")
Back to Journals » Patient Preference and Adherence » Volume 11
Quality of life assessment in patients with alopecia areata and androgenetic alopecia in the People’s Republic of China
Received 1 September 2016
Accepted for publication 28 November 2016
Published 27 January 2017 Volume 2017:11 Pages 151—155
DOI https://doi.org/10.2147/PPA.S121218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Naifeng Liu
Min Zhang,1 Nan Zhang2
1Department of Dermatology, 2Department of Oncology, Jinan Central Hospital Affiliated to Shandong University, Jinan, People’s Republic of China
Introduction: In medical terms, alopecia is considered a relatively mild dermatological condition that nevertheless is a serious condition, but it causes major depression in many sufferers. Alopecia areata (AA) and androgenetic alopecia (AGA) are the main types of hair loss. This study assessed the quality of life (QoL) of Chinese patients with AA and AGA using the Dermatology Life Quality Index (DLQI) questionnaire.
Methods: A total of 178 AA and AGA patients were enrolled in this study, and DLQI was used to evaluate the QoL of the patients. The DLQI used 10 items regarding symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment as dimensions of life. Each was scored on a 0–3 scale. The total DLQI score equaled 0–30; higher scores showed greater impact on QoL.
Results: The DLQI scores of the 178 patients ranged from 0 to 28, with a mean score of 6.3. Higher DLQI scores were reported by younger patients (P<0.05) and by those who had hair loss for a duration of >12 months (P<0.05). The DLQI score of AA patients was significantly higher than that of AGA patients (P<0.05). QoL was not affected by gender, marital status, educational level, past history of alopecia, family history of alopecia, or severity of alopecia.
Conclusion: AA and AGA moderately affected the QoL of the patients. A higher DLQI score was significantly associated with younger age, hair loss for a duration of >12 months, and AA. Both AA and AGA moderately affected the QoL of the patients not only in physiological aspects but also in their emotional and social aspects. The bio-psycho-social aspects of disease need to be addressed in patients with AA and AGA, even though these conditions are not life-threatening.
Keywords: alopecia, quality of life, People’s Republic of China
Introduction
Although alopecia is regarded by physicians as a relatively mild skin disease, many patients with alopecia consider their hair loss to be a serious problem leading to distress in their everyday life and negatively affecting their activities of daily living. Because hair is a very important component of self-image, patients with alopecia may develop a distorted body image and get negative feelings.1 Reid et al reported that some patients regard their alopecia as a more serious problem than do their dermatologists.2 Therefore, it is important to understand the impact of alopecia on the quality of life (QoL) of patients.
It has been reported that the QoL of patients with hair loss was lower than that of patients with cardiovascular disease, diabetes, and cancer.3 In recent years, the importance of QoL has been widely accepted to assess the therapeutic effects in patients with hair loss.4 Some studies have concluded that physicians and patients use different criteria to assess the severity of alopecia.5 Physicians use the severity of the signs and symptoms of disease to assess alopecia, while patients focus on impaired activities and their QoL. Therefore, it is very important to understand the impact of alopecia on the QoL of patients while assessing its severity. Different instruments and questionnaires are used to assess the QoL of patients with alopecia. In 1994, Finlay and Khan6 developed the Dermatology Life Quality Index (DLQI) questionnaire to assess the QoL of patients with different skin diseases, and it has been widely used to assess alopecic severity in many countries.7,8 DLQI is a compact questionnaire, consisting of 10 questions addressing symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment.6 The patients’ scores on the DLQI range from 0 to 30, with higher scores indicating worse QOL. Given that alopecia areata (AA) and androgenetic alopecia (AGA) are the main types of hair loss in People’s Republic of China, the purpose of this study was to assess the QoL of patients with AA and AGA in Chinese patients using DLQI.
