")
Back to Journals » Clinical Interventions in Aging » Volume 17
Quality Improvement in Delirium Health Literacy in Older Adult Patients and Their Caregivers Attending a Geriatric Clinic
Authors Azhar G, Sharma S , Lau O, Alkharisi B, Anandam A, Isa S, Mendiratta P, Pangle AK , Coker K, Wei J
Received 1 September 2022
Accepted for publication 6 December 2022
Published 28 December 2022 Volume 2022:17 Pages 1901—1906
DOI https://doi.org/10.2147/CIA.S388325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Gohar Azhar,1 Shakshi Sharma,1 Onna Lau,1 Bader Alkharisi,1 Anil Anandam,1 Sakiru Isa,2 Priya Mendiratta,1 Amanda K Pangle,1 Karen Coker,1 Jeanne Wei1
1Department of Geriatrics, Donald W. Reynolds Institute of Aging, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 2Division of Cardiovascular Diseases, University of Tennessee Health Science Center, Memphis, TN, USA
Correspondence: Gohar Azhar, Email [email protected]
Background: Delirium is a common medical condition that is highly prevalent in older adults who are at increased risk for its development with any illness, post-surgery or during hospitalization. The purpose of our study was to evaluate the health literacy of older adult patients and their caregivers about delirium, offer a brief educational intervention, and reevaluate their knowledge post intervention.
Materials and Methods: We conducted a quality improvement project, focused on delirium health literacy in older adult patients ≥ 60 years and their caregivers. Delirium knowledge of participants was evaluated in a pre-education survey after which they were given a delirium education booklet to read. A post-education delirium survey was conducted within 2– 3 weeks of the educational intervention. Chi-square test was used to analyze the knowledge base of older adults.
Results: The study population consisted of a total of 70 older adults who participated in pre-education (n=35) and post-education (n=35) surveys. Older adult patients and their caregivers had significant knowledge gaps about the potential causes or etiologies, risk factors, symptomatology, and prevention of delirium in the pre-education survey. After the educational intervention, in the post-education survey, there were overall improvements in knowledge base of older adults in differentiating delirium with dementia (43% vs 94%, p< 0.01) recognizing signs and symptoms (77% vs 94%, p< 0.05), complications (76% vs 100%, p< 0.01) and identifying the etiological factors associated with delirium.
Conclusion: The quality improvement project demonstrated that older adults and caregivers have significant knowledge deficits about the common condition of delirium. This study also demonstrated that older adults were able to improve their health literacy regarding delirium after the intervention. Appropriate education on delirium for patients and caregivers might help in earlier identification, prevention, and better overall management of delirium.
Keywords: delirium, education, aging, healthcare
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Colombo has been published for this article.
Introduction
Delirium is an acute medical condition characterized by sudden disruption in attention, cognition, and behavior.1–4, It is identified by clinical diagnosis, and there is no laboratory test or any diagnostic kit available that can help in its diagnosis.5,6 Delirium is frequently observed in older patients who are hospitalized and is associated missed or delayed diagnosis resulting in extended length of hospitalization, development of complications with decline in physical and cognitive function, loss of independence, and increased morbidity and mortality.2–4,6
With the exponential increase in the population of older adults globally, delirium prevention has become extremely pertinent. In spite of it being very common, most often clinicians fail to identify delirium at the onset, which results in poor outcomes.6–8 Older age and cognitive impairment are risk factors for delirium.9–11 Critically ill older patients are at a higher risk of developing delirium, including those with infections, electrolyte disturbances, dehydration, and those taking centrally acting medicines (such as opioids, benzodiazepines, and hypnotics). The rate of occurrence of delirium is almost 58–75% in hospitalized older adults.12,13 In US, more than 2.6 million older adults (>65 years) develop delirium each year and cost the healthcare industry approximately $164 billion.5,8 There are different delirium prevention programs initiated by multiple organizations to apprise people about the subject. Despite growing awareness, there is insufficient knowledge among older adults and inadequate education and training of students and health-care professionals on the topic of delirium.14
Currently, the best way of reducing the incidence of delirium is through prevention. Educating people of all age groups about delirium could help minimize delirium-associated complications. Additionally, in hospitals educating older patients and their families about the symptoms and risk factors associated with delirium can help in its timely detection and effective management.15,16 We, at the Reynolds Institute on Aging, conducted a quality improvement project to educate older adults and their caregivers about delirium. Our overall goal was to determine gaps in delirium health literacy among older adults and caregivers and to improve the knowledge gaps through targeted education on delirium.
