")
Back to Journals » OncoTargets and Therapy » Volume 9
Quality of life and cosmetic result of single-port access endoscopic thyroidectomy via axillary approach in patients with papillary thyroid carcinoma
Authors Huang J, Ma L, Song W, Lu B, Huang Y, Dong H
Received 6 November 2015
Accepted for publication 29 January 2016
Published 4 July 2016 Volume 2016:9 Pages 4053—4059
DOI https://doi.org/10.2147/OTT.S99980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Li
Jian-kang Huang,1 Ling Ma,2 Wen-hua Song,1 Bang-yu Lu,3 Yu-bin Huang,3 Hui-ming Dong1
1Department of Surgical Oncology, 2Department of Gynecologic Tumor, The First Affiliated Hospital of Bengbu Medical College, Bengbu, Anhui, 3Department of Minimally Invasive Surgery, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China
Background: Endoscopic thyroidectomy for minimally invasive thyroid surgery has been widely applied in the past decade. The present study aimed to evaluate the effects of single-port access transaxillary totally endoscopic thyroidectomy on the postoperative outcomes and functional parameters, including quality of life and cosmetic result in patients with papillary thyroid carcinoma (PTC).
Patients and methods: Seventy-five patients with PTC who underwent endoscopic thyroidectomy via a single-port access transaxillary approach were included (experimental group). A total of 123 patients with PTC who were subjected to conventional open total thyroidectomy served as the control group. The health-related quality of life and cosmetic and satisfaction outcomes were assessed postoperatively.
Results: The mean operation time was significantly increased in the experimental group. The physiological functions and social functions in the two groups were remarkably augmented after 6 months of surgery. However, there was no significant difference in the scores of speech and taste between the two groups at the indicated time of 1 month and 6 months. In addition, the scores for appearance, satisfaction with appearance, role-physical, bodily pain, and general health in the experimental group were better than those in the control group at 1 month and 6 months after surgery.
Conclusion: The single-port access transaxillary totally endoscopic thyroidectomy is safe and feasible for the treatment of patients with PTC. The subjects who underwent this technique have a good perception of their general state of health and are likely to participate in social activities. It is worthy of being clinically used for patients with PTC.
Keywords: total thyroidectomy, transaxillary approach, papillary thyroid carcinoma, quality of life
Introduction
Papillary thyroid carcinoma (PTC) is the most common malignancy of the endocrine system, accounting for ~80% of all thyroid malignancies.1 PTC is ranked the fifth leading malignancy in females and has a favorable prognosis in most cases.2 Conventional open thyroidectomy has been exercised worldwide for the treatment of endocrine neck surgery with low morbidity and mortality.3 The first endoscopic thyroidectomy was conducted by Huscher et al4 in 1997. With the improvement in minimally invasive surgery, various types of endoscopic thyroidectomy evolved considerably over the past 20 years. The newly developed endoscopic thyroidectomy has been demonstrated to achieve good results and advantages.5,6 The emergence of endoscopic thyroidectomy technologies provides a promising approach for the treatment of neck diseases. The recently identified endoscopic operative methods, such as axillary,7 breast,8 and anterior chest approaches,9 were successfully applied to thyroidectomy by many surgeons. The endoscopic thyroid surgery was initially appropriate only for benign thyroid diseases; owing to this, a complete thyroidectomy is not sufficiently conducted via endoscopic methods. However, there are several reasons for the clinical applications of endoscopic thyroidectomy: 1) the PTC has a relatively good prognosis;10 2) popularity of endoscopic thyroidectomy with reduced neck scarring and increased cosmetic effect; 3) enhancing cosmetic demand in more females; and 4) the introduction of transaxillary or axillary-breast gasless approach.11 The totally endoscopic thyroidectomy is gradually developed in thyroid malignancies. The indications for endoscopic thyroidectomy for the treatment of thyroid malignancies are increasingly expanding with the improvement in the techniques. As the experience of single-port access laparoscopic surgery is accumulating, it has been served as a less-invasive alternative to conventional laparoscopy. An increasing attention has been paid to the postoperative symptoms and functional outcomes in minimally invasive endoscopic thyroidectomy. The present study was conducted to assess the effects of single-port access transaxillary totally endoscopic thyroidectomy on the postoperative outcomes and functional parameters, including quality of life (QOL) and cosmetic result, in patients with PTC.
