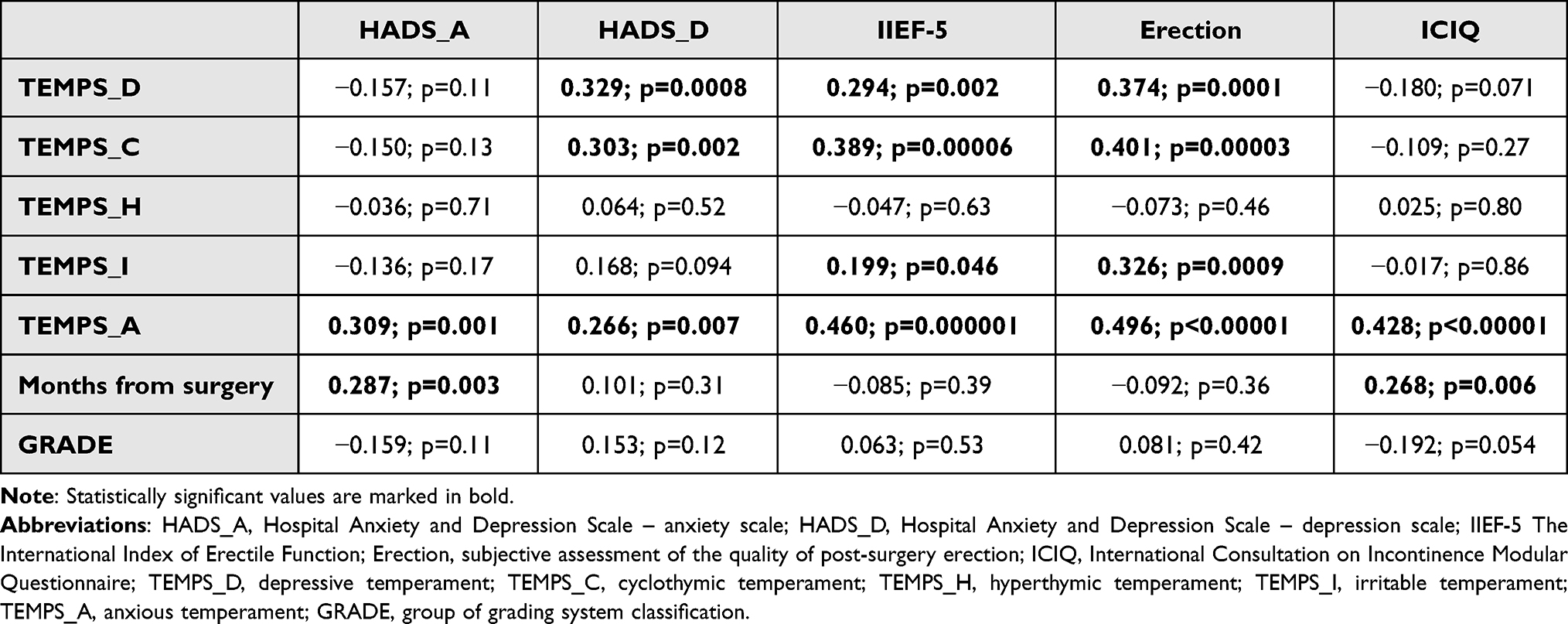 |
Table 5 R-Spearman Correlations of TEMPS Dimensions and Clinical Factors |
Multivariate analysis confirmed that depressive, cyclothymic, irritable, and anxious temperaments were associated with sexual activity. Nevertheless, the most important psychological elements in this analysis were the severity of anxiety and depression symptoms measured by HADS (Table 6).
