")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Quality and Characteristics of 4241 Case Reports of Lactic Acidosis in Metformin Users Reported to a Large Pharmacovigilance Database
Authors Brand KMG, Schlachter J , Foch C, Boutmy E
Received 4 May 2022
Accepted for publication 11 July 2022
Published 4 November 2022 Volume 2022:18 Pages 1037—1047
DOI https://doi.org/10.2147/TCRM.S372430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Kerstin MG Brand,1 Judith Schlachter,2 Caroline Foch,3 Emmanuelle Boutmy4
1Global Medical Affairs, Merck Healthcare KGaA, Darmstadt, Germany; 2Global Patient Safety, Merck Healthcare KGaA, Darmstadt, Germany; 3Global Epidemiology, Merck Healthcare KGaA, Darmstadt, Germany; 4Global Biostatistics, Merck Healthcare KGaA, Darmstadt, Germany
Correspondence: Kerstin MG Brand, Global Medical Affairs, Merck Healthcare KGaA, F135/00_N1, Frankfurter Str. 250, Darmstadt, 64293, Germany, Tel +49 6151 72 2301, Email [email protected]
Objective: Metformin-associated lactic acidosis (MaLA) occurs rarely and is thus difficult to study. We analysed 4241 individual case safety reports of lactic acidosis (LA) that implicated metformin as a suspected drug reported to the pharmacovigilance database of Merck KGaA, Darmstadt, Germany. The primary objective was to review reports for quality and completeness of data to support diagnoses of MaLA. We also explored the correlations between reported biomarkers, and associations between biomarkers and outcomes.
Research Design and Methods: Records were analysed for completeness in supporting diagnoses of LA or metformin-associated LA (MaLA), against commonly used diagnostic criteria. Correlations between indices of exposure to metformin and biomarkers of LA and mortality were investigated.
Results: Missing data was common, especially for plasma metformin. Clinical/biomarker evidence supported a diagnosis of LA in only 33% of cases (LA subpopulation) and of MaLA in only 9% (MaLA subpopulation). The metformin plasma level correlated weakly with plasma lactate (positive) and pH (negative). About one-fifth (21.9%) of cases reported a fatal outcome. Metformin exposure (plasma level or dose) was not associated with increased mortality risk (there was a suggestion of decreased risk at higher levels of exposure to metformin). Plasma lactate was the only variable associated with increased risk of mortality. Examination of concomitant risk factors for MaLA identified renal dysfunction (including of iatrogenic origin) as a potential driver of mortality in this population.
Conclusion: Despite the high frequency of missing data, this is the largest analysis of cases of MaLA supported by measurements of circulating metformin, and lactate, and pH, to date. Plasma lactate, and not metformin dose or plasma level, appeared to be the main driver of mortality in the setting of LA or MaLA. Further research with more complete case reports is required.
Keywords: lactic acidosis, metformin, type 2 diabetes, pharmacovigilance
Introduction
Metformin-associated lactic acidosis (MaLA) is a rare but life-threatening adverse event associated with the therapeutic use of metformin for the management of type 2 diabetes. The prevalence of MaLA has been estimated at about 3–10 cases/100,000 patient-years of exposure to metformin at therapeutic doses.1–5 The contraindications to metformin are largely intended to reduce the risk of MaLA. These include settings where tissue hypoxia may occur (eg, recent myocardial infarction, shock, decompensated heart failure), where metformin excretion may be reduced, leading to its accumulation in the body (eg, severe chronic kidney disease [CKD; estimated glomerular filtration rate [eGFR] <30 mL/min/1.73m2]), or when metabolic acidosis is already present. The risk of MaLA rises steeply in cohorts with severe (but not mild-to-moderate) CKD,2,6,7 or with contraindications to metformin.8,9
MaLA is a difficult condition to study, mainly due to its rarity. For example, there were no cases of lactic acidosis in a Cochrane meta-analysis designed to study the incidence of MaLA, that included 70,490 patient-years of exposure to metformin, and 55,451 patient-years of a non-metformin control group.5 In addition, other risk factors for lactic acidosis are often present in patients hospitalized for this condition.8,10–12
Large databases may provide a more useful source of data for studying MaLA than clinical trial populations.6 Merck KGaA, Darmstadt, Germany and its predecessor companies, Aron Laboratories and Lipha, have marketed formulations of metformin since 1959.13 This company administers the most comprehensive safety database of adverse drug events associated with metformin, including lactic acidosis. In this report, we describe 4241 reports of lactic acidosis from this database, which represents the largest series of case reports of suspected MaLA analysed to date.
Research Design and Methods
Objectives
The primary objective of this study was to assess the quality of reporting of diagnoses of LA and MaLA, according to whether they included data on metabolic variables needed to diagnose LA (plasma lactate, pH) or MaLA (plasma lactate, pH, plasma metformin). We determined the proportions of cases with sufficient data to support a diagnosis of LA or MaLA, according to commonly used diagnostic criteria (LA: blood pH <7.35; plasma lactate >5 mmol/L; MaLA: as above plus plasma metformin >5 mg/L [39 µM]).14–18 These cases are further referred to as “confirmed” cases.
Additional objectives were to describe the characteristics of the population, including the metformin dose, plasma lactate, pH, GFR, comorbidities, and vital status. We studied correlations between key metabolic variables: metformin dose, plasma lactate, pH, and GFR, and the association of these parameters with mortality. Finally, we compared the prevalence of known non-metformin risk factors for LA in survivors and non-survivors.
Inclusion Criteria
All cases analysed were anonymized case reports from the Pharmacovigilance Database maintained by Merck KGaA, Darmstadt, Germany; as such, they contained all information provided by the reporter, most commonly healthcare professionals, health authorities and the published literature. Cases were reviewed here if they: (a) were initially received between January 1st, 1990 and December 31st, 2018 (cases could be followed up until 31st March 2019); (b) were retrieved using the Standard Medical Query ‘Lactic acidosis’ (broad scope); (c) reported metformin as a suspected cause of lactic acidosis and (d) were medically confirmed.
Abstraction of Data from Case Reports
The dose of metformin was as presented in the case report. No attempt was made to distinguish between immediate-release and extended/prolonged release metformin formulations, due to lack of data. If >1 plasma lactate or pH value was contained in the report, the highest and lowest value, respectively, were captured. GFR was taken directly from records, or calculated where possible using the MDRD equation applied to reported serum creatinine, gender, and age.
