")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
Quality of Life and Psychological Effects of Port-Wine Stain: A Review of Literature
Authors Wanitphakdeedecha R , Ng JNC , Yan C , Manuskiatti W, Sudhipongpracha T, Jantarakolica T
Received 14 April 2021
Accepted for publication 12 May 2021
Published 22 June 2021 Volume 2021:14 Pages 681—690
DOI https://doi.org/10.2147/CCID.S315804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Rungsima Wanitphakdeedecha,1,2 Janice Natasha C Ng,1 Chadakan Yan,1 Woraphong Manuskiatti,1 Tatchalerm Sudhipongpracha,2 Tatre Jantarakolica3
1Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2College of Interdisciplinary Studies, Thammasat University, Bangkok, Thailand; 3Faculty of Economics, Thammasat University, Bangkok, Thailand
Correspondence: Rungsima Wanitphakdeedecha
Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Pran-nok Road, Bangkok, 10700, Thailand
Tel + 66-2419-4333
Fax + 66-2411-9922
Email [email protected]
Introduction: Port-wine stain (PWS) is a congenital malformation that does not resolve spontaneously and can cause a physiological or psychological burden to the patients. At present, most of the studies done on PWS are focused on the treatment rather than the quality of life and psychological effects of the disease.
Material and Methods: A comprehensive literature search was done in MEDLINE using PubMed database, Embase®, and Cochrane. All observational studies were included in this review.
Results: A total of 17 relevant articles with 2,135 PWS patients were included in this review. There were 36 measurement tools used to assess the quality of life and the psychological effects among PWS patients. The results showed that patients with facial PWS had a significant negative effect on their quality of life and had also suffered from psychological disabilities. The PWS lesion tends to worsen with age and may cause further adaptation problems towards the social environment, especially in children.
Conclusion: Early treatment, psychological assistance, and patient support are the key management in improving the quality of life of patients with PWS. Quality of life must be regularly assessed together with the improvement of treatment.
Keywords: port-wine stain, quality of life, psychological effects
Introduction
Port-wine stain (PWS) is a congenital capillary malformation commonly found in the head and neck, with an incidence of 0.3–0.9% in newborns, and affects males and females equally.1,2 In Spain, a study among 1000 newborns showed that 72% presented with birthmarks and of these, 0.8% was PWS.3 Initially, the lesions appear as pink or red macules, which do not undergo spontaneous involution and may progressively darken to reddish purple.4 The lesions grow proportionately with age and can lead to the formation of papules and nodules or they may develop into hypertrophic PWS.5 Aside from the cosmetic disfigurement, PWS hypertrophy may also impair sight, speech, nasal breathing and hearing.6
Lasers have been used in the treatment of PWS for more than 30 years.7 The pulsed dye laser (PDL) is the treatment of choice as exhibited by its clinical efficacy.8 It utilizes the principle of selective photothermolysis to injure the ectatic dermal capillaries, thereby reducing the redness and flattening the lesion.9 Aside from PDL, other treatment modalities include topical antiangiogenic agents and other lasers, such as intense pulse light (IPL), small and large spot 532 nm potassium-titanyl-phosphate (KTP) laser, 1064 nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser and Alexandrite 755 nm laser.10,11 Photodynamic therapy (PDT) is a safe and effective treatment for facial PWS in children.12 Furthermore, the large spot 532 nm KTP laser is highly effective in the treatment of PWS lesions in the body.11
PWS is associated with two uncommon syndromes: Sturge–Weber syndrome (SWS) and Klippel-Trenaunay syndrome (KTS).13 SWS is a neurocutaneous disorder characterized by PWSs usually affecting one hemiface along one or more trigeminal branches, with associated leptomeningeal angiomas, glaucoma, seizures, stroke-like episodes, and mental retardation.14,15 On the other hand, a recent study demonstrated that the distribution of facial PWS is related to the embryonic vasculature of the face rather than the trigeminal nerve. Hence, facial PWS located on the forehead appears to be a significant predictor of SWS.16 Due to these complications, many patients diagnosed with SWS would need protection and assistance to incorporate themselves into the society and have a better quality of life.17 KTS is a congenital developmental disorder characterized by PWS, venous abnormalities, soft tissue and bony hypertrophy involving a unilateral extremity.18
At present, most studies done on PWS were focused on the treatment rather than the quality of life and psychological effects of the disease. The body image of oneself and others are important in the development of personality and interpersonal relationships, and more often than not, physical appearance is rated higher than a person’s character.19 The stigma of having a disfiguring facial birthmark can lead to significant adverse psychosocial effects.20
There are several Health-Related Quality of Life (HRQoL) instruments used to assess the impact of a disease on the quality of life of the patients, which are categorized into generic and specific instruments (dermatology-specific and disease-specific instruments).21 Several generic tools are frequently used for the measurement of HRQoL in all diseases, such as the Short-Form Health Survey (SF-36), EuroQoL EQ-5D, Nottingham Health Profile (NHP), Sickness Impact Profile (SIP) and World Health Organization Quality of Life assessment (WHOQOL).21 Some dermatology-specific health-related QoL Instruments, such as the Dermatology Life Quality Index questionnaire (DLQI), Children’s Dermatology Life Quality Index (CDLQI), the Dermatology Quality of Life Scales (DQOLS), the Dermatology-Specific Quality of Life instrument (DSQL, Skindex-17 and Skindex-29 were used to assess the quality of life of skin disease.21 Lastly, there is no established disease-specific instrument for PWS patients.
