")
Back to Journals » International Journal of Women's Health » Volume 12
Psychometric Properties of the Persian Version of Mental Health Literacy Scale
Authors Heizomi H , Kouzekanani K , Asghari Jafarabadi M , Allahverdipour H
Received 3 March 2020
Accepted for publication 9 June 2020
Published 6 July 2020 Volume 2020:12 Pages 513—520
DOI https://doi.org/10.2147/IJWH.S252348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Haleh Heizomi,1 Kamiar Kouzekanani,2 Mohammad Asghari Jafarabadi,3,4 Hamid Allahverdipour5
1Department of Health Education and Promotion, Tabriz University of Medical Sciences, Tabriz, Iran; 2College of Education and Human Development, Texas A&M University-Corpus Christi, Corpus Christi, TX, USA; 3Road Traffic Injury Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 4Department of Statistics and Epidemiology, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran; 5Research Center of Psychiatry and Behavioral Sciences and Department of Health Education and Promotion, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Hamid Allahverdipour
Research Center of Psychiatry and Behavioral Sciences and Department of Health Education and Promotion, Tabriz University of Medical Sciences, Tabriz 14711, Iran
Tel/Fax +98-411-3344731
Email [email protected]
Background: Due to the lack of an instrument to measure mental health literacy among Persian/Farsi speaking people, this study was conducted to examine the psychometric properties of the Persian version of the Mental Health Literacy Scale (P-MHLS).
Participants and Methods: The 2019 cross-sectional study with 992 participants was conducted in Tabriz, Iran. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were performed to establish the construct validity of the P-MHLS. The internal consistency/reliability was estimated by computing Cronbach’s coefficient alpha. Feasibility of the scale was examined and item response theory (IRT) models were applied to characterize the test items.
Results: An exploratory factor analysis of data resulted in five factors, which included 30 of the 35 items and accounted for 42.00% of the variance. The construct validity of the 5-factor model was supported by the results of our confirmatory factor analysis. The factors were the 1) ability to recognize mental disorders, 2) confidentiality of mental health practitioners, 3) skills of mental health information seeking, 4) beliefs about mental illnesses, and 5) attitudes toward patients with mental illness.
Conclusion: The study provides initial support for the use of the MHLS among Persian/Farsi speaking adults to assess mental health literacy.
Keywords: mental health literacy, reliability, validity
Introduction
Globally, mental disorders make up a third of the burden of illness among adolescents,1 and 70% to 75% of adult mental health problems and disorders begin during adolescence.2,3 Additionally, untreated mental disorders in adolescents are known to be a predictor of poor vocational achievements, problematic interpersonal and family functioning, and reduced life expectancy due to associated medical conditions.4–7 Research shows, worldwide, between 70% and 80% of young people and adults do not receive the mental health care that they need.8–10
Despite the high global prevalence of mental illness,11 a significant treatment gap remains between requiring and receiving the care.12 One of the main reasons for this gap is low levels of the mental health literacy (MHL),13,14 which refers to an individual’s knowledge and ability to make sound mental health decisions in everyday life.13 The MHL is considered a significant determinant of mental health;15,16 however, it is a relatively new concept in health promotion research. Additionally, the MHL has been identified as an important determinant of public mental health,13,16–18 a prerequisite for early recognition and intervention in mental disorders, and a focus of research for the past few decades.19 Unfortunately, the overall level of knowledge about mental health is low.20–22 For example, it is reported that a large number of people are unable to identify signs and symptoms of common disorders21 and fail to participate in preventative and treatment programs that are designed to provide mental health services in low to middle-income countries.23–25
A systematic review of the literature showed that the knowledge of mental health and disorders, awareness of help-seeking guidelines, and reducing the stigma against mental illness at individual, community, and institutional levels may promote early identification of mental disorders, improve mental health outcomes, and increase participation in mental health services.26–28 There is some evidence that adolescent girls have a higher prevalence of psychological disorder.29,30 The girls are more vulnerable to the consequences of mothers’ mental problems than are boys.31,32 Additionally, lack of recognition of mental health problems among young people and their parents is a major barrier to help-seeking efforts.33 Mothers play an important role in younger adolescents’ development, especially among daughters;34 as a result, maternal health literacy can empower women to address factors that affect outcomes for both mothers and children.35–37
Although the MHL is considered an important determinant of mental health and has the potential to benefit both the individual and the public,15,16 its use in evidence-based practices and health promotion interventions has been limited.38 O’Connor et al39 conducted an extensive literature review and reported that most of the related investigations had not adequately addressed the psychometric properties of the measuring instruments. Additionally, they noted several important constructs (ie, disorder recognition, help and information-seeking behavior, risk factor identification, causes of mental illness, self-treatment/coping, and risk factors) had not been sufficiently investigated.
