")
Back to Journals » Clinical Epidemiology » Volume 14
Psychotropic Drug Use in Acute Myeloid Leukaemia (AML) and Myelodysplastic Syndrome (MDS): A Danish Nationwide Matched Cohort Study of 2404 AML and 1307 MDS Patients
Authors Jensen O, Øvlisen AK , Jakobsen LH, Roug AS, Nielsen RE, Marcher CW, Ebbesen Lh, Theilgaard-Mönch K, Møller P, Schöllkopf C, Torp-Pedersen C, El-Galaly TC, Severinsen MT
Received 27 August 2021
Accepted for publication 25 December 2021
Published 25 February 2022 Volume 2022:14 Pages 225—237
DOI https://doi.org/10.2147/CLEP.S336115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Irene Petersen
Oda Jensen,1 Andreas Kiesbye Øvlisen,1,2 Lasse Hjort Jakobsen,1,2 Anne Stidsholt Roug,1,2 René Ernst Nielsen,2,3 Claus Werenberg Marcher,4 Lene Hyldahl Ebbesen,5 Kim Theilgaard-Mönch,6 Peter Møller,7 Claudia Schöllkopf,8 Christian Torp-Pedersen,9,10 Tarec Christoffer El-Galaly,1,2 Marianne Tang Severinsen1,2
1Department of Haematology, Clinical Cancer Research Centre, Aalborg University Hospital, Aalborg, Denmark; 2Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 3Department of Psychiatry, Aalborg University Hospital, Aalborg, Denmark; 4Department of Haematology, Odense University Hospital, Odense, Denmark; 5Department of Haematology, Aarhus University Hospital, Aarhus, Denmark; 6Department of Haematology, Rigshospitalet, Copenhagen, Denmark; 7Department of Haematology, Roskilde Sygehus, Roskilde, Denmark; 8Department of Haematology, Herlev Hospital, Herlev, Denmark; 9Unit of Clinical Biostatistics and Epidemiology, Aalborg University Hospital, Aalborg, Denmark; 10Department of Cardiology, Nordsjællands Hospital, Hillerød, Denmark
Correspondence: Marianne Tang Severinsen, Department of Haematology, Clinical Cancer Research Centre, Aalborg University Hospital, Aalborg, Denmark, Email [email protected]
Introduction: The diagnosis of a life-threatening disease can lead to depression and anxiety resulting in pharmacological treatment. However, use of psychotropic drugs (antidepressants, anxiolytics, and antipsychotics) in acute myeloid leukaemia (AML) and myelodysplastic syndrome (MDS) is undetermined.
Methods: Prescription of psychotropic drugs in Danish AML and MDS patients was compared to a cohort matched on age, sex, and country of origin from the Danish background population using national population-based registries.
Results: In total, 2404 AML patients (median age 69 years) and 1307 MDS patients (median age 75 years) were included and each matched to five comparators from the background population. Two-year cumulative incidences showed that AML (20.6%) and MDS (21.2%) patients had a high risk of redemption of a psychotropic drug prescription compared to the background population (7.0% and 7.9%). High age, low educational level, and Charlson Comorbidity Index score ≥ 1 was associated with a higher risk in AML and MDS patients. Furthermore, non-curative treatment intent and performance status in AML patients, and high risk MDS were associated with elevated risk of psychotropic drug prescription.
Conclusion: In conclusion, diagnoses of AML and MDS were associated with a higher rate of psychotropic drugs prescription compared to the background population.
Keywords: acute myeloid leukaemia, myelodysplastic syndrome, depression, anxiety, psychotropic drugs
Introduction
Acute myeloid leukaemia (AML) is an aggressive cancer characterised by abrupt debut after days or weeks of illness, followed by a fast track diagnostic programme and information on prognosis and treatment.1,2 Treatment ranges from intensive chemotherapy with severe side-effects and intent of cure to palliative therapy used for patients with poor performance status.1,3,4
Myelodysplastic syndrome (MDS) is a heterogeneous group of preleukaemic myeloid neoplasms that, like AML, arise in myeloid stem cells.5,6 MDS leads to cytopenia and the clinical presentation ranges from asymptomatic to an AML-like condition with critical anaemia, bleeding and severe infections. MDS most often has a slow debut and some patients do not consider this condition a cancer. However, the 5-year overall survival is 31% and treatment options are limited, ranging from intensive AML-like chemotherapy and allogeneic stem cell transplantation to supportive care only.5,7–9 Utilising the revised international prognostic scoring system (IPSS-R), MDS patients are classified into five categories based on risk of transformation to AML and mortality.10,11
Patients diagnosed with cancer frequently experience psychological distress which may lead to prescription of psychotropic drugs. Several studies have found increased risk of depression and anxiety in cancer patients compared to individuals without cancer.2,12–17 In the general population, increasing age and female sex are associated with increased lifetime risk of depression and anxiety.18 For cancer patients, the risk of depression and anxiety is also associated with the specific cancer diagnosis. Patients with a poor prognosis have a higher risk of depression and anxiety compared to patients with more favourable outcomes.12 Since both AML and MDS are cancers with a poor prognosis they may be in high risk of developing depression and anxiety. However, the mental health of patients diagnosed with AML and MDS has been sparsely investigated as focus has mainly been on treatment and survival. Only few studies investigated the risk of depression and anxiety in AML patients and no current literature describe the risk of depression and anxiety in MDS patients. However, psychological distress, specifically unrecognised depression and anxiety, may negatively impact the quality of life, reduce compliance to treatment, and result in inferior survival.2,12,13,16,19 This study provided insight into the need to focus on the mental health of patients with AML and MDS.
The aim of this nationwide study was to evaluate the risk of depression and anxiety following diagnosis of AML and MDS by comparing 2-year cumulative risks of psychotropic drug prescriptions to a matched cohort from the Danish background population. Furthermore, clinical risk factors associated with prescription of psychotropic drugs in AML and MDS patients will be identified. Prevalence of depression and anxiety was defined as prescription of a psychotropic drug.
