")
Back to Journals » International Journal of General Medicine » Volume 13
Public Perceptions and Commitment to Social Distancing “Staying-at-Home” During COVID-19 Pandemic: A National Survey in Saudi Arabia
Authors Aldarhami A , Bazaid AS , Althomali OW, Binsaleh NK
Received 27 June 2020
Accepted for publication 8 September 2020
Published 22 September 2020 Volume 2020:13 Pages 677—686
DOI https://doi.org/10.2147/IJGM.S269716
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Abdu Aldarhami,1 Abdulrahman S Bazaid,2 Omar W Althomali,2 Naif K Binsaleh2
1Clinical Laboratory Sciences Department, Turabah University College, Taif University, Turabah, Saudi Arabia; 2College of Applied Medical Sciences, University of Ha’il, Ha’il, Saudi Arabia
Correspondence: Abdu Aldarhami
Clinical Laboratory Sciences Department, Turabah University College, Taif University, Turabah, Saudi Arabia
Tel +966(0)128224366
Email [email protected]
Objective: Social distancing measures, such as stay-at-home, are currently implemented to control the COVID-19 pandemic in many countries, including Saudi Arabia. The aim of this study was, therefore, to evaluate the awareness and adherence of the Saudi population to these measures.
Methods: A web-based questionnaire was designed with 16 questions (eight questions related to demographics, three related to the awareness of social distancing (stay-at-home) and five related to the overall practice of social distancing).
Results: A total of 5105 participants completed the survey [58.4% females, 66.3% young individuals (aged 18– 37 years), 55.8% bachelor degree holders and 51.0% from the western region]. The Saudi Ministry of Health (MOH) was the main source of information about COVID-19 for most of the participants (78.2%). High awareness (81.3%) regarding stay-at-home was observed, associated mainly with female participants, those from the middle region and those with a high education and income. The overall implementation of social distancing was satisfactory (score 3.13/5), with 37.8% never leaving home during the stay-at-home period. Better adherence to social distancing was observed among female participants, higher degree holders and those aged over 38 years.
Conclusion: Organised plans by the Saudi MOH have been effective in raising awareness and improving the practice of social distancing among public. However, the observed lower practice of social distancing by individuals with a lower education and income indicates the need for targeted interventions to achieve better outcomes.
Keywords: COVID-19, SARS-CoV2, public awareness, public practice, social distancing, Saudi Arabia
Plain Language Summary
The World health organization (WHO) has advised the public to stay-at-home to control the spread of the COVID-19 pandemic. The aim of this study is to assess the level of understanding and practices of the Saudi population regarding the stay-at-home strategy. We designed a questionnaire consisting of 16 questions to assess the participants’ overall awareness and practice regarding this action. About 5105 individuals completed the survey and their level of awareness about the importance of staying at home was high. However, their practice was not as high as their knowledge, especially people with less money and low education. This means that the local ministry of health has successfully raised the knowledge of most Saudi people, but people with poor practices need special attention for better results. This is because a good knowledge and practice of staying at home by the general population should be enough to contain the spread of this viral infection in a short time, both nationally and internationally.
Introduction
In late December 2019, a novel strain of Coronavirus emerged, which was first reported as a national outbreak in Wuhan, China.1,2 Subsequently, this disease was designated as Coronavirus Disease 2019 (COVID-19), which is caused by the severe acute respiratory syndrome, coronavirus 2 (SARS-CoV-2).3 The wide spread of the disease since then led the WHO to announce COVID-19 as a pandemic on March 11th, 2020.4 To date (June 25th, 2020), SARS-CoV-2 has caused over nine million cases and 480,000 deaths globally.5 In addition to its lack of effective vaccines or treatments, SARS-CoV-2 has high infectivity even before the onset of symptoms, which can take up to 14 days to manifest,2,6 during which time transmission is possible.1,2,7 Consequently, this pandemic has been announced as a high concern for health, with containing its spread worldwide proving an extremely challenging task.1,8 Currently, health authorities are left with only preventive measures to tackle the spread of the pandemic.1,9
A few measures, such as social distance, self-isolation, home-isolation and self-quarantine, have been introduced as feasible precautionary steps that can be implemented to limit, delay or flatten the reproduction rate (R0) of SARS-CoV-2.7,10 These terms have showed up more frequently in the media and various scientific publications.11–13 The exact definition of such terms overlap as they generally share similar meanings, which can emphasise the physical separation or distance between healthy people and individuals with confirmed or suspected infection.2,7,9 Social distancing measures were used in the past to combat the spread of other viral and bacterial contagions, including the plague and Severe Acute Respiratory Syndrome (SARS).14 Implementing these measures and precautions in the current SARS-CoV-2 pandemic has proven effective in controlling or containing this infection in China and other far eastern countries.7
Even before the first confirmed case of COVID-19 in the Kingdom of Saudi Arabia (KSA), the national authority closed shopping centres and suspended flights, face-to-face education and physical attendance at most governmental agencies as preventive steps.6 Further precautions followed, entailing suspending prayers at mosques and implementing a lockdown in cities with high numbers of cases.6,15 This aimed to limit the population’s mobility and minimise social gatherings in order to control transmission. Nevertheless, to date (June 25th, 2020), the statistics have reported over 170,000 cases and 1428 deaths in KSA and the numbers are continuing to rise.16 Therefore, in order to confirm whether preventive steps have been successfully implemented in KSA, the overall understanding and adherence of the general public to physical separation should be evaluated. Likewise, it is crucial to ensure that the public can access information about preventive measures from trusted agencies. Hence, the aim of the current study was to evaluate the awareness and practices of the Saudi population in relation to social distancing (stay-at-home).
