")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 7
Public health service options for affordable and accessible noncommunicable disease and related chronic disease prevention and management
Authors Brownie S, Hills AP, Rossiter R
Received 13 August 2014
Accepted for publication 23 September 2014
Published 24 November 2014 Volume 2014:7 Pages 543—549
DOI https://doi.org/10.2147/JMDH.S72636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sharon Brownie,1,2 Andrew P Hills,3,4 Rachel Rossiter5
1Workforce and Health Services, Griffith Health, Griffith University, Gold Coast, QLD, Australia; 2Oxford PRAXIS Forum, Green Templeton College, Oxford University, Oxford, United Kingdom; 3Allied Health Research, Mater Research Institute – The University of Queensland and Mater Mothers' Hospital, South Brisbane, QLD, Australia; 4Griffith Health Institute, Griffith Health, Griffith University, Gold Coast, QLD, Australia; 5MMHN and Nurse Practitioner Programs, School of Nursing and Midwifery, University of Newcastle, Callaghan, NSW, Australia
Abstract: Globally, nations are confronted with the challenge of providing affordable health services to populations with increasing levels of noncommunicable and chronic disease. Paradoxically, many nations can both celebrate increases in life expectancy and bemoan parallel increases in chronic disease prevalence. Simply put, despite living longer, not all of that time is spent in good health. Combined with factors such as rising levels of obesity and related noncommunicable disease, the demand for health services is requiring nations to consider new models of affordable health care. Given the level of disease burden, all staff, not just doctors, need to be part of the solution and encouraged to innovate and deliver better and more affordable health care, particularly preventative primary health care services. This paper draws attention to a range of exemplars to encourage and stimulate readers to think beyond traditional models of primary health service delivery. Examples include nurse-led, allied health-led, and student-led clinics; student-assisted services; and community empowerment models. These are reported for the interest of policy makers and health service managers involved in preventative and primary health service redesign initiatives.
Keywords: primary health care planning, community health care, nurse-led clinics, allied health personnel, health workforce
Introduction
What is known about the topic?
- Despite acknowledgement of the global burden of noncommunicable and related chronic disease, there is sluggishness in workforce reform and service redesign among nations aspiring to provide affordable, accessible, and effective health prevention and management services.
- This paper showcases examples of nonmedical-led primary health care innovations focused on prevention and management of noncommunicable and chronic disease. The target audience is policy makers and health service managers responsible for primary health service redesign initiatives.
What does this paper add?
The provision of accessible, affordable, and effective health services to populations with increasing levels of noncommunicable and chronic disease is a major global challenge.1–4 Paradoxically, many nations can both celebrate increases in life expectancy rates and bemoan parallel increases in chronic disease prevalence. While innovations in medical science and improved socioeconomic conditions have increased life expectancy, not all of that time is spent in good health. New Zealand statistics report that on average, a male can expect 8.9 years and a female 11.5 years of ill health prior to death.5 Combined with rising levels of obesity and related noncommunicable diseases (NCDs), the demand for health services requires the implementation of new models of affordable health care.6–9 The burgeoning level of disease burden demands new approaches to health service delivery and the attention of all health professionals rather than a reliance on doctors alone.1 All staff must be “encouraged to innovate and search for better and more affordable ways of delivering effective and appropriate care.”10
The paper highlights models of health service and leadership innovation in the prevention and management of NCD. Examples provided contrast with traditional medical-led models of care, including nurse-led, allied health-led, student-led, and community or lay person-led empowerment models. These are drawn from published literature and reported for the interest of policy makers and health service managers involved in health service redesign initiatives and grappling with rising levels of NCDs. Where available, evidence regarding the effectiveness of these emerging models of health service innovation and redesign is included.