Materials and Methods
Data Sources
All Danish citizens are registered with a 10-digit civil registration number assigned at birth or immigration for identification. The civil registration number enables linkage of data across all Danish medical and administrative registries. The Danish Civil Registry (established in 1968 and has high completeness) covers demographic data including age, sex and civil status.20,21 The Danish Education Register is annually updated and includes the highest accomplished educational level using the International Standard Classification of Education.22 The Danish National Patient Registry (complete since 1979) uses the International Classification of Diseases (ICD-10) classification to record information on all emergency and inpatient contacts in Danish hospitals, including outpatient contacts since 1995.23 The Charlson Comorbidity Index score was calculated using this information.24 The Danish National Prescription Registry (complete and valid since 1995) covers information on redemption of prescribed drugs in all Danish pharmacies and uses the Anatomical Therapeutic Chemical Classification (ATC) for identification of drugs. In this study, psychotropic drugs were defined as antidepressants (ATC - N06A), anxiolytics (ATC - N05B), and antipsychotics (ATC - N05A).25,26 Prescription of at least one psychotropic drug was used as a surrogate measure of depression or anxiety. The Danish National Acute Leukaemia Registry has collected data on all Danish AML patients since 2000 and all Danish MDS patients since 2010. Information in The Danish National Acute Leukaemia Registry has been validated and described in detail elsewhere.5 In brief, data on AML include detailed clinical information, disease status, and treatment (eg ICD-10 diagnosis, date of diagnosis, Eastern Cooperative Oncology Group performance status, and planned treatment intent). Likewise, for MDS, data include detailed clinical information, disease status, and treatment (eg ICD-10 diagnosis, date of diagnosis, cytopenia, cytogenetic risk, and blast percentage).5,27 Information from The Danish National Acute Leukaemia Registry was used to calculate the revised international prognostic scoring system (IPSS-R) score for MDS patients.10,11
Study and Background Population
The studied cohorts included all patients fulfilling the following inclusion criteria: 1) diagnosed with non-acute promyelocytic leukaemia AML in Denmark between January 1, 2005 and December 31, 2015 or diagnosed with MDS in Denmark between January 1, 2010 and December 31, 2015; 2) age ≥ 18 years at diagnosis; and 3) had not been prescribed any psychotropic drugs during the year prior to inclusion date which was date of diagnosis (index date).
For both patient cohorts, a comparison cohort was defined by matching each patient to five individuals from the Danish background population with the same sex, age (year and month of birth), and country of origin. Only comparators with no prescription of psychotropic drugs within one year prior to the index date were considered for matching.
Clinical Variables
Relevant clinical variables for identification of association to psychotropic drug prescriptions in AML and MDS patients were chosen based on prognostic value and clinical relevance. Clinical variables included sex (male, female), age (18–59 years, 60–74 years, ≥75 years), country of origin (Danish, other western country, other non-western country), civil status (married, divorced, widowed), educational level (low, medium/high), and Charlson Comorbidity Index score (0, ≥1). Detailed information regarding clinical variables can be seen in Supplementary Materials showing the diseases and weight of these included in the Charlson Comorbidity Index score. Furthermore, treatment intent (curative, non-curative) and Eastern Cooperative Oncology Group performance status (0, 1–4) for AML and IPSS-R score (very low risk, low risk, intermediate risk, high risk, very high risk) for MDS were included.10,11
Statistical Analysis
Follow-up was started at the index date until first psychotropic drug prescription, death from any cause, censoring (end of follow-up (August 2018), or emigration), or a matched comparator being diagnosed with AML or MDS.
Baseline characteristics were presented by proportions for categorical variables and medians (interquartile range) for continuous variables. The Mann–Whitney U-test and Pearson’s chi-square test were used to compare baseline characteristics between patients and matched comparators. Cumulative risks of psychotropic drug prescription were calculated using the Aalen–Johansen estimator with deaths treated as competing risk. Cumulative incidence curves were computed for: 1) time to first psychotropic drug prescription from the index date; 2) a sensitivity analysis of time to the second psychotropic drug prescription from the index date; and 3) time to first prescription from 2 years prior until 2 years after diagnosis. In the latter, patients and matched comparators who received psychotropic drug prescriptions prior to the index date were not excluded. These cumulative incidences were used to: 1) estimate the incidence of anxiety and depression; 2) validate the use of time to first psychotropic drug as an estimate for the incidence of anxiety and depression; and 3) to assess whether AML and MDS patients differed from the background population prior to diagnosis. An additional analysis was performed in which hypnotics (ATC – N05C) were included as a psychotropic drug due to their benzodiazepine-like nature. For the cumulative incidences, Gray’s test was used to determine if there was a significant difference between the AML/MDS cohort and matched comparators.28 Associations between relevant clinical variables and psychotropic drug prescriptions were assessed using Cox proportional hazards regression analysis adjusted for age and sex. Cause-specific hazard ratios (HRs) were calculated for both the AML/MDS patients and matched comparators. The threshold for a significant P-value was defined as 0.05.
R version 3.6.1 (R foundation for Statistical Computing) and SAS version 9.4 (SAS Institute Inc.) were used to compute statistical analyses.
Pseudo-anonymised data provided by the secured network governed by Statistics Denmark were used for all analysis. The Danish Data Protection Agency, the North Denmark Region, approved the study (ID-number 2018–88). According to Danish legislation, no approval from an ethics committee or informed consent from patients are required for register-based studies. The Declaration of Helsinki has been followed.