Materials and Methods
Study Design and Setting
A cross-sectional, observational study was conducted to evaluate the overall awareness and adherence of the Saudi population to social distancing to control the spread of COVID-19. The survey tool was written in Arabic, the mother tongue of the target population, and was built using an online survey form. To ensure a wide distribution, the dissemination to the target participants was carried out using various social media (Twitter, WhatsApp and Snapchat) between March 25th and April 17th, 2020. The questionnaire included introductory information to inform the participants about the purpose of the study and consent information to ensure that participation in the study was voluntary, while ensuring the confidentiality of personal data. Participants under 18 years were excluded from this study.
The questionnaire was created according to novel coronavirus (2019-nCoV) infection guidelines.17 To ensure the accuracy of the collected information, multiple choice and close-ended questions were used in this study. Used language for this questionnaire was validated by five multidisciplinary experts to suit the target participants. The resulting pre-final survey was piloted with 20 individuals from the general population of different ages and genders to address any ambiguity in the questions and assess the extent to which these questions are related to the objectives of this study. The questionnaire was then edited based on the collected feedback, which was used to prepare a final version for the study.
Measurement
The final questionnaire contained 16 questions, divided into three sections. The first covered the demographics of the participants (age, gender, monthly income, education level, marital status, occupation and geographical region of residence). The second covered their main sources of information about COVID-19 (the MOH, the WHO, friends and relatives or social media), their understanding of who should stay-at-home during the pandemic (the elderly, children, symptomatic people or the whole population), as well as their beliefs about the possibility of asymptomatic transmission. The final section comprised five questions (Supplement 1) about the practices of the participants in relation to social distancing. This included questions about their reasons for going out (work, buying necessities, purchasing a meal or entertainment), the amount of time spent outside the home (the number of days per week and hours per day), and their practices when leaving home (whether they leave alone or with others).
Scoring System and Statistical Analysis
The responses provided by the participants to each question were given designated scores; one point [1] for the most appropriate answer and no points [0] for the least appropriate or uncertain (I do not know) responses (Supplement 1). The collected responses to the questions intended to measure adherence to the stay-at-home strategy were scored as a quarter [0.25], half [0.5] or one [1] point for responses of two hours spent outside, less than one hour outside or never leaving the home, respectively. All of the statistical analyses were performed using SPSS software version 25.0 (IBM Corp, Armonk, NY). The numbers of participants, their percentages, the mean, standard deviation (SD) and the median in relation to the variables describing their knowledge and practices were assessed using descriptive analysis. The overall scores related to their practices were analysed based on their demographic characteristics using a one-way analysis of variance (ANOVA) and independent sample t-test for normally distributed data, while Kruskal–Wallis and Mann–Whitney tests were used for the non-parametric analysis.18 Questions testing knowledge were analysed using the Chi-square or Fisher’s Exact Test to determine whether there were significant differences between the responses in relation to the participants’ demographic characteristics.
Multivariable linear regression was used to identify the factors associated with the overall scores for the participants’ practices, which were determined using the stepwise method. To quantify the relationship between the variables, the odds ratios (ORs), unstandardized regression coefficients and 95% confidence intervals (CIs) were calculated. A two-steps analysis was conducted to avoid any multicollinearity between the independent variables; first, we checked that the correlation coefficients between the independent variables were below 0.7 and, second, that the tolerance and variance inflation factor (VIF) values were higher than 0.1 and 10, respectively. Statistical significance was defined by a p-value below 0.05. The maximum score assigned to individuals with perfect adherence to the stay-at-home strategy was 5. To ensure the reliability and reproducibility of the questionnaire, the Cronbach’s alpha was conducted, which scored 0.81, indicating a very good level of internal consistency between the questions.
Results
Demographic Characteristics of the Participants
A total of 5,105 participants completed the survey, of whom 58.4% were female, and most were young individuals (29.4% and 36.9% from the 18–27 and 28–37 years age groups, respectively) and married (60.9%). In addition, the contributors to this survey were mainly bachelor degree holders (55.8%), employees (45.2%), with low income (40.9%), living in western Saudi Arabia (51%) and residents of cities (93.8%) (Supplement 2).
Awareness of the Saudi Population About COVID-19
The participants were asked about their sources of information about COVID-19 to determine the most widely used sources by the Saudi population. About 78% and 49% of the participants selected the Saudi MOH and social medial as their main sources of knowledge, respectively. Seeking information about COVID-19 from friends, colleagues or relatives was the least favoured source used by the Saudi participants (Table 1).