Vital status and the presence of concomitant treatments or comorbid conditions were as per case reports. The comorbidities that were collected were those likely to increase the risk of Type A lactic acidosis (due to hypoxia and/or hypoperfusion; shock, sepsis and infections, rhabdomyolysis, respiratory failure and asthma/bronchospasm, heart failure) or of Type B lactic acidosis (unrelated to tissue hypoxia or hypoperfusion; acute or chronic renal failure, dehydration, diarrhoea and vomiting, hepatic failure, malnutrition, poorly controlled diabetes, or HIV/AIDS).19 Concomitant medications considered were those that may have increased the risk of acidosis, rhabdomyolysis or renal impairment, or were for HIV management. Concomitant use of alcohol was also extracted.
Statistics
Descriptive statistics were used to describe key metabolic variables according to the level of exposure to metformin, and according to reported survival or mortality. Continuous variables were described through the number of non-missing observations, medians (with Q1–Q3). Categorical variables were displayed by the total number of observations and missing values, and the relative percentage by category accounting for missing values as a modality of the variable, unless specified.
Analyses were performed for all cases (the overall population) and for confirmed cases of LA (the LA subpopulation) and MaLA (the MaLA subpopulation), stratified further on the recorded metformin dosages within the permitted range in Europe (≤3000 mg/day) or consistent with metformin overdosage (>3000 mg/day). The “index of exposure” to metformin was defined as the metformin dose or metformin plasma level and referred such as in the body of the manuscript.
Spearman rank correlation coefficients (displayed with rho and 95% Confidence Intervals [CI]) were used to describe correlations between metformin dose, metformin plasma level, pH, plasma lactate and renal function. The strength of associations was determined arbitrarily as “very weak” (correlation coefficient 0–0.19); “weak” (correlation coefficient 0.20–0.39); “moderate” (correlation coefficient 0.40–0.59); “strong” (correlation coefficient 0.60–0.79); or “very strong” (correlation coefficient 0.80–1.0).
We also described the differences (with 95% CI) in proportions with and without pre-specified concomitant treatment and risk factors known to be associated to lactic acidosis between survivors and non-survivors.
Logistic regression models were used to examine the impact on the probability of death according to the metformin plasma level, the lactate plasma level and pH, further adjusted for MDRD (quantitative), age (quantitative), gender (qualitative), total drug usage (quantitative, number of different drugs used), presence of at least one risk factor (qualitative binary, yes/no) and world region of the origin of the report (qualitative). For comorbidities and co-medications, the variables were further defined as categorical variables by the number of occurrences. Odds Ratios (OR) were reported with 95% CI; goodness of fit of the models was assessed with the Hosmer-Lemeshow and likelihood ratio tests, and visual inspection of the plot of residuals.
Ethics
All case reports were anonymized and thus did not require informed consent, in line with ICH-E2B [R2] and GVP module VI. Authors had no access to de-anonymized patient-level information. Thus, the article complies with the Declaration of Helsinki and all other ethical standards, and no ethical approval was required.
Results
Quality of Data Reporting (Primary Outcome)
Missing data was encountered frequently for plasma metformin (83% of cases), plasma lactate (44%), and pH (52%) (Table 1A). Online Supplementary Figure 1 shows a “missingness map” of these parameters as well as for metformin dose and GFR. The prevalence of missing data was similar for cases reporting fatal outcome versus survival (Table 1A).
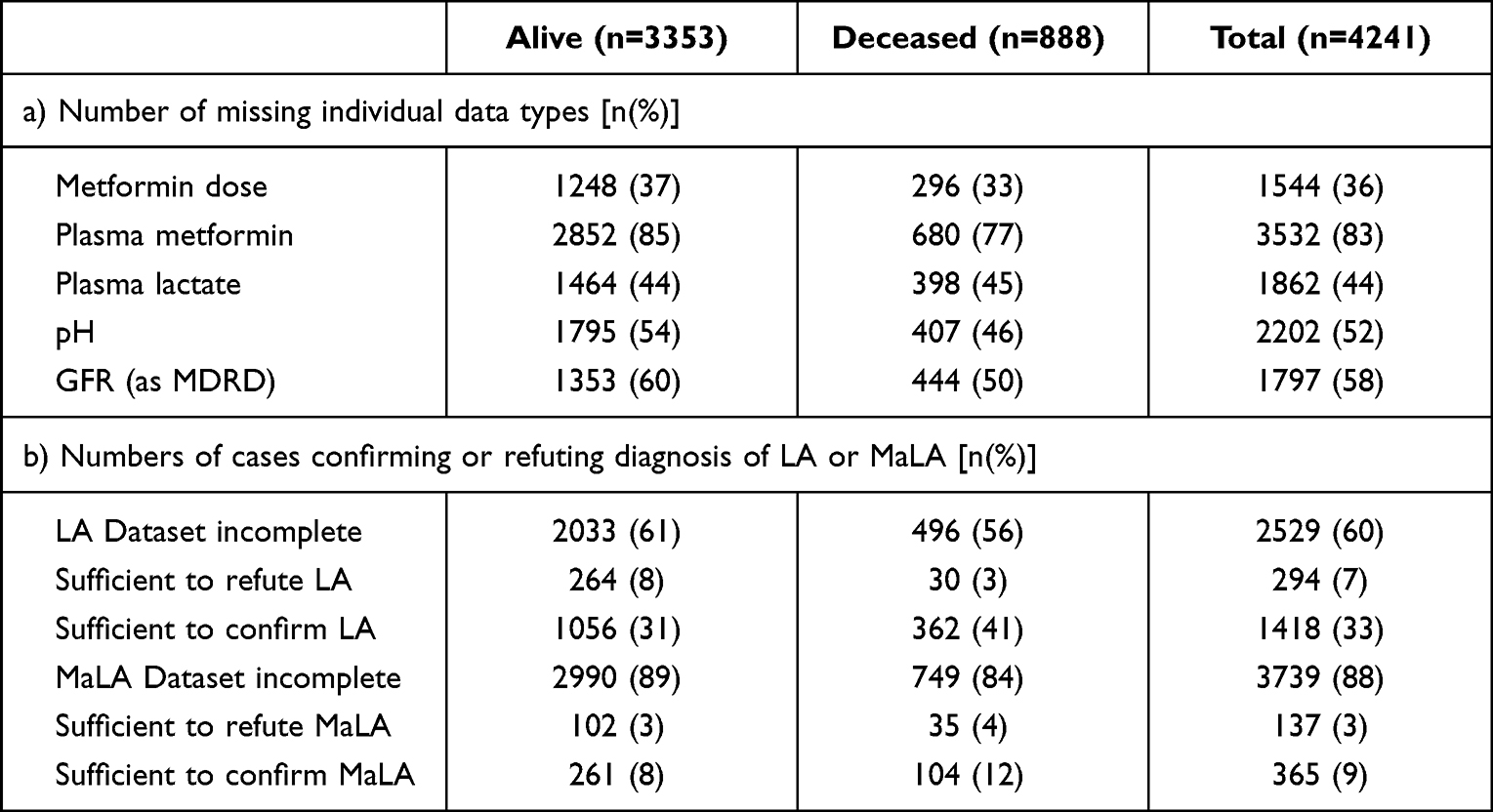 |
Table 1 Missing Data |
Within a total of 4241 cases meeting the study inclusion criteria (the overall population), 1712 cases contained sufficient information to confirm the diagnosis of LA (plasma lactate and pH; 40% of all cases) (Table 1B). Of these, 1418 cases (33% of all cases) included a correct diagnosis of LA (the LA population), and 294 cases (7% of all cases) diagnosed LA incorrectly. Only 502 cases (12% of all cases) contained sufficient information to diagnose MaLA (plasma lactate, pH and plasma metformin). Of these, 365 cases (9% of all cases) included a correct diagnosis of MaLA (the MaLA population), while 137 cases (3% of all cases) included an incorrect diagnosis of MaLA (Table 1B).
