")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Qualitative Analyses of the Reasons Why Patients Do Not Attend Scheduled Inpatient Appointments in a Hospital in Guangzhou, China
Authors Yang M , Xie J, Zhang H, Chen Y, Xie S, Peng R, Jia Y, Chen Y, Wang L
Received 7 September 2020
Accepted for publication 11 November 2020
Published 7 December 2020 Volume 2020:13 Pages 2857—2865
DOI https://doi.org/10.2147/RMHP.S280665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Mudi Yang,1,2 Jun Xie,2 Huan Zhang,2 Yingyong Chen,2 Shuo Xie,2 Rui Peng,2 Yu’e Jia,2 Yajing Chen,2 Lizi Wang1,2
1School of Nursing, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Admission Management Center of Zhujiang Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Lizi Wang
Admission Management Center of Zhujiang Hospital, Southern Medical University, 253 Gongye Road M, Haizhu District, Guangzhou, Guangdong 510280, People’s Republic of China
Tel/Fax +86 206 278 2038
Email [email protected]
Purpose: Exploration of the reasons why people miss scheduled inpatient appointments from the perspectives of patients.
Methods: Semi-structured interviews via telephone were conducted with patients who missed their inpatient appointments. Data were analyzed based on Colaizzi’s seven-step method.
Results: Twenty-five patients and five dependents were enrolled. Three themes were identified: practical barriers, lack of knowledge about the disease, and negative emotional responses. Personal social obligations, state of illness, financial issues and long waiting times were the main practical barriers preventing patients from attending their inpatient appointment. Patients’ perceptions of feasible self-solving symptoms, readily believing people around them, and a blindly optimistic attitude towards disease contributed to their insufficient knowledge about the disease. Negative emotional responses (eg, sense of fear and lack of trust in physicians) had a detrimental effect on inpatient attendance.
Conclusion: Three main factors contributed to non-attendance of inpatient appointments: practical barriers, lack of knowledge about disease, and negative emotional response. Our study provides new, valuable evidence on non-attendance of inpatient appointments in China. Our findings could offer meaningful insights into developing effective strategies to reduce non-attendance of inpatient appointments in other countries.
Keywords: non-attendance, health-seeking behavior, medical appointment services, qualitative study, inpatient appointment
Introduction
The National Commission and National Administration of Traditional Chinese Medicine jointly formulated the Action Plan for Further Improving Medical Services (2018–2020). They proposed that if conditions permit, medium-sized and large hospitals should increase the proportion of appointment services, such as creating an inpatient appointment (IA) service. This is not only the most convenient way for patients to receive treatment, but also the most efficient use of medical resources. In the meantime, with advancement of this medical-appointment service, missed appointments have become increasingly prominent. A missed IA denotes a situation whereby, when receiving a telephone reminder for hospital admission, the patient refuses to be hospitalized (ie, does not attend). A missed appointment not only affects the health service negatively, it is also detrimental to the individual’s health. Non-attendance can lead directly to economic losses and underutilized medical resources.1–3 For instance, according to the system at the University of California (USA), there are ~67,000 non-attenders in the outpatient department per year, and the estimated economic loss is ~$7 million.4 With respect to an individual’s health, missing an appointment can lead to a worse health-related outcome, including complex complications as well as an increased risk of morbidity and mortality.5–7 In addition, lengthening the waiting time of other patients results in their failure to attend an appointment in a timely manner, which could render a lost opportunity for efficacious treatment.8,9
Studies on non-attendance have, to a large extent, focused on outpatient appointments, with scant attention being paid to IAs. An IA refers to a patient with indications that can be managed in the inpatient setting who makes a scheduled appointment with the Admission Management Center (AMC) for hospitalization after the attending physician has issued a hospitalization application. In China, few studies have assessed why patients miss scheduled IAs from their perspective. We intended to fill this information gap in the present study.