Due to the lack of an instrument to measure mental health literacy among Persian/Farsi speaking people, this study was conducted to examine the psychometric properties of the Persian version of the Mental Health Literacy Scale (P-MHLS).
Participants and Methods
Subject Selection
The study was cross-sectional in nature, delimited to the mothers of female high school children, and conducted between February and April 2019 in Tabriz, Iran. The sample size estimation was based on the recommendation of having five (5) to ten (10) subjects per the scale’s items.40 We employed multistage sampling. Specifically, out of the five (5) educational districts in Tabriz, one (1) was selected at random, followed by selecting three (3) high schools within the same geographic location in the district. The mothers of all 7th to 9th graders (n = 1030) were invited to participate in the study, of which, 992 met the inclusion criteria of living with the child and being literate, and voluntarily agreed to take part in data collection. A survey questionnaire was used, which took 20 to 30 minutes to complete by the participants. The study was conducted in accordance with the ethical standards in the 1964 Declaration of Helsinki and its later amendments. All participants signed informed consent forms. Permission to conduct the study was obtained from the Ethical Research Committee of Tabriz University of Medical Sciences (#IR.TBZMED.REC.1397.527).
Translation Validity
The MHLS was developed to assess knowledge of a range of areas in mental health and attitudes toward mental health and help-seeking behaviors.41 The translation of the MHLS from English to Persian (Farsi) was conducted based on the international guidelines.9 First, two bilingual native Iranians with knowledge of social science and psychology performed the translation independently. Second, the two translators and the primary investigator (PI) discussed the translated version until reaching a consensus. Third, the Persian (Farsi) version was independently back-translated into English by two professionals in English language translation who were not aware of the original English version. Fourth, all translations were reviewed by a panel of experts, consisting of a psychologist, a psychometrician, a neurologist, two health education specialists, and the translators, who approved the content validity of the P-MHLS, which was later pilot-tested for its utility by 30 mothers who were excluded from the main study.
Persian Mental Health Literacy Scale (P-MHLS)
The P-MHLS is a self-reported tool, consisting of 35 items rated on a 4-point (1–4) or a 5-point (1–5) Likert-type scaling, with 12 reverse-coded (10, 12, 15, 20–28) items. The theoretical range for the total score is 35 to 160, higher scores indicate higher levels of mental health literacy.
Statistical Analysis
All analyses were conducted, using the STATA 14 (Stata Corp, College Station, TX). Descriptive statistics were used to summarize and organize the data. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were performed. The structural equation modeling (SEM) utilized maximum-likelihood estimates.42 Skewness and Kurtosis were examined to examine the normality of the distributions. The level of significance was set, a priori, at 0.05.
Construct Validity
The EFA and CFA were performed to examine the construct validity of the P-MHLS, utilizing two subsamples of 496 and 496, respectively. The sampling adequacy was examined by Kaiser–Meyer–Olkin (KMO) test, and 0.70 was used as an indicator of satisfactory EFA. In addition, the correlation matrix was tested with Bartlett’s test of sphericity, which ruled out the identity matrix. The factor loading of at least 0.30 was considered as acceptable, and eigenvalues greater than 1.00 determined the factor.43
To assess how well the EFA-extracted model fit the observed data, a CFA was performed, using the method of weighted least squares for estimation. The asymptotic covariance matrix was considered a weighted matrix. The input consisted of a covariance matrix of the data. The following indicators of goodness of fit were used: root-mean-square error of approximation (RMSEA) < 0.08, comparative fit index (CFI) ≥ 0.90, Tucker–Lewis index (TLI) ≥ 0.90, and standardized root-mean-square residual (SRMSR) < 0.08.44
Reliability
We used Cronbach’s coefficient alpha to estimate the reliability/internal consistency of the scale. The theoretical range is 0.00 to 1.00.
Feasibility
To assess the feasibility of the measures, the percentages of possible minimum and maximum scores were computed as floor and ceiling effects, respectively. Less than 15% was considered adequate.
IRT Model
Item response theory (IRT) models were utilized to characterize the test items based on their discrimination and difficulty indices. A discrimination index is used to describe the sensitivity of the test to differentiate among severity of the characteristics. The purpose of the difficulty index is to identify the level of a perceived problem needed to achieve a 50% probability of choosing a particular score45 and contributes to the overall information provided by the test.42
Results
A Profile of Subjects
The study’s participants were mothers of 992 adolescents, mostly housewives (82.70%) with one child (52.40%), four family members (60.00%), and moderate economic status (63.60%). The level of education ranged from primary school to university with high school diploma as the mode (47.30%). Approximately, one-third could neither identify children’s mental problems nor access assistance (26.30% and 31.00%, respectively). Results are summarized in Table 1.
