")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Psychometric Properties Of The Persian Version Of The Memory Impact Questionnaire In Older Adults
Authors Ebadi A , Ebtekar F , Parizad N , Afkhamzadeh A, Dalvand S, Ghanei Gheshlagh R
Received 12 September 2019
Accepted for publication 1 November 2019
Published 14 November 2019 Volume 2019:15 Pages 3197—3204
DOI https://doi.org/10.2147/NDT.S230823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Abbas Ebadi,1 Fariba Ebtekar,2 Naser Parizad,3 Abdorrahim Afkhamzadeh,4 Sahar Dalvand,5 Reza Ghanei Gheshlagh4
1Behavioral Sciences Research Center, Life-Style Institute, Faculty of Nursing, Baqiyatallah University of Medical Sciences, Teheran, Iran; 2Department of Midwifery, Faculty of Nursing and Midwifery, Kurdistan University of Medical Sciences, Sanandaj, Iran; 3Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Urmia University of Medical Sciences, Urmia, Iran; 4Social Determinants of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj, Iran; 5Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
Correspondence: Reza Ghanei Gheshlagh
Social Determinants of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj 575611-5111, Iran
Tel +98 9144050284
Fax +98 36235450
Email [email protected]
Background and aim: Memory impairment in the elderly has a high prevalence and can affect their performance, interactions and quality of life. A valid and reliable questionnaire is required to investigate the changes in the memory of the elderly. The aim of this study was to investigate the psychometric properties of the Persian version of the Memory Impact Questionnaire (MIQ) in the elderly.
Methods: In this methodological study, 361 elderly people (181 people for exploratory factor analysis and 180 people for confirmatory factor analysis) were selected via convenience sampling. This questionnaire was translated based on the World Health Organization’s (WHO) guidelines. Construct validities were assessed through exploratory and confirmatory factor analyses. Its reliability was also assessed using Cronbach’s alpha coefficient.
Results: In the exploratory factor analysis, three factors of lifestyle restrictions, positive coping, and negative emotion were extracted that were able to explain 54.04% of the total variance of the impact of memory change in the elderly. Confirmatory factor analysis confirmed the goodness of fit of the three-factor model of MIQ (RMSEA: 0.083; GFI: 0.97; NFI: 0.94; IFI: 0.97; PNFI: 0.86; AGFI: 0.75). The reliability of the “lifestyle restrictions”, “negative emotion” and “positive coping” factors was found to be 0.89, 0.74, and 0.67, respectively, using Cronbach’s alpha coefficient.
Conclusion: The Persian version of the MIQ is simple and practical and has acceptable reliability and validity that can be used to measure memory changes in the Iranian elderly.
Keywords: psychometrics, elderly, memory
Introduction
There are five types of memories in human beings, including procedural memory, perceptual representation systems, semantic memory, working memory and episodic memory that refer to motor task performance, rapid identification of previous stimuli, general knowledge, ability to hold and manipulate information in mind and recall personal events and experiences, respectively.1–8 Memory changes are well known in old age, whether in research and/or in popular culture, and aging has major effects on different types of memory.9
Subjective memory complaints (SMCS) are perceived experiences of everyday forgetting, which is a common phenomenon in young, middle-aged and elderly people.10 SMC has a high prevalence among healthy elderly people, so that between 27% and 43% of elderly people suffer from memory problems.11 SMC is highly prevalent among the healthy elderly population. Several studies have reported different results in this regard so that in the study of Tobiansky et al (1995), 27% of the elderly and in the study of Jonker et al (1996) 34% of healthy elderly without depression had memory problems.12,13 These problems increase with age so that the rate of memory problems was reported to be 47% in the elderly between 65 and 74 years and 88% among the elderly over 85 years old.14 Memory errors also occur in the daily lives of healthy older adults. Healthy elderly are often experiencing a memory error in the field of verbal domain (such as the tip-of-the-tongue phenomenon, forgetting the names and recently learned information).15 Other memory error is associated with forgetting what they have read recently or where they put their belongings.16,17
Given that memory problems are criteria for recognizing dementia, physicians and other health care providers are suspected of dementia based on mental impairment in patients.18 The relationship between cognitive impairment and SMC has always been controversial. Some studies have also pointed to the direct relationship between SMC and cognitive impairment and the incidence of dementia.19,20 Some other researchers believe that memory problems occur before the onset of dementia,21,22 and some also consider the SMC as the main symptom of mild cognitive problems.23 These disagreements show the importance of measuring SMC more than ever before.