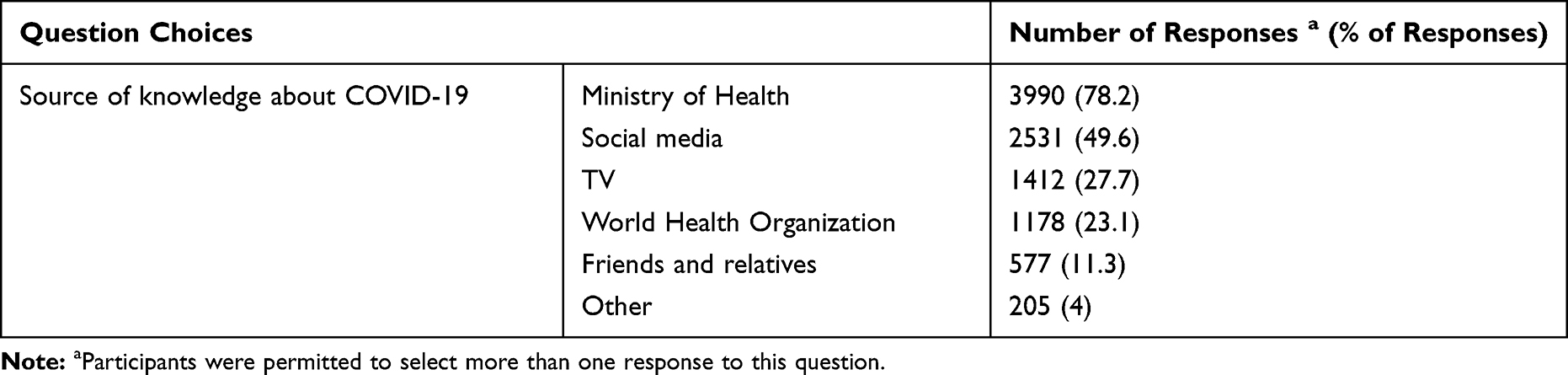 |
Table 1 Responses of Participants to the Question About the Sources They Used to Obtain Information and Updates About the COVID-19 Pandemic |
The participants expressed their views about social distancing. The majority (94.7%) were of the view that “everyone” should observe social distancing as a preventive measure, and most expressed a belief that asymptomatic transmission was possible (85.2%). This translates into an 81.3% awareness, based on both items taken together (Table 2). The multiple logistic regression analysis (Table 3) showed that females (OR 1.779, p < 0.001) and participants from the middle region (OR 1.549, p = 0.007) were considerably more likely to choose the appropriate response to the question about social distancing. In contrast, participants from the 38–47 years age group (OR 0.705, p = 0.014) and those with a secondary education or below (OR 0.561, p < 0.001) were less likely to choose the appropriate response to the question. Likewise, participants with higher educational levels (Master or PhD; OR 2.28, p < 0.001) and those with high income (>20,000 SR; OR 1.787, p = 0.017) were more aware of the likelihood of the risk of the asymptomatic transmission of COVID-19 (Table 3). In contrast, a lack of awareness about asymptomatic transmission was found to be associated with participants from the southern part of the Kingdom (OR 0.671, p = 0.01), those with a secondary and below educational level (OR 0.452, p < 0.001), diploma holders (OR 0.712, p = 0.011) and those with a low income (<3000 SR) (OR 0.74, p < 0.001) (Table 3).
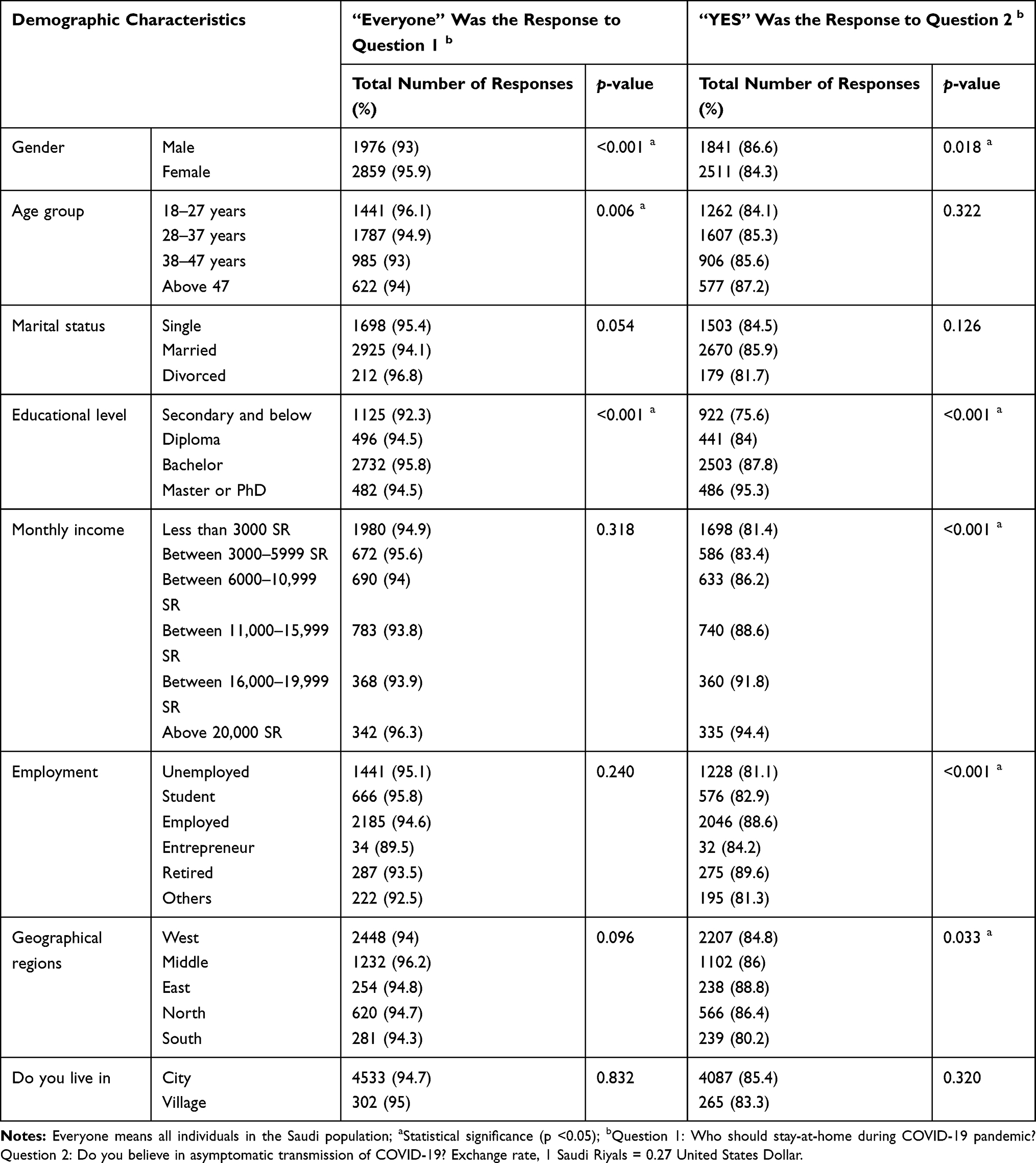 |
Table 2 Responses of the Participants to Two Questions About Knowledge Regarding Social Distancing and Awareness About Asymptomatic Transmission of COVID-19 |
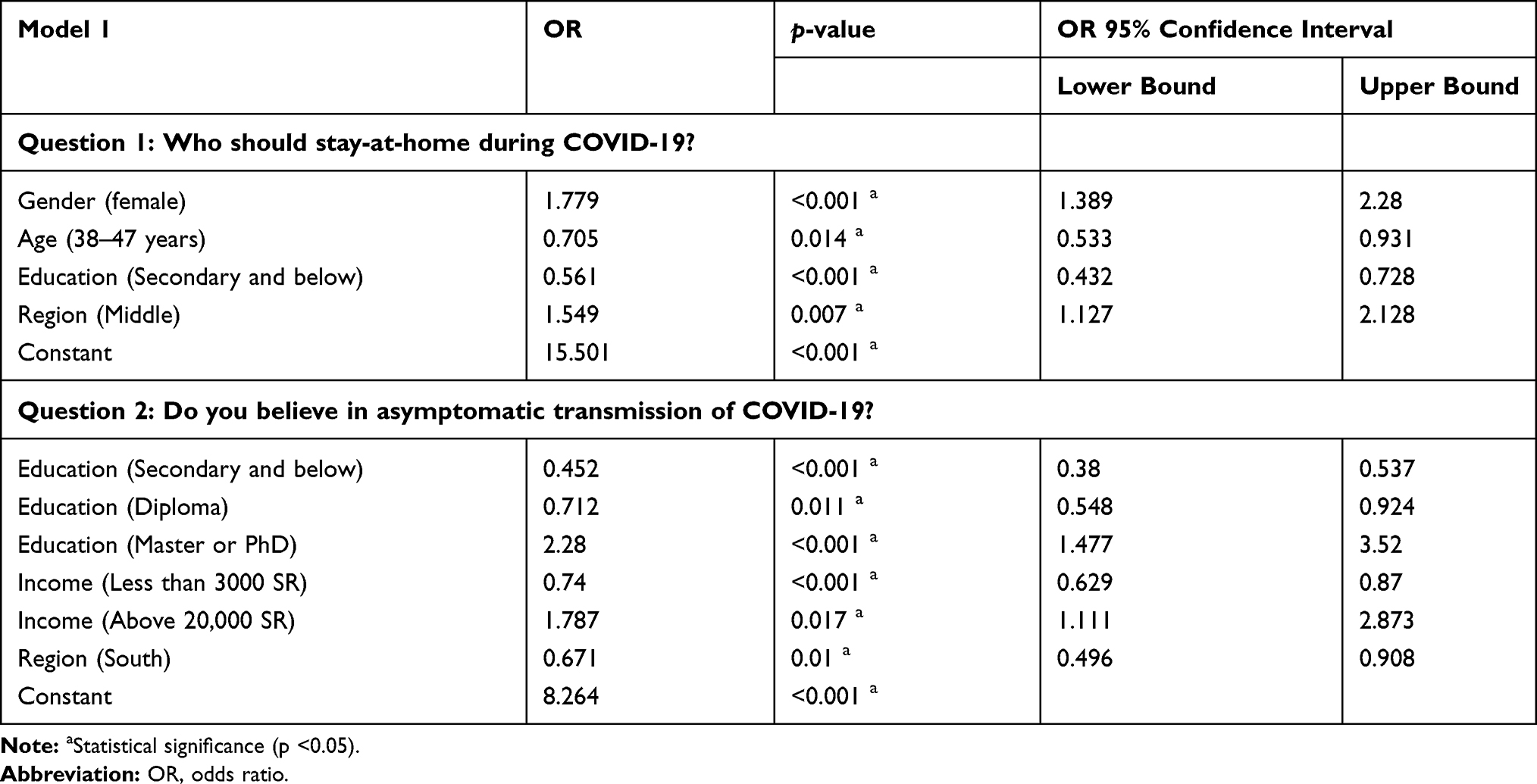 |