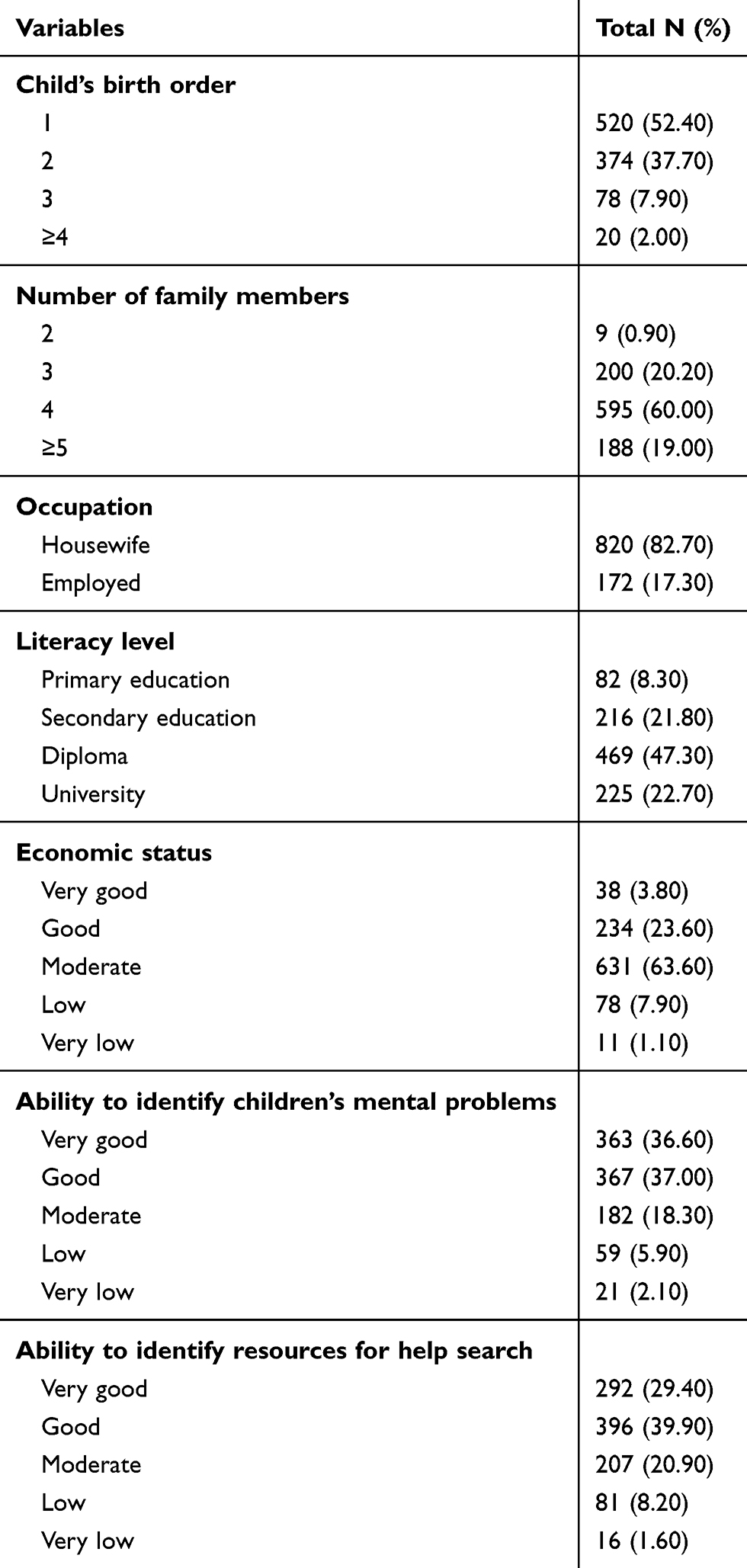 |
Table 1 A Profile of the Subjects (n = 992) |
The EFA portion of the study utilized the data from half of the 992 participants and employed Varimax rotation, because we had conceptualized that the underlying constructs were independent of each other. The KMO measure of sampling adequacy was 0.80 and Bartlett’s Test of Sphericity was statistically significant, suggesting that the correlation matrix was suitable for factor analysis. Five (5) meaningful constructs/factors emerged, namely, 1) ability to recognize mental disorders (11 items), 2) confidentiality of mental health practitioners (9 items), 3) skills of mental health information seeking (4 items), 4) beliefs about mental illnesses (4 items), and 5) attitudes toward patient with mental illness (2 items), which accounted for 42.00% of the cumulative variance. Five items did not load on any of the factors. Results are summarized in Table 2.