In general, the goal of facial PWS treatment is to cure or to achieve complete clearance of the lesion. However, if we only focus on the treatment of the lesion, there is a tendency to overlook the holistic management of the patient in terms of other aspects, such as quality of life and the psychological effects of the disease. The objective of this article is to provide an overview and assessment of published studies with regard to the quality of life and psychological effects of PWS.
Materials and Methods
A comprehensive literature search was done in MEDLINE using PubMed database, Embase®, and Cochrane last September 14, 2020. The keywords [(port wine stain) AND (quality of life) AND (psychological effects)] were used. All observational studies and full research articles written in English were included. Individual case reports, reviews, conference abstracts, presentations, and basic science manuscripts were excluded. EndnoteX8 (Thomson Reuters 2016) was used to organize the bibliography and screen the articles for duplication. Each article was independently reviewed by two of the authors. We extracted the country, sample size, study design, study population, measures used, and outcomes measured from the studies. We assigned the level of evidence based on the Oxford Centre for Evidence-based Medicine (OCEBM).
Results
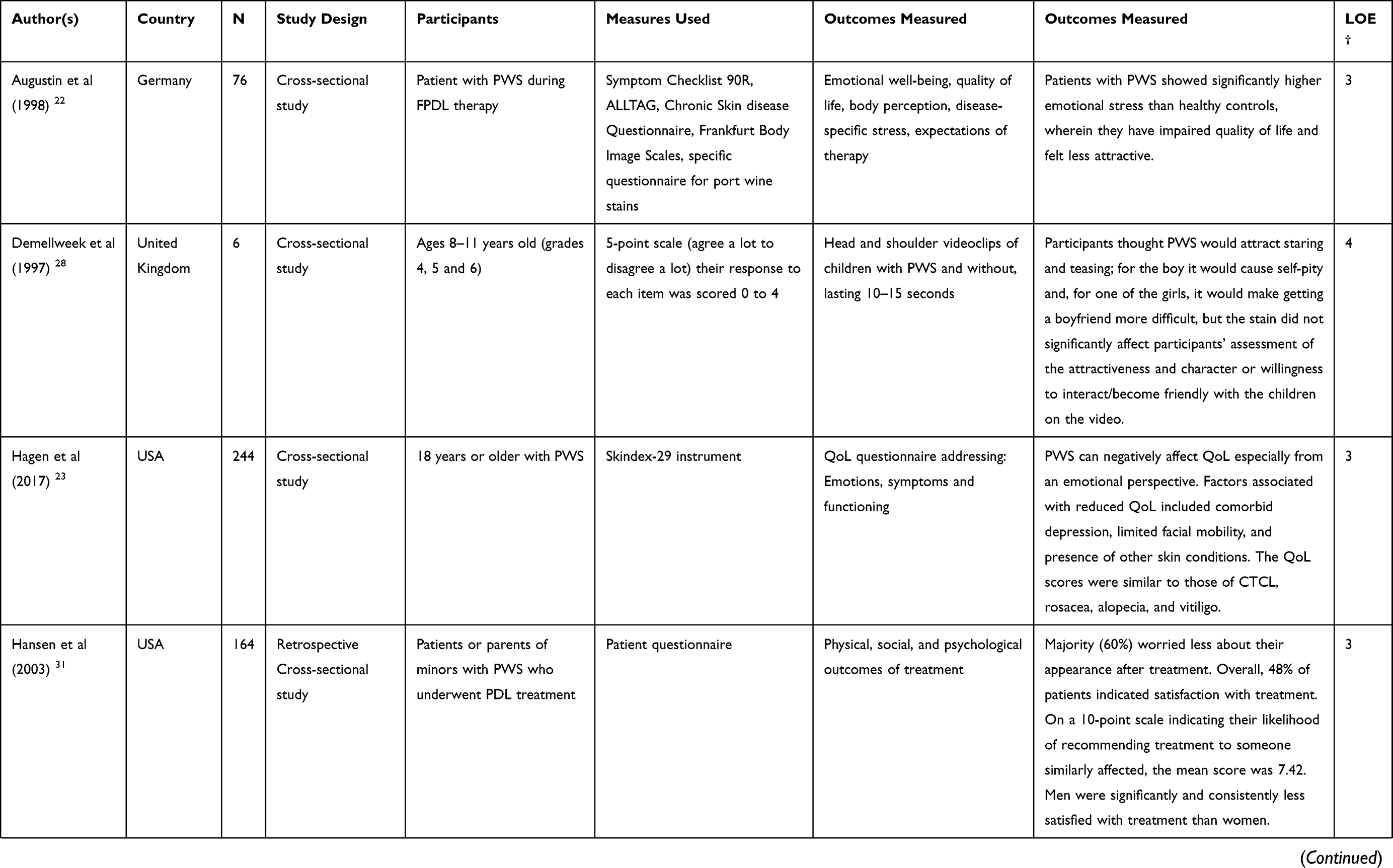
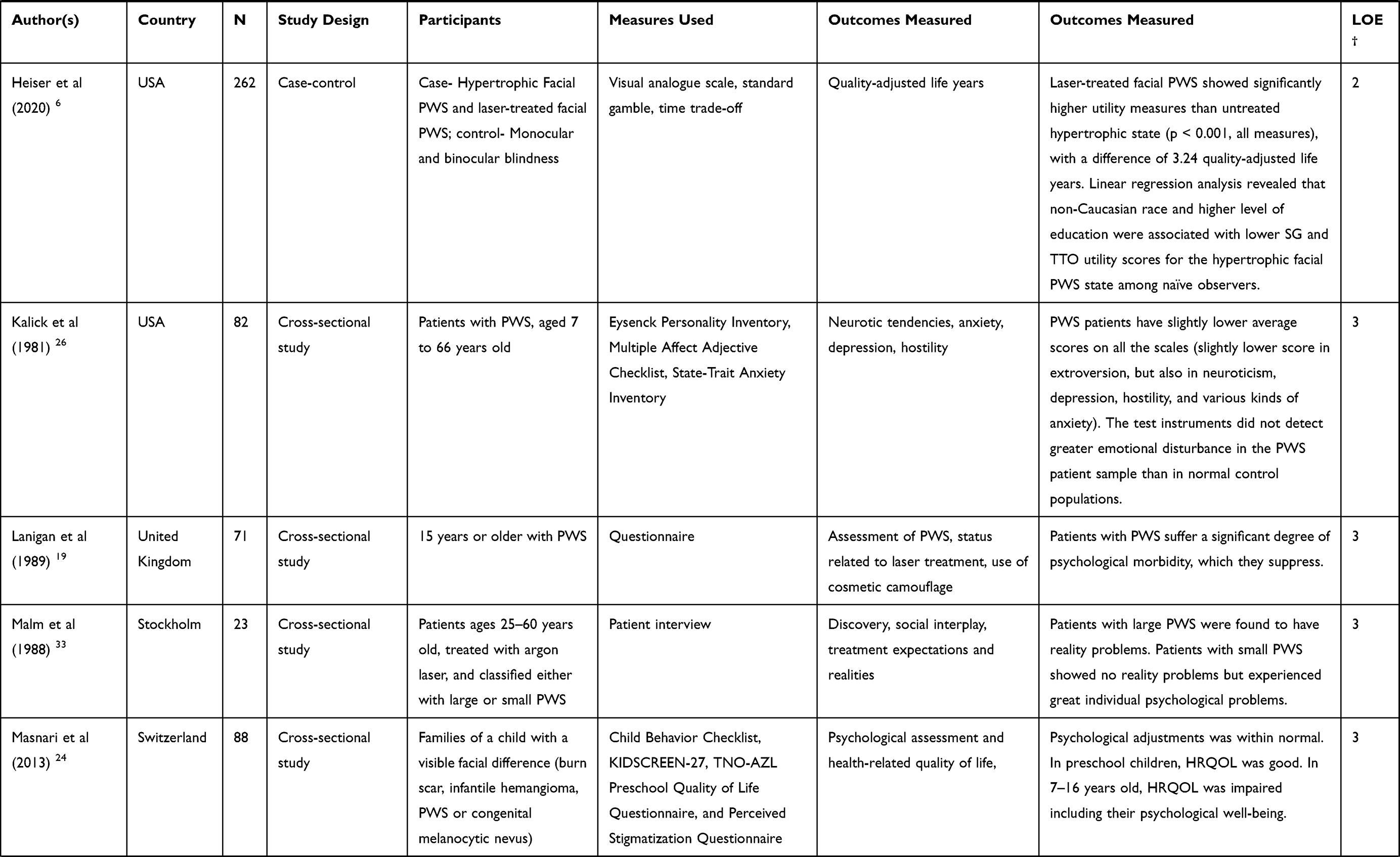
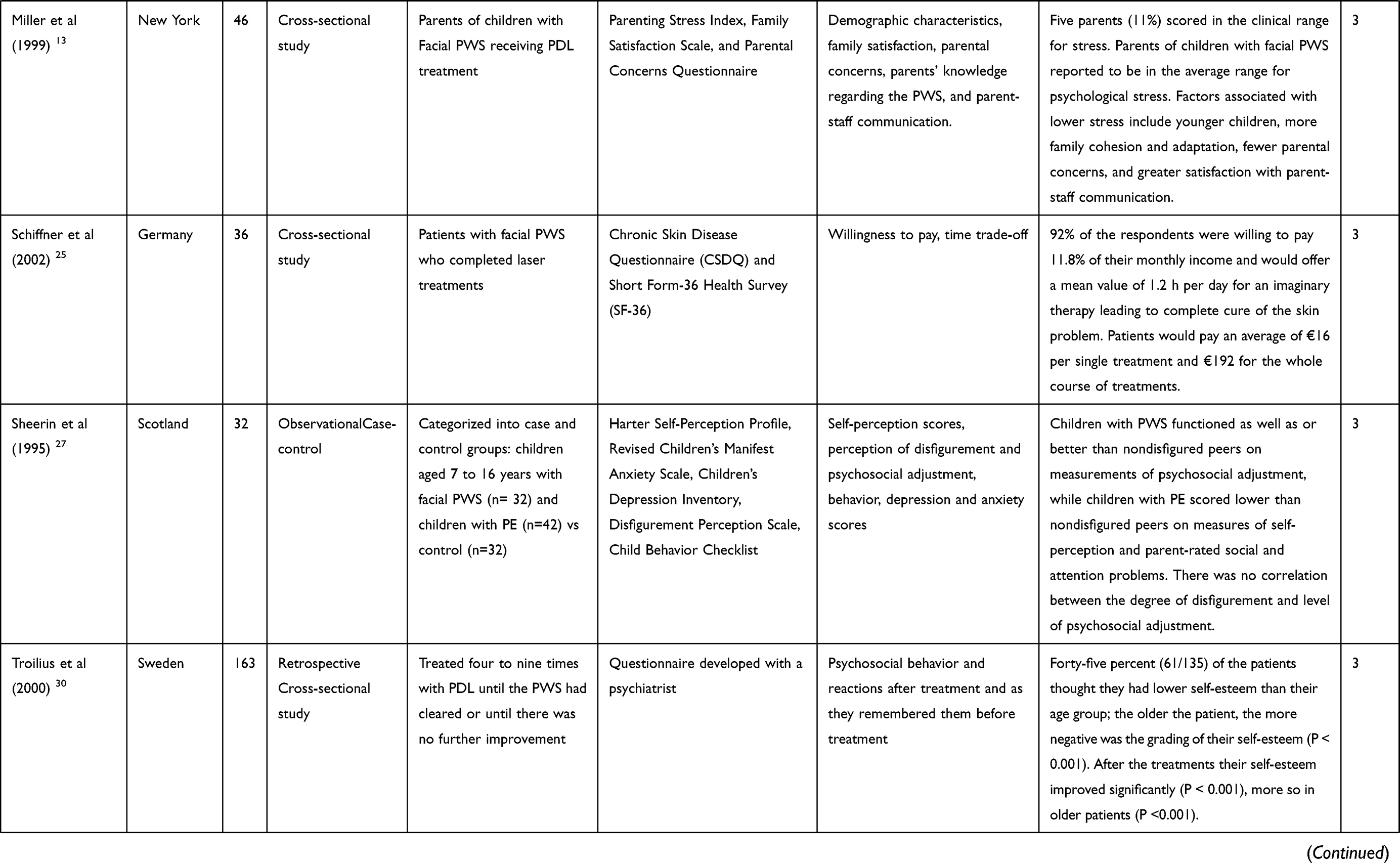
Our systematic search identified 45 articles. After screening, a total of 17 articles met the inclusion criteria and were included. Among the searched observational studies, there were 3 case-control and 14 cross-sectional studies identified. In total, the 17 studies comprised of 2,135 facial PWS patients and 36 questionnaires were included in the study. The study characteristics and the measurement tools are summarized in Table 1.