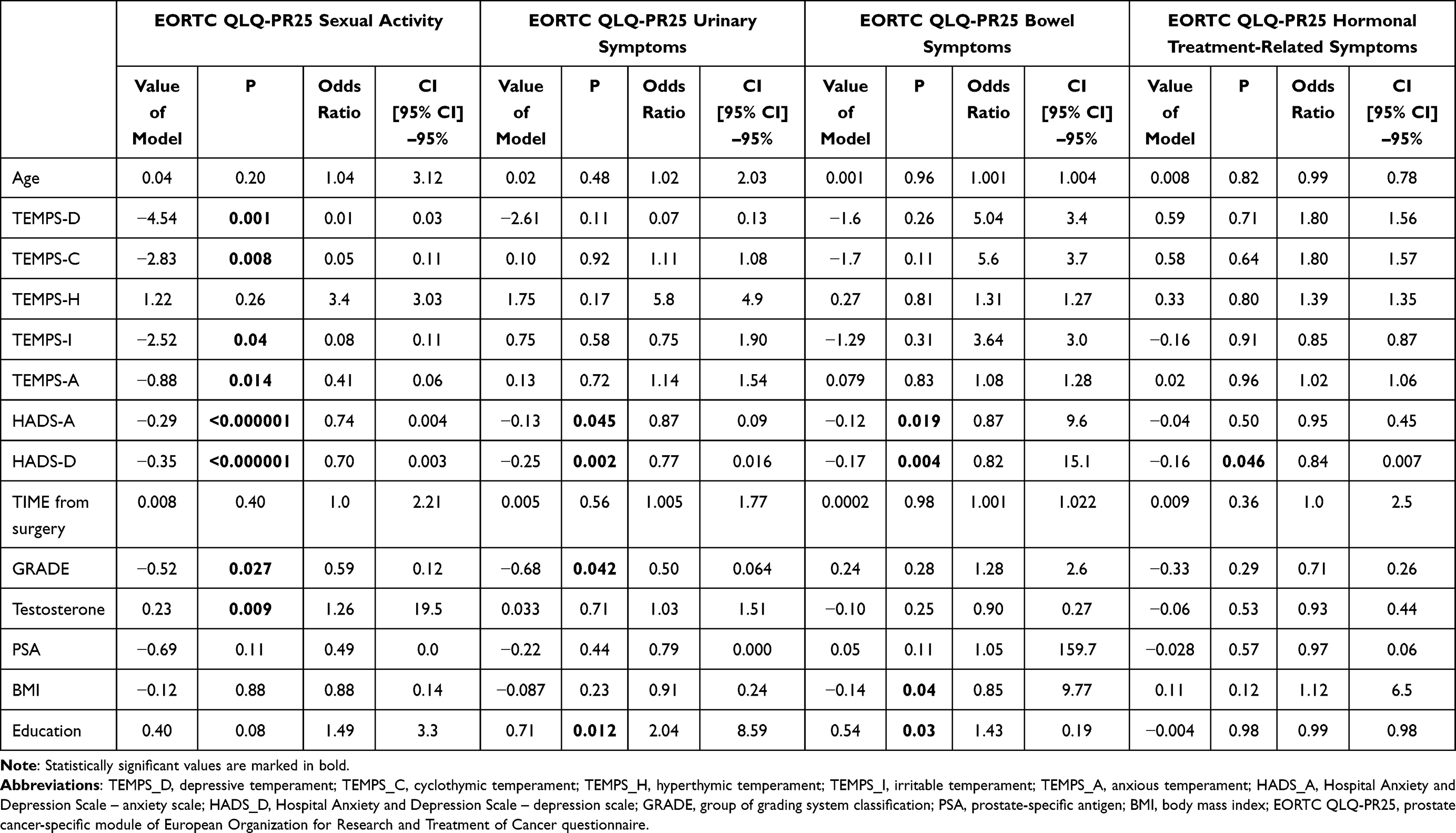 |
Table 6 Multivariate Analysis – Regression Model for Quality of Life Scores Dedicated to Patients After Prostatectomy |
Discussion
Assessment of Quality of Life
The QoL of PC patients depends on many factors.35,36 The use of hormone therapy, a low education level, and older age are associated with reduced QoL.37,38 In this study, age was not correlated with any of the dimensions of the QoL scale (Table 3); however, slight differences were observed between the groups of patients younger and older than 65 years. Younger participants had a higher level of anxiety and were more likely to report pain and sexual functioning problems (Tables 1 and 2). This is consistent with the results of previous studies.39 Sexual dysfunction is not as important for QoL in patients with advanced cancer as in patients with localized cancer. This population faces the possibility of imminent death, and sexual function may have a lower priority.35,36 A similar mechanism may be present in older people, which would explain the differences between groups, as sexual function is not as important in the elderly as in the younger population.