Results
Baseline Characteristics
In total, 2404 AML patients and 1307 MDS patients fulfilled the inclusion criteria and were matched to 12,020 and 6535 comparators from the respective background populations. AML patients had a median age of 69 (57–78) years and a male:female ratio of 1.37. MDS patients had a median age of 75 (68–82) years and a male:female ratio of 1.82. Baseline characteristics for AML/MDS patients and matched comparators are shown in Table 1.
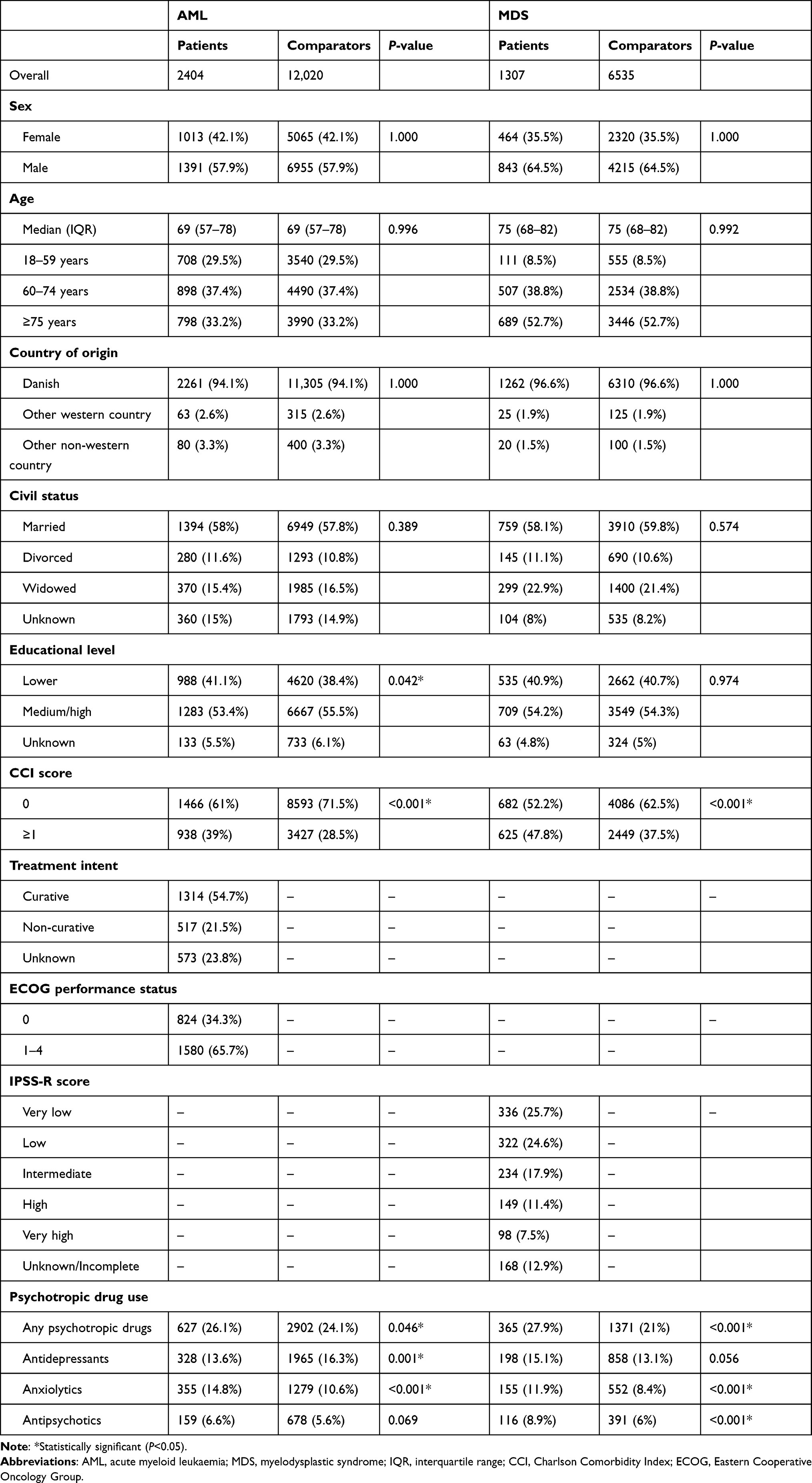 |
Table 1 Baseline Characteristics and Prescription of Psychotropic Drugs in Patients with Acute Myeloid Leukaemia (AML), Myelodysplastic Syndrome (MDS), and the Respective Matched Comparators |
Incident Psychotropic Drug Prescriptions in AML and MDS Patients
The 2-year cumulative incidence of psychotropic drug prescription stratified by type of psychotropic drug is shown in Figure 1. Overall, the 2-year cumulative incidence of time to first prescription of any psychotropic drug was 20.6% (95% CI 19.0–22.3) for AML patients and 21.2% (95% CI 18.7–23.7) for MDS patients as compared to 7.0% (95% CI 6.4–7.7) and 7.9% (95% CI 7.2–8.7) for matched comparators. This was confirmed by the crude HRs, which were 4.8 (95% CI, 4.3–5.3) and 2.5 (95% CI, 2.2–2.9) for AML and MDS patients, respectively (Table 2).