Patients and methods
Patients
A total of 178 AA and AGA patients aged >18 years were enrolled in this 2-year study at Jinan Central Hospital Affiliated to Shandong University and Qilu Hospital, Jinan, People’s Republic of China, from January 1, 2013, to December 31, 2015. All the patients were diagnosed with AA and AGA by two independent dermatologists. They included patients who visited a hospital for the treatment of alopecia and others who visited a hospital for the treatment of different diseases and showed clinical hair loss. All the patients were otherwise mentally and physically healthy and gave written informed consent to take part in the study. This study was approved by the Medical Ethics Committee for Human Studies of Shandong University.
Methods
The DLQI questionnaire consisted of 10 questions regarding symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment as dimensions of life. Each item was scored on a scale of 0–3 points. Scores were added to yield a total DLQI of 0–30 points; higher scores indicated greater impact on the patient’s QoL (Table 1).
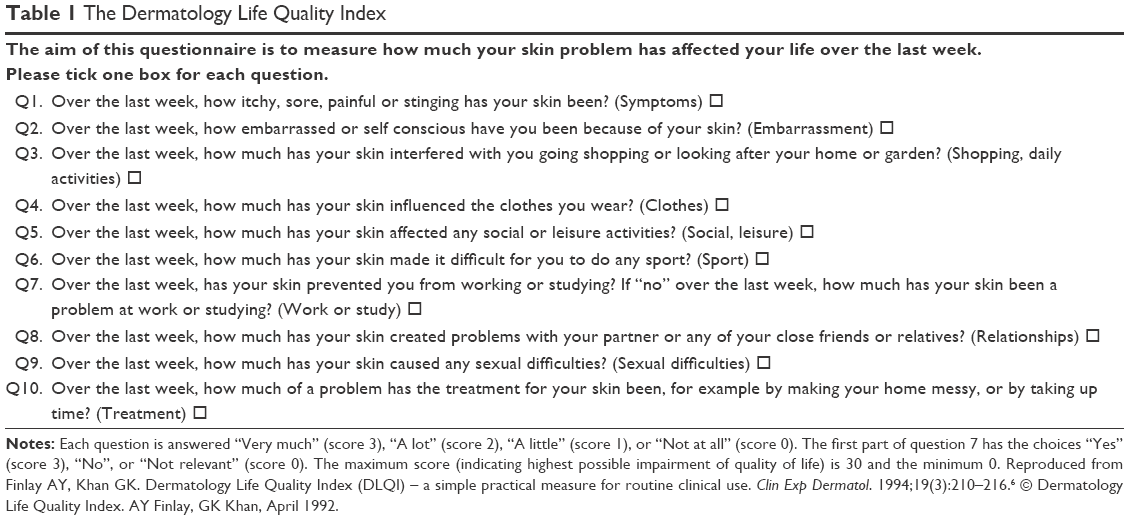 | Table 1 The Dermatology Life Quality Index |
Statistical analysis
The results were analyzed using Student’s t-test. Differences were considered significant if P-value was <0.05. The data were processed using an SPSS software package (SPSS 13.0 Inc., Chicago, IL, USA).
Results
DLQI scores
For the 178 patients with AA and AGA in this study, the DLQI scores ranged from 0 to 28, with a mean score of 6.3±6.3. Topics in questions 2 (embarrassment), 5 (social or leisure), and 7 (work or study) had the most impact on patients with hair loss (Figure 1). The lowest impacts were noted on questions 6 (sports), 8 (relationships), and 1 (symptoms) (Figures 2–5).
