")
Back to Journals » International Journal of General Medicine » Volume 14
Pulmonary Thromboembolism in Immune Thrombocytopenia: A Report of Five Cases and a Review of the Literature
Authors Tan Y, Yan M, Cheng Z, Pan X
Received 3 June 2021
Accepted for publication 22 July 2021
Published 13 August 2021 Volume 2021:14 Pages 4479—4483
DOI https://doi.org/10.2147/IJGM.S323146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yong Tan,* Min Yan,* Zhen Cheng,* Xiangtao Pan
Department of Haematology, The Taicang Hospital Affiliated of Soochow University, Taicang, 215400, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangtao Pan
Department of Haematology, The Taicang Hospital Affiliated of Soochow University, Taicang, 215400, Jiangsu, People’s Republic of China
Tel +86 18915768003
Email [email protected]
Objective: To provide a reference for the diagnosis and treatment of patients with immune thrombocytopenia (ITP) complicated with pulmonary thromboembolism (PTE) by analyzing the clinical characteristics of five such patients.
Methods: This paper summarizes the clinical manifestations and hematological indexes of five patients with ITP complicated with pulmonary embolism.
Results: In this study, the incidence of ITP complicated with PTE was 2.75%. All five cases were elderly patients with nonspecific clinical manifestations. Platelet counts were different when PTE occurred. The time from the diagnosis of ITP to the occurrence of PTE was from 5 to 24 months, with an average of 12.8 months. There was no significant change in hemoglobin, white blood cell levels, prothrombin time, activated partial thromboplastin time, thrombin time, fibrinogen levels, or the international normalized ratio. Four patients had significantly increased D-dimer levels, while D-dimer was only slightly increased in one patient. Antithrombin (AT) was significantly decreased in four cases (less than 70%), and C-reactive protein (CRP) was increased in all five cases.
Conclusion: PTE may be related to AT and CRP in patients with ITP, which is of great clinical significance to the diagnosis and treatment of ITP complicated with PTE.
Keywords: immune thrombocytopenia, pulmonary thromboembolism, C-reactive protein, antithrombin, prognosis
Introduction
Immune thrombocytopenia (ITP) is one of the commonest acquired autoimmune diseases. It is characterized by the autoantibody-mediated destruction of platelets (PLTs) and the impaired production of PLTs from megakaryocytes, and it is a common clinical hemorrhagic disease. However, an increased risk of thromboembolic events among patients with ITP has also been reported. In these reports, arterial thrombosis is more common than venous thrombosis, and pulmonary thromboembolism (PTE) is rare.1 PTE is a complex multifactorial disease caused by a perfusion defect as a result of an embolus blocking blood flow in the lungs or the right side of the heart. Pulmonary circulation changes and respiratory dysfunction are the main pathophysiological and clinical features. Its mortality rate is second only to myocardial infarction and cancer.2 Therefore, the diagnosis and treatment of ITP combined with PTE is of great clinical importance; five cases of patients with ITP who then developed PTE are presented herein.
Materials and Methods
Patients
The records of patients at Taicang Hospital of Soochow University during the five years from January 1, 2015 to December 31, 2019 were reviewed. There were 270,983 discharged hospital patients, 433 of whom had been diagnosed with PTE using computed tomography pulmonary angiogram (CTPA). Among them were five patients with ITP complicated with PTE: three males and two females, age range 68–88 years, and average age 78.6 years. All the cases were confirmed using CTPA combined with plasma D-dimer and color Doppler ultrasound to identify whether there was venous thrombosis of the extremities. The diagnosis of ITP was based on previous medical history, bone marrow analysis, hematology results, and other examination data in line with the criteria established by the ITP International Working Group.
Methods
The personal information of the enrolled patients was identified using the case management computer system of Taicang Hospital of Soochow University and included medical record number, name, gender, age, inpatient department, primary disease, inducement factor, occurrence site, preventive measures, relevant examination results, treatment, and prognosis. Eighteen healthy subjects were included as a control group to allow comparison with the hematological indicators of the patients.
Statistical Analysis
Data were analyzed using SPSS 19.0 software. The Chi-square test and the t-test were used, and a value of p < 0.05 was considered to be statistically significant.
Results
The Incidence of ITP Combined with PTE
In the hospital, there were 433 concurrent inpatients with PTE and 182 with ITP. Patients diagnosed with ITP combined with PTE accounted for 1.16% of the total number of PTE cases and 2.75% of all ITP cases.