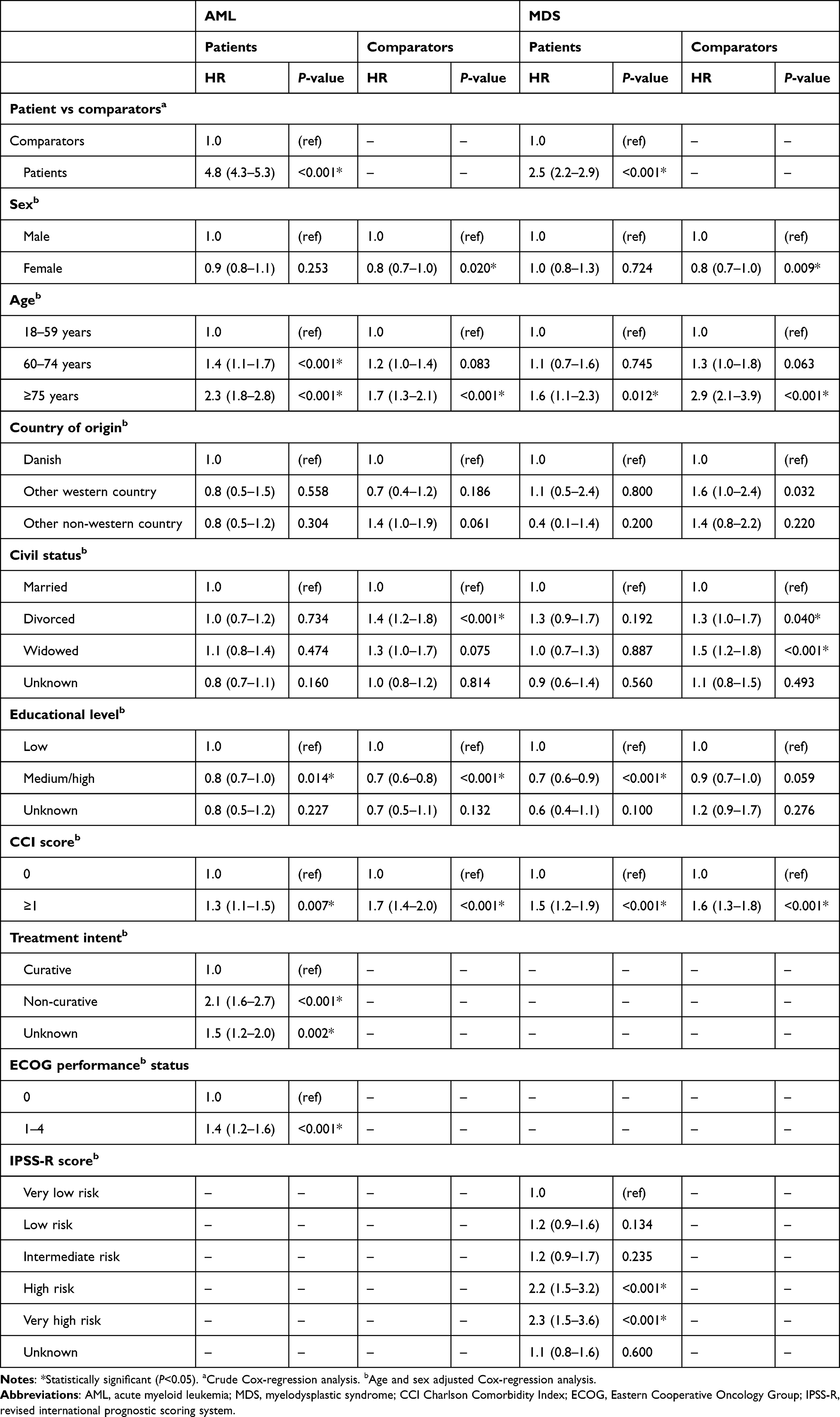 |
Table 2 Prescription of Psychotropic Drugs in Patients with Acute Myeloid Leukaemia (AML), Myelodysplastic Syndrome (MDS), and Matched Comparators in Association with Clinical Variables |
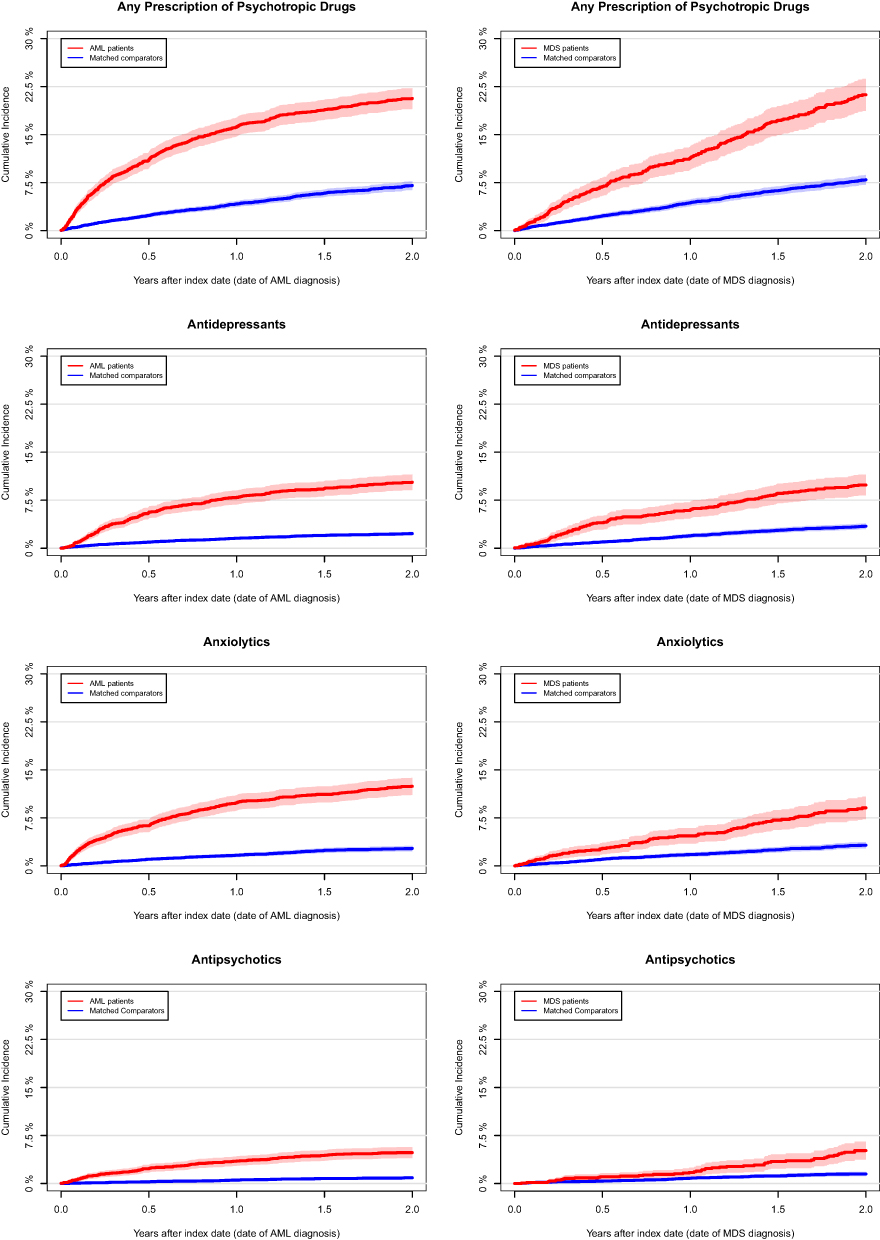 |
Figure 1 Cumulative incidence curves of time to first prescription of psychotropic drugs (antidepressants, anxiolytics, and antipsychotics) for any psychotropic drug and stratified by type of psychotropic drug in acute myeloid leukaemia (AML), myelodysplastic syndrome (MDS), and the matched comparators. For all four cumulative incidence curves, Gray’s test demonstrated that the cumulative incidences of time to first psychotropic drug prescription were significantly higher (P<0.05) in both AML and MDS patients compared to the matched comparators. |
Antidepressants (2-year risk, AML: 10.3%; MDS: 9.9%) and anxiolytics (2-year risk, AML: 12.4%; MDS: 9.1%) were the most prescribed psychotropic drugs (Figure 1) in both AML and MDS patients. When hypnotics were included, the 2-year cumulative incidence increased to 36.1% (95% CI 34.1–38.1) in AML patients and 27.0% (95% CI 24.4–29.5) in MDS patients compared to 15.4% (95% CI 14.7–16.1) and 11.8% (95% CI 11.0–12.7) in the respective background populations (Figure S1).