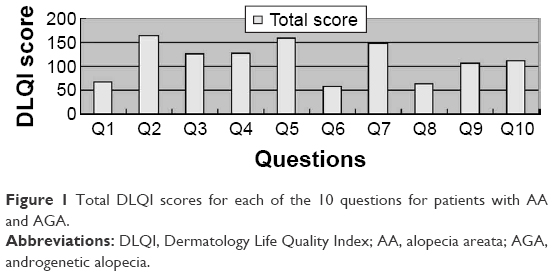 | Figure 1 Total DLQI scores for each of the 10 questions for patients with AA and AGA. |
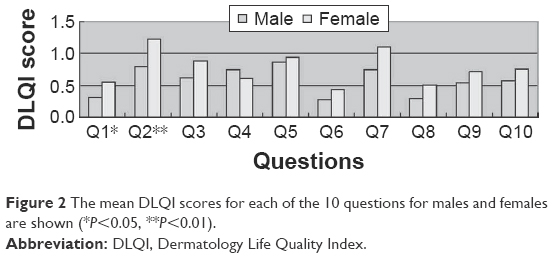 | Figure 2 The mean DLQI scores for each of the 10 questions for males and females are shown (*P<0.05, **P<0.01). |
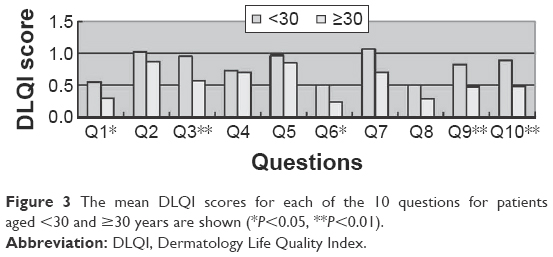 | Figure 3 The mean DLQI scores for each of the 10 questions for patients aged <30 and ≥30 years are shown (*P<0.05, **P<0.01). |
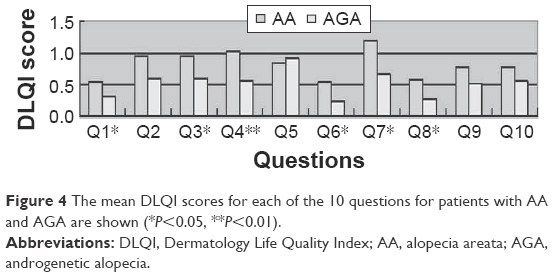 | Figure 4 The mean DLQI scores for each of the 10 questions for patients with AA and AGA are shown (*P<0.05, **P<0.01). |
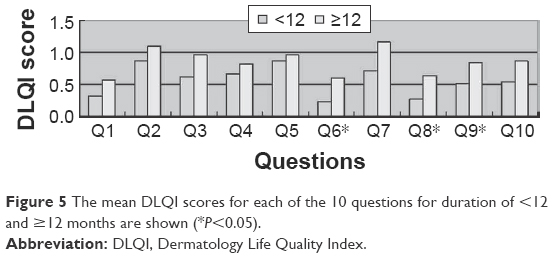 | Figure 5 The mean DLQI scores for each of the 10 questions for duration of <12 and ≥12 months are shown (*P<0.05). |
Correlation between clinical characteristics of patients and DLQI score
As shown in Table 2, a higher DLQI score was significantly correlated with younger age of the alopecia patients (P<0.05) and hair loss for a duration of >12 months (P<0.05). The DLQI score of AA patients was significantly higher than that of AGA patients (P<0.05). However, QoL was not affected by gender, marital status, educational level, past history of alopecia, family history of alopecia, or severity of alopecia (P>0.05).