 |
 |
 |
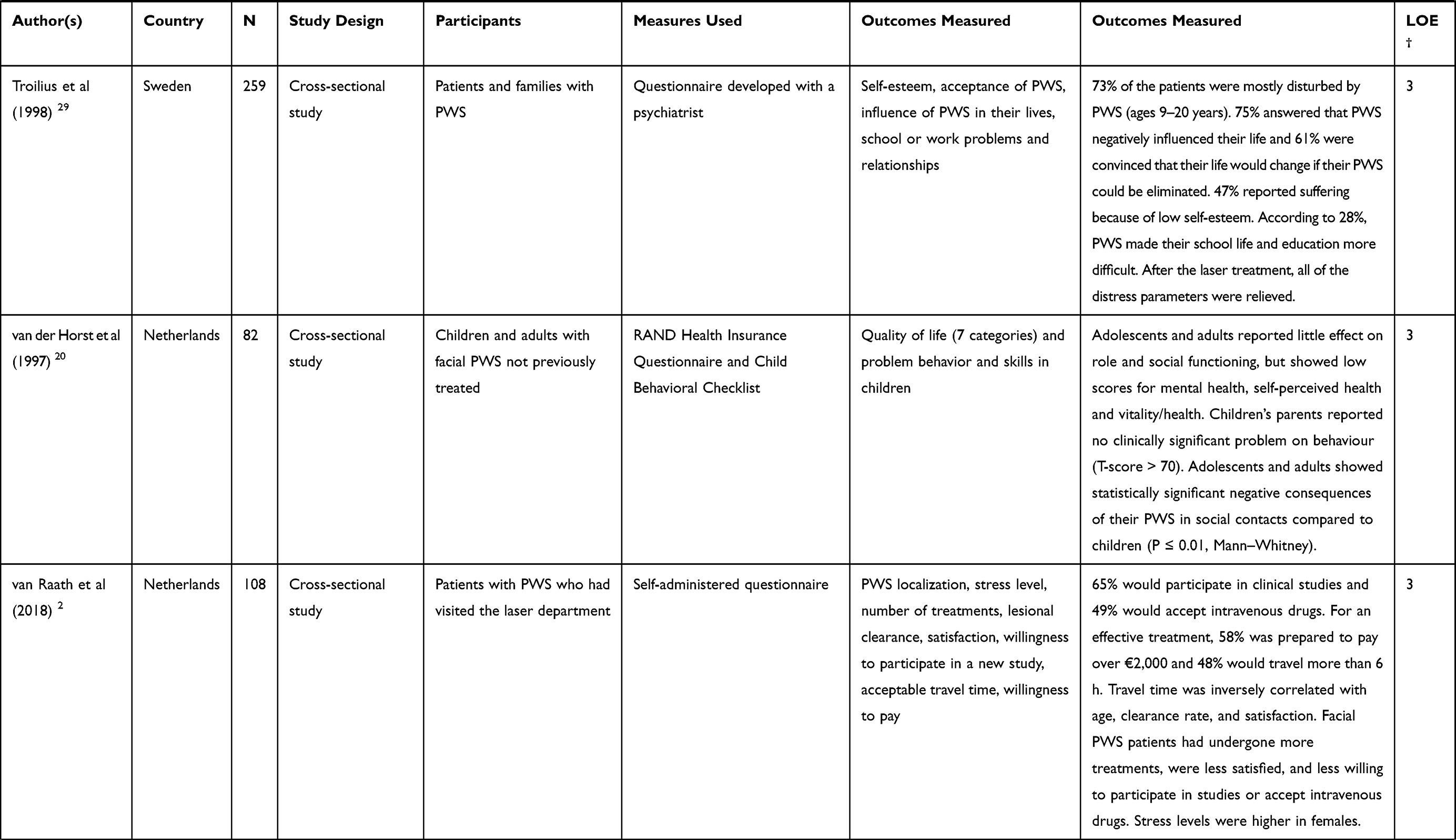 |
Table 1 Overview of Quality of Life and Psychosocial Effects in Patients with PWS |
The outcome measurement tools used to assess quality of life include Symptom Checklist 90R,22 ALLTAG,22 Chronic Skin disease Questionnaire,22 Frankfurt Body Image Scales,22 Specific questionnaire for port wine stains,22 Skindex-29 instrument,23 Child Behavior Checklist,24 KIDSCREEN-27,24 TNO-AZL Preschool Quality of Life Questionnaire,24 Chronic Skin Disease Questionnaire (CSDQ),25 Short Form-36 Health Survey (SF-36),25 RAND Health Insurance Questionnaire,20 Child Behavioral Checklist20 and DLQI.5 Based on the results of these questionnaires, it was proven that patients with Facial PWS have a significant negative effect on their quality of life.
The outcome measurement tools used to assess the psychological effects include Eysenck Personality Inventory,26 Multiple Affect Adjective Checklist,26 State-Trait Anxiety Inventory,26 Perceived Stigmatization Questionnaire,24 Parenting Stress Index,13 Family Satisfaction Scale,13 Parental Concerns Questionnaire,13 Harter Self-Perception Profile,27 Revised Children’s Manifest Anxiety Scale,27 Children’s Depression Inventory,27 Disfigurement Perception Scale,27 and Child Behavior Checklist.27 The results from these questionnaires show that patients with facial PWS suffered from psychological disabilities. The lesion is expected to worsen with age and may lead to adaptation problems towards the social environment, especially in children.19
Discussion
This systematic review examined the impact on the quality of life and psychological effects of PWS in both adults and children.