Challenges confronting health service policy makers and managers
Globally, health policy and service contexts share a number of so-called “wicked problems,” challenges epitomized by inherent complexity, “mushy” definitions, and elusiveness of solution.11,12 Underpinning this “wickedness” are issues such as 1) the burgeoning epidemic of obesity-driven NCDs and related chronic disease; 2) chronic shortages and misdistribution of qualified health professionals; 3) unsustainable rises in health care costs; 4) factors associated with compensation and remuneration across the health workforce; 5) safety concerns associated with the introduction of new drugs to elderly patients with comorbid conditions; and 6) service access issues for low-income, socioeconomically disadvantaged, vulnerable, and/or geographically isolated groups.4,13,14
Essentially, traditional medical-led services can no longer suffice; the burden of disease is too large to be managed by one profession.15 In response, new and innovative models of care must be developed and implemented.7,10 Health professionals preparation requires an increased emphasis on interprofessional education, teamwork, and collaborative care (frequently referred to as interprofessional practice) to support the delivery of effective integrated and well-coordinated health services.16 Top-down policy has limitations; therefore, communities, service users, and lay educators must be engaged and involved in service planning and delivery processes.17–19 In effect, all health professionals must be part of the solution to avert the global health challenge of avoidable NCDs.10
Sadly, while these messages have been disseminated over several decades, effective action has been limited. Rather, the health issues and disparities have worsened, leading to increasingly urgent calls for action by governments and health policy officials.20–23 However, major systems change is complex and difficult, given the associated large-scale social and behavioral shifts required to impact on the alarming trends in obesity-driven NCDs.24 In response to this global increase in NCDs, many countries are increasingly looking to nurses, midwives, and allied health professionals to provide prevention and disease management services. Noteworthy are increasing reports of successful innovations and new service delivery models.
Accessing literature
In searching the literature relevant to this topic, the intent was not to present a systematic review of all recently published research, but rather to ensure that the discussion was informed by the literature and identify a set of cases that illustrate the possibilities and potential benefits of moving beyond medical-led models of care. Sources accessed included search and alert engines, electronic databases (CINAHL, MEDLINE, Cochrane), relevant journal websites, and grey literature. The inclusion criteria applied concentrated on English language publications from 2009 to 2014. Search terms were nurse-led, allied health-led, and student-led clinics; student-assisted services; and community empowerment models. While the search term “nurse-led” in CINAHL identified 895 papers focusing on nurse-led interventions, most relate to acute care services in secondary care contexts; few of these address the growing burden resulting from the rise in NCD and comorbidity.
The following sections feature global illustrations of innovative primary health service delivery.
Nurse-led services
Traditionally, nurses and midwives have formed the backbone of primary health care services. A 2006 study described nurse-led services as a “formalized and structured health care delivery mode involving a nurse and a client … with health care needs that can be addressed by a nurse.”6 Emphasis was given to the advanced competence and ability to work both independently and interprofessionally inherent in the provision of care that bridges the gap between hospital and primary care.25 Multiple case studies are available to highlight the leadership role of nurses and midwives in both primary and secondary health care settings. In the former, the growing burden of NCD-related patient demand has significantly increased both general practice and medical specialty workloads. Earlier studies showed reduced hospital presentations when general practitioners included nurse-led clinic services within their practice.26,27 In 2007, the Australian East General Practice Network produced a useful manual summarizing the rationale and evidence for health services provided by nurse-led clinics. The publication provides pointers regarding the establishment and implementation of a nurse-led clinic and reports evidence that integrated collaboration with nurse-led services relieves medical practitioner workload, increases services to patients, and improves patient outcomes.26 A meta-analysis of 14 United States of America nurse-delivered collaborative care interventions for people with depression and long-term physical conditions reported improved depression outcomes, suggesting the potential for trialing similar models in other settings.28
Table 1 highlights different models of nurse-led services with evaluations and positive health outcomes.