Clinical and Metabolic Variables
Characteristics of the Study Population
Table 2 presents the reported demographic, treatment, and disease characteristics for the overall population and for the LA and MaLA subpopulations. In the overall population, the median metformin daily dose was 1700 (interquartile range 1000, 2550) mg. Other median values were 25.0 (6.6, 47.0) mg/L for plasma metformin, 12.0 (6.1, 19.0) mmol/L for plasma lactate, 7.1 (6.9, 7.2) for pH, and 8.0 (4.0, 28.8) mL/min for eGFR. As expected, the median dose of metformin and plasma metformin were higher in the MaLA subpopulation, 2550 (1700, 3000) mg and 38.6 (21.4, 55.7) mg/L, respectively. Furthermore, median plasma lactate was also slightly higher in this subpopulation: 17.0 mmol/L (12.0, 22.0).
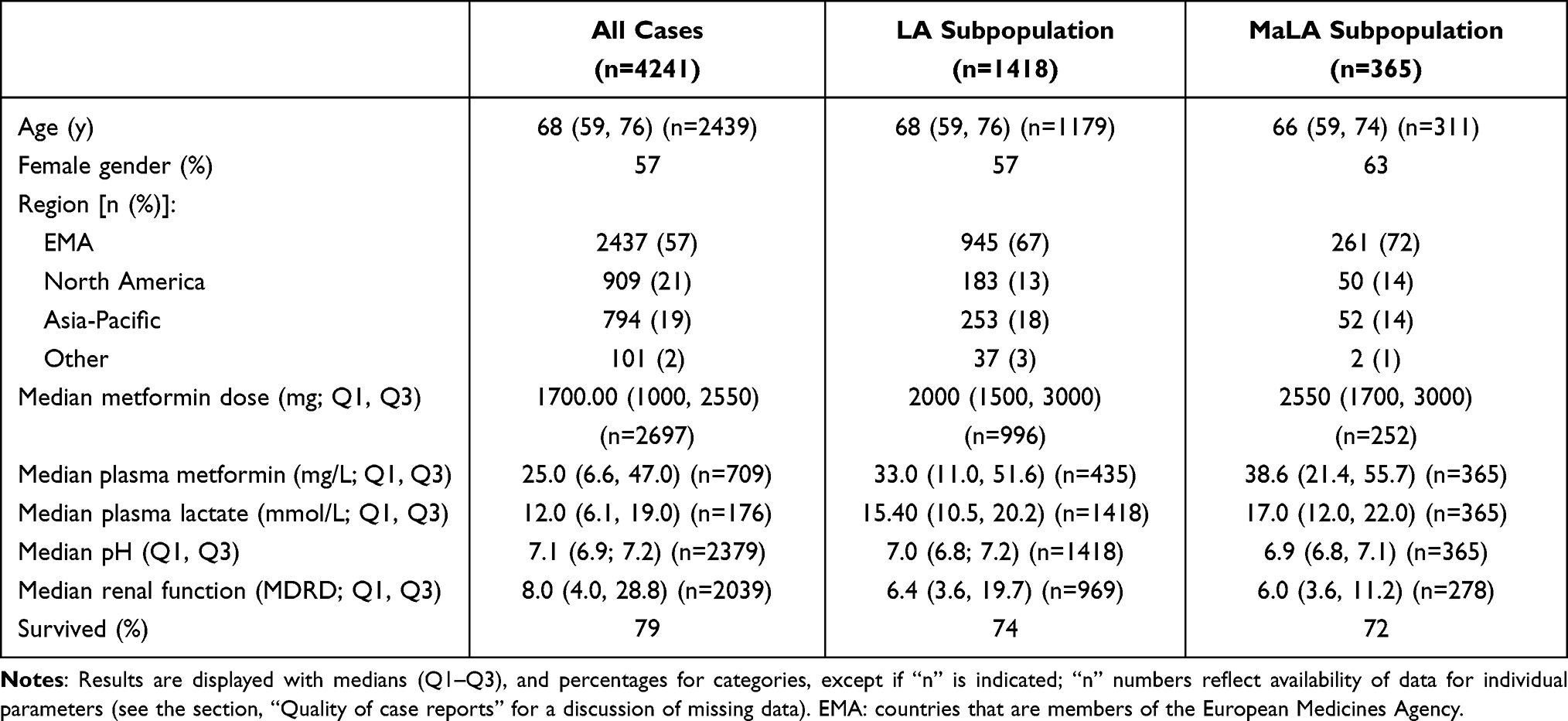 |
Table 2 Demographic Characteristics and Key Laboratory Parameters Relevant to Lactic Acidosis (LA) and Metformin-Associated Lactic Acidosis (MaLA) |
Online Supplementary Table 1 shows the results of descriptive analysis of plasma metformin, pH, and plasma lactate after stratification of the overall population for daily metformin dosage. The proportions of patients in elevated plasma metformin categories (>50 mg/L) did not increase consistently as the metformin dose increased. This was the case even where the recorded metformin dose was above the upper limit of its therapeutic dosage range (>3000 mg).