QoL also depends on the time interval since diagnosis and treatment and the stage of the cancer.35 In this study, longer time intervals were significantly associated with better overall physical functioning (Table 3). However, in the assessment of individual symptoms, it was negatively correlated only with the severity of diarrhea. Similarly, the discomfort associated with hormonal treatment and the need to use incontinence aids or experience of financial difficulties decreased over time. Previous studies reported that urination problems (such as urinary incontinence and urgency) disappear over time, whereas sexual problems (such as poor erection quality and low sexual desire) tend to persist.35,40 In this study, cancer progression affected certain QoL dimensions, such as global health status and physical functioning, as well as physical symptoms such as constipation, insomnia, and pain sensation. Consistently, Odeo and Degu in their review noted that cancer progression, as indicated by a higher clinical stage, higher Gleason score, and greater cancer severity, is a major predictor of poor health-related QoL among PC patients.38
In this study, the most prominent clinical factors associated with QoL were urinary incontinence and quality of erection after treatment (Table 3). These dysfunctions were strongly correlated with most QoL parameters, which is consistent with the results of previous studies.35,41,42 Sexual dysfunction and urinary incontinence are also the most frequently impaired health-related QoL domains in patients with localized PC.35 All types of treatments, as well as untreated disease itself, can lead to these dysfunctions.35 However, their severity and impact on QoL depend on the treatment method used.40,43,44 Removing the prostate gland is associated mostly with sexual and urinary dysfunction.35 Unlike surgery, radiotherapy is associated with bowel dysfunction and, to a lesser extent, with urinary incontinence. Adjuvant androgen-deprivation therapy increases the incidence of fatigue. Despite these differences in individual domains, prospective evaluation shows that global health-related QoL in men does not differ according to treatment modality.35,42
Assessment of the Relation Between Quality of Life and Temperament
Most of the aspects of QoL examined and included in the general EORTC-QLQ scale were significantly correlated with the individual dimensions of temperament (Table 4). Only nausea, vomiting, and diarrhea did not show such correlations. In the detailed scale of EORTC-PR25, none of the temperament types was correlated with bowel symptoms (Table 4). The specificity of the cohort may have influenced the results because gastrointestinal complications are not common in patients after radical prostatectomy.42 The results could also be attributed to the rarity of these symptoms among the present cohort.
The other dimensions of the QoL scale, namely, fatigue, pain, dyspnea, insomnia, appetite loss, constipation, and financial difficulties, as well as physical, role functioning, emotional functioning, cognitive, and social functioning and global health status, showed strong correlations with the affective temperament profile (Table 4). These correlations were mostly observed for depressive, cyclothymic, irritable, and anxious temperaments, whereas they were not present for the hyperthymic temperament subscale. The reason for this is not entirely clear. The association between temperament type and the QoL subscales was mostly negative for the hyperthymic temperament and mostly positive for the other temperament types, suggesting that the predisposition to a poorer QoL induced by most temperaments is reduced by the hyperthymic temperament. Kesebir et al observed a relation between the hyperthymic temperament and resilience in depression.45 In Italian cancer patients, traits associated with the hyperthymic temperament are correlated with better health-related QoL.46 Carta et al reported that in individuals with a hyperthymic temperament, the increased energy resulting from increased stimulation may be advantageous.47 This genetically determined type of response may therefore be an adaptive response to the difficulties associated with the cancer diagnosis and treatment. Patients with this type of temperament may experience a state of high agitation, which is not suitable for adaptation in other types of temperament. As reported by Carta et al, the lifestyle of people with a predominant hyperthymic temperament, which includes sleep and biorhythm disruptions related to life choices, can severely affect metabolic pathways, thereby increasing the risk of prostate and breast cancer.47
We found a strong correlation between an anxious temperament and the severity of anxiety and depression symptoms, erection quality (assessed objectively and subjectively), and urinary incontinence (Table 5). Depressive and cyclothymic temperaments were correlated with depressive symptoms and the quality of erection. An irritable temperament was only associated with the quality of erection. Consistent with the results of previous analyses, there was no correlation between these parameters and the hyperthymic temperament (Table 5). Symptoms of anxiety are likely to occur in patients with PC, and it is estimated that this problem affects 20–60% of patients.36 Similarly, the occurrence of depressive disorders is common among patients who have undergone prostatectomy.36,48 De Sousa et al noted the important distinction between anxiety as a “trait,” which may be present as a basic characteristic of the patient, and anxiety as a “state,” which is a situational response to a stressor. Anxiety as a state may appear while awaiting results at the time of diagnosis or treatment. Meanwhile, anxiety as a trait is not related to the external situation and corresponds to anxiety temperament.36 Anxious and depressive temperaments predispose to the development of anxiety and mood disorders.49 This correlation is markedly modified by stress exposure.50 The positive correlation between the severity of these features of the affective temperament (TEMPS_D, TEMPS_A) and anxiety and depression symptoms (HADS-A and HADS-D) may also support these results (Table 5).