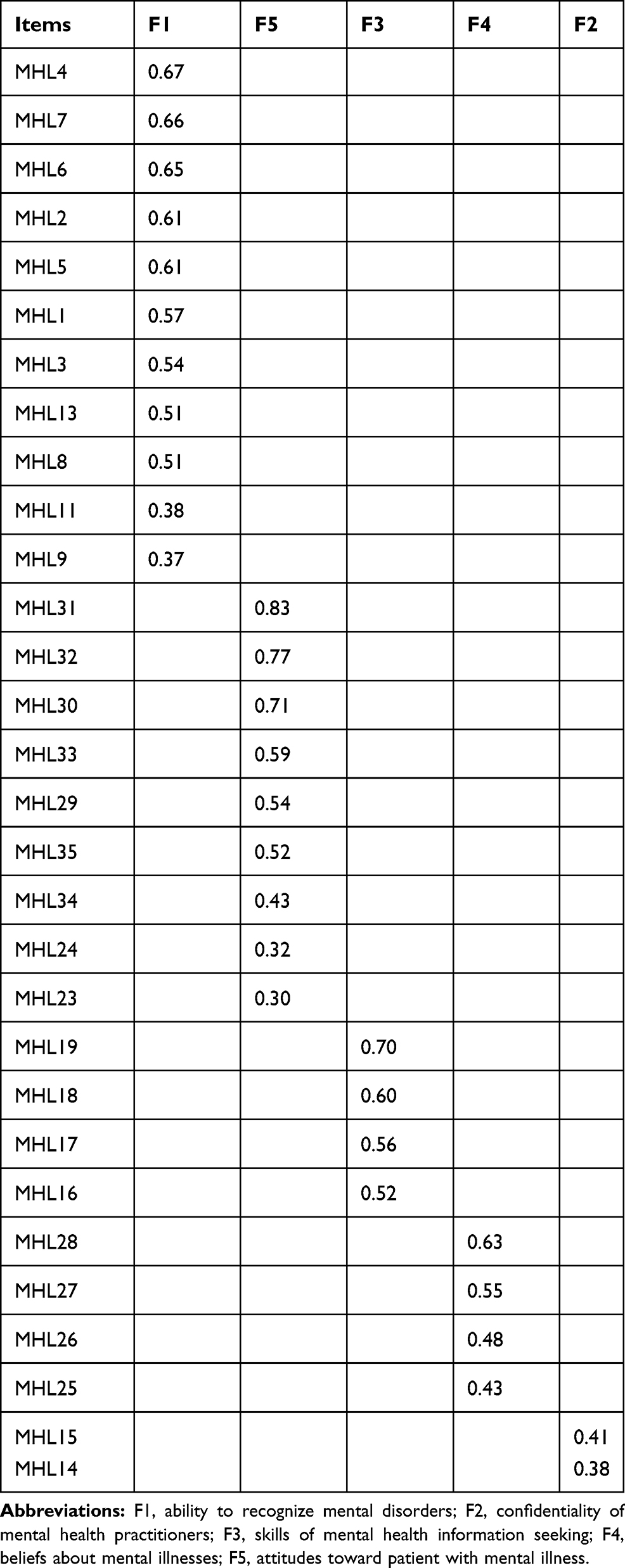 |
Table 2 Factor Structure of the Persian Mental Health Literacy Scale (n = 496) |
Feasibility and Reliability
The percentages of the ceiling and floor scores, utilizing the data from all participants, were less than 15.00% for the five (5) factors, attesting to the feasibility of the P-MHLS. Skew and Kurtosis coefficients did not suggest departure from normality. Reliability coefficients ranged from 0.61 to 0.82. Item total correlation coefficients ranged from 0.05 (items 10) to 0.42 (item 7). Results are summarized in Table 3.
 |
Table 3 A Summary of the Characteristics of the Factors (n = 992) |
Construct Validity
The CFA potion of the investigation utilized the other half of the observations and results showed that the model fit the data. Specifically, the following indices were obtained: RMSEA = 0.04, TLI = 0.91, CFI = 0.92, and SRMSR = 0.05. Results are shown in Table 4 and Figure 1.