Patients and methods
Patients and surgical treatment
This study protocol was approved by the ethics committee of The First Affiliated Hospital of Bengbu Medical College, and the written informed consent concerning the surgical risks was obtained from all the subjects. All experiments were performed in accordance with relevant guidelines and regulations. From May 2009 to December 2012, 75 patients with PTC were subjected to single-port endoscopic thyroidectomy via axillary approach. Moreover, a total of 123 patients with PTC in the same period who were subjected to conventional open total thyroidectomy served as the control group. The enrollment inclusion criteria were set as follows: 1) underwent total thyroidectomy; 2) >18 years old; 3) no recurrence or persistent disease during the time of evaluation; 4) no history of thyroiditis, neck surgery, or radiation therapy; 5) tumor size <3 cm; 6) no evidence of lymph node metastasis or local invasion on preoperative ultrasonography; and 7) underwent computed tomography and physical examination. The exclusion criteria were preoperative evidence of nodal disease or lymph node dissection of any lateral compartment during the initial operative intervention, distant metastasis, concomitant lateral neck dissection, and recurrent laryngeal nerve, and patients lost within 1 year of follow-up. The summary of patient’s characteristics is listed in Table 1. All surgical procedures were carried out by one group of surgeons, and all clinicopathological data for this study were collected and analyzed in the database. In addition, all patients enrolled in this study were asked to complete the evaluation of cosmetic and satisfaction outcomes with the aid of University of Washington QOL (UW-QOL) questionnaire, Patient Scar Assessment Questionnaire (PSAQ), and 36-Item Short Form Health Survey (SF-36) questionnaire. The single-port endoscopic thyroidectomy via axillary approach was performed as previously reported.12
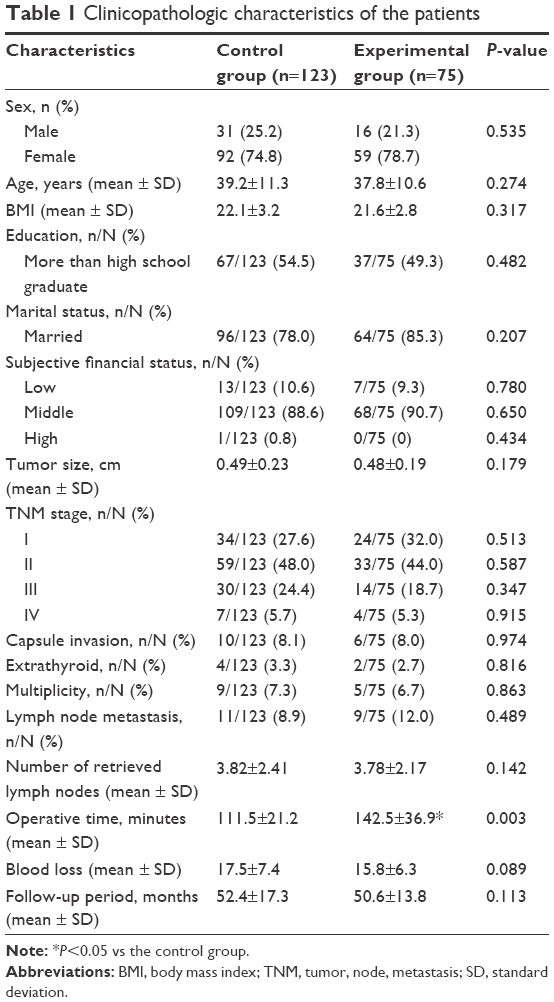 | Table 1 Clinicopathologic characteristics of the patients |
Assessment of health-related quality of life
The QOL after differentiated thyroid carcinoma therapy has been increasingly focused during long-term cancer surveillance. The health-related quality of life (HRQOL), including social, emotional, psychological, and spiritual well-being, in patients with PTC were evaluated by the UW-QOL questionnaire.13 The UW-QOL questionnaire was a commonly used, self-administered, multifactorial tool to assess the HRQOL of patients with head and neck cancer. The physiological functions, including chewing, swallowing, speech, taste, saliva, and appearance, were calculated as the average of six domain scores. The social functions, including anxiety, mood, pain, activity, recreation, and shoulder function, were also computed as the average of six domain scores. The average of 12 domain scores was recognized as the total composite score. The score ranged from 0 to 100; a score of 0 represented the worst QOL, and a score of 100 served as the best QOL. The assessment of HRQOL was performed after single-port access transaxillary totally endoscopic thyroidectomy.