Materials and Methods
Study Design
We used the Plan Do Study Act (PDSA) design to collect data.17 The study team comprised geriatric medicine fellows, graduate students, post-graduate students, and faculty members. The study population included geriatric patients and their caregivers seen at the Thomas and Lyon Longevity Clinic. Inclusion criteria for the survey were older adults ≥ age 60 who were either patients or caregivers and had the ability to provide informed consent and understand the survey questions. All races, ethnicities, and genders were included. Older adults were excluded if they had cognitive impairment, visual, language, or comprehension problems. Caregivers were allowed to participate in the study if patients did not meet the inclusion/exclusion criteria.
A 22-question, semi-structured, anonymous survey that addressed all relevant information on delirium was designed for the lay public (“Supplementary Material 1”). The survey was designed by a team of experienced geriatricians and neurologists at an academic medical center who regularly provide consultation on patients with delirium and counsel patients and caregivers regarding delirium.
The survey questions were based on literature on delirium and categorized into differentiating dementia from delirium, identifying signs and symptoms of delirium, knowledge of risk factors, common etiological causes, complications, and management. Pilot testing of the survey questions was performed on a separate focus group of patients and caregivers before finalizing the survey.
The next part of PDSA was to administer the pre-education survey to all participants.
We then used the knowledge gaps identified to design an educational booklet on delirium for older adults and caregivers. The content in the booklet was based on available literature on delirium by experts in the field. The booklet covered all aspects of delirium identification, signs and symptoms of delirium, risk factors and complications associated with delirium, types of delirium, and its prevention (‘Supplementary Material 2’). After all the participants completed the pre-education survey, they were given the delirium education booklet and instructed to read it. After the educational training, the same 22 question survey was mailed to the participants with a pre-paid envelope to return the survey. Patients and caregivers were called to remind them to complete the survey and mail it back within 2–3 weeks.
All surveys were anonymous and coded as pre- and post-education. Informed consent was obtained before conducting the surveys. The quality improvement project was approved by Institutional Review Board (IRB) at University of Arkansas for Medical Sciences (UAMS) #273639.
Statistical Analysis
Data were examined/analyzed for item response rates for the sample and relative time points (pretest and posttest). Two-sided tests of response rate differences between time points were performed with proportions tests. For analysis, survey items were categorized consistently with health information that patients receive about an illness: facts and clarifications; symptoms and signs; course; treatment; risk factors and causes; and complications and prognosis.
Frequencies and percentages of all survey item choices and of correct and incorrect responses were performed. The percentage of correct responses at pre-education and post-education time points were compared using the chi-square test or, for sparse expected cell counts, the exact chi-square test. Two-sided hypotheses were tested at a significance level of 0.05. Analysis was conducted using SAS 9.4.
Results
Demographics
There were 70 participants aged 60 years and older, out of which 35 participated in pre-education and 35 in post-education survey. Both patients and their caregivers participated in this study.
Knowledge Survey Response Rates
For both time points considered together, all items had response rates greater than 90%, with the lowest being 93%. Compared to posttest, pretest surveys, not surprisingly for knowledge-based items, had lower response rates. Still, all but two had >90% responses, with the two lowest having 86% and 89% responses. The posttest response rates all exceeded 90%.