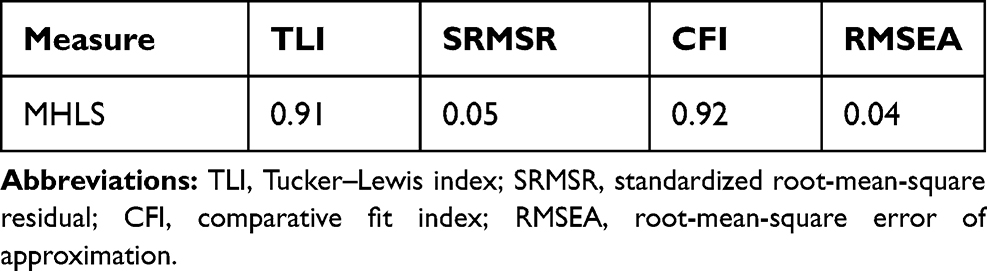 |
Table 4 The Confirmatory Factor Analysis Indices of the Persian Mental Health Literacy Scale (n = 496) |
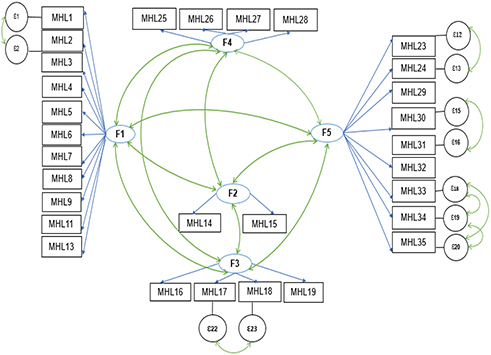 |
Figure 1 Confirmatory factor analysis of the five-factor model of the P-MHLS. |
IRT Model
The P-MHLS items were summed so that higher scores reflected better levels of mental health literacy. The overall fit of the model was found to be adequate (Chi-square = 356.42, df = 160, p < 0.05). The items and parameter estimates are summarized in Table 5.
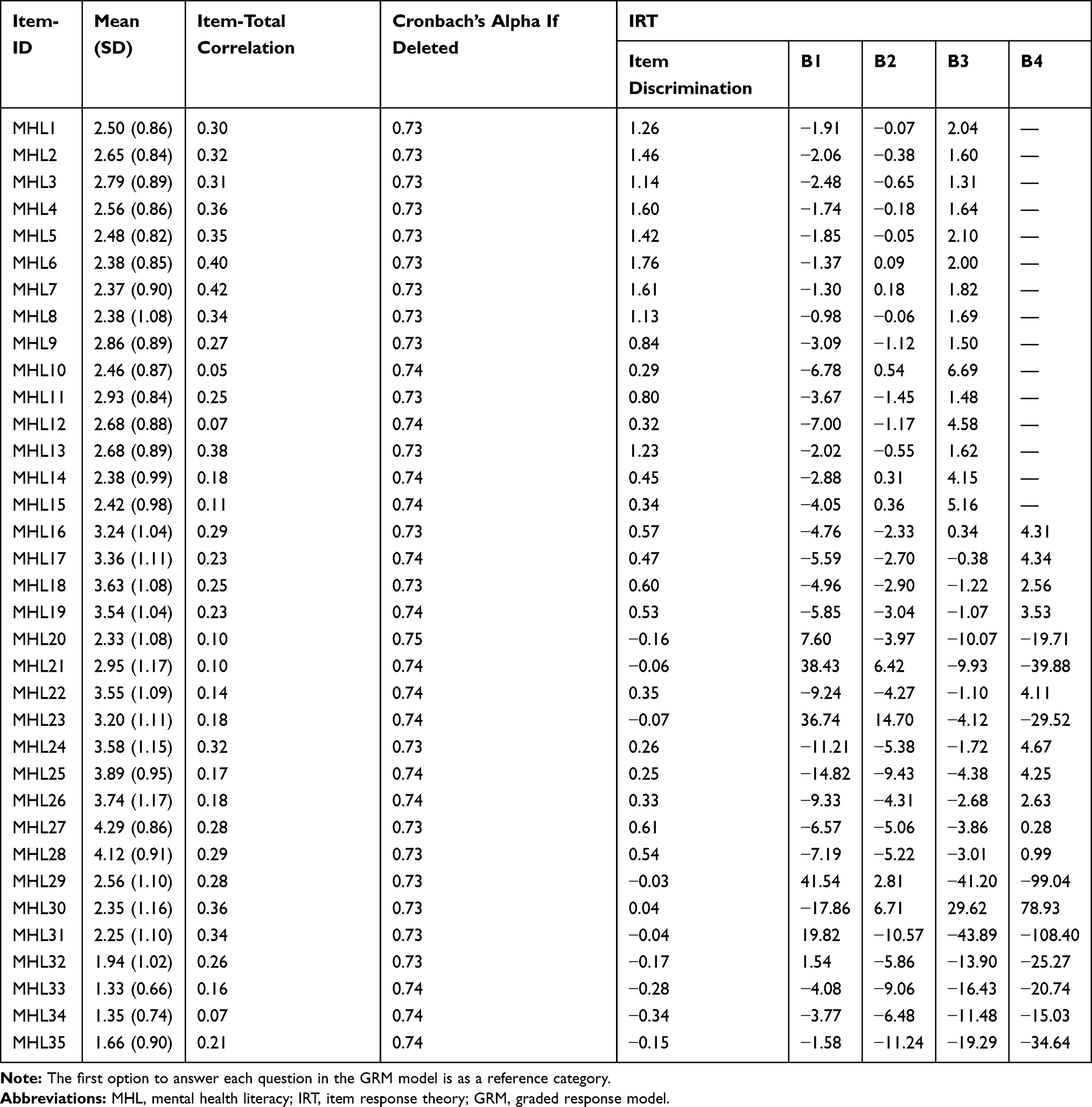 |
Table 5 IRT Calibration Results of the Persian Mental Health Literacy Scale Item Bank (N= 992) |
Discussion
The primary purpose of the study was to examine and document the psychometric properties of a Persian version of the Mental Health Literacy Scale (P-MHLS). The scale consisted of 35 items. The setting was Tabriz, Iran, and data were obtained from a sample of mothers.
An exploratory factor analysis of data resulted in five factors, which included 30 of the 35 items and accounted for 42.00% of the variance. The construct validity of the 5-factor model was supported by the results of our confirmatory factor analysis. The factors were the 1) ability to recognize mental disorders, 2) confidentiality of mental health practitioners, 3) skills of mental health information seeking, 4) beliefs about mental illnesses, and 5) attitudes toward patients with mental illness. Unlike the original study, items 10, 12, 20, 21, and 22 did not load on any factor, which could have been due to the participants’ perspectives of mental health and inadequate awareness of the importance of the subject matter.
The internal consistency of the MHLS has been reported by O’Connor et al41 and Caldwell et al.46 Although the overall internal consistency of the P-MHLS was satisfactory (Table 5), it was less than the recommended 0.70 for 2nd and 4th factors; however, we kept them in the model because of their meaningfulness. These five factors were similar to the original MHLS’s six factors. The slight differences could have been due to cultural characteristics of the study’s participants. Culture may underlie presentation of sets of