Evaluation of cosmetic and satisfaction outcomes
Data about the cosmetic result and the overall satisfaction were collected and evaluated by the PSAQ and SF-36 questionnaire, respectively, as previously described.14 The PSAQ was a method to measure the perception of scarring in each patient, which involved four subscales: scar appearance, consciousness, satisfaction with scar appearance, and satisfaction with scar symptoms. A lower PSAQ score represented a better outcome. The SF-36 questionnaire was used to assess the burden of surgery. The SF-36 questionnaire was designed to be a multipurpose, short-form health survey in the evaluation of patient’s QOL, and it comprised eight subscales such as physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. A higher score reflected a better outcome.
Statistical analysis
All data about continuous variables were expressed as mean ± SD. The Kolmogorov–Smirnov test was used to check the data distribution normality. All the domains, items, and factors in the UW-QOL questionnaire, PSAQ, and SF-36 questionnaire were made by the Mann–Whitney U-test. The test for categorical variables was done by the chi-square test, and the small-cell variables were compared by the Fisher’s exact test. All statistical analyses were conducted with SPSS 19.0.1 software (IBM Corporation, Armonk, NY, USA). A value of P<0.05 was considered statistically significant.
Results
Clinicopathologic characteristics of the patients in the two groups
The clinicopathologic characteristics of two groups are summarized in Table 1. All patients confirmed to diagnose to PTC (PTC) by the final histology report. Seventy-five patients who matched the inclusion criteria successfully underwent endoscopic thyroidectomy via the axillary approach, and 123 patients with PTC received conventional open total thyroidectomy therapy. They all completed the questionnaire. No patient had to be subjected to a conventional approach. The baseline clinical data and demographics were similar in the two groups. There were no statistically significant differences between the two groups in sex, age, body mass index (BMI), education, marital status, tumor size, tumor, node, metastasis (TNM) stage, capsule invasion, extrathyroid, multiplicity, lymph node metastasis and the number of retrieved lymph nodes. However, the mean operation time was significantly increased in the experimental group.
QOL after single-port access endoscopic thyroidectomy via axillary approach
As shown in Table 2, the physiological functions, including chewing, swallowing, saliva, and appearance, were obviously increased after 6 months of surgery in comparison with after 1 month of surgery in both the control group and experimental group. The social functions, including activity, anxiety, mood, pain, recreation, and shoulder function, were also remarkably augmented after 6 months of surgery in the two groups. However, there was no significant difference in the scores of speech and taste between the two groups in the indicated time of 1 month and 6 months. It is interesting that the mean scores of appearance and physical composite score were significantly higher in the experimental group than those in the control group at the same period of 1 month and 6 months postsurgery.