Correlations Between Metformin Dose, Metformin Plasma Level, pH, Plasma Lactate and Renal Function
Spearman correlation analyses showed that most variables correlated weakly with each other (Online Supplementary Table 2). The highest correlation (moderate magnitude) between key metabolic variables was for plasma lactate and pH (rho between –0.47 and –0.61), which was not surprising for populations with data to support diagnoses of LA or MaLA. Plasma metformin correlated weakly and positively with plasma lactate (rho 0.35) and weakly and negatively with GFR (rho –0.32) in the overall population, but not in the LA subpopulation (plasma lactate: rho 0.25; GFR: rho –0.29) or MaLA subpopulation (plasma lactate: rho 0.26; GFR: rho –0.14). A moderate and negative correlation was seen between plasma metformin and pH for the overall population (rho –0.45) and for the LA and MaLA subpopulations (rho –0.4 and –0.35, respectively).
For patients who received doses of metformin that were above or below the European maximum dosage for metformin of 3000 mg/day, the strongest correlations were seen in either dose group for plasma metformin vs plasma lactate (rho 0.63) or pH (rho −0.63), and metformin dose vs GFR (rho 0.42). Plasma metformin correlated weakly and negatively with GFR (rho –0.42) and pH correlated weakly and positively with GFR (0.3) only in the lower dose metformin group (ie, patients recorded as receiving a dose within the permitted range in the metformin label).
Mortality Outcomes
Overview of Vital Status
A total of 21% (n = 888) of the cases reported a fatal outcome. Subjects who died were on average slightly older than those who did not (mean differences were 3.7 years [95% CI 2.7, 4.7] for the overall population, 3.2 years [1.6, 4.7] for the LA subpopulation, and 2.3 years [0.5, 5.1] for the MaLA subpopulation). Similar proportions of patients in the LA (26%) and MaLA subgroups (28%) died, with regard to the overall population (21%). Median plasma metformin levels were similar among survivors (26 [7, 45] mg/L, n = 501) and non-survivors (24 [5, 53] mg/L, n = 208) in all cases with data on this parameter. Median plasma metformin was slightly higher in survivors vs non-survivors in the LA subpopulation (34 [12, 51] mg/L vs 27 [7, 55] mg/L) but not in the MaLA subpopulation (37 [24, 54] vs 42 [17, 65]).
Impact of Predefined Clinical Variables on the Probability of Death
Neither plasma metformin concentration nor metformin dose was associated with risk of death in univariate analyses (Online Supplementary Table 3). The higher category of plasma lactate (10–20 mmol/L vs <2.5 mmol/L) was associated with mortality in the analysis of all cases (with ORs of 5–7, p < 0.001 for all), and in the LA subpopulation (ORs of 3–4, p ≤ 0.008). In the MaLA subpopulation, ORs were significant for plasma lactate 10–20 mmol/L (OR 4.8, p = 0.0048) and 20–50 mmol/L (OR 7.5, p < 0.001).
Multivariable analyses included an index of exposure to metformin, together with lactate plasma levels, pH, exposure/or not to other risk factors for LA. More than 80% of case records lacked information on the plasma level of metformin (see above). For this reason, separate multivariable analyses were conducted using either the metformin plasma level (Figure 1A) or the metformin dose (Figure 1B). Higher plasma metformin levels were associated with reduced risk of death in the overall population and in the MaLA subpopulation (Figure 1). Higher levels of plasma lactate were associated with mortality in all three populations (the “outlier” values did not, perhaps due to smaller numbers of cases). There was no significant association between categories of acidosis (low pH) and risk of mortality.
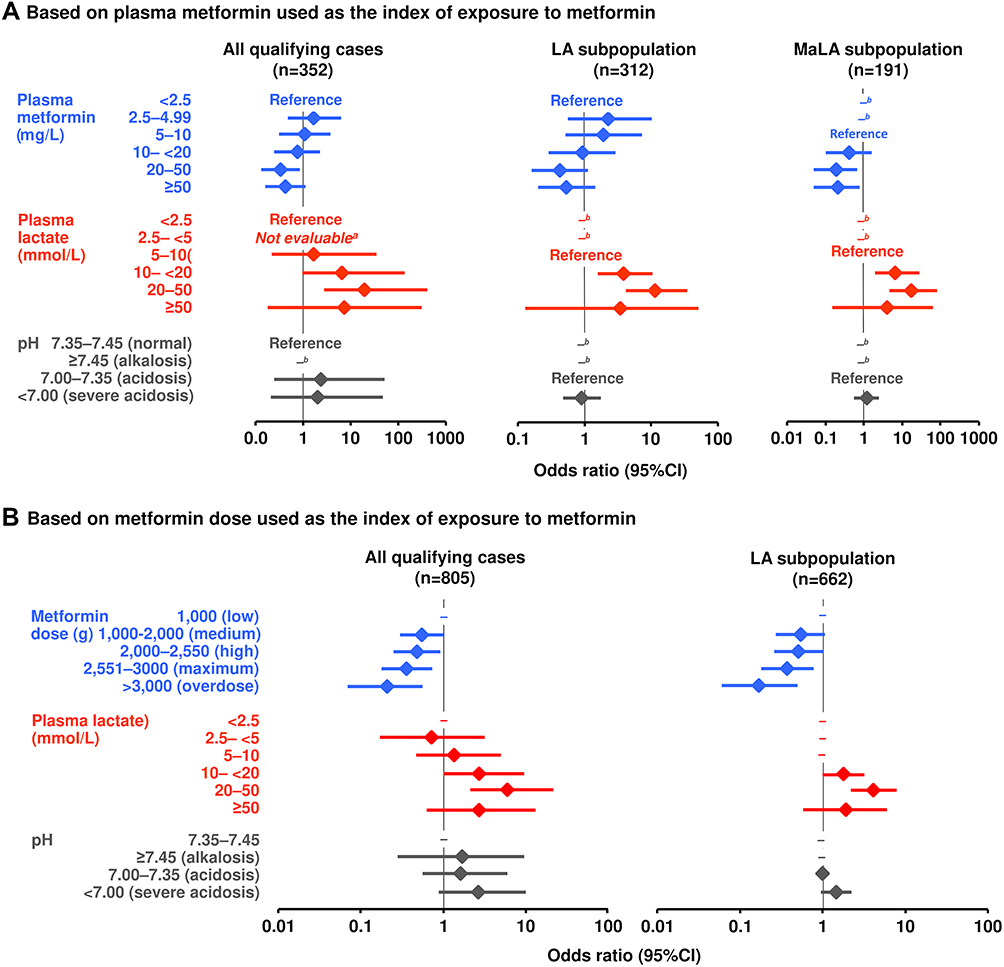 |
Figure 1 Multivariable analyses of LA variables associated with the risk of death. Odds ratios (ORs) >1 signify increased mortality risk. Results were further adjusted on MDRD (quantitative), age (continuous), gender (qualitative), total drug usage (quantitative number of different drugs used), at least one risk factor (binary, yes/no) and world region (qualitative). aNot estimable. bRecords containing data inconsistent with the inclusion criteria for subgroups were excluded (plasma lactate <5 mmol/L and pH <7.35 for both subgroups, and additionally plasma metformin <5 g/L for the MaLA subgroup; the lowest remaining category served as reference). Geographical location was analysed but is omitted here (see text). The model was not estimable in the MaLA subpopulation analysis for metformin dose due to few plasma lactate cases reported (non-positivity violation of most of the categories). Only cases with plasma lactate or pH consistent with LA were included for the LA subpopulation; other cases without odds ratios (–) had insufficient data. This footnote applies to both (A and B). |
For the overall population and the LA subpopulation in the model that included metformin dose as the index of drug exposure (Figure 1B), higher doses (including reported doses >3000 mg/day) were associated with lower mortality risk, and higher levels of plasma lactate were associated with increased mortality risk. Again, there was no significant association between pH and mortality risk. There were too few cases containing data on plasma lactate to run the metformin dose-based model for the MaLA subpopulation (non-positivity violation of most of the categories).