symptoms that are specific to certain societies or culture-bound syndromes. Actually, culture can influence the meanings that people impart to their disease, as well as the stigma associated with such illnesses.47 The feasibility of the P-MHLS was supported by the percentages of floor and ceiling effects, which were less than 15.00% for the total and subscale scores.
Strengths and Limitations
Our study has considerable strengths, including a large sample size that led to a powerful factor analysis of the data. The study also has some limitations. The setting was a major city and participants were the mothers of females, which limited the generalizability/external validity of the findings. Hence, direct and systematics replication of the study is recommended so that the results may be generalized to other populations. Due to the lack of other similar standard instruments in the literature, we could not critically examine the Persian version of the MHLS. Additionally, because of the non-experimental nature of the study, no causal inferences were drawn.
Conclusions
The current study provides initial support for the use of the MHLS among Persian/Farsi speaking adults to assess mental health literacy. Further research is recommended for cross-cultural validation of the instrument to widen its application for comparison purposes and addressing the sensitivity, feasibility and predictive validity of the scale.
Acknowledgments
The authors would like to acknowledge the sincere cooperation of the schools’ staff.
Disclosure
No potential conflicts of interest was reported by the authors.
References
1. WHO. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000–2011. Geneva: Department of Health Statistics and Information Systems; 2013.
2. Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry. 2003;60(8):837–844. doi:10.1001/archpsyc.60.8.837
3. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):593–602. doi:10.1001/archpsyc.62.6.593
4. Bhatia SK, Bhatia SC. Childhood and adolescent depression. Am Fam Physician. 2007;75(1):73–80.
5. Kessler RC, Foster C, Saunders WB, Stang PE. Social consequences of psychiatric disorders, I: educational attainment. Am J Psychiatry. 1995;152(7):1026–1032.