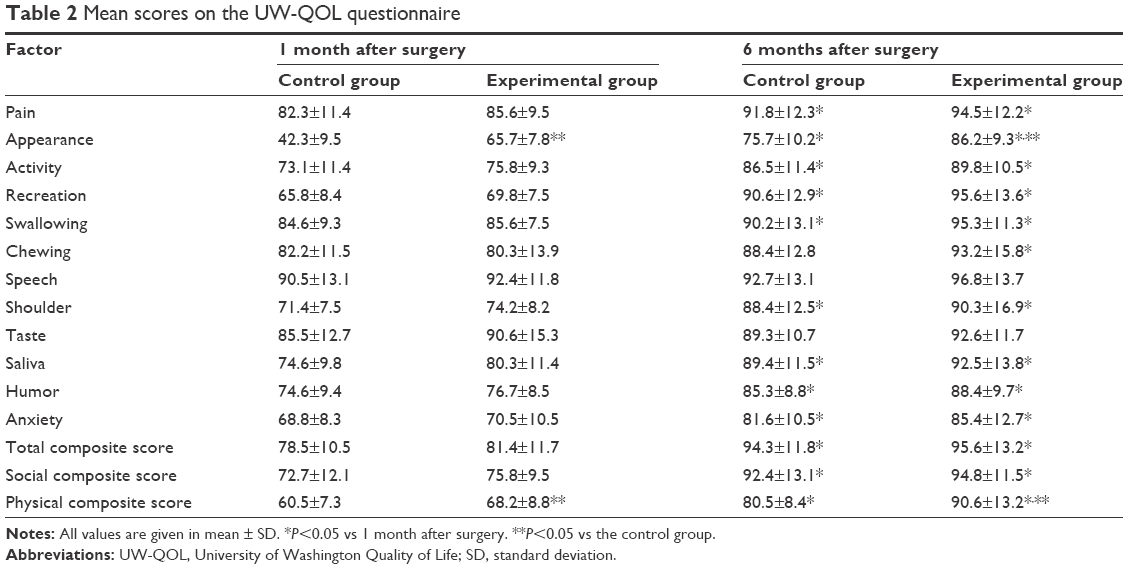 | Table 2 Mean scores on the UW-QOL questionnaire |
Cosmetic result and overall satisfaction after single-port access endoscopic thyroidectomy via axillary approach
As indicated in Table 3, with regard to PASQ, compared with after 1 month of surgery, the appearance, consciousness, satisfaction with appearance, and satisfaction with symptoms were significantly decreased after 6 months of surgery in the two groups. The scores for the SF-36 domains of physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health were significantly higher after 6 months of surgery in comparison with after 1 month of surgery in both groups. In addition, the scores for appearance, satisfaction with appearance, role-physical, bodily pain, and general health were better in the experimental group than in the control group after 1 month or 6 months of surgery.
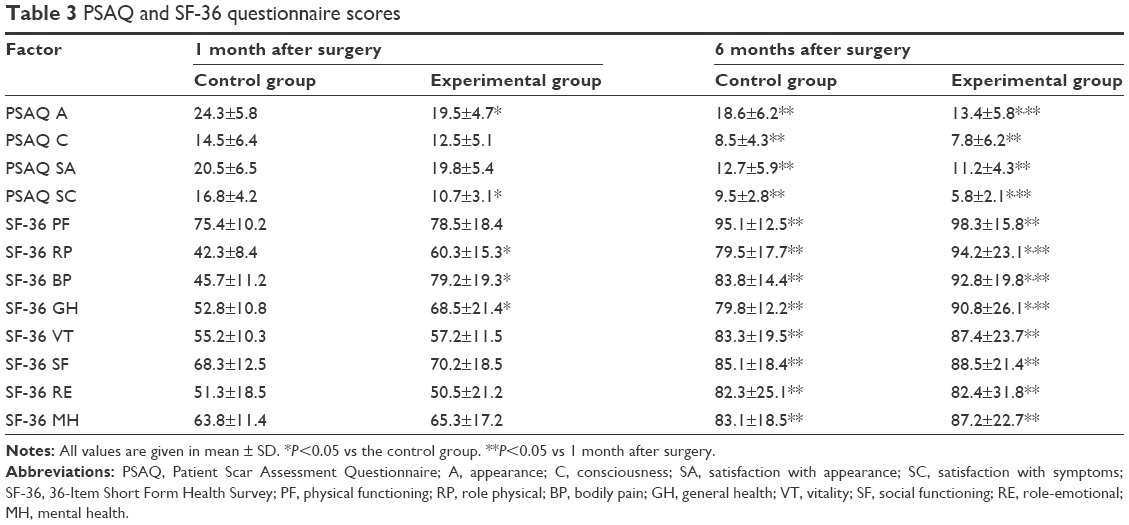 | Table 3 PSAQ and SF-36 questionnaire scores |
Operative outcomes and postoperative complications
The postoperative complications included transient vocal cord palsy, bucking, paresthesia, bleeding, seroma, and infection, each of which was treated with conservative care and resolved within 6 months. A total of three cases of transient vocal cord palsy, three cases of bucking, two cases of bleeding, two cases of seroma, and one case of infection were observed in the control group. Alternatively, two cases of transient vocal cord palsy, one case of bucking, two cases of paresthesia, three cases of bleeding, one case of seroma, and two cases of infection occurred in the experimental group. The postoperative complications showed no significant differences between the two groups.