Memory problems affect the daily performance (purchasing, financial management) and behavior and are associated with the health-related quality of life of the elderly.24 In sum, it can be said that the memory problems affect emotions and views, social interactions and relationships, work and recreational activities of the elderly.11 Identifying and early detection of memory problems allows us to slow down the progression of these neurodegenerative diseases through specific interventions. SMC can be measured by two methods of asking questions directly from a person and providing a questionnaire for response. These two methods of measurement, although not the same, are correlated.25 Most studies use only one question to assess SMC (Do you have a memory problem?).26 Also, some studies have shown that direct evaluation of memory problems is reliable by asking one question and it can identify neurodegenerative diseases.27,28
Reid and MacLullich (2006) reviewed 21 SMC studies. They found that in 40% of these studies, the SMC was evaluated only by asking one question about a memory complaint with a yes/no response (18).3 Considering the problem of measuring the memory changes in the elderly due to the lack of appropriate measuring instruments, the primary objective of this study is to examine the psychometric properties of the Persian version of the Memory Impact Questionnaire (MIQ) in the elderly.
Methods
Design And Setting
The present study is a methodological and cross-sectional descriptive study that was carried out in Sanandaj, west of Iran, in 2018–2019. The sample size is estimated based on the number of items in the tool. The minimum sample size required to conduct exploratory analysis is 3 to 10 samples per item;29 so, we chose 181 participants.
Characteristics Of Participants
In this study, 250 elderly people were selected in public places such as parks, cinemas, mosques, public stores and local markets via convenience sampling. The inclusion criteria were age over 60 and having at least reading and writing skills and the desire to complete the questionnaire. 69 questionnaires were excluded due to incompleteness. Finally, 181 completed questionnaires were analyzed.
Research Tool
The MIQ was designed by Shaikh et al (2018) and tested on the elderly. This questionnaire has 51 items with 5-point Likert responses (0 Disagree; 1 somewhat agree; 2 neither agree nor disagree; 3 somewhat agree; 4 agree). The main questionnaire has three subscales of Lifestyle Restriction (19 items), Positive Coping (19 items) and Negative Emotion (13 items). Scores of three subscales of lifestyle restriction, positive coping and negative emotion are 0 to 76, 0 to 76 and 0 to 52, respectively. Higher scores mean more effects of memory changes.11 The average factor loading of these three dimensions was 0.57, 0.53 and 0.68, respectively. These dimensions had a total eigenvalue of 18.4, 8.3 and 3.7, respectively, which explained 2.24%, 10.9% and 4.9% of the total variance. The internal consistency of these three dimensions was 0.91, 0.87 and 0.93, respectively, and the internal consistency of the whole tool was 0.83.11
Translation Process
After obtaining permission from the original designer, according to the WHO guidelines and using the Forward & Backward method, the questionnaire was translated from English into Persian and then translated back into English.30 Finally, one person coordinates Persian and English versions together and provided the final Persian version. Finally, the research team matched the Persian and English versions and the final version was prepared.
Face And Content Validities
To evaluate the psychometric properties of the MIQ, face, content and construct validity were used. The face validity was done qualitatively. At this stage, 10 elderly patients were selected and asked to read the questionnaire carefully and give us their opinion about the appearance of questionnaire items. Content validity was assessed by both qualitative and quantitative methods. In the qualitative content validity, the final Persian version of the questionnaire was sent to 10 experts who were selected purposefully and asked them to check the content of the questionnaire in terms of Persian grammar, the use of appropriate words and the proper placement of phrases. Content validity index (CVI) was used to check content validity by a quantitative approach. We sent the questionnaire to 15 specialists who are expert in the field of memory changes and aging in order to assess the cultural relevancy of the questionnaire items and select one of the options of 1 (not relevant), 2 (requires review), 3 (it is relevant but requires partial review), 4 (it is quite relevant) for each item. To calculate the CVI score for each item, the total number of specialists who gave each item a score of 3 and 4 divided by the total number of specialists. CVI score of higher than 0.79 is considered appropriate and if it is between 0.70 and 0.79 needed to be re-checked and revised. Items that score below 0.70 are also eliminated.31
Data Analysis
Data analysis was done with SPSS version 18 and Lisrel software version 8.8. In order to determine the internal consistency of the MIQ questionnaire, Cronbach’s alpha coefficient was used. To assess corrected item-total correlations, interitem correlations and Cronbach’s alpha-if item-deleted, we performed item analysis. The corrected item-total correlations and interitem correlations 0.3 to 0.7 are satisfactory.32 Also, the Cronbach’s alpha coefficient 0.7 to 0.9 indicates appropriate reliability.33 To evaluate the initial reliability and to determine which items affect the reliability, the item analysis was performed. For this purpose, MIQ was distributed among 30 elderly people who were selected by convenience sampling.
To investigate the construct validity, exploratory factor analysis (EFA) was used to extract latent factors. At this stage, the latent factors were extracted and the Kaiser Meyer Alkin Index (KMO) and the Bartlett test were calculated.29 KMO values ranging from 0.70 to 0.80 and from 0.80 to 0.90 were considered good and excellent, respectively.34,35 We extracted the latent factors by maximum likelihood using promax rotation (assuming that the factors are dependent) and the scree plot. The minimum factorial load of 0.3 was considered.36 It is recommended that the sample size used for confirmatory factor analysis is not less than 200 people,29 so 200 new samples of elderly people were selected from the public places via convenience sampling. Twenty incomplete questionnaires were excluded from the analysis and confirmatory factor analyses were performed on another 180 questionnaires.