The Demographics and Main Clinical Features of the Five Patients
The PTEs occurred in different sites: there were two in the bilateral pulmonary artery, one in the right lower lung, one in the right middle lobe, and one in the left upper pulmonary artery. Only one of the five patients, a 77-year-old female, had a PTE combined with a deep venous thrombosis (DVT) of the left leg. The five patients also experienced different symptoms: two patients presented with cough and shortness of breath, one with cough and fever, one with poor appetite and fatigue, and one with shortness of breath and black stools. The main clinical features of the five patients are shown in Table 1.
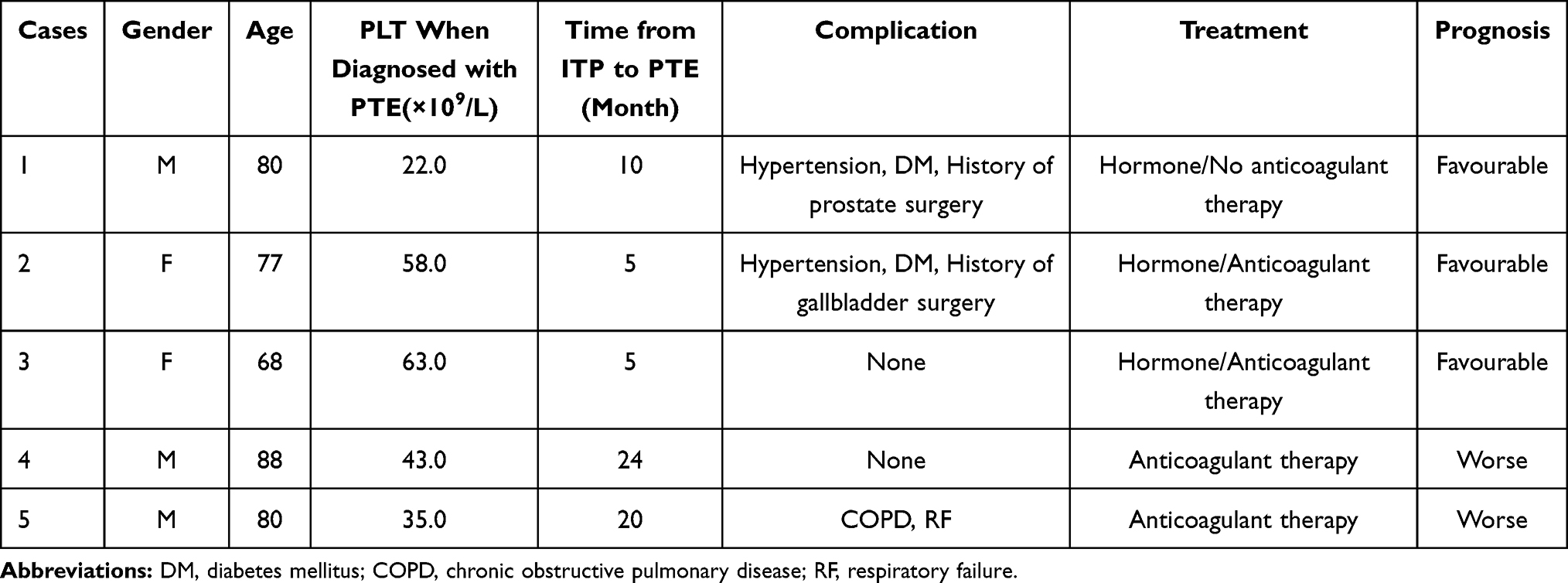 |
Table 1 Main Clinical Features of 5 Patients |
Hematological Indicators of the Five Patients
Antinuclear antibody and antiphospholipid antibody (APA) tests were negative in all five patients. The results of other hematological and coagulation indices are shown in Table 2. The comparison of hematological indices between the case group and the control group are shown in Table 3.