Not adjusting on risk factors for LA from the model (renal function, age, comorbid risk factors and medications that may increase the risk of LA) did not substantially alter the relationships between exposure to metformin, plasma lactic acid or pH with mortality risk, compared with the analyses described above (Online Supplementary Figure 2).
Impact of Concomitant Drugs and Risk Factors for Lactic Acidosis on Mortality
The intake of drugs known to be associated with an increased risk of LA (other than metformin), rhabdomyolysis or renal impairment, and comorbid shock, renal impairment, and dehydration, diarrhoea, or vomiting were all present in more than 20% of the study population (Table 3). Most of these were numerically more prevalent in the LA and MaLA subgroups, compared with the overall population.
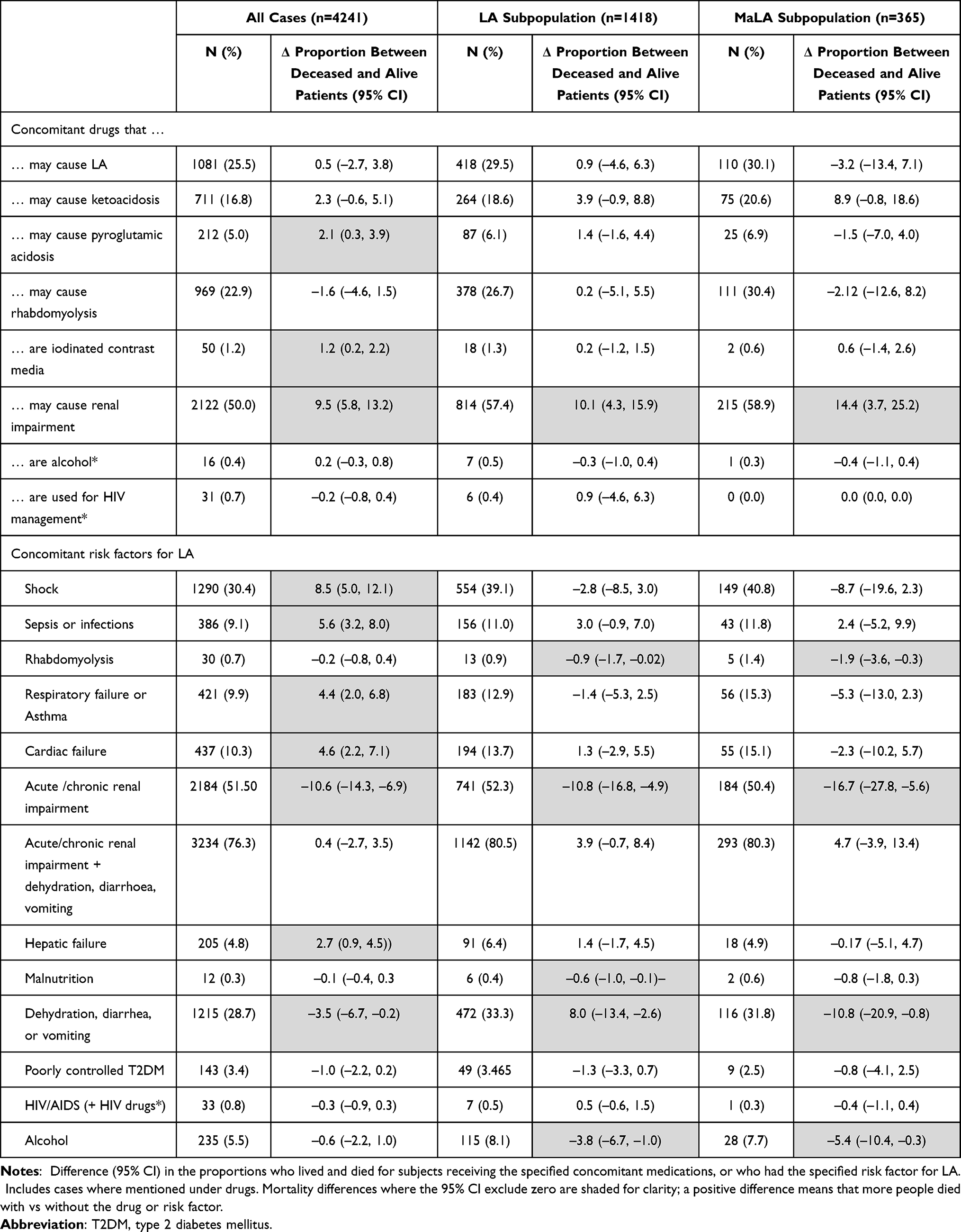 |
Table 3 Risk Factors for Lactic Acidosis (LA) in Relation to the Frequency of a Fatal Outcome |
The only variables associated with a difference in frequency of death cases (ie, where the 95% CI for the difference in frequency of death cases versus alive cases excluded zero) across all three main populations studied were drugs that may cause renal impairment (~10–14% were more frequently reported with death cases); acute or chronic renal impairment (~11–17% mortality less frequently reported); and dehydration, nausea or vomiting (~3–11% were less frequently reported with death cases). Otherwise, differences in mortality between those with or without a drug or risk factor were generally small, other than a difference of 8.5% for shock in the population including all cases.