At this stage, extracted factors with confirmatory factor analysis common model fit indices, such as goodness of fit, root mean of squares of approximation, comparative index of fitness, standardized normal goodness index and goodness index of adjusted fit, were assessed. The threshold for acceptance of the fitting indicators of the model is given in Table 1.37
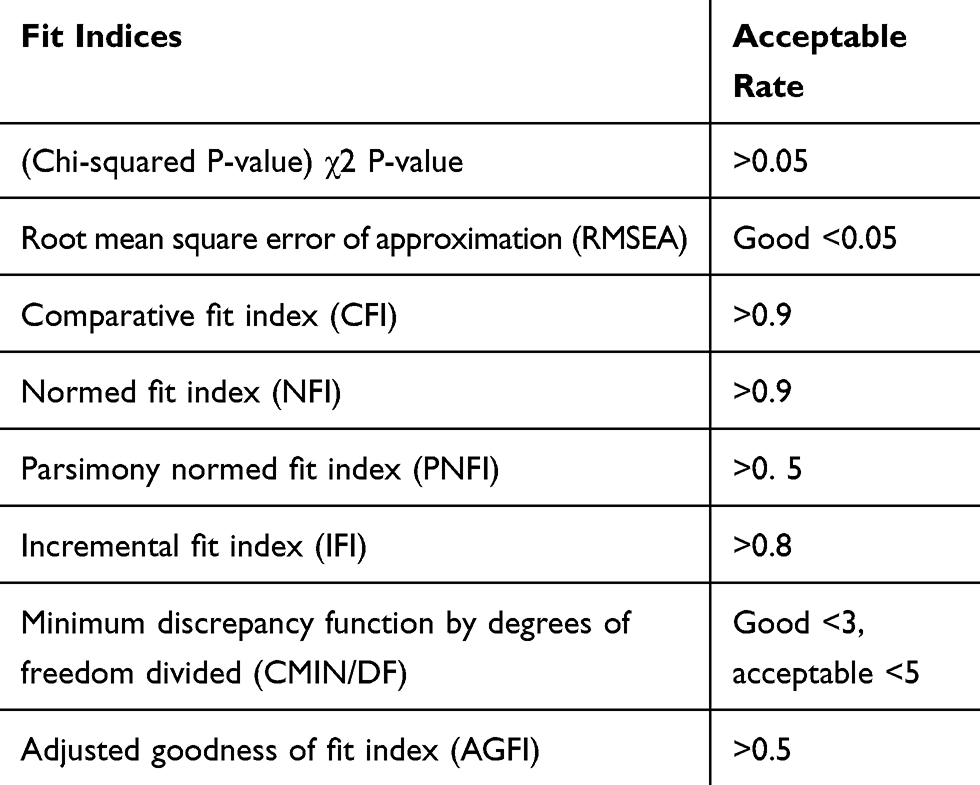 |
Table 1 Acceptable Thresholds Of The Fit Indices In The Confirmatory Factor Analysis Model |
Ethical Consideration
The present article was extracted from a research project at Kurdistan University of Medical Sciences (IR.MUK.REC.1397/160). Before being included in the study, the participants were informed about the study objectives, and their verbal consents (this is accepted and approved by the Ethics Committee of Kurdistan University of Medical Sciences) were obtained. In addition, they were reassured that their personal information remained completely confidential. We already contacted Oxford University Press and asked them for their permission, also I already had got permission for the scale designer (Dr Sheikh). We filled out an online form as their request and are waiting for their response. So, we are in the process of getting their permission.
Results
The elderly participated in the study including 66 males and 115 females with an average age of 68.88 ± 7.09 years, with a range of 60 to 94 years old. Most of the elderly were housewives and retirees (75.7%) and married (63.5%) and had high school education level (40.9%). Nearly half of them (44.8%) had a monthly income of 10 to 20 million rials, and 39.2% of them were completely dissatisfied with their income. The qualitative face and content validities were confirmed and applied after reviewing the views of the elderly and qualified specialists. The demographic characteristics of the two selected samples are presented in Table 2.