Methods
Study Design and Setting
We sought out the reasons why patients missed their scheduled IA in an affiliated, third-grade class-A, general-public hospital with >2500 beds in Guangzhou (China). Guangzhou is the capital of Guangdong Province, which has >15 million residents. There are ~20 third-grade, class-A general-public hospitals with high-quality medical resources that admit local patients and patients with complicated/severe disease outside Guangzhou. The studied hospital has >100,000 inpatients each year, among which 60% of the patients come from outside Guangzhou. The prevalence of non-attendance in the studied hospital is ~10%, a value that is consistent with that of other studies of tertiary hospitals in China.10 If non-attendance is to be managed, it is crucial to understand the thoughts of patients and to identify the factors that could be subject to change. We utilized a qualitative research design that allowed a broad exploration of the issues and in-depth understanding of the patients’ perspective into the reasons why they missed their scheduled IA.11
Some sections of large-scale tertiary hospitals have implemented an IA service. Usually, beds are not available as soon as patients arrive at hospital, and they must wait. As a result, there are >200 patients waiting in line for hospitalization every day in the studied hospital. Facing this situation, seven senior nurses in the AMC are responsible for bed reservation, notification of hospital admission, and bed allocation. In general, the staff of the AMC inform patients that they are to be hospitalized 1 day in advance, according to the principle of “emergency first, critical illness first, and mild illness in order”. If a patient wishes to cancel the IA, he/she can make a telephone call to the AMC directly to inform the staff the reasons why he/she wishes to cancel the appointment. An addition to this, the staff provide health education to patients according to their individual health condition and tell them they have lost an opportunity for efficacious treatment.
Participants
We wished to choose a representative sample for our studies. Hence, purposive sampling based on the proportion of non-attendance for different academic ranks of attending physicians was adopted to screen interviewees. When all the questions had been answered, the interview was terminated. Participants were included if they missed hospitalization appointments at least once. Patients who met one of the following criteria were excluded: 1) had been transferred to other hospital departments for treatment of different diseases while waiting; 2) had been admitted to the emergency department due to sudden changes in their health condition while waiting; 3) did not have a telephone number or had given an incorrect telephone number.
Data Collection
Telephone interviews were carried out by two members of staff responsible for scheduling IAs in the AMC. Both had >3 years of experience of making IAs. The training program for interviewers was developed and delivered by Mudi Yang who, at the time of the study, was in charge of the study design. The training program comprised sections on confidentiality, ethics, interviewing skills, and reflexivity. The duration of the training program was two evenings. To increase the response rate of telephone interviews, investigators contacted patients within 2–3 days after they missed their IAs. Patients who could not make the health-seeking decision by themselves (eg, adolescents or those with a serious health condition) were replaced by a guardian to participate in this interview. At the beginning of the interview, investigators introduced themselves and also explained the purpose of the investigation to interviewees. Upon obtaining verbal informed consent (which was required by our ethics committee) and