Too few cases received metformin >3000 mg to support meaningful analysis of the risk of mortality in this subgroup.
Discussion
It is important to understand the pathophysiology of lactic acidosis and the contexts in which it arises, as there is evidence that fear of this adverse outcome has led to under use of metformin in patients with conditions, such as chronic kidney disease, hepatic dysfunction and heart failure.20 Moreover, a range of potential therapeutic actions of metformin in addition to its antihyperglycaemic actions in recent years, including possibly beneficial actions on the cardiovascular system (on the vascular endothelium 21 and the failing heart) 22,23, an anti-inflammatory action of potential relevance to rheumatic immunological diseases 24, anti-cancer activity 25, and potential for the treatment of morbidities associated with aging 26. The possibility of extensions to the therapeutic indications for metformin beyond prediabetes and diabetes in the future adds to the need to study this rare, but serious side-effect.
Our analysis evaluated 4241 spontaneous reports of LA attributed to metformin in terms of their quality (completeness of relevant data). Only about one-third of these included sufficient data on plasma lactate and pH to support a diagnosis of LA according to commonly used criteria of pH <7.35 and plasma lactate >5 mmol/L.14–18 Less than one-tenth of cases included data on the plasma metformin level, in addition to pH and lactate. An earlier report (incorporating data from 1995 to 2010) from the same database as the present study found that only 10% of the 869 case studies supported the diagnosis of MaLA with demonstration of low pH, elevated plasma lactate and high plasma metformin.27
A recent publication addressed the difficulty of distinguishing between MaLA, “metformin-induced lactic acidosis” (MiLA), and “metformin unrelated lactic acidosis” (MuLA).14 These authors proposed a checklist of key information to include when assessing or reporting a case of suspected MaLA, including timings and amounts of metformin intake, renal status, detailed information on acid-base status, levels of plasma and erythrocyte metformin (and when these were measured compared with metabolic and clinical findings), and details of concomitant medications and comorbid risk factors for LA. In the absence of plasma metformin measurement, accumulation of metformin could be diagnosed based on steady-state or acute changes in renal status, and the size and timing of the last metformin dose. The administration of this Pharmacovigilance Database involves the use of a targeted questionnaire checking for all of the above since 2016, however reporters rarely collect the required information and should be encouraged to do so when documenting a MaLA case. Such information would support classification of reports into MuLA (LA with low plasma metformin), MaLA (LA with plasma metformin >5 mg/L, as per the present study), and MiLA (LA with very high plasma metformin). Our MaLA subpopulation satisfied the criteria for MaLA or MiLA (we did not seek to distinguish between these diagnoses). Our LA subpopulation was likely a mix of cases of MuLA and MaLA. A high proportion of MiLA is most likely represented in the group with a daily dose higher than the upper limit of its therapeutic dosage range (>3000 mg).
We sought to explore relationships between exposure to metformin and the severity of LA or MaLA. With regard to metabolic indices, correlations between metformin dose and metabolic parameters were weak. The dose of metformin as presented in the case report may not have been a reliable surrogate for exposure to metformin, however, as this could have been the usual daily dose, or a single dose considered to be associated with a MaLA event. Plasma metformin correlated more strongly with plasma lactate (positively) and pH (negatively) in all populations studied. It is well known that treatment with metformin induces a modest increase in lactate levels,28 so the latter finding would not be surprising. A previous report suggested that acute kidney injury was an important driver of elevated lactate in this setting.29 The fall in pH as plasma metformin increased may provide a suggestion of an association of increased exposure to metformin and lactic acidosis, however.
The limitations of our study were as follows. We used diagnostic criteria for LA which are used commonly;14–18 however, other criteria have been employed by other authors studying MaLA.30 A lack of unambiguous diagnostic criteria, especially on a “safe” metformin plasma concentration, hampers this field of research. We had little or no information on the relative timing of metformin doses, which is critical to the diagnosis of MaLA, especially where data on plasma metformin are absent, as described above. We also had little information on the time windows within which plasma lactate, pH and metformin measurements were made, or the intervals between metformin exposure, the onset of LA and death. These factors may be a source of bias relating to analysis of mortality outcomes and are important limitations of our analyses based on the metformin dose.14,31 In addition, the maximum recommended dosage for immediate-release metformin varies between regions (eg, 2550 mg/day in the USA and 3000 mg in Europe) and also formulation, as the recommended maximal dose for the once-daily prolonged release (XR or SR) formulation is 2000 mg/day. Moreover, whether immediate-release or XR metformin was used would complicate diagnostic interpretation of the relationship between the time/amount of metformin ingestion and presentation with LA. We suggest adding the formulation of metformin to the checklist of key data necessary to confirm or exclude MaLA. Plasma metformin levels are themselves challenging to interpret. Metformin is distributed into certain tissues rapidly after ingestion, with the highest concentrations found in tissues such as gut and liver, where it is believed to exert most of its antihyperglycemic effect.32 Little information is available on the actual therapeutic plasma concentration of metformin, which is remarkable for a drug that has been in continuous therapeutic use in Europe for more than 60 years.33 The impact of the metformin plasma concentration on the case outcome and the comparison of the LA and MaLA subpopulations (Figure 1A) support the threshold of a safe plasma concentration at 5 mg/L, rather than 2.5 mg/L as discussed elsewhere.34
We also considered mortality as a key outcome. Previous reports based on 169 or 26035 reported diagnoses of MaLA with plasma metformin measurements found that survivors had higher plasma metformin concentrations than non-survivors, respectively. Our data from this larger population did not support this finding: only slightly higher plasma metformin levels on the overall and LA subpopulation were small in comparison with the variability of this parameter, and median plasma metformin was lower in survivors in our MaLA subpopulation. Moreover, the logistic regression analyses provided scant support for a relationship between either plasma metformin or metformin dose and increased risk of mortality. Indeed, there was a suggestion of reduced risk of mortality as measure of exposure to metformin increased, which may be consistent with earlier reports of lower risk of mortality in recipients vs non-recipients of metformin among populations with lactate levels consistent with LA.31,36 Higher plasma lactate was the only metabolic variable convincingly related to increased risk of mortality in our multivariable analysis. This finding does not concur with the earlier analysis of a subset of this population,27 although increased lactate has been associated with increased risk of mortality in other studies in populations with LA.37 Also, lower vs higher categories of pH did not drive higher mortality risk in our study, which concurs with the earlier analysis of some of our cases.38
Other risk factors (drug treatments and comorbid conditions) that may predispose to LA were common, as would be expected, and previous reports have ascribed a substantial part of the risk of death during a MaLA event to such comorbid drug or disease factors.10,11,38,39 Examination of individual potential risk factors revealed a strong influence of acute or chronic renal dysfunction on the risk of mortality; this finding supports the maintenance of the current contraindications for metformin treatment relating acute renal impairment and to severe chronic kidney. Renal function per se (calculated from reported data), age and gender did not markedly influence mortality outcomes.