6. Mezuk B, Eaton WW, Albrecht S, Golden SH. Depression and type 2 diabetes over the lifespan. Diabetes Care. 2008;31(12):2383–2390. doi:10.2337/dc08-0985
7. Rugulies R. Depression as a predictor for coronary heart disease: a review and meta-analysis. Am J Prev Med. 2002;23(1):51–61. doi:10.1016/S0749-3797(02)00439-7
8. Leaf PJ, Alegria M, Cohen P, et al. Mental health service use in the community and schools: results from the four-community MECA study. Methods for the epidemiology of child and adolescent mental disorders study. J Am Acad Child Adolesc Psychiatry. 1996;35(7):889–897. doi:10.1097/00004583-199607000-00014
9. Thornicroft G. Most people with mental illness are not treated. Lancet. 2007;370(9590):807–808. doi:10.1016/S0140-6736(07)61392-0
10. Waddell C, McEwan K, Shepherd CA, Offord DR, Hua JM. A public health strategy to improve the mental health of Canadian children. Can J Psychiatry. 2005;50(4):226–233. doi:10.1177/070674370505000406
11. Steel Z, Marnane C, Iranpour C, et al. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. Int J Epidemiol. 2014;43(2):476–493. doi:10.1093/ije/dyu038
12. Results from the 2011 National Survey on Drug Use and Health: Mental Health Findings. U.S. Department of Health and Human Services Substance Abuse and Mental Health Services Administration Center for Behavioral Health Statistics and Quality. 2012.
13. Jorm AF. Mental health literacy: empowering the community to take action for better mental health. Am Psychol. 2012;67(3):231–243. doi:10.1037/a0025957
14. Kelly CM, Jorm AF, Wright A. Improving mental health literacy as a strategy to facilitate early intervention for mental disorders. Med J Aust. 2007;87(7 Suppl):S26–30.
15. Wei Y, McGrath PJ, Hayden J, Kutcher S. Mental health literacy measures evaluating knowledge, attitudes and help-seeking: a scoping review. BMC Psychiatry. 2015;15(1):291. doi:10.1186/s12888-015-0681-9
16. Kutcher S, Wei Y, Coniglio C. Mental health literacy: past, present, and future. Can J Psychiatry. 2016;61(3):154–158. doi:10.1177/0706743715616609
17. Broder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM. Erratum to: health literacy in childhood and youth: a systematic review of definitions and models. BMC Public Health. 2017;17(1):419. doi:10.1186/s12889-017-4365-x
18. Wei Y, Hayden JA, Kutcher S, Zygmunt A, McGrath P. The effectiveness of school mental health literacy programs to address knowledge, attitudes and help seeking among youth. Early Interv Psychiatry. 2013;7(2):109–121. doi:10.1111/eip.12010
19. Campos L, Dias P, Palha F, Duarte A, Veiga E. Development and psychometric properties of a new questionnaire for assessing mental health literacy in young people. Univ Psychol. 2016;15(2):61–72. doi:10.11144/Javeriana.upsy15-2.dppq
20. Bartlett H, Travers C, Cartwright C, Smith N. Mental health literacy in rural Queensland: results of a community survey. Aust N Z J Psychiatry. 2006;40(9):783–789. doi:10.1080/j.1440-1614.2006.01884.x
21. Jorm AF, Christensen H, Griffiths KM. The public’s ability to recognize mental disorders and their beliefs about treatment: changes in Australia over 8 years. Aust N Z J Psychiatry. 2006;40(1):36–41. doi:10.1080/j.1440-1614.2006.01738.x
22. Farrer L, Leach L, Griffiths KM, Christensen H, Jorm AF. Age differences in mental health literacy. BMC Public Health. 2008;8(1):125. doi:10.1186/1471-2458-8-125
23. Parker G, Lee C, Chen H, Kua J, Loh J, Jorm AF. Mental health literacy study of general practitioners: a comparative study in Singapore and Australia. Australas Psychiatry. 2001;9(1):55–59. doi:10.1046/j.1440-1665.2001.00304.x
24. Thara R, Srinivasan TN. How stigmatising is schizophrenia in India? Int J Soc Psychiatry. 2000;46(2):135–141. doi:10.1177/002076400004600206
25. Kermode M, Bowen K, Arole S, Joag K, Jorm AF. Community beliefs about causes and risks for mental disorders: a mental health literacy survey in a rural area of Maharashtra, India. Int J Soc Psychiatry. 2010;56(6):606–622. doi:10.1177/0020764009345058
26. Rusch N, Evans-Lacko S, Henderson C, Flach C, Thornicroft G. Knowledge and attitudes as predictors of intentions to seek help for and disclose a mental illness. Psychiatr Serv. 2011;62(6):675–678. doi:10.1176/ps.62.6.pss6206_0675
27. Corrigan PW, Watson AC. Factors that explain how policy makers distribute resources to mental health services. Psychiatr Serv. 2003;54(4):501–507. doi:10.1176/appi.ps.54.4.501
28. Henderson C, Evans-Lacko S, Thornicroft G. Mental illness stigma, help seeking, and public health programs. Am J Public Health. 2013;103(5):777–780. doi:10.2105/AJPH.2012.301056
29. Khalid S, Gelban AL. Prevalence of psychological symptoms in Saudi secondary school girls in Abha, Saudi Arabia. Ann Saudi Med. 2009;29(4):275–279. doi:10.4103/0256-4947.55308
30. Mundy LK, Simmons JG, Allen NB, et al. Study protocol: the childhood to adolescence transition study (CATS). BMC Pediatr. 2013;13(160). doi:10.1186/1471-2431-13-160.