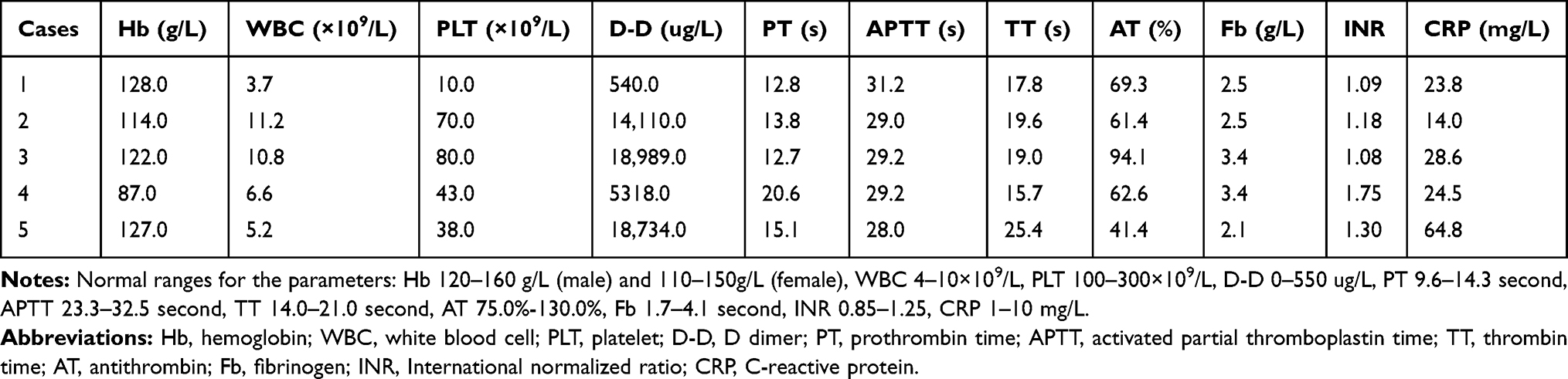 |
Table 2 Results of Hematology and Coagulation Indexes in 5 Patients |
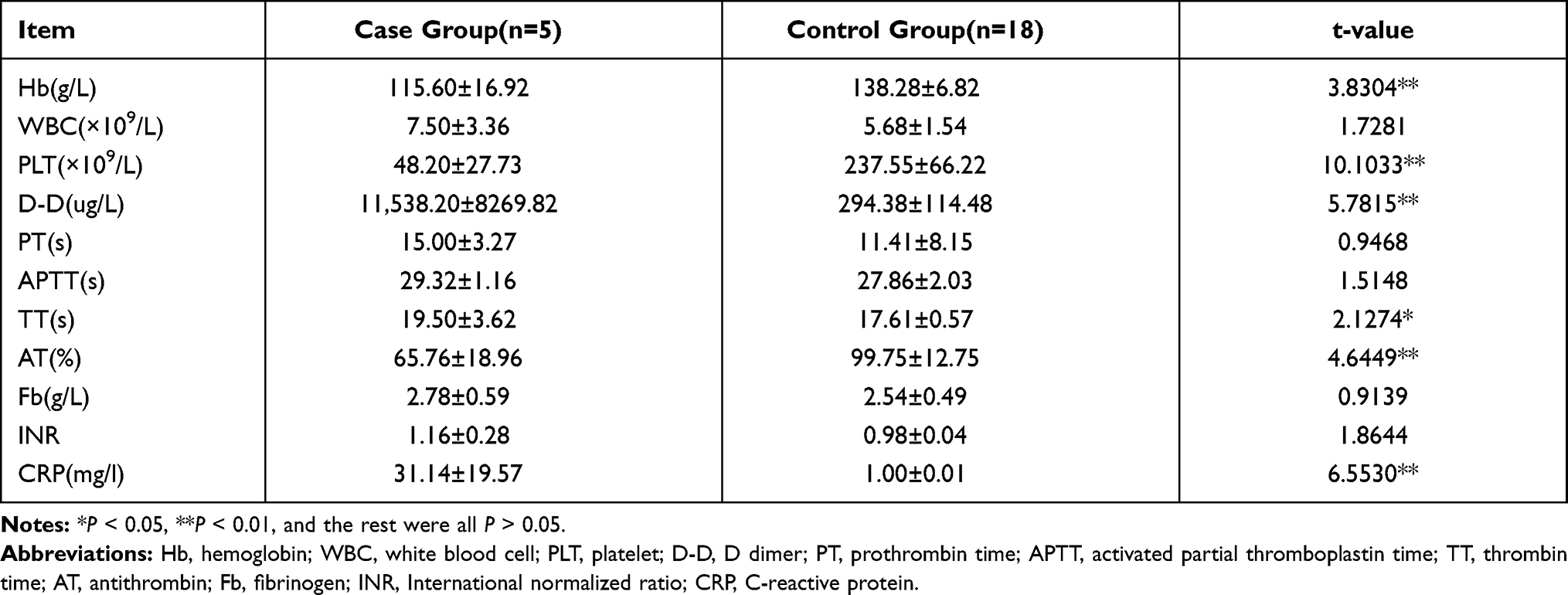 |
Table 3 The Results of All Indexes Compared Between the Case Group and the Normal Control |
Discussion
ITP is a chronic disease characterized by a low PLT count and bleeding. However, an increased thrombotic tendency has been identified in ITP patients in recent years. A meta-analysis of five large population-based studies established that there is a two-fold increased risk of venous thromboembolism (VTE) and a trend towards an increased risk of antithrombin (AT) in ITP as compared with the general population.2 The exact incidence of thrombosis in ITP is not clear, but most scholars believe that the risk of thrombosis is higher in the presence of ITP than in the general population.3,4 Aledort reported close to 5.1% of cancer patients with a high incidence of thrombosis.5 Bennett et al reported that chronic ITP was 6.9%.6 The incidence of ITP combined with PTE in this study was only 2.75% (5/182 cases), lower than that reported above. Two possible explanations are: (1) this review only included cases of ITP combined with PTE as opposed to all cases of thrombosis in general, and (2) some ITP patients may have been lost to follow-up.