The sensitivity analysis in which an event was defined as prescription of at least two psychotropic drugs showed a consistent higher incidence of prescriptions in patients compared to the background populations (Figure 2).
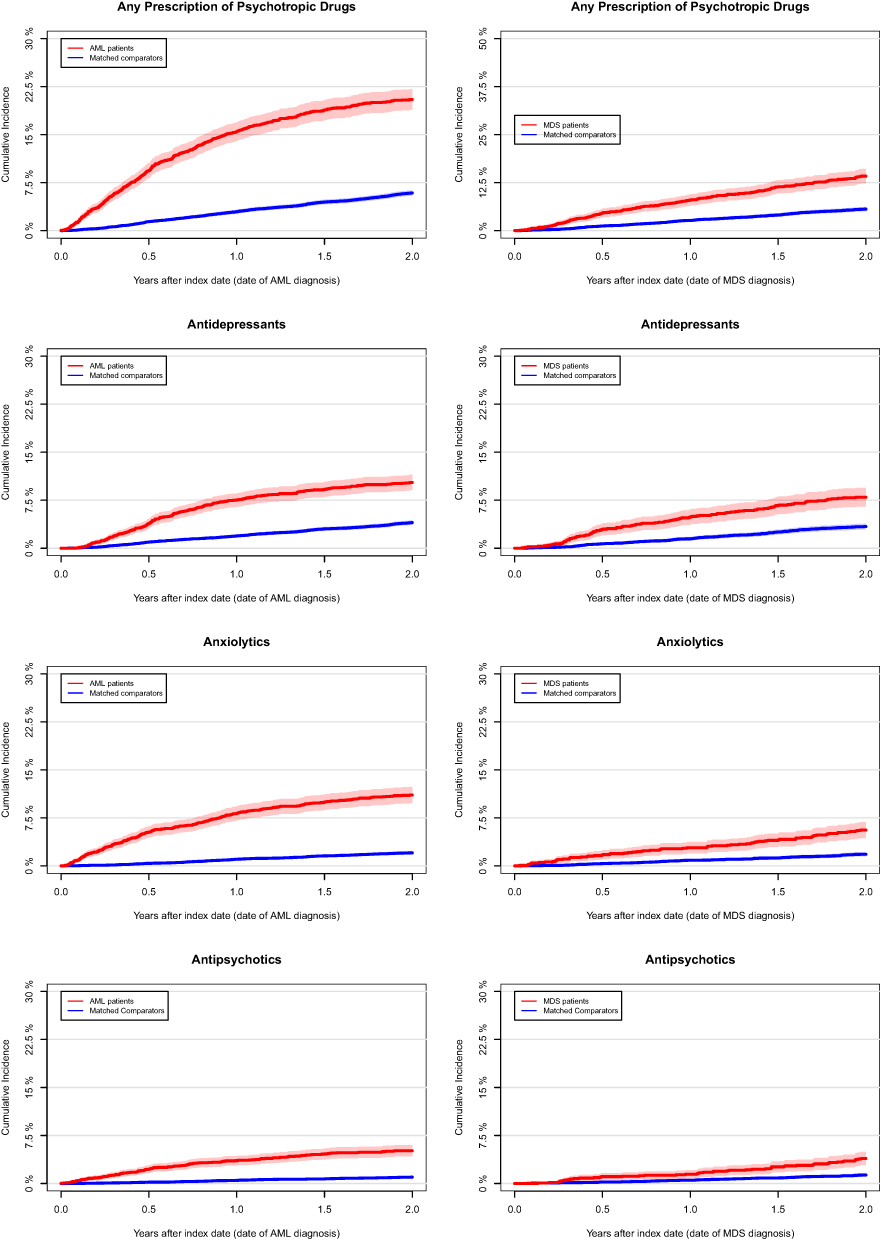 |
Figure 2 Cumulative incidence curves of time to second prescription of psychotropic drugs (antidepressants, anxiolytics, and antipsychotics) for any psychotropic drug and stratified by type of psychotropic drug in acute myeloid leukaemia (AML), myelodysplastic syndrome (MDS), and the matched comparators. For all four cumulative incidence curves Gray’s test demonstrated that the cumulative incidences of time to first psychotropic drug prescription were significantly higher (P<0.05) in both AML and MDS patients compared to the matched comparators. |
Figure 3 shows the cumulative incidence for incident psychotropic drug use from 2 years prior until 2 years after diagnosis of AML or MDS. This demonstrates that the incident prescription of psychotropic drug in AML and MDS patients was not different to the matched comparators prior to the index date. However, after the index date both AML and MDS patients were prescribed psychotropic drugs more often.