Discussion
A number of studies have indicated the exact role of transaxillary endoscopic thyroidectomy in thyroid diseases.15,16 The transaxillary endoscopic thyroidectomy is usually applied to patients with differentiated thyroid cancer who had no invasion to peripheral structure or lateral lymph node metastasis.17 With the improvements in transaxillary endoscopic thyroidectomy, the indications for transaxillary endoscopic thyroidectomy have been extended to minimal metastatic thyroid cancer. A single-port access transaxillary totally endoscopic thyroidectomy has been employed as an important approach in thyroid diseases.12 The present study confirmed that the single-port access transaxillary totally endoscopic thyroidectomy can achieve good physiological functions and favorable social functions in patients with PTC.
With the development in surgical techniques and accumulation in surgical experiences, the feasibility and safety of endoscopic thyroidectomy have been growing in the treatment of thyroid diseases.18,19 The incidence rate of thyroid tumors is recently increasing in people, especially in young women.20 The therapeutic effects of the thyroid tumors are not only focused but also the patients are increasingly interested in the cosmetic satisfaction and postoperative QOL. Although the technical limitations of endoscopic thyroidectomy have been reviewed in large series of patients, the newly developed endoscopic operative methods, including the transaxillary or axillary-breast gasless approach, the bilateral axillary-breast approach, the postauricular and axillary approach, the facelift gasless approach, and the infraclavicular approach, were introduced to clinical therapy of thyroid disease.21 Among them, the transaxillary approach is one of the most frequently used. A single-port access transaxillary totally endoscopic thyroidectomy seems to be safe and feasible in benign thyroid tumors.12 It is accepted that the PTC has a relatively favorable prognosis with a 10-year survival exceeding 90%.22 A host of papers have reported that the total endoscopic thyroidectomy via a transaxillary approach can be applied to PTC therapy.23 In the present study, we introduced the single-port access transaxillary totally endoscopic thyroidectomy to PTC surgery. There were no statistically significant differences between the two groups in sex, age, BMI, education, marital status, tumor size, TNM stage, capsule invasion, extrathyroid, multiplicity, lymph node metastasis, and the number of retrieved lymph nodes. However, the mean operation time was significantly increased in the group of single-port access transaxillary totally endoscopic thyroidectomy. This may be attributed to two reasons: 1) the control of meticulous bleeding and lymph node dissection may require longer operation times without using drains and 2) most surgeries were conducted with the aid of unskilled assistants. Meanwhile, the longer operation time may be positively correlated with the increased postoperative complications and morbidity from general anesthesia. Although the longer operation time was one of the disadvantages of this technique, it can be decreased with more surgical experience.6,24
The UW-QOL questionnaire is usually used to assess the HRQOL in patients with head and neck cancer.25 The HRQOL assessments are frequently performed in patients with differentiated thyroid carcinoma. The HRQOL is verified to be worse than that of the healthy population, despite the excellent prognosis of differentiated thyroid carcinoma.26 Compared with conventional thyroidectomy, the higher HRQOL scores are found in robotic thyroidectomy treatment of PTC.23 A study showed that psychological problems, memory loss, and migraine headaches occurred in 518 thyroid cancer survivors who underwent thyroidectomy.27 Thus, both survival rate and good HRQOL should be preserved in the therapy of thyroid cancer. In the present study, we found that the physiological functions and social functions in the two groups were remarkably augmented after 6 months of surgery. However, there was no significant difference in the scores of speech and taste between the two groups in the indicated time of 1 month and 6 months. It is interesting that the mean scores of appearance and physical composite score were significantly higher in the experimental group than those in the control group at the same period of 1 month and 6 months postsurgery. These results indicated that single-port access transaxillary totally endoscopic thyroidectomy is helpful for recovery of social, emotional, psychological, and spiritual well-being in subjects with PTC.
The PSAQ is specifically designed to evaluate the scar.28 With regard to PASQ, compared with after 1 month of surgery, the appearance, consciousness, satisfaction with appearance, and satisfaction with symptoms were significantly decreased after 6 months of surgery in the two groups. A single-port access transaxillary totally endoscopic thyroidectomy exhibited a favored appearance and satisfaction with scar appearance scores in patients with PTC, because the axillary skin incision was made in the border of the pectoralis major muscle with no exposure to natural skin folds.