Quality of Life
Facial PWS was proven to have a significant negative effect on the quality of life, and had scores similar to those diagnosed with cutaneous T-cell lymphoma (CTCL), rosacea, alopecia and vitiligo.23 On the contrary, it was reported that these patients functioned as well or even better than their normal peers and it was concluded that psychosocial adjustment depends on the type of disfigurement or deformity, and it was unrelated to the severity of the disfigurement.27
Difference Among Age Groups
In general, patients with PWS suffer considerable psychological disabilities that they suppress, and these difficulties do not improve with advancing age and may cause further adaptation problems to their social environment.19 In our literature search, we found that adults and children have a different reaction towards the psychosocial effects of PWS.
Children with PWS are usually discriminated by their peers.28 A study was done among school-aged children with visible facial differences (PWS, burn scar, infantile hemangioma and congenital melanocytic nevus) and was found to have an impaired quality of life and psychological well-being relative to the norm, but these findings were not seen in pre-school children.24
Compared with children, adolescents and adults with PWS showed statistically significant negative consequences among their social contacts.20 Adults with PWS also complain of how they were treated by others, and they believed that their skin condition makes it more difficult to attract potential sexual partners.28 The progression of the PWS lesion increases with age as presented in Figure 1.
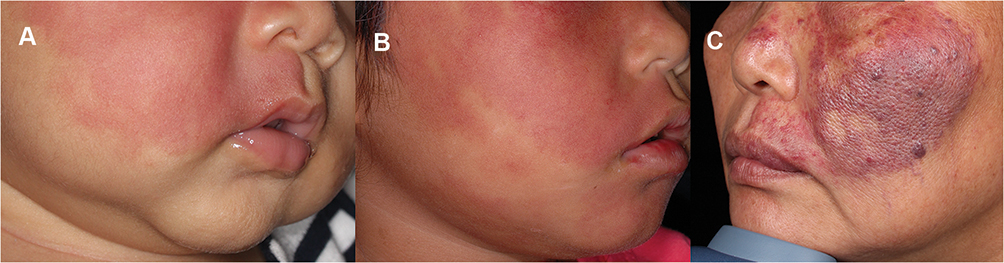 |
Figure 1 Clinical photographs of facial PWS among patients. Clinical photographs of facial PWS among patients in different age groups (A) a 4-month infant (B) a 5-year old child and (C) a 51-year old woman. |
Early Treatment
In a previous study, 75% answered that PWS negatively influenced their life and 61% were convinced that their life would change if their PWS could be eliminated.29 Several studies have reported that patients with PWS showed improved psychosocial status after their treatment when compared to before.29,30
The societal-perceived utility of hypertrophic facial PWS was found to be similar to monocular blindness, while laser-treated facial PWS was significantly perceived more favorably than the untreated hypertrophic state.6 This shows the burden of the disease and the impact of treating it with laser. Among 164 PWS patients treated with PDL, 60% were satisfied with the treatment and 61% would recommend it to others, although men were significantly less satisfied with the treatment compared to women.31 During treatment, close attention must be performed to assess the quality of life and mental status of female PWS patients, lesion areas >30 cm2, or those with hypertrophic PWS.5 Among the different lesional characteristics, size was found to be the most important in the overall disfiguring effect of PWS.32 Patients with large PWS may have problems in their interactions with their environment characterized by their individual life events and personality dynamics, while those with small PWS experienced great individual psychological problems.33
Patients with PWS who had greater emotional stress were found to have unrealistic expectations with regards to therapy.22 It is important to clarify this prior to treatment, since excessive therapy expectations can lead to a less stable emotional well-being and unfavorable coping mechanism.22
Willingness to Pay for Treatment
Patients with facial PWS were willing to pay 11.8% of their monthly income and would offer a mean value of 1.2 hours per day for an imaginary therapy leading to a complete cure of their skin problem.25 It was reported that females with PWS are more willing to undergo experimental treatments and accept intravenous administration.2 These findings can be useful in evaluating the expected compliance of patients to a possible new treatment modality.
Parental Support
Management of a patient with PWS involves a holistic approach, which includes extensive family support. As much as we want to recommend early treatment, the common dilemma of parents includes weighing the possible future social risks of PWS against the pain of laser therapy and its costs.4 It was reported that parents of children with facial PWS had lower stress when they had younger children, more family cohesion and adaptation, fewer parental concerns, and greater satisfaction with parent-staff communication.13 This study suggests the importance of having a clear and comprehensive communication, which is sensitive to the psychological needs of the patients and the parents.
Despite the significant findings, only a few number of studies have been published with regards to this topic. Therefore, it is recommended that future studies with a large sample size be conducted. Also, it would be more useful if a standardized assessment tool specifically for the quality of life and psychological effects of PWS be established.