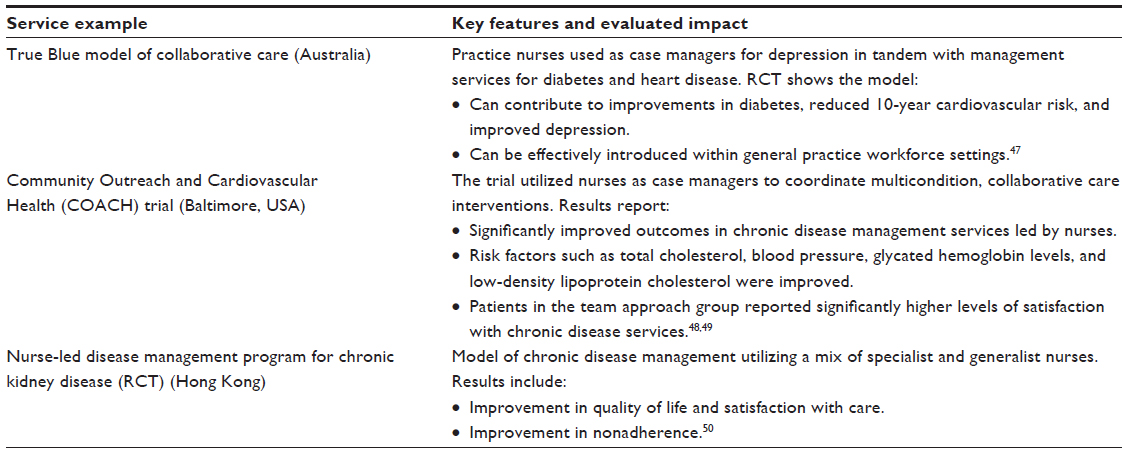 | Table 1 Nurse-led primary health care services |
Allied health-led services
It has long been recognized that allied health professionals can make significant contributions to address gaps in primary health care services and to improve outcomes for vulnerable individuals at risk of adverse health outcomes. More than 35 years ago, members of the medical profession recognized the very significant contribution that could be made by other health professionals: “Allied health professionals have the required skills to provide preventive services with a greater sense of job satisfaction than do physicians.”29
Allied health professions have been “defined as those professions that are distinct from medicine, dentistry, and nursing.”30 Allied health professionals working in a multi- or interdisciplinary context have an important role to play in chronic disease management.31 Typically, allied health services are not provided in isolation but as part of a chronic disease management model led by medical colleagues, often with nursing support. In the Australian context, chronic disease management led by general practitioners (GPs) supports structured care planning for individuals with chronic disease, with incentives for care plans implemented under team care arrangements involving the GP and relevant allied health professionals, including Accredited Exercise Physiologists and dietitians.32–35 The role of allied health professionals in providing effective care was emphasized in the clinical practice guidelines for stroke.36 A key recommendation in these guidelines highlights the utilization of integrated multidiscipline care approaches by allied health professionals to improve health outcomes. More recently, clinical practice guidelines for the management of overweight and obesity report evidence that care delivered by multidisciplinary teams can be more effective than that provided by an individual health professional.37 Table 2 points to examples of allied health involvement in the management of NCDs.
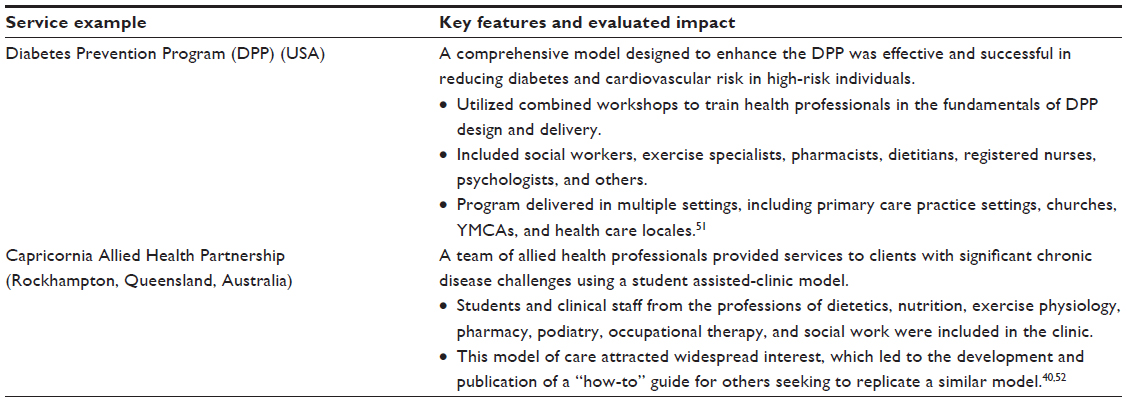 | Table 2 Allied health-led primary health care services |
Student-led and student-assisted services
Student-led and student-assisted services have the potential to deliver several benefits, including well-supervised quality health care services, to vulnerable, low-income, or poorly serviced individuals and communities while also enabling nursing and allied health students to gain valuable clinical experience in primary care settings. A diverse range of Australian and international models are available for consideration (see Table 3).