Scores for the SF-36 domains of physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health were significantly higher after 6 months of surgery in comparison with those after 1 month of surgery in both the two groups. In addition, the scores for appearance, satisfaction with appearance, role physical, bodily pain, and general health in the experimental group were better than those in the control group after 1 month or 6 months of surgery. These results further suggested that the patients who underwent single-port access transaxillary totally endoscopic thyroidectomy were satisfied with their scars and had a better perception of their general state of health and were likely to participate in social activities. The endoscopic thyroidectomy via remote access has been suggested to be cosmetic, but it is not still recognized as minimally invasive due to adequate exposure of the lesion in the surgery. The three ports access the developed endoscopic thyroidectomy based on the previous endoscopic thyroidectomy, and it was separately located on the thorax or breasts with formation of three subcutaneous tunnels within the anterior neck. A single-incision endoscopic thyroidectomy was developed on the basis of multiple-incision techniques and was designed to further improve the cosmetic results and obtain minimally invasive values. In our present study, we dissected a smaller and more hidden area of the subcutaneous tissue with the aid of a single tunnel with the incision placed below the armpit with fewer invasions and less pain after operation. It neatly realized the aims of minimal invasion and improvement in postoperative functional outcomes, including cosmesis and postoperative QOL.
Conclusion
We established the feasibility, safety, and favorable surgical outcomes of single-port access transaxillary totally endoscopic thyroidectomy for treatment of patients with PTC. The developing less invasive instruments and surgical techniques of single-port access transaxillary totally endoscopic thyroidectomy have high cosmetic satisfaction with neck appearance, reduction in injury to the anterior neck tissue. The subjects who underwent this technique had a good perception of their general state of health and were likely to participate in social activities. A single-port access transaxillary totally endoscopic thyroidectomy shows not only the improvement in several incisions but also the perfect combination of cosmetic results and minimally invasive surgery in the field of thyroid surgery.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Balta AZ, Filiz AI, Kurt Y, Sucullu I, Yucel E, Akin ML. Prognostic value of oncoprotein expressions in thyroid papillary carcinoma. Med Oncol. 2012;29(2):734–741. | ||
Hung W, Sarlis NJ. Current controversies in the management of pediatric patients with well-differentiated nonmedullary thyroid cancer: a review. Thyroid. 2002;12(8):683–702. | ||
Bae DS, Koo do H, Choi JY, Kim E, Lee KE, Youn YK. Current status of robotic thyroid surgery in South Korea: a web-based survey. World J Surg. 2014;38(10):2632–2639. | ||
Huscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997;11(8):877. | ||
Duh QY. Presidential address: minimally invasive endocrine surgery – standard of treatment or hype? Surgery. 2003;134(6):849–857. | ||
Lee J, Yun JH, Nam KH, Soh EY, Chung WY. The learning curve for robotic thyroidectomy: a multicenter study. Ann Surg Oncol. 2011;18(1):226–232. | ||
Kim HS, Kim SH, Kim JH, Kim BT, Lee KH. Multifocal hot spots demonstrated by whole-body 131I scintigraphy and SPECT/CT after transaxillary endoscopic thyroidectomy. Clin Nucl Med. 2015;40(3):260–262. | ||
Park KN, Cho SH, Lee SW. Nationwide multicenter survey for current status of endoscopic thyroidectomy in Korea. Clin Exp Otorhinolaryngol. 2015;8(2):149–154. | ||
Wang X, Yang W, Sun Y. Clinical application of endoscopic thyroidectomy via an anterior chest wall approach. Surg Laparosc Endosc Percutan Tech. 2014;24(3):254–258. | ||