Pre-Education Knowledge of Older Adults
In pre-education survey only 43% of older adults could differentiate delirium from dementia and depression (Figure 1). When asked about onset of delirium, duration and signs and symptoms, more than 60% of all survey participants responded correctly. The participants were also found to be knowledgeable about the management (85%) and treatment (67%) of delirium. The survey participants also appeared to be somewhat informed about potential etiological causes of delirium such as Covid-19 (77%), respiratory tract infection (74%), chemotherapy (40%), sodium imbalance (47%) and use of over-the-counter medications such as Tylenol PM (58%). When asked about the life-threatening illness and falls and other complications of delirium more than 50% of participants answered correctly.
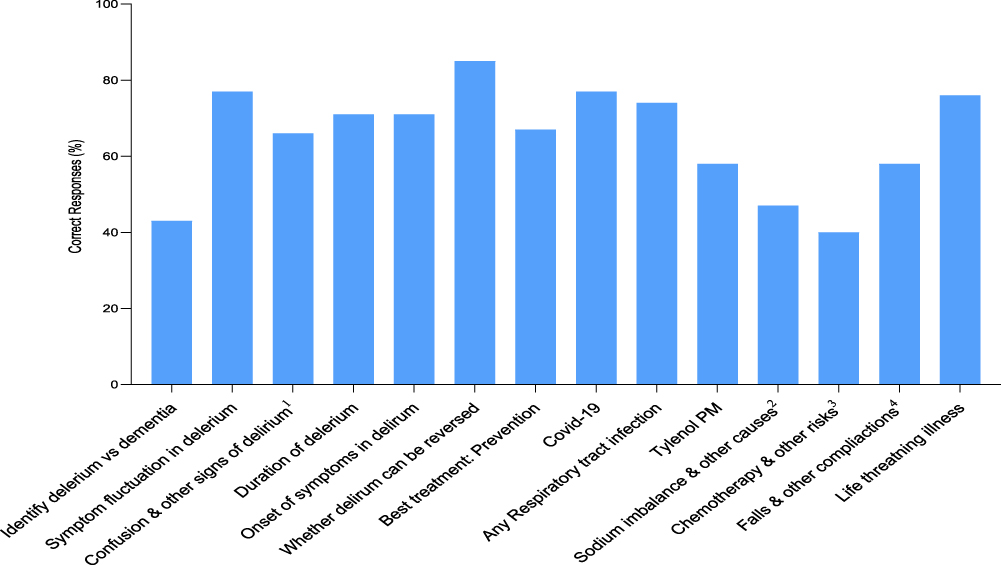 |
Figure 1 Delirium knowledge of adults aged 60+ years at pretest: symptoms, signs, treatment, risk factors and etiological causes. aIncludes sleepiness, trouble focusing, restlessness or agitation, hallucinations, becomes angry easily. bSodium imbalances due to pneumonia, dehydration, constipation, fever. cIncludes dementia, having a urinary tract infection, alcohol use or withdrawal, hearing loss, age over 70. dIncludes harm to self or others, death, longer stay in hospital. |
Knowledge Improvement Post Education
Overall, there were significant improvements in older adults’ delirium health literacy from pre-education to post-education after reading the delirium booklet. Older adults were better informed about differentiating delirium from depression and dementia post education (43% vs 94%, p<0.01); in recognizing signs and symptoms (77% vs 94%, p<0.05) (Figure 2). Majority of older adults had greater understanding about the etiological factors associated with delirium such as sodium imbalance (47% vs 80%, p<0.01), and chemotherapy (40% vs 77%, p<0.01) after reading the booklet. Education also improved their knowledge about serious and life-threatening complications associated with delirium (76% vs 100%, exact p<0.01).