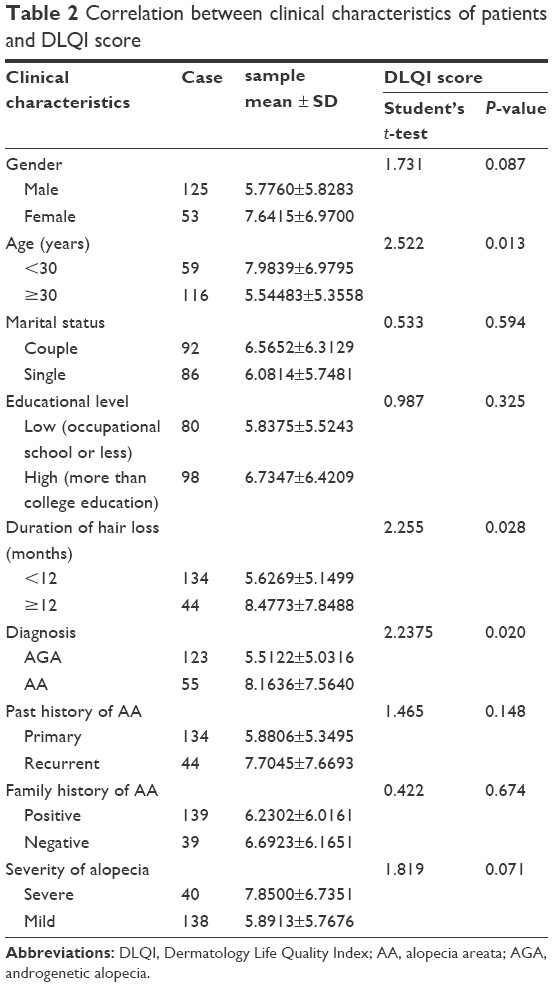 | Table 2 Correlation between clinical characteristics of patients and DLQI score |
Discussion
In our study, the mean score of DLQI was 6.3±6.3, and this is taken to represent a moderate limitation of QoL. A study by Williamson et al9 that included 70 patients with alopecia showed that the mean score of DLQI was 8.3±5.6. They found that the DLQI scores of patients with alopecia were similar to those of patients with severe psoriasis.9 Cartwright et al studied 300 patients with severe AA and found that the mean DLQI score was 13.5.10 Qi et al studied 698 Chinese patients with AA and found that the mean DLQI score was 5.8±5.6.11 These difference in findings might be due to the differences in the type of alopecia patients selected and in the degrees of severity of these alopecia patients. Our study showed that AA and AGA moderately affected the QoL, including feelings of loss of self-confidence and low self-esteem. In our study, the DLQI score of AA patients was 8.2±7.6, which was significantly higher than that of the AGA patients. Stressful life events can be triggering factors for AA patients and they may find themselves in a vicious circle of anxiety.12 In the questionnaire used in our study, items 1 and 9 referred to the physiological effects, while the remaining (2–10) referred to emotional and social effects of the disease. Our study showed that AA and AGA affected not only the physiological aspects of the patients’ lives but also their emotional and social well-being.
In this study, we found that continued changes in physiological appearance made QoL worse over time. We also found that regardless of the severity of alopecia, the mean score of younger patients was higher than that of the older ones. It appeared that the impact of alopecia on their appearance made the QoL of younger patients who were applying for a job, seeking a partner, or participating in other social activities worse. Although there were few local symptoms, presence of an itchy, sore, and painful scalp was associated with a significant increase in DLQI score.
Whether the QoL of female patients is more severely affected than that of males remains controversial. Hair has different symbolic meanings for people across cultures, affecting religious, social, and/or political beliefs in different people.13 Hair quality and appearance can be an indicator of attractiveness and sexuality for many people, and visible hair loss can have a major negative impact, particularly in some women, on self-perceptions of feminine characteristics and attractiveness.14 This appears to be a result of the emphasis and importance of physical appearance and body image in social settings.15 Some studies show that women with hair loss experience increased self-consciousness, feelings of unattractiveness, social withdrawal, emotional stress, and worry compared with women without hair loss or men with hair loss.16 Recently, however, a number of studies have also verified the psychosocial difficulties experienced by men with hair loss. These studies concluded that men with visible hair loss are generally seen by others as being significantly older, less physically and socially attractive, weaker, duller, and less potent than their peers.1 In our study, the mean DLQI scores in female patients were slightly but not significantly higher than those in male patients, and overall QoL in the male and female patients was similar.
The present study had several limitations. First, all the patients in our study were recruited in a dermatology clinic in a tertiary hospital, and selection bias may, therefore, have affected the results. Also, the study sample was relatively small compared to the total population of alopecia patients in People’s Republic of China.