informing the participants that their responses would be published in an anonymized way, interviewers continued to ask them a series of open-ended questions based on the theory of planned behavior and the investigators’ own experience (Table 1). Each interview lasted 10–30 min and was audio-recorded with the interviewee’s permission. Written notes were also taken simultaneously. The sociodemographic information of patients was obtained from the Hospital Information System. Thirty interviews were completed. To protect the privacy of interviewees, interview records were coded in sequence from P1 to P30 afterwards. In addition to this strategy, investigators maintained an objective position throughout interviews. Opinions expressed from the patients’ viewpoint were respected and not discussed during or after the conversation.
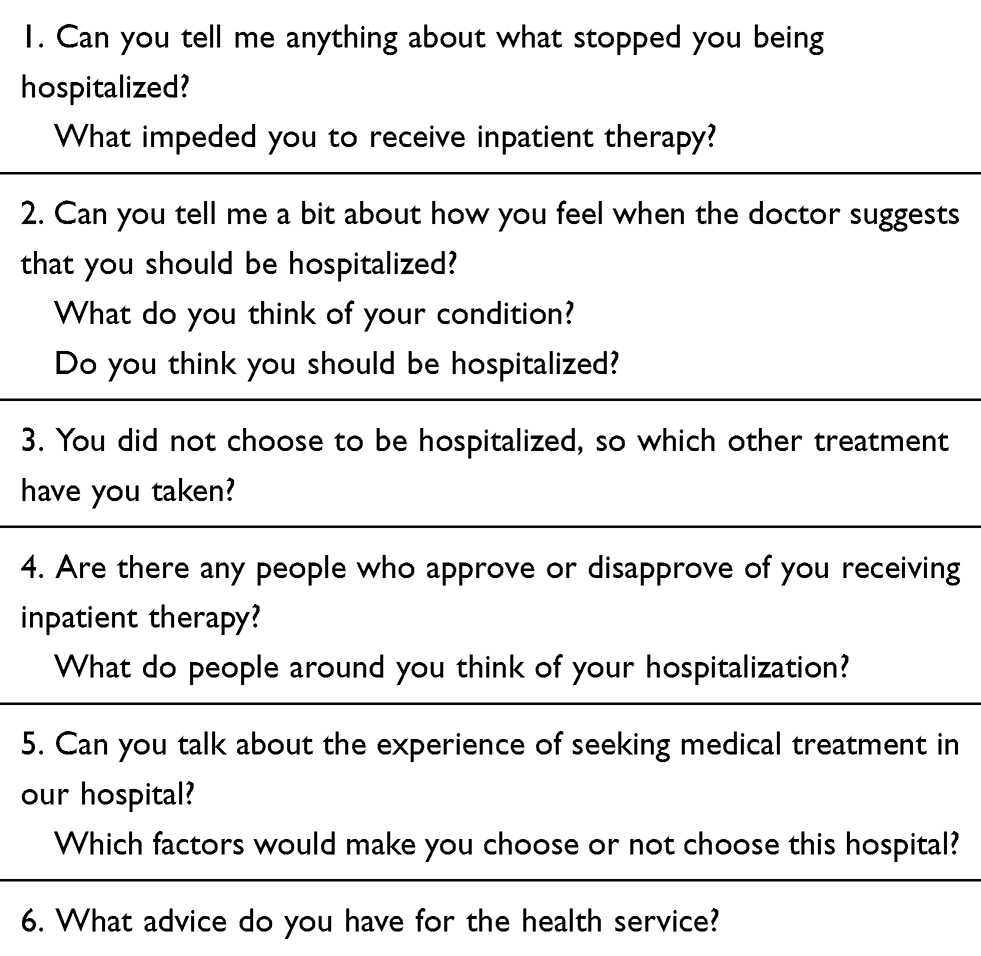 |
Table 1 Interview Questions for Patients |
Data Analyses
Analyses of interview data were in strict accordance with Colaizzi’s seven-step analytical method.12 That is, two investigators transcribed the audio-taped interviews within 24 h of conducting each interview themselves, and two other investigators checked the consistency of the transcripts. If there were differences between what was uttered in the audiotape and the transcript, investigators listened repeatedly to the contents of the audio recording to verify and revise the answers. Then, all research members of the research team stopped reading and re-reading manuscripts until they became familiar with the content and identified important recurring statements. After that, they encoded recurring and important contents and collected encoded opinions to construct meaningful units. Then, they identified all the meaningful units to “cluster” common concepts to form themes. Lastly, the results of the subject structure were returned to interviewees for final verification to ensure the maximum accuracy of results. Most importantly, if paradoxical answers were obtained, researchers re-analyzed the interview data from the first step. Our coding team consisted of four investigators (research assistant, two postgraduate students, and an AMC member) who had experience in analyzing qualitative data. With the supervision and mentorship of senior nurses (LZW, YEJ), the team members worked independently and collaboratively to encode data, thereby ensuring that the analytical process was rigorous. The team met to ensure that the analyses were reliable.
Ethical Considerations
Participants were well informed and had the option to participate or decline participation in our study. They could also terminate the interview at any time. Interviewers made assurances to interviewees from the start, including promising 1) not to reveal participants’ identities and 2) that audiotapes would be stored in a locked cabinet and available only to members of the research team for academic use. At the end of the study, the audiotapes were destroyed. The study protocol was approved (2020-KY-028-01) by the Ethics Committee of Zhujiang Hospital (an affiliated hospital of Southern Medical University) in Guangzhou. Our study was conducted in accordance with the Declaration of Helsinki 1964 and its later amendments.
Results
In total, 79 telephone calls were provided. Twenty-six patients did not answer telephone calls three times. Nine patients refused to participate directly in the interview because they did not have sufficient time or because their health improved. When 25 patients and five guardians had been interviewed, the topic reached saturation. The demographic characteristics of participants are shown in Table 2. Three main themes relating to the reasons why patients missed IAs were identified: 1) practical barriers; 2) lack of knowledge about the disease; and 3) negative emotional responses.