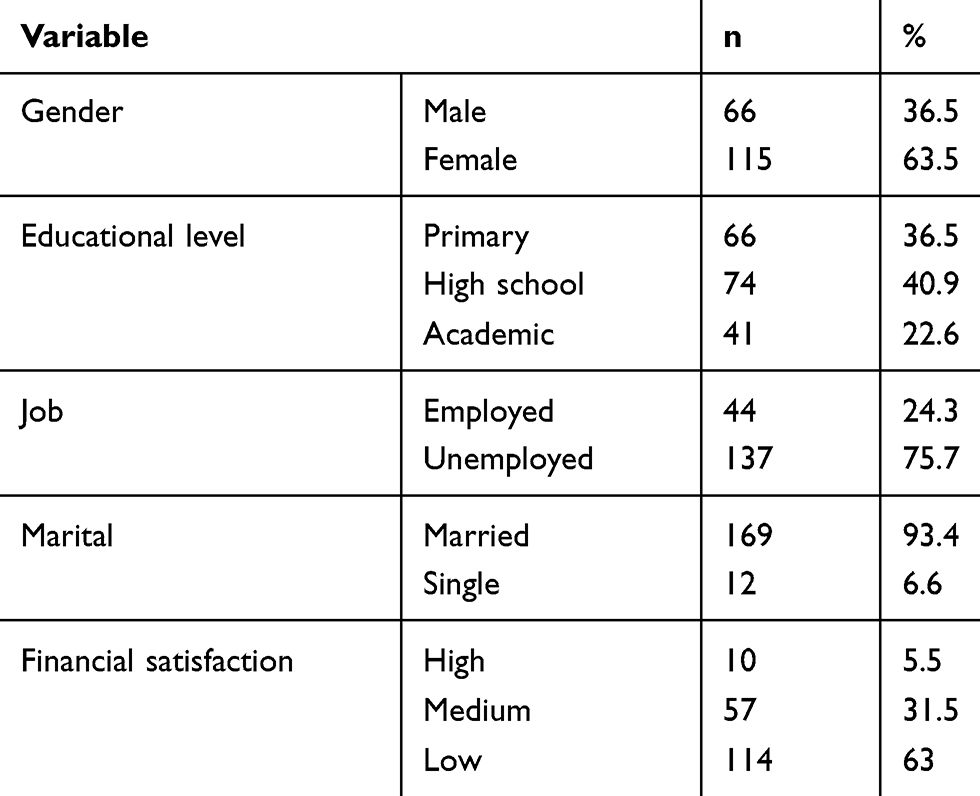 |
Table 2 Demographic Characteristics Of Samples |
Initially, confirmatory factor analysis was performed that the model did not fit and the fit indices were not optimal. Thus, we conducted exploratory factor analysis.
The KMO indicated sampling adequacy (KMO=0.86). Bartlett’s test of sphericity was statistically significant (X2=1062.6, df =78, P=0.001). Initial exploratory analysis with likelihood maximum and PCA showed that the variety of factors is high. Some items were not included in any factor. Therefore, we performed item analysis after calculating the internal consistency, and we eliminated items that had a very low correlation (less than 0.20) with the total score and the score of the other items (items 5, 15, 21, 24, 38, 40 and 43). Factor analysis was performed again. The results showed that 10 items (47, 45, 27, 6, 31, 28, 38, 2, 18 and 8) were not included in any factor; therefore, they were eliminated (8, 18, 2, 38, 28, 31, 6, 27, 45 and 47). Finally, for the third time, factor analysis was performed and items 12, 16, 30, 10, 19 and 51 were deleted. In the exploratory factor analysis, three factors were extracted: lifestyle restrictions (items 25, 37, 46, 33, 13, 29, 9, 36, 48, 7, 14, 39, 41, 17, 44 and 1), negative