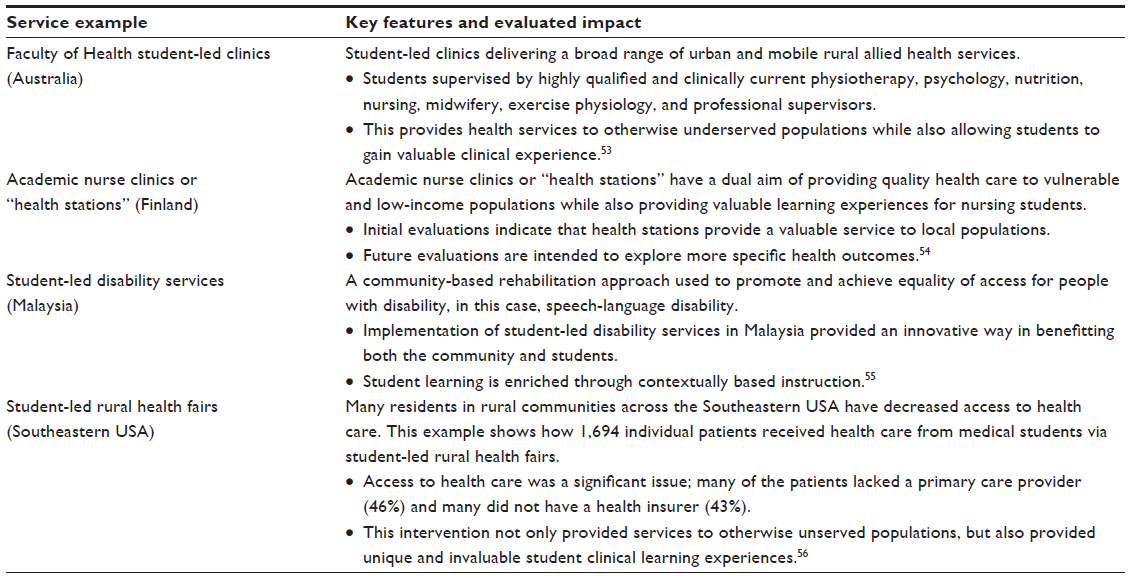 | Table 3 Student-led and student-assisted primary health care services |
Models with services delivered by community-based lay health educators
In addition to models of care provided by qualified health professionals, a growing literature describes community-delivered primary health care services (Table 4). Current terminology describing help provided by community members employs a range of descriptors, such as peer educators, community health workers, lay health educators, outreach workers, and natural helpers.38 The work of lay health educators who act in a “spirit of collaboration and mutuality” has the potential to promote the very best of principles and best practice in patient-centered care and health literacy.39 Lay members of the community are described as having the capacity to decrease health care disparities and, through familiar and trusted relationships, build bridges between professional health care services while also addressing cultural gaps that might otherwise not be possible.39,40
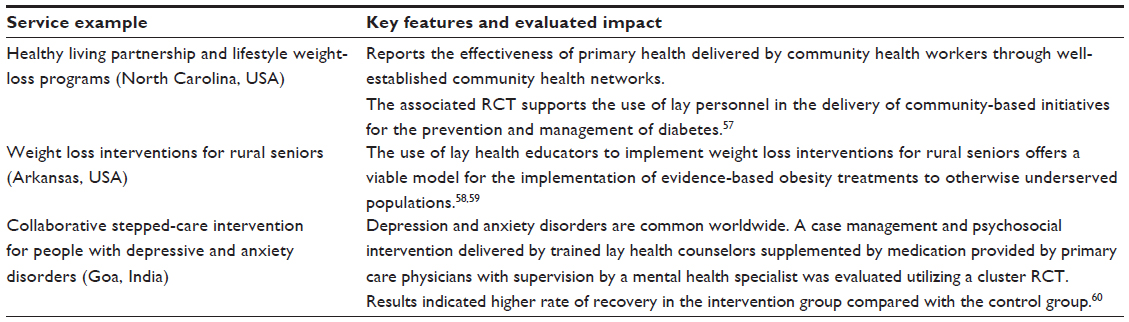 | Table 4 Community-led primary health care services |
What can be learned from these examples?
The examples profiled in this paper support the notion that management of chronic health conditions is best provided by a range of health professionals and community lay members working together.41 The examples provide a rich resource of evaluated innovations which highlight the potential and benefits which can be realized through interprofessional collaboration, professional-community partnerships, and redesigned models of care. While an increasing array of initiatives is being trialed, implemented, and evaluated, such models are not yet embedded as the norm throughout health care systems. All too often, professional boundaries are maintained and traditional models of care prevail.