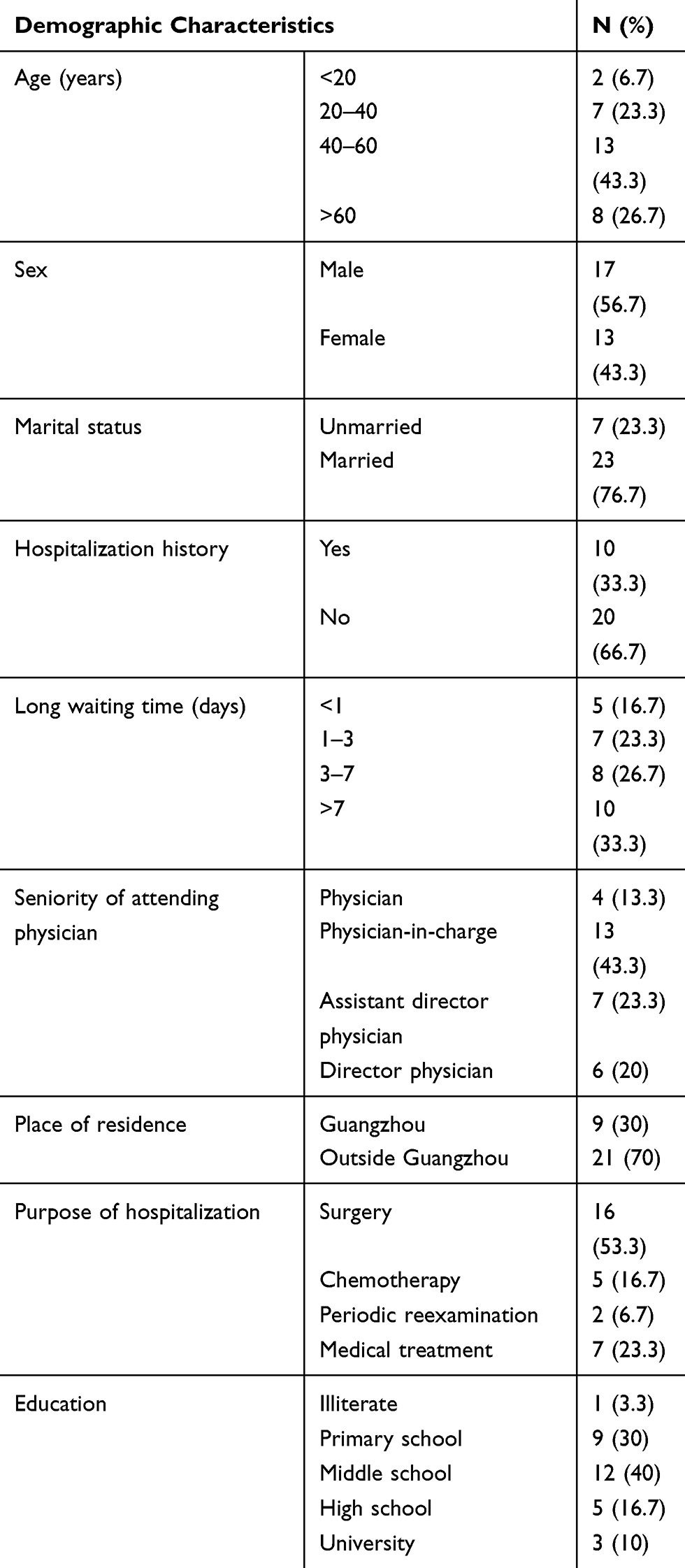 |
Table 2 Demographic Characteristics of People Who Did Not Attend an Inpatient Appointment (n = 30) |
Practical Barriers
According to respondents’ statements, we learnt that there was a range of problems and factors that prevented them from receiving inpatient therapy. For some patients, family obligations and work obligations were the most important barriers. For those with a serious illness, financial issues were the most perspicuous reasons why participants were discouraged from attending AIs. In addition, most of the patients who arrived at the hospital and who were being diagnosed would expect to be treated in a timely manner and did not wish to be discouraged. However, there was limited availability of beds in the hospital, so an increasing number of patients would have to make an appointment. That was another reason why they gave up waiting and sought treatment in another hospital.
Social Obligations
Five participants stated clearly that they wanted to be hospitalized. However, competing demands for their time (eg, family obligations, employer obligations) often took precedence over personal health.
My boss doesn’t allow me to take sick leaves. Besides, I work in Shenzhen which is far away from your hospital; it is so inconvenient for me.… So I consider being hospitalized in our local hospital because at least I don’t need to take so many sick leaves. (P1)
I don’t have any problems attending an appointment. It is just that my house is being renovated at the moment.… If I go to the hospital, no one would take care of it.… So I would not be able to be hospitalized until my house renovation is finished. (P2)
I’m so sorry … as a matter of fact I was still in Guangzhou the day when you informed me.… A few hours later, I received a phone call from my brother, telling me that one of my family members had passed away. That is why I have to delay my appointment with the hospital in order to deal with this issue. (P3)
Physical Status
For most patients, traveling to appointments was not difficult. However, some participants had difficulties in mobility that made the long journey to the hospital an insurmountable hurdle. One guardian mentioned that the mobility problems of his father stopped them from attending.