In this study, the anxious temperament was strongly correlated with urinary incontinence and sexual dysfunction, which are the symptoms of PC that are strongly associated with QoL (Table 5). There are no studies on such a relationship in the literature. However, there are works on the implications of both anxiety and depressive symptoms (understood as a state and not a trait) on these complications.13 An earlier retrospective analysis of a large cohort showed that patients with preoperative depression or anxiety are at a higher risk of postoperative urinary incontinence after prostatectomy.51 Similarly, the presence of anxiety and depression may contribute to the occurrence of sexual dysfunction.52–54
In the next stage of the study, we performed a multivariate analysis of the EORTC-PR25 subscales and examined psychological and clinical parameters, which confirmed the significance of anxious, depressive, cyclothymic, and irritable temperaments in terms of sexual activity. Nevertheless, the most important psychological factor in this analysis was the severity of anxiety and depression symptoms measured by HADS. These factors were important not only for sexual function, but also for the other EORTC-PR25 subscales. These results confirm our observations and indicate that the type of temperament plays an important role in the development of depression and anxiety symptoms as well as in QoL.
Limitations
The present study had limitations such as the small number of participants (throughout the study and in subgroups), and the nature of the study (although we used validated questionnaires, there are still the biases involved with self-reporting questionnaires); however, the findings provide insight into the role of affective temperaments in the QoL of PC survivors. Another limitation of the study is that factors, such as mood, may also affect the self-description of the respondents. Although temperament is generally stable, it can also change slightly throughout life.
Conclusion
The QoL of patients after radical prostatectomy depends on many factors, including age, interval since diagnosis, the stage of the cancer, treatment, and complications. There is also a clear relationship between the individual dimensions of affective temperament and QoL in PC survivors. Depressive, cyclothymic, irritable, and anxious temperaments are generally associated with poorer QoL in selected domains, whereas this was not observed for the hyperthymic temperament. The temperament profile is also associated with the mood and anxiety level of patients, which were identified in our study as severe determinants of a poorer QoL/functioning. The relationship between temperament, mental state, and QoL in PC survivors requires better understanding and further research.
Acknowledgments
This Research Received No External Funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dyba T, Randi G, Bray F, et al. The European cancer burden in 2020: incidence and mortality estimates for 40 countries and 25 major cancers. Eur J Cancer Oxf Engl 1990. 2021;157:308–347. doi:10.1016/j.ejca.2021.07.039
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
3. Rawla P. Epidemiology of prostate cancer. World J Oncol. 2019;10(2):63–89. doi:10.14740/wjon1191
4. Schover LR, Fouladi RT, Warneke CL, et al. Defining sexual outcomes after treatment for localized prostate carcinoma. Cancer. 2002;95(8):1773–1785. doi:10.1002/cncr.10848
5. Gaither TW, Awad MA, Osterberg EC, et al. The natural history of erectile dysfunction after prostatic radiotherapy: a systematic review and meta-analysis. J Sex Med. 2017;14(9):1071–1078. doi:10.1016/j.jsxm.2017.07.010
6. Chen RC, Hamstra DA, Sandler HM, Zietman AL. Complications of prostate cancer treatment. Lancet Oncol. 2014;15(4):e150. doi:10.1016/S1470-2045(14)70126-3
7. Salazar A, Regis L, Planas J, et al. Early continence after radical prostatectomy: a systematic review. Actas Urol Esp. 2019;43(10):526–535. doi:10.1016/j.acuro.2019.06.003
8. Bratu O, Oprea I, Marcu D, et al. Erectile dysfunction post-radical prostatectomy - a challenge for both patient and physician. J Med Life. 2017;10(1):13–18.