Conclusion
Early treatment, psychological assistance and patient support are the key management in improving the quality of life of patients with PWS. Quality of life must be regularly assessed together with the improvement of treatment.
Abbreviations
PWS, Port-wine stain; DLQI, Dermatology Life and Quality Index; QoL, quality of life; CTCL, cutaneous T-cell lymphoma; h, hour; PDL, pulsed dye laser; PE, prominent ears; FPDL, flashed lamp-pumped pulsed dye laser; ALLTAG, A questionnaire to record functional capacity in everyday life; HRQOL, health-related quality of life; SG, standard gamble; TTO, time trade-off; HRQoL, Health-Related Quality of Life; LOE, Level of evidence.
Acknowledgments
This systematic review is supported by the Faculty of Medicine Siriraj Hospital, Mahidol University. The authors wish to thank Dr. Surachet Sirisuthivoranunt, Ms. Phonsuk Yamlexnoi and Ms. Chutikan Kiatphansodsai for their assistance in managing the database.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Almeida de Arruda JA, Andrade ES, Andrade RA, Pereira JRD, Callou G. Vascular malformation of the face: a rare case with follow-up of 18 years. Acta Stomatol Croat. 2017;51(4):332–335. doi:10.15644/asc51/4/8
2. van Raath MI, Bambach CA, Dijksman LM, Wolkerstorfer A, Heger M. Prospective analysis of the port-wine stain patient population in the Netherlands in light of novel treatment modalities. J Cosmet Laser Ther. 2018;20(2):77–84. doi:10.1080/14764172.2017.1368669
3. Monteagudo B, Labandeira J, León-Muiños E, et al. [Prevalence of birthmarks and transient skin lesions in 1,000 Spanish newborns]. Actas Dermosifiliogr. 2011;102(4):264–269. doi:10.1016/j.ad.2010.08.001
4. Strauss RP, Resnick SD. Pulsed dye laser therapy for port-wine stains in children: psychosocial and ethical issues. J Pediatr. 1993;122(4):505–510. doi:10.1016/S0022-3476(05)83527-9
5. Wang J, Zhu YY, Wang ZY, et al. Analysis of quality of life and influencing factors in 197 Chinese patients with port-wine stains. Medicine. 2017;96(51):e9446. doi:10.1097/MD.0000000000009446
6. Heiser A, Jowett N, Occhiogrosso J, Tessler O, Tan OT. Societal-perceived health utility of hypertrophic facial port-wine stain and laser treatment. Facial Plast Surg Aesthet Med. 2020;22(5):327–335. doi:10.1089/fpsam.2020.0059
7. De Borgie CA, Bossuyt PM, van der Horst CM, van Gemert MJ. Introduction of the flash-lamp pulsed-dye laser treatment of facial port-wine stains in childhood: a case of health care technology assessment. Lasers Surg Med. 2001;28(2):182–189. doi:10.1002/lsm.1037
8. Faurschou A, Olesen AB, Leonardi-Bee J, Haedersdal M. Lasers or light sources for treating port-wine stains. Cochrane Database Syst Rev. 2011;11:Cd007152. doi:10.1002/14651858.CD007152.pub2
9. Loffeld A, Zaki I, Abdullah A, Lanigan S. Study of patient-reported morbidity following V-beam pulsed-dye laser treatment of port wine stains. Lasers Med Sci. 2005;20(3–4):114–116. doi:10.1007/s10103-005-0351-0
10. Updyke KM, Khachemoune A. Port-wine stains: a focused review on their management. J Drugs Dermatol. 2017;16(11):1145–1151.