My father, who suffers from cerebral infarction, has to stay in bed and has a problem in mobility.… As the road construction work is in progress, our car will be diverted at this time … so we need to spend seven hours on the road to the hospital.… We are afraid he cannot stand the long distance. (P4)
Three family dependents mentioned that the financial burden started to add up during inpatient treatments, which led to them not being able to attend a future appointment.
He had surgery in your hospital, and the doctor suggested that he should come back regularly for rehabilitation therapy. It is worth noting that the operation has already cost us a lot.… And our health insurance is a new rural cooperative medical scheme which only reimburses a small part of the expense. Apart from all of the above factors, under such circumstance, I certainly would want to follow doctor’s advice and want him to receive further professional treatments. (P7)
I was sad.… If we could afford it, my daughter wouldn’t have to stand so much pain … when she cries, my heart is broken … (P9)
His condition is not optimistic … together, this comes with the huge burden in finance. I really don’t see any hopes … (P15)
Eight patients and one dependent complained that the long waiting time was the direct cause for them missing the appointment. At the time, they were anxious about how quickly the illness could progress. They perceived a need to move forward quickly with treatment while they were waiting. With an unsettled feeling, they gave up waiting and turned to another hospital for treatment.
My mother’s condition is urgent. She temporarily stayed in the emergency department waiting for a bed in the ordinary department … there was an available bed once, then she got transferred into the ordinary department. However, there was still no bed for the next few days. At the emergency department, they were just offering some injections to control her vomiting situation, but the effect was not that good … so we gave up waiting and went to another hospital. (P19)
Although the doctor prescribed some medicines, I was still feeling pretty uneasy while waiting. The tumor was in my brain, and I don’t know how quickly it could progress.… I was extremely worried that it would grow bigger or turn malignant … (P6)
I have been waiting for several days without any news from the hospital (AMC). One of my friends introduced me to another hospital which successfully cured her relative with the same disease. Hence, I gave up waiting … (P11)
Lack of Knowledge About the Disease
The level of knowledge among patients regarding disease was low. For example, if symptoms improved slightly, patients began to wonder about the state of their illness, thinking it might not be as serious as they believed at first. In addition, some participants had no knowledge of their disease, so they readily believed people around them, or held blindly optimistic attitudes towards disease.
Patients’ Perception of Feasible Self-Solving Symptoms
If illness occurred, most participants described a sense of urgency in scheduling an appointment. However, once participants sensed a slight improvement in their health, they started to hesitate and wonder whether they should wait for the appointment, especially if several days had lapsed since scheduling the appointment with the AMC. In the interview, four participants mirrored this situation.
After taking the medication, I feel better than before and my pain is gone … the absence of pain made me wonder that maybe it is not that serious as the doctor described. Therefore, I did not ask for sick leave, and went back to work right away. (P20)
I feel much better after taking the medicine these days. That is why I want to cancel the appointment for now and try staying at home for observation.… If I continue to feel uncomfortable, then at that time I would consider to be hospitalized. (P14)
Readily Believe People Around Them
Another five patients disclosed that they had no knowledge of the cause, treatment, or outcome of their disease. As a result, they were misled readily by the opinions of their families or friends. They stopped listening to the opinion of the attending physician.
I had absolutely no idea what it was. Like a deer caught in the headlights when I got to know my conditions from the doctor … I was scared. Then I phoned one of my close friends who assured me that it was not that scary … she directed me to an herbalist in the end. (P21)
The lump was painful, at times, but my breast looked normal. Many friends of mine had the same symptoms as what I had. They said it was caused by endocrine disorder.… From that, I was not that worried anymore and I did not consider it as serious as the doctor said. (P12)
I had heard a little about the fact that tonsil is an immune organ. I informed my parents about the information from the doctor suggesting I have an operation. Surprisingly, they managed to dissuade me.… From where they stand, it is normal for someone to have chronic tonsillitis. There is no need for an operation if it comes with no severe consequences … (P17)
Blindly Optimistic Attitude Towards Disease
A lack of in-depth understanding about their disease meant that, as long as their condition did not affect their daily lives, patients would not be alert to the potential risks and severity of their disease. Thus, seven patients decided that there was no need to come to an inpatient treatment.
Isn’t it just colon polyps? It doesn’t matter whether you remove it or not, because it would still reappear after some time even if you did remove it before … (P5)
It has been a year since I first felt sick. The doctor recommended a surgery.… Isn’t it a common phenomenon that people suffer from tonsillitis? Besides, it hasn’t affected my life yet. (P23)
I just want to have a routine examination. But the doctor asked me to be hospitalized just for an angiogram. Why the fuss? I quite understand my condition. I suppose it is a little too much for this test … (P30)
Negative Emotional Response
Study participants dictated the thoughts and feelings they experienced previously. Ten participants stated explicitly that emotional barriers were the main causes holding back their attendance. These emotional barriers included: a sense of fear towards the surgical procedure; worries about future side effects of treatments; feeling of distrust towards the physician.