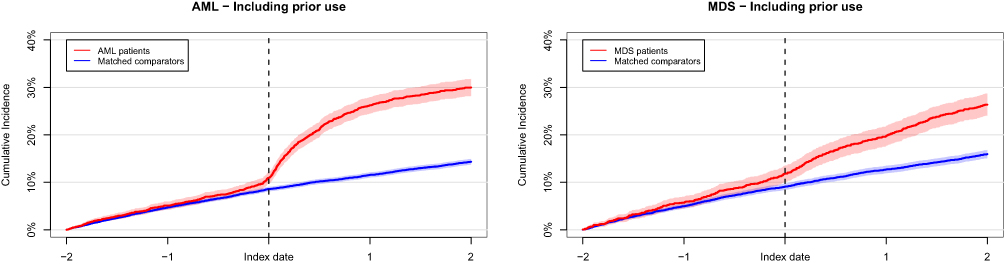 |
Figure 3 Cumulative incidence curves of time to first prescription from 2 years prior to 2 years after diagnosis of psychotropic drugs (antidepressants, anxiolytics, and antipsychotics) for any psychotropic drug in acute myeloid leukaemia (AML) and myelodysplastic syndrome (MDS) and the matched comparators. |
Risk Factors for Psychotropic Drug Prescriptions in AML and MDS Patients
Association between psychotropic drug prescriptions and clinically relevant variables in AML/MDS patients and matched comparators adjusted for age and sex are presented in Table 2. Increasing age, lower educational level, comorbidity (Charlson Comorbidity Index score ≥1), non-curative treatment intent, and poor performance status (score 1–4) were associated with higher risk of psychotropic drug prescription in AML patients. For MDS patients, increasing age, lower educational level, comorbidity (Charlson Comorbidity Index score ≥1), and high risk MDS (increasing IPSS-R score) were associated with elevated risk of psychotropic drug prescription. Sex, country of origin, and civil status did not impact psychotropic drug prescriptions in AML and MDS patients.
Discussion
In this nationwide study we showed that the 2-year cumulative incidence of psychotropic drug prescription was higher in AML (20.6%) and MDS (21.2%) patients as compared to the background population (7.0% and 7.9%). Importantly, before diagnosis no significant differences in psychotropic drug prescriptions were observed between AML/MDS patients and comparators. These results indicate that the stressful situation of being diagnosed with a potentially lethal disease, such as AML or MDS, was associated with redemption of prescriptions of treatment of depression and anxiety.
Increasing age, lower educational level, and comorbidity (Charlson Comorbidity Index score ≥1) were associated with prescription of psychotropic drugs in AML and MDS patients. Furthermore, non-curative treatment intent and poor performance status (score 1–4) in AML patients and high risk MDS (increasing IPSS-R score) were associated with psychotropic drug prescriptions, all of which are related to unfavourable outcome, which could result in a larger psychological stressor possibly explaining why these are risk factors for receiving a psychotropic drug prescription.10,29 Female sex is reported to be associated with increased risk of mental health issues in cancer patients, but this was not the case in our study.12 A likely explanation of this difference is the exclusion of patients who received any psychotropic drugs within one year prior to the index date in our study, which would exclude female patients with prevalent mental health issues.
AML and MDS patients had a higher overall 2-year cumulative incidence of psychotropic drug prescriptions compared to the background population (Figure 1). Antidepressants and anxiolytics were prescribed more often than antipsychotics in both AML and MDS patients. Moreover, the curve for AML patients shows a steep slope during the first year, after which it flattens out. MDS on the other hand has a less steep slope but does not flatten out like the curve for AML. Even though AML and MDS share similar symptoms and prognosis, the results suggest that MDS patients tend to start using psychotropic drugs at a later time point as compared to AML patients. This may be reasoned by the moderate onset of the disease, or because MDS patients do not realise the severity of the disease, as asymptomatic patients may not consider their diagnosis lethal.7,8
To the best of our knowledge, the prevalence of depression and anxiety has not been studied in MDS patients previously, and only few studies have investigated depression and anxiety in AML patients.
A recent study conducted by Ding et al2 assessed the prevalence and severity of depression and anxiety in 208 de novo AML patients (median age 48.6±14.1; male:female ratio 1.3) using the Hospital Anxiety and Depression Scale. The authors found that 58 (27.9%) of the AML patients fulfilled the criteria for depression and 81 (38.9%) for anxiety, which was significantly higher as compared to the healthy controls (10.0% depression, 12.5% anxiety). In an American study by El-Jawahri et al4 it was reported that the risk of depression and anxiety in older AML patients (median age 71, range 60–100; male:female ratio 1.6) receiving intensive and non-intensive chemotherapy were 33.3% and 30.0%, respectively, also using the Hospital Anxiety and Depression Scale. Using the Hospital Anxiety and Depression Scale, both studies were able to distinguish between depression and anxiety. Therefore, comparisons to our study should be made with precaution, as we were not able distinguish between depression and anxiety due to the use of psychotropic drug prescriptions. However, both studies support our findings of AML patients having higher risk of mental problems including depression and anxiety.