emotion (items 3, 20, 22 and 34) and positive coping (items 4, 8, 11, 26 and 35), respectively, having the eigenvalues of 7.24, 2.21 and 1.65, respectively, and they were able to explain 54.04% of the total variance of the impact of memory change in the elderly (Table 3). Also the correlation between the extracted factors is presented in Table 4.
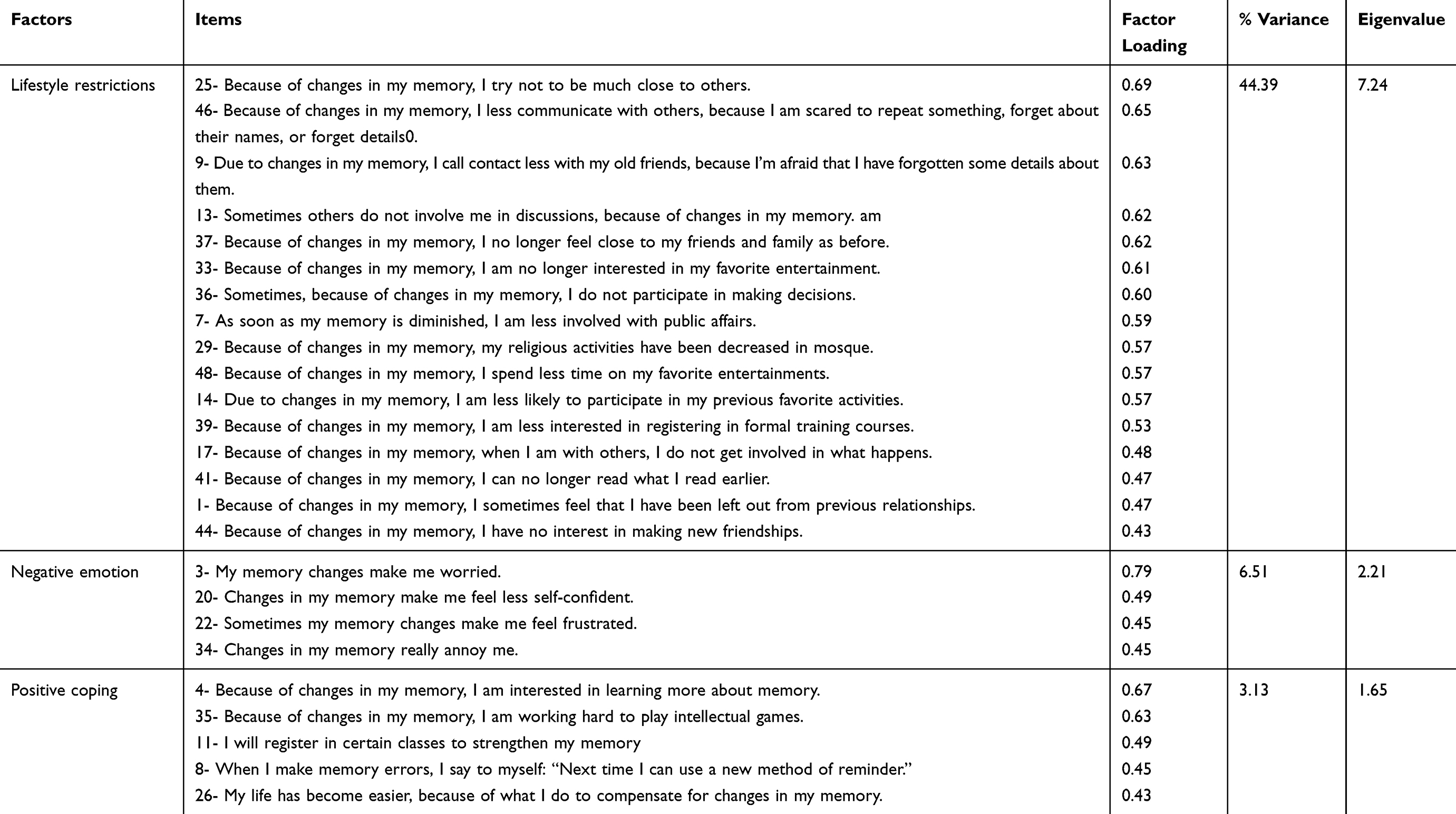 |
Table 3 The Results Of Exploratory Factor Analysis, Extracted Factors, Eigenvalues And Predicted Variance Percentages |
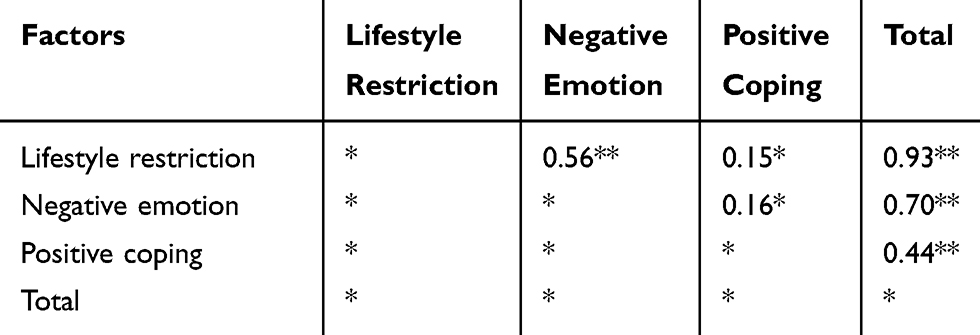 |
Table 4 The Correlation Of The Three Subscales |
To confirm the confirmatory factor, the questionnaires were again distributed to 200 elderly people and confirmatory factor analysis was performed on 180 return questionnaires. First, the Chi-square goodness of fit test was performed (X2=609.91, P=0.01). In order to evaluate the fitting of the model, we examined other indicators, all confirming the fitness fit for the final model: RMSEA: 0.083; CFI: 0.97; NFI: 0.94; IFI: 0.97; PNFI: 0.86; AGFI: 0.75, CMIN/df: 2.24. Overall, the results showed that the confirmatory factor analysis based on the three-factor model derived from the exploratory factor analysis has a relatively good fit with the obtained data (Figure 1).