Table 3 Multiple Logistic Regression Analysis on Demographic Characteristics Associated with Responses to Two Questions About Knowledge Regarding Social Distancing and Awareness About Asymptomatic Transmission of COVID-19 |
Practice of Social Distancing Among the Saudi Population
The practice of the participants was scored based on Supplement 1; a summary of the scores in relation to demographics is shown in Table 4 and the results of the regression analysis are shown in Table 5. The average score of the respondents was approximately 3.13 (SD 1.38, range 0–5), representing a 62.6% implementation. However, just over a third (37.8%) of the participants confirmed that they had never left home since social distancing was introduced (Table 6). Females (β 0.969, p < 0.001), Master or PhD holders (β 0.190, p = 0.002), people from the 38–47 years age group (β 0.108, p = 0.016) and individuals over 47 years (β 0.316, p < 0.001) were associated with a higher score (Table 5). In contrast, participants with a low income (3000–5999 SR, β −0.175, p = 0.001), employees (β −0.438, p < 0.001), entrepreneurs (β −0.561, p = 0.006), retired participants (β −0.237, p = 0.011) and residents in the south (β −0.180, p = 0.018) or north (β −0.302, p < 0.001) of the Kingdom were associated with a lower score (Table 5). Almost half (46.9%) of the participants went out to buy necessities, whereas going to work or a hospital was the reason for leaving home for almost 13% of the respondents. In addition, nearly a third (30%) and about a quarter (24%) of the participants stated that they spent one day per week and less than an hour per day outside, respectively. Approximately one in five of the respondents acknowledged that they left their home 2–3 days a week for a total time of 1–2 hours per day. In the context of practicing social distancing, about 41% of the participants went out alone, while 19% were accompanied by another adult (Table 6).