Jovanovic L, Delahunt B, McIver B, et al. Distinct genetic changes characterise multifocality and diverse histological subtypes in papillary thyroid carcinoma. Pathology. 2010;42(6):524–533. | ||
Kiong KL, Iyer NG, Skanthakumar T, et al. Transaxillary thyroidectomies: a comparative learning experience of robotic vs endoscopic thyroidectomies. Otolaryngol Head Neck Surg. 2015;152(5):820–826. | ||
Fan Y, Wu SD, Kong J. Single-port access transaxillary totally endoscopic thyroidectomy: a new approach for minimally invasive thyroid operation. J Laparoendosc Adv Surg Tech A. 2011;21(3):243–247. | ||
Rogers SN, Rajlawat B, Goru J, Lowe D, Humphris GM. Comparison of the domains of anxiety and mood of the University of Washington Head and Neck Cancer Questionnaire (UW-QOL V4) with the CES-D and HADS. Head Neck. 2006;28(8):697–704. | ||
Materazzi G, Fregoli L, Manzini G, Baggiani A, Miccoli M, Miccoli P. Cosmetic result and overall satisfaction after minimally invasive video-assisted thyroidectomy (MIVAT) versus robot-assisted transaxillary thyroidectomy (RATT): a prospective randomized study. World J Surg. 2014;38(6):1282–1288. | ||
Kwak HY, Kim SH, Chae BJ, Song BJ, Jung SS, Bae JS. Learning curve for gasless endoscopic thyroidectomy using the trans-axillary approach: CUSUM analysis of a single surgeon’s experience. Int J Surg. 2014;12(12):1273–1277. | ||
Hakim Darail NA, Lee SH, Kang SW, Jeong JJ, Nam KH, Chung WY. Gasless transaxillary endoscopic thyroidectomy: a decade on. Surg Laparosc Endosc Percutan Tech. 2014;24(6):e211–e215. | ||
Lee J, Yun JH, Nam KH, Choi UJ, Chung WY, Soh EY. Perioperative clinical outcomes after robotic thyroidectomy for thyroid carcinoma: a multicenter study. Surg Endosc. 2011;25(3):906–912. | ||
Mercante G, Battaglia P, Manciocco V, Cristalli G, Pellini R, Spriano G. Three-dimensional minimally invasive video-assisted thyroidectomy: preliminary report. J Exp Clin Cancer Res. 2013;32:78. | ||
Wang CC, Wu CH. Non-recurrent inferior laryngeal nerve identification during robotic thyroidectomy. J Laryngol Otol. 2014;128(2):199–202. | ||
Lee DY, Oh KH, Cho JG, et al. The benefits and risks of prophylactic central neck dissection for papillary thyroid carcinoma: prospective cohort study. Int J Endocrinol. 2015;2015:6. [Article ID 571480]. | ||
Dhepnorrarat RC, Witterick IJ. New technologies in thyroid cancer surgery. Oral Oncol. 2013;49(7):659–664. | ||
Chow SM, Law SC, Chan JK, Au SK, Yau S, Lau WH. Papillary microcarcinoma of the thyroid-prognostic significance of lymph node metastasis and multifocality. Cancer. 2003;98(1):31–40. | ||
Lee DY, Lim S, Kang SH, et al. A prospective 1-year comparative study of transaxillary total thyroidectomy regarding functional outcomes: is it really promising? Surg Endosc. 2016;30(4):1599–1606. | ||
Park JH, Lee J, Hakim NA, et al. Robotic thyroidectomy learning curve for beginning surgeons with little or no experience of endoscopic surgery. Head Neck. 2015;37(12):1705–1711. | ||
Rogers SN, Hogg ES, Cheung WK, Lai LK, Jassal P, Lowe D. The use of health related quality of life data to produce information sheets for patients with head and neck cancer. Ann R Coll Surg Engl. 2015;97(5):359–363. | ||
Gallop K, Kerr C, Simmons S, McIver B, Cohen EE. A qualitative evaluation of the validity of published health utilities and generic health utility measures for capturing health-related quality of life (HRQL) impact of differentiated thyroid cancer (DTC) at different treatment phases. Qual Life Res. 2015;24(2):325–338. | ||
Taieb D, Sebag F, Cherenko M, et al. Quality of life changes and clinical outcomes in thyroid cancer patients undergoing radioiodine remnant ablation (RRA) with recombinant human TSH (rhTSH): a randomized controlled study. Clin Endocrinol (Oxf). 2009;71(1):115–123. | ||
McCarus SD. Scar assessment for patients undergoing minimal invasive hysterectomy. Surg Technol Int. 2014;25:150–156. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.