Sense of Fear
While selecting the optimal treatment, participants would measure the risks among different options. In general, surgery was considered the “last resort” because respondents were fearful of postoperative complications and sequelae. Hence, it is understandable that participants would become hesitant if physicians suggested a surgical procedure, and six participants felt this way.
I was scared by the idea that they might resect in the wrong site when I am unconscious under the anesthetic … (P22)
All I knew was that the surgery is horrible … the doctor was going to dig a hole in my brain. It could kill me at any time if the doctor himself is not good enough with the surgical skills.… I do not want to experience that.… I got panicked and scared … (P16)
I am anxious about the subsequent effects of the surgery.… As long as medicine can control it, I do not want to mention surgery. (P8)
Do you know how much a surgery can harm your body? You would potentially have to endure a series of surgical complications which could be extreme haunting.… If other options existed, I believe no one would go along with the surgery … (P26)
Lack of Trust
At the time of an initial visit, physicians may not provide adequate information or clear explanations to patients regarding their condition. Consequently, four patients suspected that the main purpose of the physician was to increase their personal income. This absence of trust in a relationship between physicians and patients was very destructive, and was another obstacle to attending an IA.
I have been to several hospitals.… Different doctors had different opinions about it. The doctor in other hospitals did not say that my condition was as serious as yours did. (P10)
I felt like the doctor deliberately stressed the potential consequences of my condition and meant to scare me a bit when they’re.… From my point of view, I did not consider it as something serious. (P17)
My test results have not come back to me yet, but the doctor had already asked me to be hospitalized.… Don’t you think in this case it sounds a bit odd? (P13)
Discussion
Identifying the reasons for not attending IAs is important to improve IA services, and subsequently improve the health and reduce the risk of morbidity and mortality of patients. Scholars have shown that the factors that determine treatment-seeking behaviors are complex and multifactorial, and can be influenced by socioeconomic status,13 perceived knowledge about the diseases,3 the influence of family members and others,14 and accessibility of services.3
We revealed that work obligations, family obligations, health conditions, and financial issues were the major barriers for attendance of IAs. The barriers determined in our study are largely consistent with those reported in studies conducted in primary-care clinics in Scotland, with the exception of financial issues.15,16 In primary-care clinics, medical expenses are not as high as those in the inpatient setting, so the financial issue might not be such a barrier for patients. For low-income families, undergoing hospitalization would undoubtedly be a heavy financial burden. Such patients would withstand any disease or health-related issues until they cannot bear it because they are afraid that undergoing inpatient treatment would result in them being absent from work. In general, people who have a low perception of the importance of health have demands that compete with attending IAs.3 Therefore, providing information about early treatment and the potential consequences of delaying treatment are important because they would allow patients to be more alert to their health condition and to take timely actions.17
We discovered that a long waiting time also contributed to non-attendance. Studies have demonstrated that a long wait for treatment has a detrimental effect on the appointment-keeping behaviors of patients.18,19 Indeed, a long waiting time can impose physical and psychological burdens upon individuals who are worried about the potential consequences of their health condition, and some could turn to other hospitals. One strategy to mitigate the psychological burden is to set up “waiting-time slots”.20 In this way, patients would be informed of the earliest admission time and latest admission time in advance. Hence, they would know precisely the time they need to wait and arrange their schedules reasonably before the appointment. If the patient has not been admitted to the hospital at the latest admission time, they could receive relevant compensation or preferential treatment, such as being transferred to private hospital wards. In general, bed utilization differs in different departments in tertiary hospitals. For example, some departments are always overcrowded, whereas others lay idle. The imbalance in utilization of bed resources has seriously affected hospital capacities, resulting in increasing numbers of patients waiting for an IA.21 A unified approach to manage and dispatch available beds in the entire hospital can help to balance the discrepancy of different departments and increase bed utilization.22,23 Patients with a serious disease would be given priority for hospital admission, thereby ensuring timely treatment for patients requiring urgent care.