Currently, the training of health care professionals and the structure of the Australian health system mitigates the optimal achievement of collaborative service delivery. For example, there are few examples of joint training of health professionals, the logical starting point for an understanding of, and respect for, the skills and contribution of each professional group. Optimal outcomes for patients, including those with chronic disease, require practitioners to have a clear understanding of respective role delineation and contribution42 and to respect this contribution.43 In addition, responsibility for policy development, planning, and service delivery is the province of two levels of government, traditionally poorly integrated.44 Further, the mix of private and public sector organizations, plus significant differences in the mix of health professionals working in these settings, is a challenge. This situation is further complicated by the differential in payment for GPs and allied health professionals, fee-for-service in private practice, and activity-based block funding in the public sector. Newly published reports continue to call for reform in education and training with greater emphasis on interprofessional activity, working together, and re-envisioning the roles of the health workforce.45,46
What further developments are needed?
Nurse, allied health, and community-led or -assisted primary care clinics are currently heterogeneous in nature, with no systematic review available to evaluate effectiveness between one model or another. Existing models are limited by factors such as the aforementioned professional boundaries, regulatory and licensing restrictions, mismatched funding models, the availability of health professionals with advanced practice competencies, deficits in policy implementation, and more.19,45
Conclusion
It is not possible for GPs and other medical professionals alone to meet NCD-driven levels of health service demand. Where and how health professionals are utilized is important for effective health service delivery and access to care. Action is required by both health policy makers and health service managers to provide the right mix of health care professionals in the right places to deliver effective preventative and primary care services, which will help stem the growing tide of NCDs. The involvement of all health professionals and the support of the community are needed to effectively meet health needs now and in the future. Ongoing discussion is needed regarding possible options, and more research is required to evaluate current developments and to inform the sustainability of funding models and policy implementation processes going forward.
Disclosure
The authors report no conflicts of interest in this work.
References
De Maeseneer J, Roberts RG, Demarzo M, et al. Tackling NCDs: a different approach is needed. Lancet. 2012;379(9829):1860–1861. | |
Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4–14. | |
Noncommunicable Diseases and Mental Health WHO. Global Status Report on Noncommunicable Diseases 2010. Italy: World Health Organization; 2011. | |
Kaplan W, Wirtz VJ, Mantel-Teeuwisse A, Stolk P, Duthey B, Laing R. Priority Medicines for Europe and the World 2013 Update. Geneva, Switzerland: 2013. | |
Ministry of Health and Accident Compensation Corporation. Injury-related Health Loss: A Report from the New Zealand Burden of Diseases, Injuries and Risk Factors Study 2006–2016. Wellington: Ministry of Health; 2013. | |
Singh D, Ham C. Improving Care for People with Long-term Conditions: A Review of UK and International Frameworks. University of Birmingham Health Services Management Centre and National Health Service Institute for Innovation and Improvement; 2006. | |
Allotey P, Reidpath DD, Yasin S, Chan CK, de-Graft Aikins A. Rethinking health-care systems: a focus on chronicity. Lancet. 2011; 377(9764):450–451. | |
King D. The future challenge of obesity. Lancet. 2011;378(9793):743–744. | |
Independent Commission on Whole Person Care. One Person One Team One System: Report of the Independent Commission on Whole Person Care for the Labour Party. Feb 2014. | |
Hancock C. Foreword. In: Nolte E, Knai C, McKee M, editors. Managing Chronic Conditions: Experience in Eight Countries. Europe: WHO Regional Office 2008:xii–xiv. | |
Australian Government: Australian Public Service Commission. Tackling Wicked Problems: A Public Policy Perspective. In: Australian Public Service, editor. Canberra, Australia: Australian Government; 2007. | |