11. Kwiek B, Sieczych J, Rożalski M, Kowalewski C, Ambroziak M. Usefulness of three-dimensional digital image analysis for objective evaluation of the efficacy of non-facial port-wine stain treatment with large spot 532 nm laser. Postepy Dermatologii I Alergologii. 2020;37(4):572–578. doi:10.5114/ada.2019.83520
12. Zhang B, Zhang T-H, Huang Z, Li Q, Yuan K-H, Hu Z-Q. Comparison of pulsed dye laser (PDL) and photodynamic therapy (PDT) for treatment of facial port-wine stain (PWS) birthmarks in pediatric patients. Photodiagnosis Photodyn Ther. 2014;11(4):491–497. doi:10.1016/j.pdpdt.2014.06.004
13. Miller AC, Pit-Ten Cate IM, Watson HS, Geronemus RG. Stress and family satisfaction in parents of children with facial port-wine stains. Pediatr Dermatol. 1999;16(3):190–197. doi:10.1046/j.1525-1470.1999.00051.x
14. Bianchi F, Auricchio AM, Battaglia DI, Chieffo DRP, Massimi L. Sturge-Weber syndrome: an update on the relevant issues for neurosurgeons. Childs Nerv Syst. 2020;36(10):2553–2570. doi:10.1007/s00381-020-04695-3
15. Jagtap S, Srinivas G, Harsha KJ, Radhakrishnan N, Radhakrishnan A. Sturge-Weber syndrome: clinical spectrum, disease course, and outcome of 30 patients. J Child Neurol. 2013;28(6):725–731. doi:10.1177/0883073812451326
16. Waelchli R, Aylett SE, Robinson K, Chong WK, Martinez AE, Kinsler VA. New vascular classification of port-wine stains: improving prediction of Sturge-Weber risk. Br J Dermatol. 2014;171(4):861–867. doi:10.1111/bjd.13203
17. Pascual-Castroviejo I, Pascual-Pascual SI, Velazquez-Fragua R, Viaño J. Sturge-Weber syndrome: study of 55 patients. Can J Neurol Sci. 2008;35(3):301–307. doi:10.1017/S0317167100008878
18. Latessa V, Frasier K. Case study: a minimally invasive approach to the treatment of Klippel-Trenaunay syndrome. J Vasc Nurs. 2007;25(4):76–84. doi:10.1016/j.jvn.2007.09.004
19. Lanigan SW, Cotterill JA. Psychological disabilities amongst patients with port wine stains. Br J Dermatol. 1989;121(2):209–215. doi:10.1111/j.1365-2133.1989.tb01800.x
20. van der Horst CM, de Borgie CA, Knopper JL, Bossuyt PM. Psychosocial adjustment of children and adults with port wine stains. Br J Plast Surg. 1997;50(6):463–467. doi:10.1016/S0007-1226(97)90335-0
21. Prinsen CA, de Korte J, Augustin M, et al. Measurement of health-related quality of life in dermatological research and practice: outcome of the EADV taskforce on quality of life. J Eur Acad Dermatol Venereol. 2013;27(10):1195–1203. doi:10.1111/jdv.12090
22. Augustin M, Zschocke I, Wiek K, Peschen M, Vanscheidt W. Psychosocial stress of patients with port wine stains and expectations of dye laser treatment. Dermatology. 1998;197(4):353–360. doi:10.1159/000018031
23. Hagen SL, Grey KR, Korta DZ, Kelly KM. Quality of life in adults with facial port-wine stains. J Am Acad Dermatol. 2017;76(4):695–702. doi:10.1016/j.jaad.2016.10.039
24. Masnari O, Schiestl C, Rössler J, et al. Stigmatization predicts psychological adjustment and quality of life in children and adolescents with a facial difference. J Pediatr Psychol. 2013;38(2):162–172. doi:10.1093/jpepsy/jss106
25. Schiffner R, Brunnberg S, Hohenleutner U, Stolz W, Landthaler M. Willingness to pay and time trade-off: useful utility indicators for the assessment of quality of life and patient satisfaction in patients with port wine stains. Br J Dermatol. 2002;146(3):440–447. doi:10.1046/j.1365-2133.2002.04613.x
26. Kalick SM, Goldwyn RM, Noe JM. Social issues and body image concerns of port wine stain patients undergoing laser therapy. Lasers Surg Med. 1981;1(3):205–213. doi:10.1002/lsm.1900010303
27. Sheerin D, MacLeod M, Kusumakar V. Psychosocial adjustment in children with port-wine stains and prominent ears. J Am Acad Child Adolesc Psychiatry. 1995;34(12):1637–1647. doi:10.1097/00004583-199512000-00014
28. Demellweek C, Humphris GM, Hare M, Brown J. Children’s perception of, and attitude towards, unfamiliar peers with facial port-wine stains. J Pediatr Psychol. 1997;22(4):471–485. doi:10.1093/jpepsy/22.4.471
29. Troilius A, Wrangsjö B, Ljunggren B. Potential psychological benefits from early treatment of port-wine stains in children. Br J Dermatol. 1998;139(1):59–65. doi:10.1046/j.1365-2133.1998.02314.x
30. Troilius A, Wrangsjö B, Ljunggren B. Patients with port-wine stains and their psychosocial reactions after photothermolytic treatment. Dermatol Surg. 2000;26(3):190–196. doi:10.1046/j.1524-4725.2000.09204.x
31. Hansen K, Kreiter CD, Rosenbaum M, Whitaker DC, Arpey CJ. Long-term psychological impact and perceived efficacy of pulsed-dye laser therapy for patients with port-wine stains. Dermatol Surg. 2003;29(1):49–55. doi:10.1046/j.1524-4725.2003.29010.x
32. Koster PH, Bossuyt PM, van der Horst CM, Gijsbers GH, van Gemert MJ. Characterization of portwine stain disfigurement. Plast Reconstr Surg. 1998;102(4):1210–1218. doi:10.1097/00006534-199809020-00047
33. Malm M, Carlberg M. Port-wine stain–a surgical and psychological problem. Ann Plast Surg. 1988;20(6):512–516. doi:10.1097/00000637-198806000-00002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.