Lack of knowledge about the disease contributed to non-attendance of IAs in the present study. This finding is similar to data from a study in Malaysia whereby, owing to non-recognition of symptoms, patients avoided medical guidance that led to delays in seeking treatment.24 In general, early treatment is pivotal to disease management.17 However, some participants in our study stressed that they were unwilling to attend health services if their health status did not affect their personal life. Confusingly, they blindly held an optimistic attitude towards their condition and did not realize that disease was threatening their health. They would seek treatment only if they were severely ill. Because they lacked knowledge about their disease, some participants felt confused when they first learnt about their condition from the attending physician. Hence, they tended to turn to their families/friends for help rather than physicians. This strategy could lead to inappropriate treatment-seeking behaviors through the sharing of experiences of families or friends. The factors that determined the path to seeking treatment were dependent upon the level of disease awareness: the more a patient knew about his/her disease, the more he/she took targeted measures.14,25 Hence, enhancing the health literacy of patients should be taken into consideration. Problems with comprehension and communication of medical recommendations could be tackled by enhancing the cultural awareness of medical staff.26
Our results raise questions about the delivery of medical services to patients fearful of what could happen after an IA. For such patients, negative emotional responses (eg, fear, anxiety, hesitancy) could explain the higher risk of not attending appointments. Owing to fears aggravated by health providers, some participants travelled back-and-forth in between several hospitals for further confirmation of the information received. A study conducted in the UK stated that some participants felt fearful before an appointment, worrying that they might receive bad news from the attending physician.15 Moreover, with surgery being seen as a last resort, most of the patients in our study were inclined to seek a traditional healer. Surgery was considered only if other treatments were not feasible practically. This finding was also demonstrated by Arumugam and colleagues: when a disease was perceived as threatening life, only then would a patient consider the advice of the attending physician.14 Any intervention to tackle this perception may need to be “tailored” to the individual.27
Our study had three main limitations. First, we detailed the perspectives of patients and not the views from medical professionals; the latter may have been privy to other vital information. Second, some family members replaced the patients to be interviewed, and these family members might not have been able to communicate adequately and provide the necessary information. Not considering the cause to attend a scheduled appointment was the third limitation of our study. A future study should focus on the most common findings from our study to formulate interventions to reduce non-attendance of IAs (eg, developing a queuing model to allocate beds).
Conclusions
Three main factors contributed to non-attendance of IAs: practical barriers, lack of knowledge about disease, and negative emotional response. Our study provides new, valuable evidence on non-attendance of IAs in China. Our findings could offer meaningful insights into developing effective strategies to reduce non-attendance of IAs in other countries.
Acknowledgments
We thank Xiaocong Li for critical review of this manuscript, providing language help, and writing assistance.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study was funded by the Health Commission of Guangdong Province (A2020436).
Disclosure
All authors declared no potential conflicts of interest.
References
1. Huang Y, Hanauer DA. Patient no-show predictive model development using multiple data sources for an effective overbooking approach. Appl Clin Inform. 2014;5(3):836–860. doi:10.4338/ACI-2014-04-RA-0026
2. Lacy NL, Paulman A, Reuter MD, Lovejoy B. Why we don’t come: patient perceptions on no-shows. Ann Fam Med. 2004;2(6):541–545. doi:10.1370/afm.123
3. Akter S, Doran F, Avila C, Nancarrow S. A qualitative study of staff perspectives of patient non-attendance in a regional primary healthcare setting. Australas Med J. 2014;7(5):218–226. doi:10.4066/AMJ.2014.2056
4. Fiorillo CE, Hughes AL, I‐Chen C. Factors associated with patient no-show rates in an academic otolaryngology practice. Laryngoscope. 2018;128(3):626–631.
5. Bonora E, Monami M, Bruno G, Zoppini G, Mannucci E. Attending diabetes clinics is associated with a lower all-cause mortality. A meta-analysis of observational studies performed in Italy. Nutr Metab Cardiovasc Dis. 2018;28(5):431–435. doi:10.1016/j.numecd.2018.02.009
6. Fahmy N, Aprikian A, Al-Otaibi M, et al. Impact of treatment delay in patients with bladder cancer managed with partial cystectomy in Quebec: a population-based study. Can Urol Assoc J. 2009;3(2):131–135. doi:10.5489/cuaj.1045
7. Nuti LA, Lawley M, Turkcan A, et al. No-shows to primary care appointments: subsequent acute care utilization among diabetic patients. BMC Health Serv Res. 2012;12:304. doi:10.1186/1472-6963-12-304
8. Bower P, Roland M, Campbell J, Mead N. Setting standards based on patients’ views on access and continuity: secondary analysis of data from the general practice assessment survey. BMJ. 2003;326(7383):258. doi:10.1136/bmj.326.7383.258
9. Pomerantz A, Cole BH, Watts BV, Weeks WB. Improving efficiency and access to mental health care: combining integrated care and advanced access. Gen Hosp Psychiatry. 2008;30(6):546–551. doi:10.1016/j.genhosppsych.2008.09.004
10. Xiaoyun Y, Zhang L. Analyzing the cause of Non-attendance at inpatient appointments in a large tertiary general hospital. Chin J Hosp Admin. 2016;32(8):589–591.