9. Ryan C, Wefel JS, Morgans AK. A review of prostate cancer treatment impact on the CNS and cognitive function. Prostate Cancer Prostatic Dis. 2020;23(2):207–219. doi:10.1038/s41391-019-0195-5
10. Treanor CJ, Li J, Donnelly M. Cognitive impairment among prostate cancer patients: an overview of reviews. Eur J Cancer Care. 2017;26(6):e12642. doi:10.1111/ecc.12642
11. Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site. Psychooncology. 2001;10(1):19–28. doi:10.1002/1099-1611(200101/02)10:1<19::aid-pon501>3.0.co;2-6
12. van de Wal M, van Oort I, Schouten J, Thewes B, Gielissen M, Prins J. Fear of cancer recurrence in prostate cancer survivors. Acta Oncol Stockh Swed. 2016;55(7):821–827. doi:10.3109/0284186X.2016.1150607
13. Jarzemski P, Brzoszczyk B, Popiołek A, et al. Cognitive function, depression, and anxiety in patients undergoing radical prostatectomy with and without adjuvant treatment. Neuropsychiatr Dis Treat. 2019;15:819–829. doi:10.2147/NDT.S200501
14. Üstündağ S, Zencirci AD. Factors affecting the quality of life of cancer patients undergoing chemotherapy: a questionnaire study. Asia-Pac J Oncol Nurs. 2015;2(1):17–25. doi:10.4103/2347-5625.152402
15. Gu ZH, Qiu T, Yang SH, Tian FQ, Wu H. A study on the psychological factors affecting the quality of life among ovarian cancer patients in China. Cancer Manag Res. 2020;12:905–912. doi:10.2147/CMAR.S239975
16. Heydarnejad MS, Hassanpour DA, Solati DK. Factors affecting quality of life in cancer patients undergoing chemotherapy. Afr Health Sci. 2011;11(2):266–270.
17. Akiskal HS, Akiskal KK, Haykal RF, Manning JS, Connor PD. TEMPS-A: progress towards validation of a self-rated clinical version of the temperament evaluation of the Memphis, Pisa, Paris, and San Diego Autoquestionnaire. J Affect Disord. 2005;85(1–2):3–16. doi:10.1016/j.jad.2004.12.001
18. Maremmani I, Maremmani AGI, Leonardi A, et al. Temperamental traits and results of psychoaptitude tests in applicants to become a cadet officer in the Italian Navy. J Affect Disord. 2013;150(2):634–638. doi:10.1016/j.jad.2013.02.006
19. Burnos A, Skrobowski A. Temperamental and personality traits as factors related to changes in health behaviors and quality of life in patients with metabolic syndrome in Poland. Front Psychol. 2021;12:709935. doi:10.3389/fpsyg.2021.709935
20. Janowski K, Steuden S. The temperament risk factor, disease severity, and quality of life in patients with psoriasis. Ann Dermatol. 2020;32(6):452–459. doi:10.5021/ad.2020.32.6.452
21. Boussac M, Arbus C, Dupouy J, et al. Personality dimensions are associated with quality of life in fluctuating parkinson’s disease patients (PSYCHO-STIM). J Park Dis. 2020;10(3):1057–1066. doi:10.3233/JPD-191903
22. Crestani Calegaro V, Canova Mosele PH, Lorenzi Negretto B, Zatti C, Miralha da Cunha AB, Machado Freitas LH. The role of personality in posttraumatic stress disorder, trait resilience, and quality of life in people exposed to the kiss nightclub fire. PLoS One. 2019;14(7):e0220472. doi:10.1371/journal.pone.0220472
23. Laroche F, Perrot S, Medkour T, et al. Quality of life and impact of pain in women treated with aromatase inhibitors for breast cancer. A multicenter cohort study. PLoS One. 2017;12(11):e0187165. doi:10.1371/journal.pone.0187165