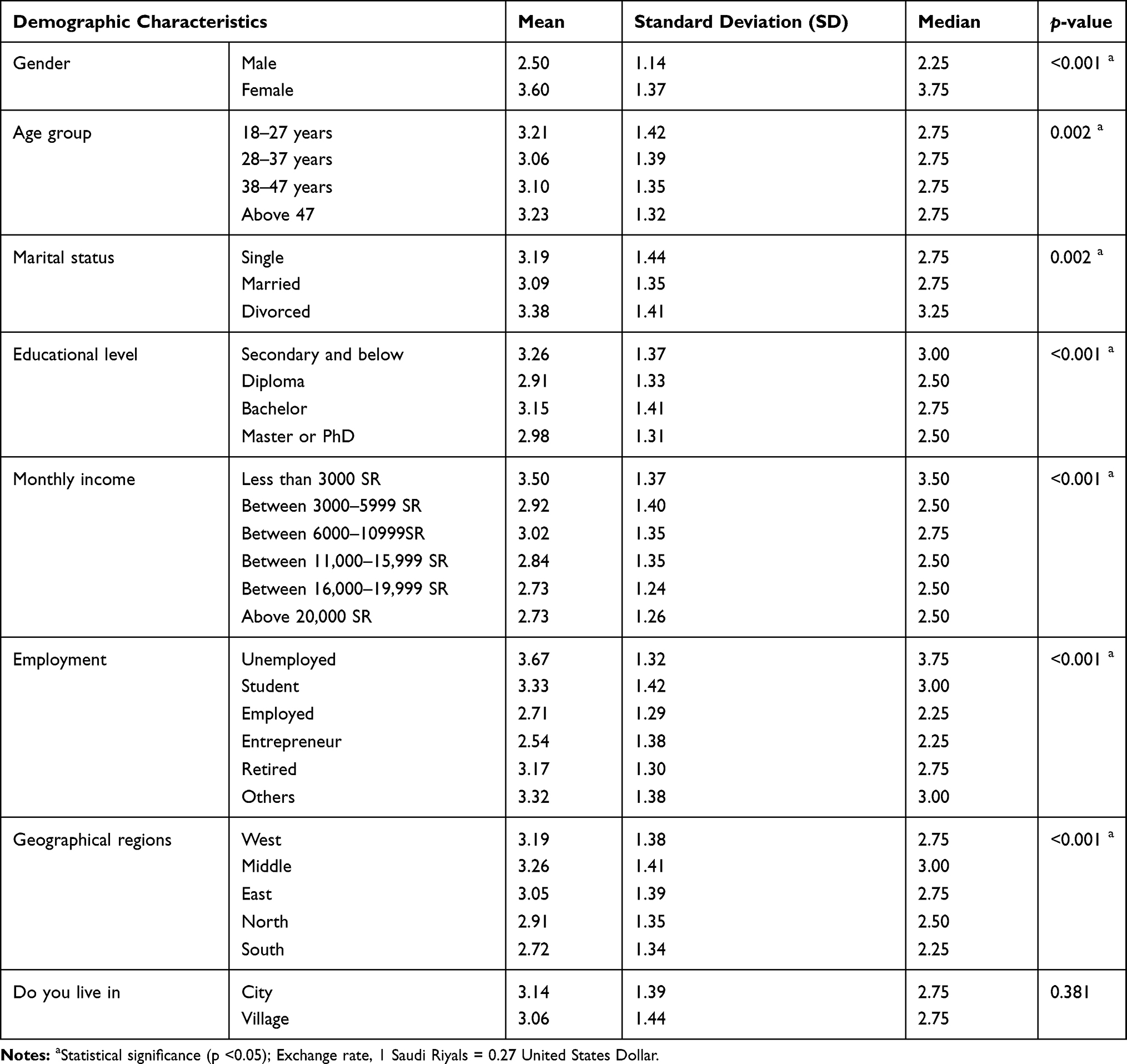 |
Table 4 Total Scores of Participants in Relation to Practicing Staying Home Strategy During the COVID-19 Pandemic |
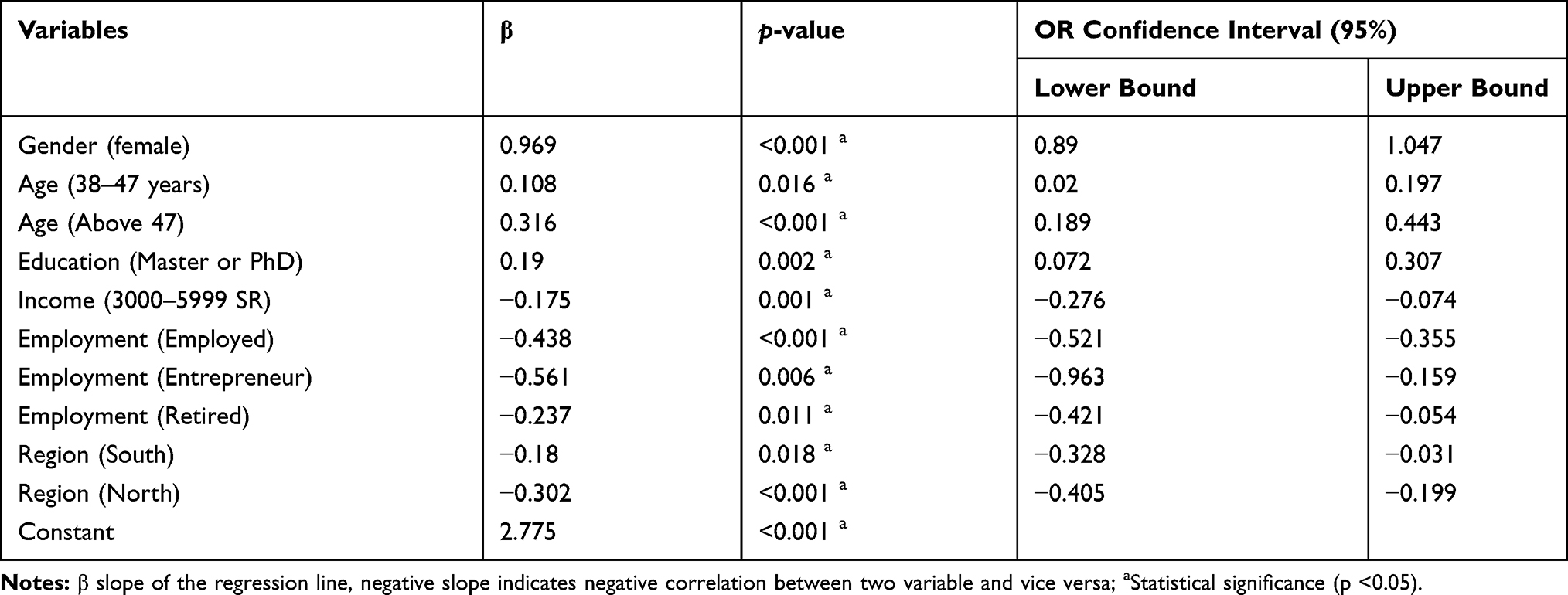 |
Table 5 Multiple Logistic Regression Analysis of the Association of Demographic Characteristics with Participants’ Scores in Relation to Practicing the Staying Home Strategy |
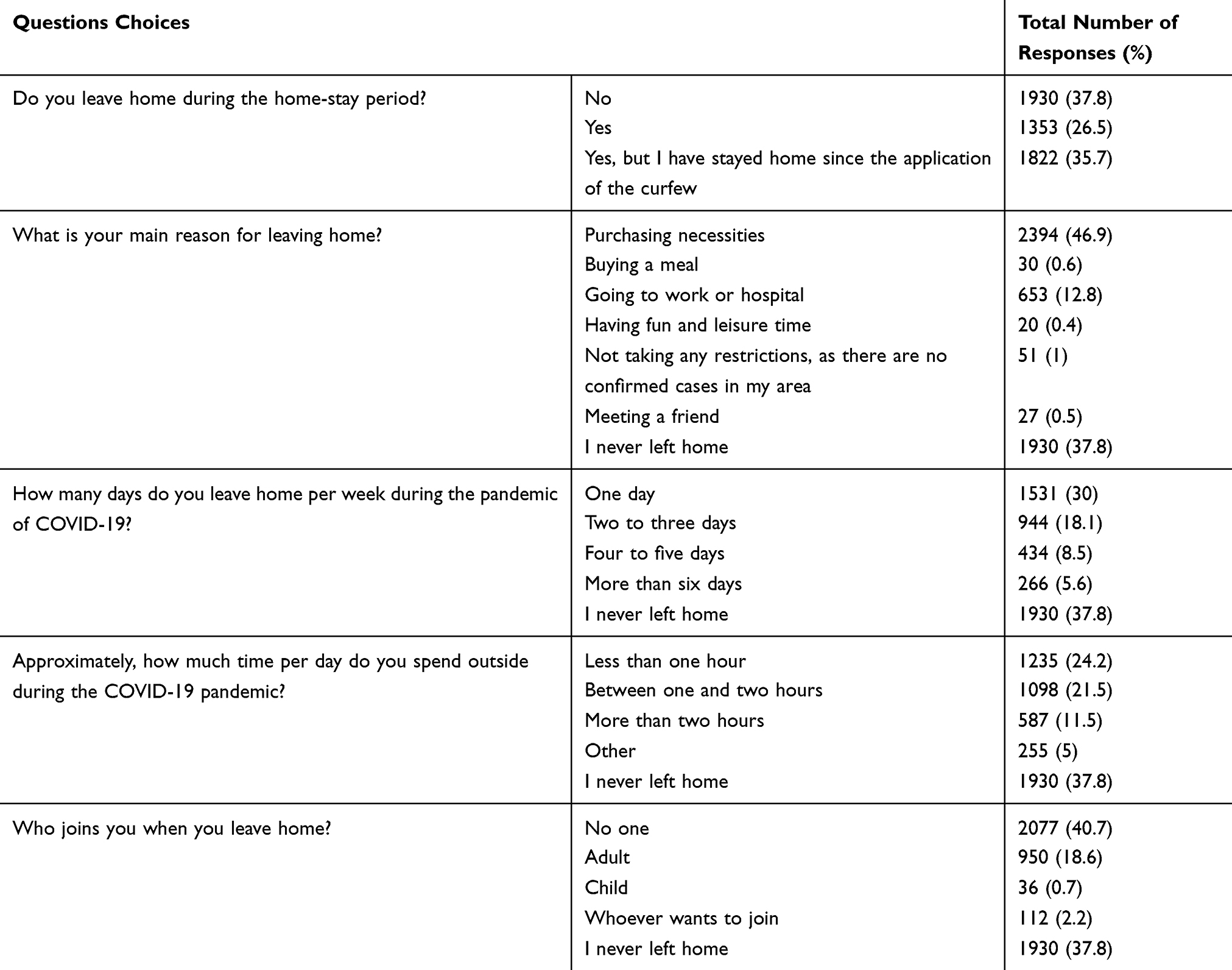 |
Table 6 Responses of Participants to Questions Assessing Their Practice During COVID-19 Pandemic (n = 5105) |
Discussion
Awareness of the public is crucial in controlling the spread of COVID-19, both nationally and internationally, because the level of awareness in society affects the implementation of precautionary measures.7 Therefore, this study was conducted to analyse the knowledge and practices of the population in KSA in relation to staying at home as a preventive measure for containing the COVID-19 pandemic. To the best of our knowledge, this is the first study performed to evaluate the adherence of individuals to the stay-at-home measure in KSA and to provide suggestions about the multiple reasons behind any deficiency in its application.