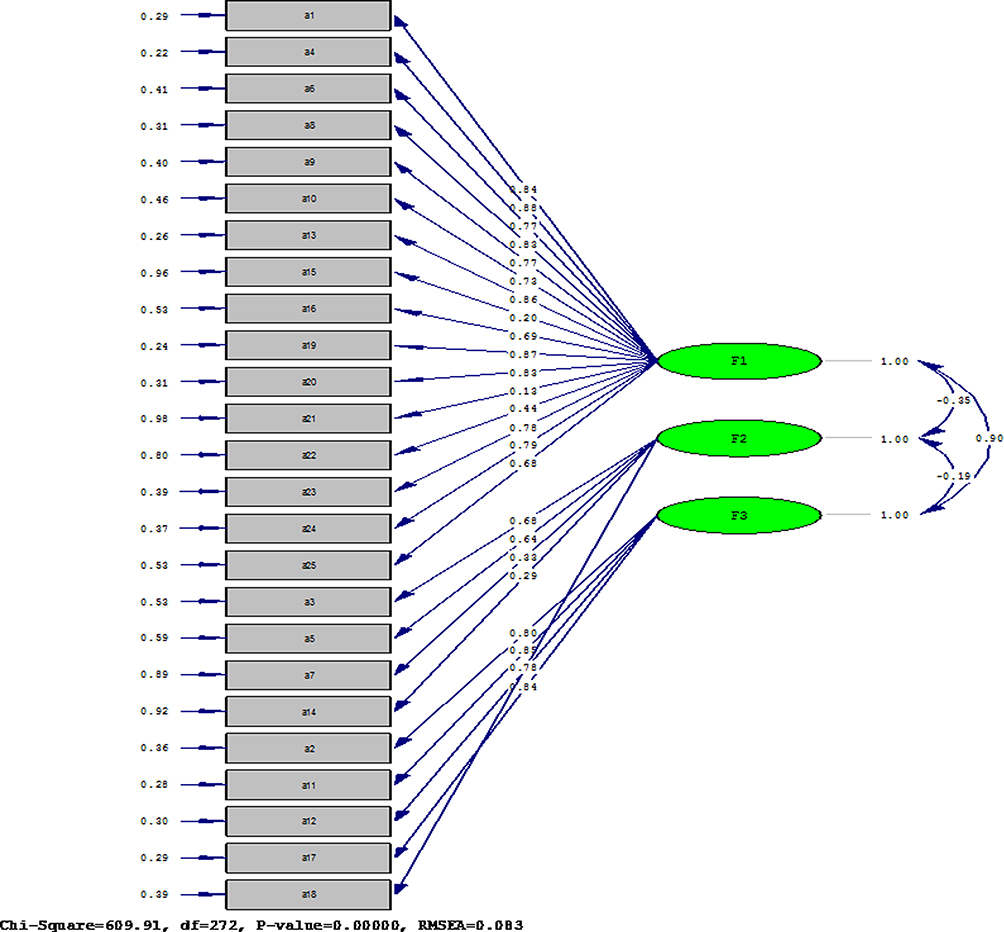 |
Figure 1 The final structure of the model. |
Reliability was performed with Cronbach’s alpha. The Cronbach’s alpha coefficient for the whole tool was 0.87. The reliability of the “lifestyle restrictions,” “negative emotion” and “positive coping” was, respectively, 0.89, 0.74 and 0.67 using Cronbach’s alpha coefficient.
Discussion
This methodological study was conducted to investigate the psychometric properties of the Persian version of the questionnaire assessing the impact of memory changes in older adults. Based on exploratory factor analysis findings and in accordance with the results of Shaikh et al, three factors of lifestyle restrictions, negative emotion and positive coping were extracted. These factors were able to explain 54.04% of the total variance of MIQ in the elderly, which was more than the total variance explained in the original questionnaire (37.4%).11
The first factor (lifestyle restrictions) had an eigenvalue of 11.460 and explained 44.396% of the overall variance. In the original version, this factor had an eigenvalue of 18.4% and explained 24.2% of the total variance of MIQ of the elderly. This item has 16 items in the Persian version and 19 items in the original questionnaire. All 16 items in the Persian version were in the original version. This dimension shows the negative effects of memory changes on social relationships, work and activities. The results of Flöel et al (2008) showed that there was a positive and significant correlation between lifestyle index score with better memory score; this means that with the increase in the score of the lifestyle index, a better memory score was also increased.38 In the qualitative study of Parikh et al (2015), on the elderly with memory problems, two themes of change in life activities and changes in social relationships and social interactions were extracted that are consistent with this factor.39
The second factor (negative emotion) had an eigenvalue of 2.222 which explained 6.512.6% of the overall variance. In the original version, this factor had a special value of 3.7% and components account for 4.9% of the variance in total scores. In the Persian version, this factor has 4 items and in the original version, it has 13 items. These items refer to negative emotions such as worries, loss of confidence, frustration and harassment that the elderly experiences due to memory changes. The third factor (positive coping) in this study had an eigenvalue of 1.289 and explained 3.136% of the overall variance. In the original version, this dimension had an eigenvalue of 8.3 and explained 10.9% of the total variance of memory impairment. In the Persian version, this factor has five items and in the original version, it has 19 items. All of these five items of the Persian version were in the same dimension of the original version. These items refer to things like the desire to learn about memory, doing mental games, enrolling in memory boost classes, and doing things to compensate for memory impairment.