24. Andrea M, Andrea M, Figueira ML. Self-perception of quality of life in patients with functional voice disorders: the effects of psychological and vocal acoustic variables. Eur Arch Oto-Rhino-Laryngol off J Eur Fed Oto-Rhino-Laryngol Soc EUFOS Affil Ger Soc Oto-Rhino-Laryngol - Head Neck Surg. 2018;275(11):2745–2754. doi:10.1007/s00405-018-5090-5
25. Costa J, García-Blanco A, Cañada Y, et al. Are affective temperaments determinants of quality of life in euthymic patients with bipolar disorder? J Affect Disord. 2018;230:101–107. doi:10.1016/j.jad.2018.01.007
26. Ozcan Dag Z, Alpua M, Isik Y, Buturak SV, Tulmac OB, Turkel Y. The evaluation of temperament and quality of life in patients with polycystic ovary syndrome. Gynecol Endocrinol off J Int Soc Gynecol Endocrinol. 2017;33(3):250–253. doi:10.1080/09513590.2016.1254610
27. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
28. van Leenders GJLH, van der Kwast TH, Grignon DJ, et al. The 2019 International Society of Urological Pathology (ISUP) consensus conference on grading of prostatic carcinoma. Am J Surg Pathol. 2020;44(8):e87. doi:10.1097/PAS.0000000000001497
29. Klovning A, Avery K, Sandvik H, Hunskaar S. Comparison of two questionnaires for assessing the severity of urinary incontinence: the ICIQ-UI SF versus the incontinence severity index. Neurourol Urodyn. 2009;28(5):411–415. doi:10.1002/nau.20674
30. Rosen R, Cappelleri J, Smith M, Lipsky J, Peña B. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):319–326. doi:10.1038/sj.ijir.3900472
31. Borkowska A, Rybakowski JK, Drozdz W, et al. Polish validation of the TEMPS-A: the profile of affective temperaments in a college student population. J Affect Disord. 2010;123(1):36–41. doi:10.1016/j.jad.2009.09.024
32. Mitchell AJ, Meader N, Symonds P. Diagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: a meta-analysis. J Affect Disord. 2010;126(3):335–348. doi:10.1016/j.jad.2010.01.067
33. Fayers P, Bottomley A. Quality of life research within the EORTC—the EORTC QLQ-C30. Eur J Cancer. 2002;38:125–133.
34. van Andel G, Bottomley A, Fosså SD, et al. An international field study of the EORTC QLQ-PR25: a questionnaire for assessing the health-related quality of life of patients with prostate cancer. Eur J Cancer Oxf Engl 1990. 2008;44(16):2418–2424. doi:10.1016/j.ejca.2008.07.030
35. Eton DT, Lepore SJ. Prostate cancer and health-related quality of life. Psychooncology. 2002;11(4):307–326. doi:10.1002/pon.572
36. De Sousa A, Sonavane S, Mehta J. Psychological aspects of prostate cancer: a clinical review. Prostate Cancer Prostatic Dis. 2012;15(2):120–127. doi:10.1038/pcan.2011.66
37. Chambers S, Ng SKA, Baade P, et al. Trajectories of quality of life, life satisfaction and psychological adjustment after prostate cancer: quality of life trajectories after prostate cancer. Psychooncology. 2016;26. doi:10.1002/pon.4342
38. Odeo S, Degu A. Factors affecting health-related quality of life among prostate cancer patients: a systematic review. J Oncol Pharm Pract off Publ Int Soc Oncol Pharm Pract. 2020;26(8):1997–2010. doi:10.1177/1078155220959414
39. Nelson CJ, Weinberger MI, Balk E, Holland J, Breitbart W, Roth AJ. The chronology of distress, anxiety, and depression in older prostate cancer patients. The Oncologist. 2009;14(9):891–899. doi:10.1634/theoncologist.2009-0059
40. Lubeck DP, Litwin MS, Henning JM, Stoddard ML, Flanders SC, Carroll PR. Changes in health-related quality of life in the first year after treatment for prostate cancer: results from CaPSURE. Urology. 1999;53(1):180–186.