A survey was distributed and 5,105 responses were returned by participants from different demographic groups to ensured that the collected data represent, to an acceptable level, the Saudi population. The responses indicated a high level of awareness among the Saudi population, with the majority of the participants (94%) expressing the view that everyone should practice social distancing. The respondents (85%) were also aware of the potential asymptomatic transmission of the infection. A population with this level of awareness is speculated to practice social distancing successfully. Previous studies conducted on Chinese and Japanese populations13,19 produced similar findings regarding the public’s knowledge about COVID-19.
In the context of raising awareness, the local public health has established multiple campaigns and launched health applications and call centres, offering the public information about COVID-19 as well as providing answers to related queries.6 This approach has provided Saudi individuals with information related to the benefits of staying at home and encouraged its implementation.6 The respondents indicated that the Saudi MOH was their main source of information (78%), whereas seeking related information from friends and relatives was their least favoured method. Irrespective of the source of information, almost half of Saudi population obtained information about COVID-19 from social media (eg, Twitter) compared to other audio, print and visual media.
The high level of awareness among the Saudi population demonstrated in the early stages of the pandemic indicates the existence of established plans by the government to educate the nation about coronaviruses. This might be the result of the response to the Middle East Respiratory Syndrome (MERS) epidemic in 2012; both Saudi people and the MOH learnt from this previous experience how to contain similar infections.15,20 Consequently, the Saudi authorities acted very early (even before the pandemic reached KSA) by establishing campaigns to enhance public awareness and engage the public in actively learning and searching for information about COVID-19 and the related precautionary measures. In contrast, a recent study conducted in the initial stage of this pandemic demonstrated that the participants living in three Arabic-speaking countries, including Saudi Arabia, had a moderate level of knowledge (66%).21 This could be because more than a quarter of the participants were over 50 years-old. During the COVID-19 pandemic, the information to raise the awareness of individuals was mainly delivered online, which may not be accessible or easy to use by the elderly. In contrast, since the majority of the participants in this study were found to be young, it can be speculated that the observed high level of knowledge of the participants is linked to their ability to access online information about COVID-19 more easily. Therefore, since elderly people are more susceptible to COVID-19 than younger individuals,22 national public health needs to ensure that the information about this pandemic is received by all age groups. The local health authority recently introduced the approach of texting individuals with information about COVID-19 in multiple languages. This step will increase the knowledge of people of various age groups, who speak various languages, as well as the residents of the rural areas, where the internet connection can be poor. In line with the findings of,13,21 the level of education was positively associated with increased awareness. This is self-evident, as well-educated individuals are able to seek, access and understand information far more easily than those who are less well educated.
Regional discrepancies were demonstrated in relation to the awareness within Saudi society about social distancing, with participants living in the middle of the Kingdom showing higher levels of knowledge compared to the other regions. Although the total number of recorded COVID-19 cases is almost identical between the cities in the western region, eg, Makkah (3381) and Medina (2438), and the middle region (Riyadh, 2679), the number of daily reported cases has dropped dramatically, to about 150 cases in Riyadh compared to 200 cases in Makkah and Medina.16 Therefore, the higher awareness of individuals in the middle region of Saudi Arabia may have contributed to the decrease in the numbers of daily cases in Riyadh.
With respect to the practice of staying at home, the overall implementation of social distancing by the participants was found to be moderate (3.13/5). However, a high level of implementation (5/5) was followed by 37% of the participants, who never left home after the introduction of the stay-at-home advice. In addition, the participants who left home mentioned the reasons for this, such as buying necessities (47%), going to work (13%) or going out for leisure (around 2%). Furthermore, the majority of those who left home (46% of the respondents) returned within two hours, and their frequency of leaving was less than three days a week, showing a satisfactory level of implementation of social distancing. Moreover, the majority of responders either went out alone (41%) or with another adult (19%), indicating a positive adherence by limiting contact between individuals to reduce viral dissemination among the population.23 These results are supported by a mobility report for the Saudi communities during the COVID-19 pandemic, which was provided by Google, in which about a 45% reduction was observed in the number of people visiting food warehouses and pharmacies in the Kingdom.24 These outcomes should increase the overall stay-at-home practice from a moderate to a high level; however, there still remains a possibility for greater improvement, encouragement and support to reach higher levels of adherence, especially for those who left home seeking entertainment. As a good adherence to social distancing by Chinese individuals was a key element in the efforts by the authorities to contain the COVID-19 pandemic,7 COVID-19 may be contained in Saudi Arabia relatively early. Nevertheless, the behavioural changes of the Saudi population related to the implementation of precautionary measures (eg, washing hands) outside the home need to be investigated.