Head BW, Alford J. Wicked Problems: Implications for Public Policy and Management. Admin Soc. 2013:0095399713481601. | |
Allotey P, Davey T, Reidpath DD. NCDs in low and middle-income countries – assessing the capacity of health systems to respond to population needs. BMC Public Health. 2014;14(Supplement):1–3. | |
Godman B, Malmström RE, Diogene E, et al. Dabigatran – a continuing exemplar case history demonstrating the need for comprehensive models to optimize the utilization of new drugs. Front Pharmacol. 2014;5:109. | |
Bangalore, Framingham. Squeezing out the doctor. Economist. June 2, 2012. | |
Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. | |
Bambra CL, Hillier FC, Moore HJ, Cairns-Nagi JM, Summerbell CD. Tackling inequalities in obesity: a protocol for a systematic review of the effectiveness of public health interventions at reducing socioeconomic inequalities in obesity among adults. Syst Rev. 2013;2:27. | |
Patel V, Saxena S. Transforming lives, enhancing communities – innovations in global mental health. N Engl J Med. 2014;370(6):498–501. | |
Noyes J, Lewis M, Bennett V, Widdas D, Brombley K. Realistic nurse-led policy implementation, optimization and evaluation: novel methodological exemplar. J Adv Nurs. 2014;70(1):220–237. | |
Gaziano TA, Galea G, Reddy KS. Scaling up interventions for chronic disease prevention: the evidence. Lancet. 2007;370(9603):1939–1946. | |
Marmot S, Friel S, Bell R, Houweling TAJ, Taylor S. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372(9650):1661–1669. | |
Geneau R, Stuckler D, Stachenko S, et al. Raising the priority of preventing chronic diseases: a political process. Lancet. 2010;376(9753):1689–1698. | |
Mbanya JC, Squire SB, Cazap E, Puska P. Mobilising the world for chronic NCDs. Lancet. 2011;377(9765):536–537. | |
Ezzati M, Riboli E. Behavioral and Dietary Risk Factors for Noncommunicable Diseases. New England Journal of Medicine. 2013;369(10):954–964. | |
Wong FK, Chung LC. Establishing a definition for a nurse-led clinic: structure, process, and outcome. J Adv Nurs. 2006;53(3):358–369. | |
Melbourne East GP Network. Chronic Disease Management in General Practice: Nurse Led Clinics. Melbourne: Australian Department of Health & Ageing; 2007:1–48. | |
Delamaire ML, Lafortune G. Nurses in Advanced Roles: A description and evaluation of experiences in 12 developed countries. OECD Health Working Papers. 2010:1–54. | |
Ekers D, Murphy R, Archer J, Ebenezer C, Kemp D, Gilbody S. Nurse-delivered collaborative care for depression and long-term physical conditions: a systematic review and meta-analysis. J Affect Disord. 2013;149(1–3):14–22. | |
Johnson KG, Deuschle KW. Strategies for prevention using allied health professionals. Prev Med. 1977;6(3):386–390. | |
Arena RA, Goldberg LR, Ingersoll CD, Larsen DS, Shelledy D. Research in the allied health professions: why fund it? A report of the ASAHP Research Committee. J Allied Health. 2011;40(3):161–166. | |
Turnbull C, Grimmer-Somers K, Kumar S, May E, Law D, Ashworth E. Allied, scientific and complementary health professionals: a new model for Australian allied health. Aust Health Rev. 2009;33(1):27–37. | |
Allied Health Professions Australia. Chronic Disease Management for General Practitioners, General Practice Nurses and Allied Health Professionals: Sharing the care and understanding between General Practice and Allied Health Professionals. Allied Health Professions Australia; 2010:1–54. | |
Australian Government Department of Health. Chronic Disease Management – Patient Information 2014 [cited November 2, 2014]. Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/F17F6787B14E6CF1CA257BF0001B0AEC/$File/Fact%20Sheet%20-%20CDM%20-%20Patient%20Info%20-%20Feb%202014.pdf. Accessed November 2, 2014. | |
Australian Government Department of Health. Chronic disease management – allied health individual services. Updated April 10, 2014. http://www.health.gov.au/internet/main/publishing.nsf/Content/Chronic+Disease+Allied+Health+Individual+Services. Accessed September 30, 2014. | |
Soan EJ, Street SJ, Brownie SM, Hills AP. Exercise physiologists: essential players in interdisciplinary teams for noncommunicable chronic disease management. J Multidiscip Healthc. 2014;7:65–68. | |
National Stroke Foundation. Clinical Guidelines for Stroke Management. Melbourne, Australia: Stroke Foundation; 2010: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/cp126.pdf. Accessed September 30, 2014. | |