31. Grant KE, Compas BE, Stuhlmacher AF, Thurm AE, McMahon SD, Halpert JA. Stressors and child and adolescent psychopathology: moving from markers to mechanisms of risk. Psychol Bull. 2003;129(3):447–466. doi:10.1037/0033-2909.129.3.447
32. Bosco GL, Renk K, Dinger TM, Epstein MK, Phares V. The connections between adolescents’ perceptions of parents, parental psychological symptoms, and adolescent functioning. J Appl Dev Psychol. 2003;24(2):179–200. doi:10.1016/S0193-3973(03)00044-3
33. Logan DE, King CA. Parental facilitation of adolescent mental health service utilization: a conceptual and empirical review. Clin Psychol Sci Pract. 2001;8(3):319–333. doi:10.1093/clipsy.8.3.319
34. Updegraff KA, Delgado MY, Lorey A, Wheeler LA. Exploring mothers’ and fathers’ relationships with sons versus daughters: links to adolescent adjustment in Mexican immigrant families. Sex Roles. 2009;60(7–8):559–574. doi:10.1007/s11199-008-9527-y
35. Lu MC, Halfon N. Racial and ethnic disparities in birth outcomes: a life-course perspective. Matern Child Health J. 2003;7(1):13–30. doi:10.1023/A:1022537516969
36. Mobley SC, Thomas SD, Sutherland DE, Hudgins J, Ange BL, Johnson MH. Maternal health literacy progression among rural perinatal women. Matern Child Health J. 2014;18(8):1881–1892. doi:10.1007/s10995-014-1432-0
37. Smith SA, Carroll LN. Data-driven maternal health literacy promotion and a postscript on its implications. Inf Serv Use. 2017;37(2):235–252. doi:10.3233/ISU-170832
38. Riebschleger J, Costello S, Cavanaugh DL, Grove C. Mental health literacy of youth that have a family member with a mental illness: outcomes from a new program and scale. Front Psychiatry. 2019;10(2). doi:10.3389/fpsyt.2019.00002
39. O’Connor M, Casey L, Clough B. Measuring mental health literacy – a review of scale-based measures. J Ment Health. 2014;23(4):197–204. doi:10.3109/09638237.2014.910646
40. Yong AG, Pearce S. A beginner’s guide to factor analysis: focusing on exploratory factor analysis. Tutor Quant Methods Psychol. 2013;9(2):79–94. doi:10.20982/tqmp.09.2.p079
41. O’Connor M, Casey L. The mental health literacy scale (MHLS): anew scale-based measure of mental health literacy. Psychiatry Res. 2015;229(1–2):511–516. doi:10.1016/j.psychres.2015.05.064
42. Corp S. Stata Statistical Software: Release 14. Station C, Editor. TX: StataCorp LP; 2015.
43. Tinsley HE, Brown SD. Handbook of Applied Multivariate Statistics and Mathematical Modeling. Academic Press; 2000.
44. Woo JP. The Concept and Understanding of Structural Equation Model. Seoul: Hannarae Academy; 2012.
45. Nguyen TH, Han HR, Kim MT, Chan KS. An introduction to item response theory for patient-reported outcome measurement. Patient. 2014;7(1):23–35. doi:10.1007/s40271-013-0041-0
46. Caldwell T, Jorm A. Mental health nurses‘ beliefs about interventions for schizophrenia and depression: a comparison with psychiatrists and the public. Aust N Z J Psychiatry. 2000;34(4):602–611. doi:10.1080/j.1440-1614.2000.00750.x
47. Lasebikan VO. Cultural aspects of mental health and mental health service delivery with a focus on Nigeria within a global community. Ment Health Relig Cult. 2016;19(4):323–328. doi:10.1080/13674676.2016.1180672
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.