A statistical analysis of the responses revealed that females, people aged 38 years or over and Master or PhD holders showed a higher commitment to social distancing compared to their counterparts. This is in agreement with a previous study on the awareness of Saudi people regarding MERS, which demonstrated that females were more likely to apply safety precautions than males.20 A possible explanation for this might be that, culturally, males tend to go out more frequently than females. In relation to the better adherence by people of middle age and older, the people of this age group may have been influenced by published findings from Chinese epidemiological studies, which showed that older patients are more prone to develop invasive forms of COVID-19, with a high fatality rate.22 In addition, the study showed a reduced practice of staying at home among employees and entrepreneurs, possibility because the nature of their work requires them to leave their home regularly compared to other types of jobs. Notably, residents of the northern and southern parts of KSA presented a lower engagement with social distancing, which could be attributed to the delayed appearance of COVID-19 cases in those regions. Areas with limited cases of COVID-19 tend to be associated with reduced knowledge and practice.13 The immediate application of the lockdown strategy has proven effective in flattening the curve of COVID-19’s spread in the cities (regions) of the Kingdom, as the northern and southern parts were protected from a sharp propagation of cases.6,15 A full curfew (24 hours a day) was applied to cities with the high numbers of daily cases in the western, eastern and middle regions, whereas the less affected cities in northern and southern regions were locked down partially (12–15 hours a day).15 This might explain the variation in the level of overall adherence between the regions. However, it was found that the application of the lockdown strategy managed to limit their frequency of leaving home for about 35% of the participants. The establishment of the national lockdown strategy may have been treated by individuals as an alarming sign, indicating the serious, urgent need for action, which may have encouraged them to practice better adherence.
In line with,13 the responses by low-income individuals reflected a lower social distancing practice, and this finding might be related to their need to work to secure their income. Fortunately, a minority of the respondents admitted a lack of commitment to social distancing, mainly because of the absence of cases in their area. Poor practice can result from the lower knowledge of individuals about asymptomatic carriers who can spread the infection. These groups who lack good practice regarding social distancing, especially those with a low income, need to be investigated more closely, so that appropriate solutions to enhance their adherence can be implemented.
Data Sharing Statement
All data generated during this study are included in this published article and its supplementary file.
Ethical Approval
This study was approved by Ethics Committee at the University of Hail (Ethics approval reference number H-2020-080).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which the article will be submitted; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflict of interest.
References
1. Nemati M, Ebrahimi B, Nemati F. Assessment of Iranian nurses’ knowledge and anxiety toward COVID-19 during the current outbreak in Iran. Arch Clin Infect Dis. 2020;15:e102848. doi:10.5812/archcid.102848
2. Singhal TA. Review of coronavirus disease-2019 (COVID-19). Indian J Pediatr. 2020;87:281–286. doi:10.1007/s12098-020-03263-6
3. World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it. 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it.
4. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91:157–160.
5. World Health Organization. WHO COVID-19 dashboard. 2020. Available from: https://covid19.who.int/.
6. Algaissi A, Alharbi N, Hassanain M, Hashem A. Preparedness and response to COVID-19 in Saudi Arabia: building on MERS experience. J Infect Public Health. 2020;13(6):834–838. doi:10.1016/j.jiph.2020.04.016
7. Aslam F. COVID-19 and importance of social distancing. Preprints. 2020.
8. Modi P, Nair G, Uppe A, Modi J, Tuppekar B, Langade DCOVID-19. Awareness among healthcare students and professionals in Mumbai metropolitan region: a questionnaire-based survey. Cureus. 2020;12:e7514.
9. Sen-Crowe B, McKenney M, Elkbuli A. Social distancing during the COVID-19 pandemic: staying home save lives. Am J Emerg Med. 2020.
10. Center for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19). 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-distancing.html.
11. Abel T, McQueen D. The COVID-19 pandemic calls for spatial distancing and social closeness: not for social distancing! Int J Public Health. 2020;65:231. doi:10.1007/s00038-020-01366-7
12. Tellis G, Sood A, Sood N. How long should social distancing last? Predicting time to moderation, control, and containment of COVID-19. SSRN Electron J. 2020. doi:10.2139/ssrn.3562996
13. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16:1745–1752. doi:10.7150/ijbs.45221
14. Center for Disease Control and Prevention. History of quarantine. 2012. Available from: https://www.cdc.gov/quarantine/historyquarantine.html.
15. Yezli S, Khan A. COVID-19 social distancing in the Kingdom of Saudi Arabia: bold measures in the face of political, economic, social and religious challenges. Travel Med Infect Dis. 2020;101692. doi:10.1016/j.tmaid.2020.101692
16. Ministry of Health. COVID 19 dashboard: Saudi Arabia. 2020. Available from: https://covid19.moh.gov.sa/.
17. The Saudi Center for Disease Prevention and Control. Novel coronavirus (2019-nCoV) infection guidelines. 2020. Available from: https://www.moh.gov.sa/en/CCC/healthp/regulations/Documents/Novel%20Corona%20Virus%20Infection%20Guidelines.pdf.
18. Field AP. Discovering Statistics Using IBM SPSS Statistics. London: SAGE; 2018.
19. Machida M, Nakamura I, Saito R, et al. Adoption of personal protective measures by ordinary citizens during the COVID-19 outbreak in Japan. Int J Infect Dis. 2020;94:139–144. doi:10.1016/j.ijid.2020.04.014
20. Aldowyan N, Abdallah AS, El-Gharabawy R. Knowledge, attitude and practice (KAP) study about middle east respiratory syndrome coronavirus (MERS-CoV) among population in Saudi Arabia. Int Arch Med. 2017;10.
21. Naser AY, Dahmash EZ, Alwafi H, et al. Knowledge and practices towards COVID-19 during its outbreak: a multinational cross-sectional study. medRxiv. 2020.
22. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323:1239–1242. doi:10.1001/jama.2020.2648
23. Zhang J, Litvinova M, Liang Y, et al. Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China. Science. 2020;eabb8001.
24. Google. COVID-19 community mobility report Saudi Arabia. 2020. Available from: https://www.gstatic.com/covid19/mobility/2020-04-26_SA_Mobility_Report_en.pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.