In a study by Parikh et al (2015), one of the extracted themes was deliberate increases in compensatory behavior that is consistent with this factor.39
The Cronbach’s alpha coefficient was 0.876 for the whole instrument. It was 0.892 for lifestyle restriction, 0.747 for negative emotions and 0.671 for positive coping. In the main study, Cronbach’s alpha coefficient for three subscales was 0.91, 0.87 and 0.93, respectively. When comparing the internal consistency of the Persian version with the original version, it is necessary to note that the number of items in the Persian version is less than the original version. Devellis believes that the Cronbach’s alpha coefficient between 0.7 and 0.9 indicates good reliability, which is almost consistent with the internal consistency of our questionnaire subscales.33
So far, there has not been a Persian questionnaire for evaluating the elderly’s memory change and the existence of such a valid and reliable tool can be very useful in future studies. One of the limitations of this study was that the samples were not randomly selected, so this sample might not be representative of the Iranian elderly community. Given the few studies in this field, it was not possible to report the results of other studies and compare the findings. In general, the Persian version of the MIQ is simple and practical and has acceptable reliability and validity that can be used to measure memory impact changes in the Iranian elderly. Since the number of items in this questionnaire is low, Iranian elderly people who are often low educated or illiterate can more easily complete it.
Acknowledgement
The authors offer special thanks to the deputy of the Kurdistan University of Medical Sciences for providing financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Churchill JD, Stanis JJ, Press C, Kushelev M, Greenough WT. Is procedural memory relatively spared from age effects? Neurobiol Aging. 2003;24(6):883–892. doi:10.1016/S0197-4580(02)00194-X10.1159/000096295
2. Daselaar SM, Rombouts SA, Veltman DJ, Raaijmakers JG, Jonker C. Similar network activated by young and old adults during the acquisition of a motor sequence. Neurobiol Aging. 2003;24(7):1013–1019. doi:10.1016/S0197-4580(03)00030-7
3. Geraci L, Barnhardt TM. Aging and implicit memory: examining the contribution of test awareness. Conscious Cogn. 2010;19(2):606–616. doi:10.1016/j.concog.2010.03.015
4. Geraci L, Hamilton M, Guillory JJ. Age effects in implicit memory: the role of response competition induced by relative word frequency. Exp Aging Res. 2015;41(5):496–509. doi:10.1080/0361073X.2015.1085745
5. Kennedy KM, Rodrigue KM, Bischof GN, Hebrank AC, Reuter-Lorenz PA, Park DC. Age trajectories of functional activation under conditions of low and high processing demands: an adult lifespan fMRI study of the aging brain. Neuroimage. 2015;104:21–34. doi:10.1016/j.neuroimage.2014.09.056
6. Verhaeghen P. Aging and vocabulary score: a meta-analysis. Psychol Aging. 2003;18(2):332. doi:10.1037/0882-7974.18.2.332
7. Facal D, Juncos-Rabadán O, Guardia-Olmos J, Pereiro AX. Temporal changes in semantic and lexical access related to mild cognitive impairment. Aging Clin Exp Res. 2016;28(3):497–504. doi:10.1007/s40520-015-0436-y
8. Luo L, Craik FI. Aging and memory: a cognitive approach. Can J Psychiatry. 2008;53(6):346–353. doi:10.1177/070674370805300603
9. Shaikh KT Development and validation of the memory impact questionnaire. York University, 2016 [Dissertation].
10. Montejo P, Montenegro M, Fernández MA, Maestú F. Subjective memory complaints in the elderly: prevalence and influence of temporal orientation, depression and quality of life in a population-based study in the city of Madrid. Aging Ment Health. 2011;15(1):85–96. doi:10.1080/13607863.2010.501062
11. Shaikh KT, Tatham EL, Parikh PK, McCreath GA, Rich JB, Troyer AK. Development and psychometric validation of a question naire assessing the impact of memory changes in older adults. Gerontologist. 2018;1–10.