The clinical manifestations showed no specificity. While all five cases involved elderly patients, the PLT counts when PTE occurred were different: some were higher than 50.0 × 109/L, while others were lower than 50.0 × 109/L. The time from ITP diagnosis to PTE onset was between 5 and 24 months, with an average of 12.8 months. Some researchers7,8 believe that APA, splenectomy, hormone, globulin, and other therapeutic interventions are high-risk factors for PTE occurrence in ITP patients. In this study, some of the five ITP patients had high-risk factors such as hypertension, diabetes mellitus, surgical history, infection, and hormone application, but there were also some without complications. Prognosis was not always related to anticoagulant therapy: in this study, one patient recovered without anticoagulant therapy due to a low PLT count, while two other patients deteriorated despite receiving anticoagulant therapy. Therefore, prognosis may be related to the occurrence and speed of onset of PTE, the location and extent of the embolism, and the severity of the primary disease.
The pathogenesis of ITP combined with thrombosis is multifactorial and possible mechanisms include the following: (1) PLTs release microparticles (MPs) that can activate the coagulation cascade.9–11 In fact, PLT-derived microparticles (PMPs) are 50–100 times more procoagulant than those on the PLT surface membrane. In addition, PMPs are potentially thrombogenic due to their high content of large von Willebrand factor multimers that play an important role in coagulation and PLT aggregation. One study found that 21% of ITP patients had MPs, mainly PMPs, and this could explain the increased risk of thrombosis and reduced bleeding tendency seen in some ITP patients;12 (2) APA promotes PLT activation and aggregation and releases PMPs,11 thus increasing the risk of thrombosis.13 The proportion of APA in ITP patients ranges from 8.6% to 73%;14 (3) activation of the complement system mediates the generation of MPs;15 (4) treatment-related factors: intravenous immunoglobulin can not only increase blood viscosity and lead to hypercoagulability, but it can also reversibly increase vascular tension and induce arterial vasospasm. This may destroy atherosclerotic plaques and lead to intimal injury, in situ thrombosis, and arterial occlusion.16 Heavy use of glucocorticoids can also increase blood viscosity and result in a hypercoagulable state that can induce thrombosis. Danazol promotes thrombosis by increasing PLTs to produce thromboxane A2 or decreasing PLTs to produce prostaglandin I2.17 Splenectomy results in an increased risk of thrombosis due to an increase in MP levels;18 and (5) ITP per se is a thrombophilic condition, which is largely attributable to the presence of younger PLTs with a greater thrombogenic potential.14 There were no particular changes in hemoglobin or white blood cell levels, prothrombin time, activated partial thromboplastin time, thrombin time, fibrinogen levels, or the international normalized ratio. One patient had a slightly higher D-dimer, while the D-dimers in the other four patients were significantly increased. AT was significantly decreased in four cases (less than 70.0%), and C-reactive protein (CRP) was increased in all five cases. This suggests that the occurrence of PTE may have an important relationship with AT and CRP. Some researchers believe that CRP is associated with arterial thrombosis, while the relationship with VTE remains unclear.19 However, other studies have suggested that both