Conclusion
Both AA and AGA moderately affected the QoL of our patients. A higher DLQI score was significantly associated with younger age, hair loss for a duration of more >12 months, and AA. We found that AA and AGA moderately affected the QoL of the patients not only with respect to basic physiological aspects of hair loss but also with respect to the emotional and social aspects of their lives. The medical system needs to adequately address the problems of daily living and bio-psycho-social concerns of these patients, even though their visible hair loss is not a life-threatening condition.
Acknowledgment
The authors would like to thank Shandong University for its cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
Han SH, Byun JW, Lee WS, et al. Quality of life assessment in male patients with androgenetic alopecia: result of a prospective, multicenter study. Ann Dermatol. 2012;24(3):311–318. | ||
Reid EE, Haley AC, Borovicka JH, et al. Clinical severity does not reliably predict quality of life in women with alopecia areata, telogen effluvium, or androgenic alopecia. J Am Acad Dermatol. 2012;66(3):e97–e102. | ||
Nichol MB, Margolies JE, Lippa E, Rowe M, Quell J. The application of multiple quality-of-life instruments in individuals with mild-to-moderate psoriasis. Pharmacoeconomics. 1996;10(6):644–653. | ||
Ashcroft DM, Li Wan Po A, Williams HC, Griffiths CE. Quality of life measures in psoriasis: a critical appraisal of their quality. J Clin Pharm Ther. 1998;23(5):391–398. | ||
Krueger GG, Feldman SR, Camisa C, et al. Two considerations for patients with psoriasis and their clinicians: what defines mild, moderate, and severe psoriasis? What constitutes a clinically significant improvement when treating psoriasis? J Am Acad Dermatol. 2000;43(2 Pt 1):281–285. | ||
Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI) – a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. | ||
Nakagawa H, Schenkel B, Kato M, Kato T, Igarashi A; Japanese Ustekinumab Study Group. Impact of ustekinumab on health-related quality of life in Japanese patients with moderate-to-severe plaque psoriasis: results from a randomized, double-blind, placebo-controlled phase 2/3 trial. J Dermatol. 2012;39(9):761–769. | ||
Torii H, Sato N, Yoshinari T, Nakagawa H; Japanese Infliximab Study Investigators. Dramatic impact of a Psoriasis Area and Severity Index 90 response on the quality of life in patients with psoriasis: an analysis of Japanese clinical trials of infliximab. J Dermatol. 2012;39(3):253–259. | ||
Williamson D, Gonzalez M, Finlay AY. The effect of hair loss on quality of life. J Eur Acad Dermatol Venereol. 2001;15(2):137–139. | ||
Cartwright T, Endean N, Porter A. Illness perceptions, coping and quality of life in patients with alopecia. Br J Dermatol. 2009;160(5):1034–1039. | ||
Qi S, Xu F, Sheng Y, Yang Q. Assessing quality of life in alopecia areata patients in China. Psychol Health Med. 2015;20(1):97–102. | ||
Güleç AT, Tanriverdi N, Dürü C, Saray Y, Akçali C. The role of psychological factors in alopecia areata and the impact of the disease on the quality of life. Int J Dermatol. 2004;43(5):352–356. | ||
Erol O, Can G, Aydiner A. Effects of alopecia on body image and quality of life of Turkish cancer women with or without headscarf. Support Care Cancer. 2012;20(10):2349–2356. | ||
Helms RL, O’Hea EL, Corso M. Body image issues in women with breast cancer. Psychol Health Med. 2008;13(3):313–325. | ||
Cash TF, Price VH, Savin RC. Psychological effects of androgenetic alopecia on women: comparisons with balding men and with female control subjects. J Am Acad Dermatol. 1993;29(4):568–575. | ||
Dolte KS, Girman CJ, Hartmaier S, Roberts J, Bergfeld W, Waldstreicher J. Development of a health-related quality of life questionnaire for women with androgenetic alopecia. Clin Exp Dermatol. 2000;25(8):637–642. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.