Linden et al12 investigated the prevalence of depression and anxiety prior to treatment in patients with various types of cancers by distributing questionnaires developed by the British Columbia Cancer Agency Centres. According to the Psychosocial Screen for Cancer (PSSCAN), 22.8% had depression and 16.9% had anxiety of patients in the subgroup with haematological cancers. Similarly, Linden et al12 showed a high risk of depression and anxiety in haematological cancer patients. However, as detailed information on type of haematological cancer was not provided, we were not able to directly compare the results with our study.
Usage of high-quality nationwide population-based registries enabled identification and inclusion of all eligible AML and MDS patients in Denmark ensuring high coverage, near to complete follow-up of all patients, and minimal risk of selection bias. Matching of patients with the Danish background population based on age, sex, and country of origin allowed identification of relevant comparators.
The study was subject to limitations. Firstly, an important limitation was the use of psychotropic drug prescriptions as a surrogate for depression and anxiety. According to national guidelines, pharmacological treatment of depression is only initiated when severity is moderate or severe.30,31 Therefore, our study included only patients with, supposedly, moderate or severe depression. In addition, indication for prescription of a psychotropic drug was not available and antidepressants are prescribed on various other indications than depression, such as pain and nausea management.32–34 However, this probably has less impact on the difference in cumulative incidences as this was the case for both patients and matched comparators. The use of psychotropic drug prescriptions as a surrogate measure for depression and anxiety was time- and cost-effective. It ensured high representability of the population as patients and comparators were not required to participate. And in contrast to questionnaire-based surveys it did not risk making patients and comparators notice symptoms of psychological distress they may not have considered otherwise. The use of psychotropic drug as a surrogate for the prevalence of depression and anxiety is a valid measure as all patients with moderate or severe depression and anxiety treated according to guidelines were included.
Secondly, symptoms of depression and anxiety such as insomnia, fatigue, unrest, and changes in appetite might be interpreted as a manifestation of the somatic disease, a side effect of the treatment, or a natural reaction to the deadly disease course, hereby, causing an underestimation of treatment-requiring depression and anxiety in AML and MDS patients. On the contrary, surveillance bias is introduced as AML and MDS patients are seen more frequently by a doctor as compared to the background population. Additionally, AML and MDS patients may have been prescribed psychotropic drugs due to an adjustment disorder, which share similar symptoms with depression, but which most commonly would be only treated briefly with benzodiazepine-like drugs and not antidepressants, antipsychotics, or anxiolytics. A meta-analysis which found the prevalence of adjustment disorders within 5 years of diagnosis was 19.4% in oncological and haematological settings, supported this notion.35
Thirdly, the amount of psychotropic drug prescriptions was not accounted for. In our study, prescription of an antidepressant was interpreted as having depression; however, one psychotropic drug prescription is not enough to treat depression of any severity. The sensitivity analysis with time to second prescription of any psychotropic drug showed results that resemble those using only one prescription of psychotropic drug as event. If a patient received at least two prescriptions of psychotropic drugs, we believe it is likely that the patient did have treatment requiring depression or anxiety. In this study we measure redemption of a prescription of psychotropic drugs. However, there could be prescriptions that had not been redeemed. Furthermore, we do not know if the medication had been used.
In conclusion, we showed that both AML and MDS patients were prescribed psychotropic drugs with a higher probability compared to the background population, most likely due to the stressful situation of being diagnosed with a cancer disease with a poor prognosis. The prescription risk was nearly identical in AML and MDS patients. In AML patients, the psychotropic drug prescriptions were initiated mainly during the first months after diagnosis, whereas in MDS patients, the prescriptions were more evenly distributed over follow-up time. Further research is required to identify the true incidence of depression and anxiety in AML and MDS patients using validated screening tools, such as the Hospital Anxiety and Depression Scale, Patient Health Questionnaire (PHQ-9), and Generalized Anxiety Disorder (GAD-7) by which also mild depression and anxiety may be identified.36,37 Furthermore, it is important to investigate the effect of psychological support and pharmacological therapy in a clinical setting to secure that the mental health issues following diagnosis of AML and MDS are treated properly.
Disclosure
Dr Andreas Kiesbye Øvlisen reports covered travel expenses from Pfizer and AbbVie, outside the submitted work. Dr Lasse Hjort Jakobsen reports personal fees from Takeda, outside the submitted work. Dr Christian Torp-Pedersen reports grants for randomised study from Bayer, grants for epidemiological study from Novo Nordisk, during the conduct of the study. Professor Tarec Christoffer El-Galaly was previously employed by Roche, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Deschler B, Lübbert M. Acute myeloid leukemia: epidemiology and etiology. Cancer. 2006;107(9):2099–2107. doi:10.1002/cncr.22233
2. Ding T, Wang X, Fu A, Xu L, Lin J. Anxiety and depression predict unfavorable survival in acute myeloid leukemia patients. Med (United States). 2019;98(43):1–7.
3. Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136–1152. doi:10.1056/NEJMra1406184
4. El-Jawahri A, Abel GA, Traeger L, et al. Quality of life and mood of older patients with acute myeloid leukemia (AML) receiving intensive and non-intensive chemotherapy. Leukemia. 2019;33:2393–2402. doi:10.1038/s41375-019-0449-1
5. Østgård LSG, Nørgaard JM, Raaschou-Jensen KK, et al. The Danish national acute leukemia registry. Clin Epidemiol. 2016;8:553–560. doi:10.2147/CLEP.S99460
6. Dan C, Chi J, Wang L. Molecular mechanisms of the progression of myelodysplastic syndrome to secondary acute myeloid leukaemia and implication for therapy. Ann Med. 2015;47(3):209–217. doi:10.3109/07853890.2015.1009156
7. Besson C, Rannou S, Elmaaroufi H, et al. Disclosure of myelodysplastic syndrome diagnosis: improving patients’ understanding and experience. Eur J Haematol. 2013;90(2):151–156. doi:10.1111/ejh.12048
8. Sekeres MA, Maciejewski JP, List AF, et al. Perceptions of disease state, treatment outcomes, and prognosis among patients with myelodysplastic syndromes: results from an internet‐based survey. Oncologist. 2011;16(6):904–911. doi:10.1634/theoncologist.2010-0199
9. Group TDAL. Annual leukemia report 2019 [in Danish]. Aarhus, Denmark; 2019.
10. Steensma DP. Myelodysplastic syndromes current treatment algorithm 2018. Blood Cancer J. 2018;8(5):47. doi:10.1038/s41408-018-0085-4
11. Montalban-Bravo G, Garcia-Manero G. Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and management. Am J Hematol. 2018;93(1):129–147. doi:10.1002/ajh.24930
12. Linden W, Vodermaier A, MacKenzie R, Greig D. Anxiety and depression after cancer diagnosis: prevalence rates by cancer type, gender, and age. J Affect Disord. 2012;141(2–3):343–351. doi:10.1016/j.jad.2012.03.025
13. Gheihman G, Zimmermann C, Deckert A, et al. Depression and hopelessness in patients with acute leukemia: the psychological impact of an acute and life-threatening disorder. Psychooncology. 2016;989:979–989. doi:10.1002/pon.3940
14. Ng CG, Boks MP, Smeets HM, Zainal NZ, De Wit NJ. Prescription patterns for psychotropic drugs in cancer patients; A large population study in the Netherlands. Psychooncology. 2013;22(4):762–767. doi:10.1002/pon.3056
15. Ng CG, Boks MPM, Zainal NZ, De Wit NJ. The prevalence and pharmacotherapy of depression in cancer patients. J Affect Disord. 2011;131(1–3):1–7. doi:10.1016/j.jad.2010.07.034
16. Jacob L, Kostev K, Kalder M. Treatment of depression in cancer and non-cancer patients in German neuropsychiatric practices. Psychooncology. 2016;25(11):1324–1328. doi:10.1002/pon.4066
17. Øvlisen AK, Jakobsen LH, Kragholm KH, et al. Depression and anxiety in Hodgkin lymphoma patients: a Danish nationwide cohort study of 945 patients. Cancer Med. 2020;9(12):4395–4404. doi:10.1002/cam4.2981
18. Hinz A, Krauss O, Hauss JP, et al. Anxiety and depression in cancer patients compared with the general population. Eur J Cancer Care (Engl). 2010;19(4):522–529. doi:10.1111/j.1365-2354.2009.01088.x
19. Pinquart M, Duberstein PR. Depression and cancer mortality: a meta-analysis. Psychol Med. 2010;40(11):1797–1810. doi:10.1017/S0033291709992285
20. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
21. Pedersen CB. The Danish Civil Registration System. Scand J Public Health. 2011;39(7):22–25. doi:10.1177/1403494810387965
22. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7):91–94. doi:10.1177/1403494810394715
23. Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. Dove Medical Press Ltd. doi:10.2147/CLEP.S91125
24. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sørensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med Res Methodol. 2011;11(1):83. doi:10.1186/1471-2288-11-83
25. Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish national prescription registry. Int J Epidemiol. 2017;46(3):798. doi:10.1093/ije/dyw213
26. Wallach Kildemoes H, Toft Sørensen H, Hallas J. The Danish National Prescription Registry. Scand J Public Health. 2011;39(7_suppl):38–41. doi:10.1177/1403494810394717
27. Granfeldt Østgård LS, Nørgaard JM, Severinsen MT, et al. Data quality in the Danish National acute Leukemia Registry: a hematological data resource. Clin Epidemiol. 2013;5(1):335–344. doi:10.2147/CLEP.S48411
28. Gray R. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat. 1988;16(3). doi:10.1214/aos/1176350951
29. Juliusson G, Antunovic P, Derolf Å, et al. Age and acute myeloid leukemia: real world data on decision to treat and outcomes from the Swedish Acute Leukemia Registry. Blood. 2009;113(18):4179–4187. doi:10.1182/blood-2008-07-172007
30. Sundhedsstyrelsen. Referenceprogram for unipolar depression hos voksne. [Internet]; [cited December 22, 2020]. Available from: http://sst.dk.
31. Sundhedsstyrelsen. National klinisk retningslinje for non-farmakologisk behandling af unipolar depression. [Internet]; [cited December 22, 2020]. Available from: http://sst.dk.
32. Peterson LG, Leipman M, Bongar B. Psychotropic medications in patients with cancer. Gen Hosp Psychiatry. 1987;9(5):313–323. doi:10.1016/0163-8343(87)90062-4
33. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci. 2001;26(1):30.
34. Skånland SS, Cieślar-Pobuda A. Off-label uses of drugs for depression. Eur J Pharmacol. 2019;865:172732. doi:10.1016/j.ejphar.2019.172732
35. Mitchell AJ, Chan M, Bhatti H, et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 2011;12(2):160–174. doi:10.1016/S1470-2045(11)70002-X
36. Esser P, Hartung TJ, Friedrich M, et al. The Generalized Anxiety Disorder Screener (GAD-7) and the anxiety module of the Hospital and Depression Scale (HADS-A) as screening tools for generalized anxiety disorder among cancer patients. Psychooncology. 2018;27(6):1509–1516. doi:10.1002/pon.4681
37. Vodermaier A, Linden W, Siu C. Screening for emotional distress in cancer patients: a systematic review of assessment instruments. J Natl Cancer Inst. 2009;101:1464–1488. doi:10.1093/jnci/djp336
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.