11. Lape EC, Katz JN, Losina E, Kerman HM, Gedman MA, Blauwet CA. Participant-reported benefits of involvement in an adaptive sports program: a qualitative study. PM R. 2018;10(5):507–515. doi:10.1016/j.pmrj.2017.10.008
12. Abalos EE, Rivera RY, Locsin RC, Schoenhofer SO. Husserlian phenomenology and Colaizzi’s method of data analysis: exemplar in qualitative nursing inquiry using nursing as caring theory. Int J Hum Caring. 2016;20(1):19–23.
13. Tsai WC, Lee WC, Chiang SC, Chen YC, Chen TJ. Factors of missed appointments at an academic medical center in Taiwan. J Chin Med Assoc. 2019;82(5):436–442. doi:10.1097/JCMA.0000000000000068
14. Arumugam P, Tengku Ismail TA, Daud A, et al. Treatment-seeking behavior among male civil servants in Northeastern Malaysia: a mixed-methods study. Int J Environ Res Public Health. 2020;17(8):2713. doi:10.3390/ijerph17082713
15. Eades C, Alexander H. A mixed-methods exploration of non-attendance at diabetes appointments using peer researchers. Health Expect. 2019;22(6):1260–1271. doi:10.1111/hex.12959
16. Samuels RC, Ward VL, Melvin P, et al. Missed appointments: factors contributing to high no-show rates in an urban pediatrics primary care clinic. Clin Pediatr (Phila). 2015;54(10):976–982. doi:10.1177/0009922815570613
17. Basharat S, Shaikh BT, Rashid HU, Rashid M. Health seeking behaviour, delayed presentation and its impact among oral cancer patients in Pakistan: a retrospective qualitative study. BMC Health Serv Res. 2019;19(1):715. doi:10.1186/s12913-019-4521-3
18. Rodríguez-García M, McLean-Carranza AA, Prado-Prado JC, Domínguez-Caamaño P. Managing waiting times to predict no-shows and cancelations at a children’s hospital. J Ind Eng Manag. 2016;9(5):1107–1118. doi:10.3926/jiem.2075
19. Ansell D, Crispo JAG, Simard B, Bjerre LM. Interventions to reduce wait times for primary care appointments: a systematic review. BMC Health Serv Res. 2017;17(1):295. doi:10.1186/s12913-017-2219-y
20. Luo J, Lu W. The problem of scheduling elective inpatients admission based on waiting time slots-a new type of appointment mode. Light Ind Sci Technol. 2019;35(09):
21. Luo L, Li J, Xu X, Shen W, Xiao L. A data-driven hybrid three-stage framework for hospital bed allocation: a case study in a large tertiary hospital in China. Comput Math Methods Med. 2019;2019:7370231. doi:10.1155/2019/7370231
22. Sæther SMM, Heggestad T, Heimdal J-H, Myrtveit M. Long waiting times for elective hospital care - breaking the vicious circle by abandoning prioritisation. Int J Health Policy Manag. 2020;9(3):96–107. doi:10.15171/ijhpm.2019.84
23. Lizi Wang L, Guo H, Zhong Q, et al. Practice and effect analysis of setting up the bed allocation center in a tertiary class-A hospital. Chin Hosp Manag. 2018;38(09):41–43.
24. Azhar N, Doss JG. Health-seeking behaviour and delayed presentation of oral cancer patients in a developing country: a qualitative study based on the self-regulatory model. Asian Pac J Cancer Prev. 2018;19(10):2935–2941.
25. Zhang N, Fielding R, Soong I, et al. Psychometric assessment of the Chinese version of the brief illness perception questionnaire in breast cancer survivors. PLoS One. 2017;12(3):e0174093. doi:10.1371/journal.pone.0174093
26. Safety ACo, Care QiH. Australian Safety and Quality Framework for Health Care. ACSQHC Sydney; 2010.
27. Vass A, Mitchell A, Dhurrkay Y. Health literacy and Australian indigenous peoples: an analysis of the role of language and worldview. Health Promot J Austr. 2011;22(1):33–37. doi:10.1071/HE11033
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.