AT and CRP have a strong relationship with the occurrence and development of PTE. For example, Esmon et al20 found that the increase in CRP resulted in a decrease in AT, while the decrease in AT reduced anticoagulant activity, one of the reasons for the hypercoagulable state leading to DVT.21 In immune diseases, inflammatory stimulants such as CRP and tumor necrosis factor can promote clotting, leading to elevated clotting factor levels and DVT formation.22,23 In general, multiple factors and mechanisms combine in the development of PTE in ITP patients. A reduction in PLTs due to disease or other factors cannot prevent PTE from occurring.24–26 Survival was also associated with bleeding rather than thrombosis.27
For patients diagnosed with ITP combined with PTE, identifying both the appropriate treatment for the primary ITP along with anticoagulant therapy for PTE is of great importance. It is recommended that ITP patients should have a PLT count of at least 50.0 × 109/L during anticoagulation therapy.15 Patients with a PLT count ≥ 50.0 × 109/L can receive full-dose low molecular weight heparin (LMWH) anticoagulation therapy, while patients with a PLT count <50.0 × 109/L can receive half-dose LMWH anticoagulation therapy at first, increasing to full-dose anticoagulation once the PLT count exceeds 50.0 × 109/L.17 A multicenter retrospective study of patients with ITP combined with VTE suggested that long-term anticoagulation is beneficial for ITP patients with unexplained VTE or recurrent VTE. In addition, adequate corticosteroid therapy for ITP can maintain a PLT count of 30.0–50.0 × 109/L, and patients can be safely treated with anticoagulation therapy without the risk of bleeding increasing.16
In conclusion, ITP complicated with PTE has multiple causes, meaning that it is not clinically easy to detect or prevent it early on, and it can even be missed. Consequently, it is necessary to conduct in-depth research on such patients in order to improve their prognosis, cure, and survival rates.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Taicang Hospital Affiliated of Soochow University (2021-KY-154) and informed consent was taken from all the patients.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rodeghiero F. Is ITP a thrombophilic disorder? Am J Hematol. 2016;91(1):39–45. doi:10.1002/ajh.24234
2. Kraaijpoel N, Tritschler T, Guillo E, Girard P, Le Gal G. Definitions, adjudication, and reporting of pulmonary embolism-related death in clinical studies: a systematic review. J Thromb Haemost. 2019;17(10):1590–1607. doi:10.1111/jth.14570
3. Feudjo-Tepie MA, Le Roux G, Beach KJ, Bennett D, Robinson NJ. Comorbidities of idiopathic thrombocytopenic purpura: a population-based study. Adv Hematol. 2009;2009:963506. doi:10.1155/2009/963506
4. Feudjo-Tepie MA, Hall SA, Logie J, Robinson NJ. Risk of cataract among idiopathic thrombocytopenic purpura patients in the UK general practice research database. Pharmacoepidemiol Drug Saf. 2009;18(5):380–385. doi:10.1002/pds.1723
5. Aledort LM, Hayward CP, Chen MG, Nichol JL, Bussel J; ITP Study Group. Prospective screening of 205 patients with ITP, including diagnosis, serological markers, and the relationship between platelet counts, endogenous thrombopoietin, and circulating antithrombopoietin antibodies. Am J Hematol. 2004;76(3):205–213. doi:10.1002/ajh.20104
6. Bennett D, Forssen U, Enger C, et al. Risk of thromboembolic events(TE) among patients with chronic idiopathic thrombocytopenic purpura (ITP). Haematologica. 2008;93(Supplement1):125.