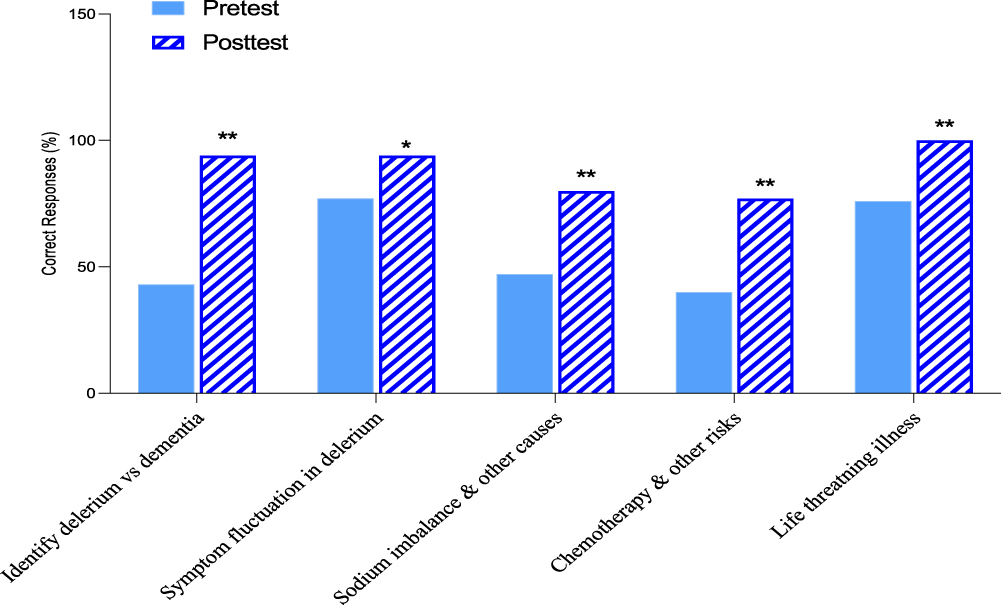 |
Figure 2 Pretest vs posttest delirium knowledge of adults aged 60+ years *P<0.05 for the difference in pretest and posttest for the 60+ years age group; **P<0.01. |
Discussion
This is one of the first studies discussing improvement in health literacy of older adult patients and caregivers after education on delirium. The findings from this study revealed significant knowledge gaps in majority of older adults about many aspects of delirium. Acute, hyperactive, or mixed delirium is often confused with dementia as they both share some common symptoms and it often becomes difficult for health-care professionals to recognize delirium in patients suffering from dementia.18 We see a significant increase in the participants' knowledge about the difference between delirium, dementia, and depression in the post-education survey as compared to the pre-education survey.
Older hospitalized adults (≥60 years) are at higher risk of developing delirium during or after their stay in the hospital.6,19 Longer hospital stays are one of the most common reasons that leads to the development of delirium in older patients as they tend to feel alone and isolated in hospitals. The treatment of delirium is also expensive, and failure in its timely recognition can result in physical, mental, and emotional stress and increase the probability of death.20,21 In hospitals, only one-third of delirium cases can be considered preventable because patients arrive with acute conditions superimposed on multimorbidity that is not often preventable. It is predicted that in the near future the estimated cost of care for delirium could exhaust the resources of health-care systems.8,21–23 Not incorporating delirium awareness programs could result in a lack of knowledge about this disease and complicate its clinical outcomes.9 Helping older patients and caregivers understand the risk factors associated with this disease can also aid in its timely management. Patients and their caregivers and family members could all play a major role in prevention of this disease.16,17 Our study is unique because we focused on educating older patients and caregivers in the outpatient setting and helped them to become more knowledgeable about this illness. Educating caregivers is also very important as they can assist with earlier identification of delirium as well as provide comfort, care, and support to their loved ones suffering from delirium.24 In the present study, we found that after education both patients and caregivers became better acquainted with symptoms and treatment of delirium. A number of studies cited in the literature, have demonstrated that educational intervention significantly increased the knowledge of nurses and caregivers about delirium in hospitals.24–26
Participants, especially the older ones, were quite unaware of the risk factors associated with delirium. Providing simple yet effective information in a manner that is easily understood can certainly make a big difference. Education will result in greater prevention of delerium with improved health outcomes and a potentially better quality of life.