The retrospective design of our study, based on spontaneous adverse event reporting (which probably reflected the most serious LA events occurring in patients receiving usual-care metformin treatment, a potential source of bias), is the most important limitation of the study, which could be remedied only by the reporter of spontaneous adverse events providing as much detail as possible. We have demonstrated a lack of important data in these reports, especially with regard to plasma metformin levels and detailed information on the amount, timings and formulation of metformin intakes. Likewise, lack of variables implies that the logistic models assessing the association between LA variables and risk of death were based on the limited common set of cases with non-missing values. Only cases with complete information on all adjustment variables were analysed in the logistic models. Different diagnostic criteria for MaLA have also been used. Accordingly, the associations with death should be interpreted with caution even in this large series of reports of MaLA. Similarly, other limitations were our inability to adjust for other potential confounders that were not reported, and the relatively limited number of cases available for logistic regression analysis (especially for the MaLA subpopulation). Its principal strength was the size of the population in the database under study (this is the largest case series of its kind to date) which allowed construction of specific LA and MaLA subpopulations.
Conclusions
Most of a large series of reports of MaLA in a pharmacovigilance database did not provide sufficient data to confirm the validity of a diagnosis of either LA of any etiology, or MaLA, in particular. The quality of these reports does not seem to have improved over recent decades. Exposure to metformin (as judged by plasma metformin concentrations) correlated to some extent with rising lactate levels and reduced pH, but did not influence mortality, including in subpopulations with a high likelihood of having LA or MaLA.
Acknowledgments
The study team wish to express their gratitude to the many health-care professionals who, despite busy schedules, dedicated their time and expertise to reporting the adverse events we analysed here. In order to make the best use, ultimately for other patients, we encourage you to share as much detail as possible, especially regarding lab values and potential confounders, whether considered related or not, in your report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Preliminary results of this study were presented in part in the IDF 2019 Congress (2–6 December 2019, abstract BU-04319) and in a comment on ‘Flory et al. Reports of lactic acidosis attributed to metformin, 2015–2018. Diabetes Care. 2020;43:244–246’.
Funding
The study was funded by Merck healthcare KGaA, Darmstadt, Germany. Dr. Mike Gwilt (GT Communications), provided editorial assistance in the development of the manuscript, funded by Merck Healthcare KGaA Darmstadt, Germany.
Disclosure
All authors are full-time employees of Merck KGaA, Darmstadt, Germany. The authors report no other conflicts of interest in this work.
References
1. Eppenga WL, Lalmohamed A, Geerts AF, et al. Risk of lactic acidosis or elevated lactate concentrations in metformin users with renal impairment: a population-based cohort study. Diabetes Care. 2014;37:2218–2224. doi:10.2337/dc13-3023
2. Richy FF, Sabidó-Espin M, Guedes S, Corvino FA, Gottwald-Hostalek U. Incidence of lactic acidosis in patients with type 2 diabetes with and without renal impairment treated with metformin: a retrospective cohort study. Diabetes Care. 2014;37:2291–2295. doi:10.2337/dc14-0464
3. Howlett HC, Bailey CJ. A risk-benefit assessment of metformin in type 2 diabetes mellitus. Drug Saf. 1999;20:489–503. doi:10.2165/00002018-199920060-00003
4. Stang M, Wysowski DK, Butler-Jones D. Incidence of lactic acidosis in metformin users. Diabetes Care. 1999;22:925–927. doi:10.2337/diacare.22.6.925
5. Salpeter S, Greyber E, Pasternak G, Salpeter E. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Database Syst Rev. 2006;25(1):CD002967.
6. Inzucchi SE, Lipska KJ, Mayo H, Bailey CJ, McGuire DK. Metformin in patients with type 2 diabetes and kidney disease: a systematic review. JAMA. 2014;312:2668–2675. doi:10.1001/jama.2014.15298
7. Alvarez CA, Halm EA, Pugh MJV, et al. Lactic acidosis incidence with metformin in patients with type 2 diabetes and chronic kidney disease: a retrospective nested case-control study. Endocrinol Diabetes Metab. 2020;4:e00170. doi:10.1002/edm2.170
8. Chan NN, Brain HP, Feher MD. Metformin-associated lactic acidosis: a rare or very rare clinical entity? Diabet Med. 1999;16:273–281. doi:10.1046/j.1464-5491.1999.00006.x
9. van Berlo-van de Laar IR, Vermeij CG, Doorenbos CJ. Metformin associated lactic acidosis: incidence and clinical correlation with metformin serum concentration measurements. J Clin Pharm Ther. 2011;36:376–382. doi:10.1111/j.1365-2710.2010.01192.x
10. Lalau JD, Race JM. Lactic acidosis in metformin therapy: searching for a link with metformin in reports of ‘metformin-associated lactic acidosis’. Diabetes Obes Metab. 2001;3:195–201. doi:10.1046/j.1463-1326.2001.00128.x
11. Lalau JD, Race JM. Lactic acidosis in metformin-treated patients. Prognostic value of arterial lactate levels and plasma metformin concentrations. Drug Saf. 1999;20:377–384. doi:10.2165/00002018-199920040-00006
12. Stades AM, Heikens JT, Erkelens DW, Holleman F, Hoekstra JB. Metformin and lactic acidosis: cause or coincidence? A review of case reports. J Intern Med. 2004;255:179–187. doi:10.1046/j.1365-2796.2003.01271.x
13. Bailey CJ, Campbell IW, Chan JCN, Davidson JA, Howlett HCS, Ritz P. Metformin: The Gold Standard. A Scientific Handbook. Chichester (UK): Wiley; 2007.