7. Kojouri K, Vesely SK, Terrell DR, George JN. Splenectomy for adult patients with idiopathic thrombocytopenic purpura: a systematic review to assess long-term platelet count responses, prediction of response, and surgical complications. Blood. 2004;104(9):2623–2634. doi:10.1182/blood-2004-03-1168
8. Wittstock M, Benecke R, Zettl UK. Therapy with intravenous immunoglobulins: complications and side-effects. Eur Neurol. 2003;50(3):172–175. doi:10.1159/000073059
9. Mause SF, Weber C. Microparticles: protagonists of a novel communication network for intercellular information exchange. Circ Res. 2010;107(9):1047–1057. doi:10.1161/CIRCRESAHA.110.226456
10. Owens AP, Mackman N. Microparticles in hemostasis and thrombosis. Circ Res. 2011;108(10):1284–1297. doi:10.1161/CIRCRESAHA.110.233056
11. Krajewska-Włodarczyk M, Owczarczyk-Saczonek A, Żuber Z, Wojtkiewicz M, Wojtkiewicz J. Role of microparticles in the pathogenesis of inflammatory joint diseases. Int J Mol Sci. 2019;20(21):5453. doi:10.3390/ijms20215453
12. Wong RS, Bakshi K, Brainsky A. Thrombophilia in patients with chronic immune thrombocytopenia. Scand J Clin Lab Invest. 2015;75(1):13–17. doi:10.3109/00365513.2014.962597
13. Moulis G, Audemard-Verger A, Arnaud L, et al. Risk of thrombosis in patients with primary immune thrombocytopenia and antiphospholipid antibodies: a systematic review and meta-analysis. Autoimmun Rev. 2016;15(3):203–209. doi:10.1016/j.autrev.2015.11.001
14. Jain A, Saluja S, Chaudhry S, Gupta DK. Recurrent arterial and venous thrombosis in chronic immune thrombocytopenia: clinical paradox and therapeutic challenges. Indian J Hematol Blood Transfus. 2019;35(3):590–592. doi:10.1007/s12288-019-01136-3
15. Najaoui A, Bakchoul T, Stoy J, et al. Autoantibody-mediated complement activation on platelets is a common finding in patients with immune thrombocytopenic purpura (ITP). Eur J Haematol. 2012;88(2):167–174. doi:10.1111/j.1600-0609.2011.01718.x
16. Paran D, Herishanu Y, Elkayam O, Shopin L, Ben-Ami R. Venous and arterial thrombosis following administration of intravenous immunoglobulins. Blood Coagul Fibrinolysis. 2005;16(5):313–318. doi:10.1097/01.mbc.0000172694.85233.a8
17. Alvarado RG, Liu JY, Zwolak RM. Danazol and limb-threatening arterial thrombosis: two case reports. J Vasc Surg. 2001;34(6):1123–1126. doi:10.1067/mva.2001.118078
18. Fontana V, Jy W, Ahn ER, et al. Increased procoagulant cell-derived microparticles (C-MP) in splenectomized patients with ITP. Thromb Res. 2008;122(5):599–603. doi:10.1016/j.thromres.2007.12.022
19. Lippi G, Favaloro EJ, Montagnana M, Franchini M. C-reactive protein and venous thromboembolism: causal or casual association? Clin Chem Lab Med. 2010;48(12):1693–1701. doi:10.1515/CCLM.2010.335
20. Esmon CT. Inflammation and thrombosis. J Thromb Haemost. 2003;1(7):1343–1348. doi:10.1046/j.1538-7836.2003.00261.x
21. Croles FN, Borjas-Howard J, Nasserinejad K, Leebeek FWG, Meijer K. Risk of venous thrombosis in antithrombin deficiency: a systematic review and Bayesian meta-analysis. Semin Thromb Hemost. 2018;44(4):315–326. doi:10.1055/s-0038-1625983
22. Tamaki H, Khasnis A. Venous thromboembolism in systemic autoimmune diseases: a narrative review with emphasis on primary systemic vasculitides. Vasc Med. 2015;20(4):369–376. doi:10.1177/1358863X15573838
23. Falanga A, Marchetti M. Thrombosis in myeloproliferative neoplasms. Semin Thromb Hemost. 2014;40(3):348–358. doi:10.1055/s-0034-1370794
24. Kopolovic I, Lee AY, Wu C. Management and outcomes of cancer-associated venous thromboembolism in patients with concomitant thrombocytopenia: a retrospective cohort study. Ann Hematol. 2015;94(2):329–336. doi:10.1007/s00277-014-2198-6
25. Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100(10):3484–3488. doi:10.1182/blood-2002-01-0108
26. Labrador J, Lopez-Anglada L, Perez-Lopez E, et al. Analysis of incidence, risk factors and clinical outcome of thromboembolic and bleeding events in 431 allogeneic hematopoietic stem cell transplantation recipients. Haematologica. 2013;98(3):437–443. doi:10.3324/haematol.2012.069559
27. Houghton DE, Key NS, Zakai NA, Laux JP, Shea TC, Moll S. Analysis of anticoagulation strategies for venous thromboembolism during severe thrombocytopenia in patients with hematologic malignancies: a retrospective cohort. Leuk Lymphoma. 2017;58(11):2573–2581. doi:10.1080/10428194.2017.1306644
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.