It was encouraging to note that, the majority of older adults in our study seemed to be interested and were willing to learn more about delirium and its associated risk factors and treatment. This was reflected in their considerably improved performance in the post-education survey. Our findings are in line with previous results indicating positive outcomes from educating patients and nurses with improvement in their knowledge about delirium.27,28 It is important to expand this approach of educating patients and caregivers nationwide, for earlier identification, prevention, and better management of delirium.
Limitations
This was a relatively small, single-site study in rural Arkansas. In addition, we cannot exclude the possibility that high rate of correct responses by the older adults could be due to random selection. Nevertheless, there were significant differences between pre- and post-educational responses.
Conclusion
This study reveals the importance of educating patients and caregivers about delirium. Addressing risk factors associated with delirium can help in reducing the incidence of delirium and improve functioning in older patients and caregivers. Better awareness and management of delirium will reduce delirium-related complications including falls, mobility impairment, decreased cognition, and hospital length of stay. We observed a significant improvement in knowledge scale of older adults about delirium after education. Our study also provides evidence of the older adult’s interest in being better informed about their health, and in this case about delirium. This will hopefully encourage health providers to educate the older adult population and engage them in their own care.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Egberts A, Moreno-Gonzalez R, Alan H, Ziere G, Mattace Raso F. Anticholinergic drug burden and delirium: a systematic review. J Am Med Dir Assoc. 2021;22(1):65–73.
2. Sinvani L, Kozikowsk A, Pekmezaris R, Akerman M, Wolf-Klein G. Delirium: a survey of healthcare professionals’ knowledge, beliefs, and practices. J Am Geriatr Soc. 2016;2016(64):297–303. doi:10.1111/jgs.14544
3. Marcantonio ER. Postoperative delirium: a 76-year-old woman with delirium following surgery. JAMA. 2012;308(1):73–81. doi:10.1001/jama.2012.6857
4. Inouye SK, Rushing JT, Foreman MD, Palmer RM, Pompei P. Does delirium contribute to poor hospital outcomes? J Gen Intern Med. 1998;13:234–242. doi:10.1046/j.1525-1497.1998.00073.x
5. Tripp BA, Dillon ST, Yuan M, et al. Targeted metabolomics analysis of postoperative delirium. Sci Rep. 2021;11:1521. doi:10.1038/s41598-020-80412-z
6. Esther OH, Fong TG, Hshieh TT, Inouye SK. Delirium in older persons: advances in diagnosis and treatment. JAMA. 2017;318(12):1161–1174. doi:10.1001/jama.2017.12067
7. Sabzwari S, Kumar D, Bhanji S, Sheerani M, Azhar G. Proportion, predictors and outcomes of delirium at a tertiary care hospital in Karachi, Pakistan. Ageing Int. 2014;39:33–45. doi:10.1007/s12126-012-9152-5
8. Kalish VB, Gillham JE, Unwin BK. Delirium in older persons: evaluation and management. Am Fam Physician. 2014;90(3):150–158.