14. Lalau JD, Kajbaf F, Protti A, Christensen MM, De Broe ME, Wiernsperger N. Metformin-associated lactic acidosis (MALA): moving towards a new paradigm. Diabetes Obes Metab. 2017;19:1502–1512. doi:10.1111/dom.12974
15. Kraut JA, Madias NE. Lactic acidosis. N Engl J Med. 2014;371:2309–2319. doi:10.1056/NEJMra1309483
16. Kraut JA, Madias NE. Lactic acidosis: current treatments and future directions. Am J Kidney Dis. 2016;68:473–482. doi:10.1053/j.ajkd.2016.04.020
17. Lewis J. Lactic acidosis. MSD Manual, Professional. Available from https://www.msdmanuals.com/professional/endocrine-and-metabolic-disorders/acid-base-regulation-and-disorders/lactic-acidosis.
18. Glucophage® (metformin hydrochloride) Tablets. US prescribing information. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/020357s037s039,021202s021s023lbl.pdf.
19. Foucher CD, Tubben RE. Lactic acidosis. StatPearls. Available from https://www.ncbi.nlm.nih.gov/books/NBK470202/.
20. Salvatore T, Pafundi PC, Marfella R, et al. Metformin lactic acidosis: should we still be afraid? Diabetes Res Clin Pract. 2019;157:107879. doi:10.1016/j.diabres.2019.107879
21. Salvatore T, Pafundi PC, Galiero R, et al. Can metformin exert as an active drug on endothelial dysfunction in diabetic subjects? Biomedicines. 2020;9:3. doi:10.3390/biomedicines9010003
22. Salvatore T, Galiero R, Caturano A, et al. Effects of metformin in heart failure: from pathophysiological rationale to clinical evidence. Biomolecules. 2021;11:1834. doi:10.3390/biom11121834
23. Schernthaner G, Brand K, Bailey CJ. Metformin and the heart: update on mechanisms of cardiovascular protection with special reference to comorbid type 2 diabetes and heart failure. Metabolism. 2022;130:155160. doi:10.1016/j.metabol.2022.155160
24. Salvatore T, Pafundi PC, Galiero R, et al. Metformin: a potential therapeutic tool for rheumatologists. Pharmaceuticals. 2020;13:234. doi:10.3390/ph13090234
25. Morgillo F, Fasano M, Della Corte CM, et al. Results of the safety run-in part of the METAL (METformin in Advanced Lung cancer) study: a multicentre, open-label Phase I-II study of metformin with erlotinib in second-line therapy of patients with stage IV non-small-cell lung cancer. ESMO Open. 2017;2:e000132. doi:10.1136/esmoopen-2016-000132
26. Salvatore T, Pafundi PC, Morgillo F, et al. Metformin: an old drug against old age and associated morbidities. Diabetes Res Clin Pract. 2020;160:108025. doi:10.1016/j.diabres.2020.108025
27. Kajbaf F, Lalau JD. The criteria for metformin-associated lactic acidosis: the quality of reporting in a large pharmacovigilance database. Diabet Med. 2013;30:345–348. doi:10.1111/dme.12017
28. Davis TM, Jackson D, Davis WA, Bruce DG, Chubb P. The relationship between metformin therapy and the fasting plasma lactate in type 2 diabetes: the Fremantle Diabetes Study. Br J Clin Pharmacol. 2001;52:137–144. doi:10.1046/j.0306-5251.2001.01423.x
29. Posma RA, Hulman A, Thomsen RW, Jespersen B, Nijsten MW, Christiansen CF. Metformin use and early lactate levels in critically ill patients according to chronic and acute renal impairment. Crit Care. 2020;24:585. doi:10.1186/s13054-020-03300-y
30. Bennis Y, Bodeau S, Batteux B, et al. A study of associations between plasma metformin concentration, lactic acidosis, and mortality in an emergency hospitalization context. Crit Care Med. 2020;48:e1194–e1202. doi:10.1097/CCM.0000000000004589
31. Krowl L, Al-Khalisy H, Kaul P. Metformin-induced lactic acidosis (MILA): review of current diagnostic paradigm. Am J Emerg Med. 2018;36:e3–e908. doi:10.1016/j.ajem.2018.01.097
32. Wilcock C, Bailey CJ. Accumulation of metformin by tissues of the normal and diabetic mouse. Xenobiotica. 1994;24:49–57. doi:10.3109/00498259409043220
33. Kajbaf F, De Broe ME, Lalau JD. Therapeutic concentrations of metformin: a systematic review. Clin Pharmacokinet. 2016;55:439–459. doi:10.1007/s40262-015-0323-x
34. Lalau JD, Kajbaf F, Bennis Y, Hurtel-Lemaire AS, Belpaire F, De Broe ME. Metformin treatment in patients with type 2 diabetes and chronic kidney disease stages 3A, 3B, or 4. Diabetes Care. 2018;41:547–553. doi:10.2337/dc17-2231
35. Boucaud-Maitre D, Ropers J, Porokhov B, et al. Lactic acidosis: relationship between metformin levels, lactate concentration and mortality. Diabet Med. 2016;33:1536–1543. doi:10.1111/dme.13098
36. Posma RA, Frøslev T, Jespersen B, et al. Prognostic impact of elevated lactate levels on mortality in critically ill patients with and without preadmission metformin treatment: a Danish registry-based cohort study. Ann Intensive Care. 2020;10:36. doi:10.1186/s13613-020-00652-0
37. Yeh HC, Ting IW, Tsai CW, Wu JY, Kuo CC. Serum lactate level and mortality in metformin-associated lactic acidosis requiring renal replacement therapy: a systematic review of case reports and case series. BMC Nephrol. 2017;18:229. doi:10.1186/s12882-017-0640-4
38. Misbin RI. The phantom of lactic acidosis due to metformin in patients with diabetes. Diabetes Care. 2004;27:1791–1793. doi:10.2337/diacare.27.7.1791
39. Lalau JD, Lacroix C, Compagnon P, et al. Role of metformin accumulation in metformin-associated lactic acidosis. Diabetes Care. 1995;18:779–784. doi:10.2337/diacare.18.6.779
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.