12. Tobiansky R, Blizard R, Livingston G, Mann A. The Gospel Oak Study stage IV: the clinical relevance of subjective memory impairment in older people. Psychol Med. 1995;25(4):779–786. doi:10.1017/S0033291700035029
13. Jonker C, Launer LJ, Hooijer C, Lindeboom J. Memory complaints and memory impairment in older individuals. J Am Geriatr Soc. 1996;44(1):44–49. doi:10.1111/jgs.1996.44.issue-1
14. Larrabee GJ, Crook TH. Estimated prevalence of age-associated memory impairment derived from standardized tests of memory function. Int Psychogeriatr. 1994;6(1):95–104. doi:10.1017/S1041610294001663
15. Ossher L, Flegal KE, Lustig C. Everyday memory errors in older adults. Aging Neuropsychol Cogn. 2013;20(2):220–242. doi:10.1080/13825585.2012.690365
16. Farias ST, Mungas D, Reed BR, Harvey D, Cahn-Weiner D, DeCarli C. MCI is associated with deficits in everyday functioning. Alzheimer Dis Assoc Disord. 2006;20(4):217–223. doi:10.1097/01.wad.0000213849.51495.d9
17. Smith G, Del Sala S, Logie RH, Maylor EA. Prospective and retrospective memory in normal ageing and dementia: a questionnaire study. Memory. 2000;8(5):311–321. doi:10.1080/09658210050117735
18. Reid LM, MacLullich AM. Subjective memory complaints and cognitive impairment in older people. Dement Geriatr Cogn Disord. 2006;22(5–6):471–485. doi:10.1159/000096295
19. Wang PN, Wang SJ, Fuh JL, et al. Subjective memory complaint in relation to cognitive performance and depression: a longitudinal study of a rural Chinese population. J Am Geriatr Soc. 2000;48(3):295–299. doi:10.1111/j.1532-5415.2000.tb02649.x
20. Antikainen R, Hänninen T, Honkalampi K, et al. Mood improvement reduces memory complaints in depressed patients. Eur Arch Psychiatry Clin Neurosci. 2001;251(1):6–11. doi:10.1007/s004060170060
21. Palmer K, Bäckman L, Winblad B, Fratiglioni L. Detection of alzheimer’s disease and dementia in the preclinical phase: population based cohort study. BMJ. 2003;326(7383):245–250. doi:10.1136/bmj.326.7383.245
22. St John P, Montgomery P. Are cognitively intact seniors with subjective memory loss more likely to develop dementia? Int J Geriatr Psychiatry. 2002;17(9):814–820. doi:10.1002/(ISSN)1099-1166
23. Balash Y, Mordechovich M, Shabtai H, Giladi N, Gurevich T, Korczyn A. Subjective memory complaints in elders: depression, anxiety, or cognitive decline? Acta Neurol Scand. 2013;127(5):344–350. doi:10.1111/ane.2013.127.issue-5
24. Frank L, Lloyd A, Flynn JA, et al. Impact of cognitive impairment on mild dementia patients and mild cognitive impairment patients and their informants. Int Psychogeriatr. 2006;18(1):151–162. doi:10.1017/S1041610205002450
25. Abdulrab K, Heun R, Subjective Memory Impairment. A review of its definitions indicates the need for a comprehensive set of standardised and validated criteria. Eur Psychiatry. 2008;23(5):321–330. doi:10.1016/j.eurpsy.2008.02.004
26. Kaup AR, Nettiksimmons J, LeBlanc ES, Yaffe K. Memory complaints and risk of cognitive impairment after nearly 2 decades among older women. Neurology. 2015;85(21):1852–1858. doi:10.1212/WNL.0000000000002153
27. Schofield PW, Jacobs D, Marder K, Sano M, Stern Y. The validity of new memory complaints in the elderly. Arch Neurol. 1997;54(6):756–761. doi:10.1001/archneur.1997.00550180064014
28. Geerlings MI, Jonker C, Bouter LM, Adèr HJ, Schmand B. Association between memory complaints and incident alzheimer’s disease in elderly people with normal baseline cognition. Am J Psychiatr. 1999;156(4):531–537. doi:10.1176/ajp.156.4.531
29. Plichta SB, Kelvin EA, Munro BH. Munro S Statistical Methods for Health Care Research. Wolters Kluwer Health/Lippincott Williams & Wilkins; 2013.
30. Instruments. WPotaao. Available from: http://www.who.int/substance_abuse/AfUr.
31. Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2009.
32. Ferketich S. Focus on psychometrics. Aspects of item analysis. Res Nurs Health. 1991;14(2):165–168. doi:10.1002/nur.4770140211
33. DeVellis RF. Scale Development: Theory and applications. Sage publications; 2016.
34. Mokhlesi S, Kariman N, Ebadi A, Khoshnejad F, Dabiri F. Psychometric properties of the questionnaire for urinary incontinence diagnosis of married women of Qom city in 2015. J Rafsanjan Univ Med Sci. 2016;15(10):955–966.
35. Nia HS, Ebadi A, Lehto RH, Mousavi B, Peyrovi H, Chan YH. Reliability and validity of the persian version of templer death anxiety scale-extended in veterans of Iran–iraq warfare. Iran J Psychiatry Behav Sci. 2014;8(4):29.
36. Vakili MM, Hidarnia AR, Niknami S. Development and psychometrics of an interpersonal communication skills scale (ASMA) among Zanjan health volunteers. J Hayat. 2012;18(1):5–19.
37. Sharif Nia H, Pahlevan Sharif S, Goudarzian AH, Haghdoost AA, Ebadi A, Soleimani MA. An evaluation of psychometric properties of the templer’s death anxiety scale-extended among a sample of Iranian chemical warfare veterans. J Hayat. 2016;22(3):229–244.
38. Flöel A, Witte AV, Lohmann H, et al. Lifestyle and memory in the elderly. Neuroepidemiology. 2008;31(1):39–47. doi:10.1159/000137378
39. Parikh PK, Troyer AK, Maione AM, Murphy KJ. The impact of memory change on daily life in normal aging and mild cognitive impairment. Gerontologist. 2015;56(5):877–885. doi:10.1093/geront/gnv030
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.