9. Grealish L, Todd J, Krug M, Teodorczuk A. Education for delirium prevention: knowing, meaning and doing. Nurse Educ Pract. 2019;40:102622. doi:10.1016/j.nepr.2019.102622
10. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. doi:10.1016/S0140-6736(13)60688-1
11. Fong TG, Davis D, Growdon ME, Albuquerque A, Inouye SK. The interface between delirium and dementia in elderly adults. Lancet Neurol. 2015;14(8):823–832. doi:10.1016/S1474-4422(15)00101-5
12. Li X, Zhang L, Gong F, Yuhang A. Incidence and risk factors for delirium in older patients following intensive care unit admission: a prospective observational study. J Nurs Res. 2020;28(4):101. doi:10.1097/jnr.0000000000000384
13. Lin WL, Chen YF, Wang J. Factors associated with the development of delirium in elderly patients in intensive care units. J Nurs Res. 2015;23(4):322–329. doi:10.1097/JNR.0000000000000082
14. Yanamadala M, Wieland D, Heflin MT. Educational interventions to improve recognition of delirium: a systematic review. J Am Geriatr Soc. 2013;61(11):1983–1993. doi:10.1111/jgs.12522
15. Carbone MK, Gugliucci MR. Delirium and the family caregiver: the need for evidence-based education interventions. Geront. 2015;55(3):345–352. doi:10.1093/geront/gnu035
16. Paulson CM, Monroe T, McDougall GJ Jr, Fick DM. A family-focused delirium educational initiative with practice and research implications. Gerontol Geriatr Educ. 2016;37(1):4–11. doi:10.1080/02701960.2015.1031896
17. Morelli MS. Using the plan, do, study, act model to implement a quality improvement program in your practice. Off J Am Coll Gastroenterol. 2016;9:1220–1222. doi:10.1038/ajg.2016.321
18. Lippmann S, Perugula ML. Delirium or Dementia. Innov Clin Neurosci. 2016;13(9–10):56–57.
19. Bellelli G, Brathwaite JS, Mazzola P. Delirium: a marker of vulnerability in older people. Front Aging Neurosci. 2021;13:626127. doi:10.3389/fnagi.2021.626127
20. Marcantonio ER, Solomon CG. Delirium in hospitalized older adults. N Engl J Med. 2017;377(15):1456–1466. doi:10.1056/NEJMcp1605501
21. Dharmarajan K, Swami S, Gou RY, Jones RN, Inouye SK. Pathway from delirium to death: potential in-hospital mediators of excess mortality. J Am Geriatr Soc. 2017;65(5):1026–1033. doi:10.1111/jgs.14743
22. Deeken F, Sánchez A, Rapp MA, et al. Outcomes of a delirium prevention program in older persons after elective surgery: a stepped-wedge cluster randomized clinical trial. JAMA Surg. 2022;157(2):216370. doi:10.1001/jamasurg.2021.6370
23. Marquetand J, Bode L, Fuchs S, et al. Risk factors for delirium are different in the very old: a comparative one-year prospective cohort study of 5831 patients. Front Psychiatry. 2021;12:655087. doi:10.3389/fpsyt.2021.655087
24. Ewens B, Seaman K, Whitehead L. A delirium prevalence audit and a pre and post evaluation of an interprofessional education intervention to increase staff knowledge about delirium in older adults. BMC Nurs. 2021;20:202. doi:10.1186/s12912-021-00692-2
25. Racine AM, Tommet D, D’Aquila ML. Machine learning to develop and internally validate a predictive model for post-operative delirium in a prospective, observational clinical cohort study of older surgical patients. J Gen Intern Med. 2021;36:265–273. doi:10.1007/s11606-020-06238-7
26. Velthuijsen V, Zwakhalen EL, Warnier R, et al. Can education improve clinical practice concerning delirium in older hospitalized patients? Results of a pre-test post-test study on an educational intervention for nursing staff. BMC Med Educ. 2018;18(1):59. doi:10.1186/s12909-018-1177-3
27. Helgesen AK, Larsen DW, Grøndahl VA. Quality of care in a nursing home as experienced by patients with dementia. J Multidiscip Healthc. 2020;15(13):1947–1955. doi:10.2147/JMDH.S285668
28. Wand AP, Thoo W, Sciuriaga H, Ting V, Baker J, Hunt GE. A multifaceted educational intervention to prevent delirium in older inpatients: a before and after study. Int J Nurs Stud. 2014;51(7):974–982.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.