41. de Lira GHS, Fornari A, Cardoso LF, Aranchipe M, Kretiska C, Rhoden EL. Effects of perioperative pelvic floor muscle training on early recovery of urinary continence and erectile function in men undergoing radical prostatectomy: a randomized clinical trial. Int Braz J Urol off J Braz Soc Urol. 2019;45(6):1196–1203. doi:10.1590/S1677-5538.IBJU.2019.0238
42. Baker H, Wellman S, Lavender V. Functional quality-of-life outcomes reported by men treated for localized prostate cancer: a systematic literature review. Oncol Nurs Forum. 2016;43(2):199–218. doi:10.1188/16.ONF.199-218
43. Ansmann L, Winter N, Ernstmann N, Heidenreich A, Weissbach L, Herden J. Health-related quality of life in active surveillance and radical prostatectomy for low-risk prostate cancer: a prospective observational study (HAROW - Hormonal therapy, Active Surveillance, Radiation, Operation, Watchful Waiting). BJU Int. 2018;122(3):401–410. doi:10.1111/bju.14215
44. Taylor JM, Chen VE, Miller RC, Greenberger BA. The impact of prostate cancer treatment on quality of life: a narrative review with a focus on randomized data. Res Rep Urol. 2020;12:533–546. doi:10.2147/RRU.S243088
45. Kesebir S, Gündoğar D, Küçüksubaşı Y, Tatlıdil Yaylacı E. The relation between affective temperament and resilience in depression: a controlled study. J Affect Disord. 2013;148(2–3):352–356. doi:10.1016/j.jad.2012.12.023
46. Bonacchi A, Miccinesi G, Guazzini M, et al. Temperament and character traits associated with health-related quality of life in cancer patients. Tumori. 2012;98(3):377–384. doi:10.1700/1125.12408
47. Carta MG, Preti A, Akiskal HS. Coping with the new era: noise and light pollution, hperactivity and steroid hormones. towards an evolutionary view of bipolar disorders. Clin Pract Epidemiol Ment Health CP EMH. 2018;14:33–36. doi:10.2174/1745017901814010033
48. Boeri L, Capogrosso P, Ventimiglia E, et al. Depressive symptoms and low sexual desire after radical prostatectomy: early and long-term outcomes in a real-life setting. J Urol. 2018;199(2):474–480. doi:10.1016/j.juro.2017.08.104
49. Unseld M, Vyssoki B, Bauda I, et al. Correlation of affective temperament and psychiatric symptoms in palliative care cancer patients. Wien Klin Wochenschr. 2018;130(21–22):653–658. doi:10.1007/s00508-018-1400-6
50. Gonda X, Eszlári N, Sutori S, et al. Nature and nurture: effects of affective temperaments on depressive symptoms are markedly modified by stress exposure. Front Psychiatry. 2020;11:599. doi:10.3389/fpsyt.2020.00599
51. Pompe RS, Krüger A, Preisser F, et al. The impact of anxiety and depression on surgical and functional outcomes in patients who underwent radical prostatectomy. Eur Urol Focus. 2020;6(6):1199–1204. doi:10.1016/j.euf.2018.12.008
52. Yang Y, Song Y, Lu Y, Xu Y, Liu L, Liu X. Associations between erectile dysfunction and psychological disorders (depression and anxiety): a cross-sectional study in a Chinese population. Andrologia. 2019;51(10):e13395. doi:10.1111/and.13395
53. Hedon F. Anxiety and erectile dysfunction: a global approach to ED enhances results and quality of life. Int J Impot Res. 2003;15(Suppl 2):S16–19. doi:10.1038/sj.ijir.3900994
54. Liu Q, Zhang Y, Wang J, et al. Erectile dysfunction and depression: a systematic review and meta-analysis. J Sex Med. 2018;15(8):1073–1082. doi:10.1016/j.jsxm.2018.05.016
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.