National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia. Melbourne, Australia: National Health and Medical Research Council; 2013. | |
Souder E, Terry TL. Use of lay educators to overcome barriers to research with Black older adults: a case study using Alzheimer’s Disease Center. Res Gerontol Nurs. 2009;2(4):235–242. | |
Auger S, Verbiest S. Lay health educators’ roles in improving patient education. N C Med J. 2007;68(5):333–335. | |
Frakes K-A, Tyack ZF, Miller M, Davis LA, Swanston A, Brownie S. The Capricornia Project: Developing and Implementing an interprofessional Student-assisted Allied Health Clinic. Brisbane, Australia: Clinical Education and Training (ClinEdQ), Queensland Health; 2011. | |
McDonald J, Harris M, Jayasuriya R. Collaboration between Health Professionals across Organisational Boundaries: A Case Study of Diabetes. School of Public Health and Community Medicine, Faculty of Medicine, University of New South Wales; 2012. | |
Harris MF, Zwar NA. Care of patients with chronic disease: the challenge for general practice. Medical Journal of Australia. 2007;187(2):104. | |
Boyce RA, Moran MC, Nissen LM, Chenery HJ, Brooks PM. Interprofessional education in health sciences: the University of Queensland Health Care Team Challenge. Med J Aust. 2009;190(8):433–436. | |
Davies GP, Perkins D, McDonald J, Williams A. Special series: Integrated primary health care: Integrated primary health care in Australia. Int J Integr Care. 2009;9:e95. | |
Duckett S, Breadon P. Access All Areas: New Solutions for GP Shortages in Rural Australia. Melbourne: Grattan Institute; 2013. | |
Duckett S, Breadon P. Unlocking Skills in Hospitals: Better Jobs, More Care. Grattan Institute; 2014. | |
Morgan MA, Coates MJ, Dunbar JA, Reddy P, Schlicht K, Fuller J. The TrueBlue model of collaborative care using practice nurses as case managers for depression alongside diabetes or heart disease: a randomised trial. BMJ Open. 2013;3(1). | |
Allen JK, Dennison-Himmelfarb CR, Szanton SL, et al. Community Outreach and Cardiovascular Health (COACH) Trial: a randomized, controlled trial of nurse practitioner/community health worker cardiovascular disease risk reduction in urban community health centers. Circ Cardiovasc Qual Outcomes. 2011;4(6):595–602. | |
Rosenberg K. Nurse-led teams in chronic disease management. Am J Nurs. 2012;112(4):16. | |
Wong FK, Chow SK, Chan TM. Evaluation of a nurse-led disease management programme for chronic kidney disease: a randomized controlled trial. Int J Nurs Stud. 2010;47(3):268–278. | |
Kramer MK, Kriska AM, Venditti EM, et al. Translating the Diabetes Prevention Program: a comprehensive model for prevention training and program delivery. Am J Prev Med. 2009;37(6):505–511. | |
Frakes KA, Brownie S, Davies L, Thomas J, Miller ME, Tyack Z. Experiences from an interprofessional student-assisted chronic disease clinic. J Interprof Care. 2014:1–3. | |
Faculty of Health University of Canberra. Student Led Clinics. 2013; http://www.canberra.edu.au/faculties/health/community-connections/clinics/student-led-clinics. Accessed September 30, 2014. | |
Ponto M, Paloranta H, Akroyd K. An evaluation of student led health station in Finland. Prog Health Sci. 2011;1(1):5–13. | |
Van Dort S, Coyle J, Wilson L, Ibrahim HM. Implementing the World Report on Disability in Malaysia: a student-led service to promote knowledge and innovation. Int J Speech Lang Pathol. 2013;15(1):90–95. | |
Landy DC, Gorin MA, O’Connell MT. Student-led rural health fairs: attempting to improve medical education and access to health care. South Med J. 2011;104(8):598–603. | |
Katula JA, Vitolins MZ, Morgan TM, et al. The Healthy Living Partnerships to Prevent Diabetes study: 2-year outcomes of a randomized controlled trial. Am J Prev Med. 2013;44(4 Suppl 4):S324–S332. | |
Krukowski RA, Pope RA, Love S, et al. Examination of costs for a lay health educator-delivered translation of the Diabetes Prevention Program in senior centers. Prev Med. 2013;57(4):400–402. | |
Krukowski RA, Lensing S, Love S, et al. Training of lay health educators to implement an evidence-based behavioral weight loss intervention in rural senior centers. Gerontologist. 2013;53(1):162–171. | |
Patel V, Weiss HA, Chowdhary N, et al. Effectiveness of an intervention led by lay health counsellors for depressive and anxiety disorders in primary care in Goa, India (MANAS): a cluster randomised controlled trial. Lancet. 2010;376(9758):2086–2095. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.